
Abstract
The effort to standardize the methodology and adherence to recommended principles for all economic evaluations has been emphasized in medical literature. The objective of this review is to examine whether economic evaluations in traumatic brain injury (TBI) research have been compliant with existing guidelines. Medline search was performed between January 1, 1995 and August 11, 2012. All original TBI-related full economic evaluations were included in the study. Two authors independently rated each study's methodology and data presentation to determine compliance to the 10 methodological principles recommended by Blackmore et al. Descriptive analysis was used to summarize the data. Inter-rater reliability was assessed with Kappa statistics. A total of 28 studies met the inclusion criteria. Eighteen of these studies described cost-effectiveness, seven cost-benefit, and three cost-utility analyses. The results showed a rapid growth in the number of published articles on the economic impact of TBI since 2000 and an improvement in their methodological quality. However, overall compliance with recommended methodological principles of TBI-related economic evaluation has been deficient. On average, about six of the 10 criteria were followed in these publications, and only two articles met all 10 criteria. These findings call for an increased awareness of the methodological standards that should be followed by investigators both in performance of economic evaluation and in reviews of evaluation reports prior to publication. The results also suggest that all economic evaluations should be made by following the guidelines within a conceptual framework, in order to facilitate evidence-based practices in the field of TBI.
Introduction
I
Methods for healthcare-related economic evaluation studies were well described in the medical literature 3 decades ago. 12 Since then, many guidelines have been published on the use of economic methods in the evaluation of health care practices and technologies. 13 –18 These methods are intended to enhance the validity of the health- and economic evaluation studies and reduce bias. The primary aim of economic evaluation studies is to evaluate the outcomes and costs of interventions simultaneously, such as interventions designed, for example, to improve health or prevent diseases.
Health economic evaluation comparatively analyzes the cost and effect of two or more interventions. In general, there are four different types of economic evaluations: cost-benefit analysis (CBA), cost minimization analysis (CMA), cost-effective analysis (CEA), and cost-utility analysis (CUA). 17,18 CBA addresses the question of “should a given goal be pursued to a greater or less extent?” and measures both the benefit and cost of two or more alternative interventions in terms of the potential money gained or saved as compared to the money invested in the intervention. CMA and CEA are commonly used to answer the research question of “which is the most efficient way of achieving a given health benefit?” When the intervention alternatives are known to produce the same benefit but different cost, CMA searches for the least costly alternative. However, when the alternatives are different in both benefit and cost, CEA compares the per unit benefit with per unit cost on an incremental basis of the alternatives. CUA can be used to decide the best way of spending a given budget. The approach employs utilities, such as quality-adjusted life-years (QALYs) or disability-adjusted life-years (DALYs), as the outcome measure to compare and evaluate two or more interventions incrementally. CUA is similar to CEA if monetary unit is applied to the effect, such as life-years gained per monetary units. However, this two are different if the effect is measured in terms of more disease specific outcomes.
The effort to standardize methodology and adherence to the recommended principles for all economic evaluations has been emphasized in medical literatures and journals. 12,13,15 –18 Several studies evaluating the adherence of economic evaluations from various disciplinarians have suggested low compliances and insufficiencies. 19 –23 However, to our knowledge, no existing study has evaluated whether the principles of economic evaluations have been successfully incorporated into intervention and prevention programs in the field of TBI.
Thus far, the results from many published economic evaluation studies in TBI have limited general applications and comparability between the studies, which can be attributed to various analytic approaches, types of costs, data sources for costs and outcome measures, and lack of sensitivity analysis to handle uncertainty. The objective of this review is to evaluate and compare the methods of economic evaluations in TBI research with existing guidelines through an evaluation and synthesis of information in the published literature. It is expected that the findings will be used to facilitate more standardized cost-benefit, cost-effective, and cost-utility evaluations of diagnostic, intervention, and prevention programs in TBI. Such information could form an evidence base for decision making in the future.
Materials and Methods
Search methodology and inclusion/exclusion criteria
A two-stage systematic search of the English-language medical literature for original TBI-related economic evaluation studies published from January 1, 1995 through August 11, 2012 using Medline was conducted. The search terms included “cost-effective,” “cost-effectiveness,” “cost-utility,” “cost-benefit,” or “health care cost” and “traumatic brain injury” or “head injury” to identify articles that included economic evaluations in TBI related diagnostic, intervention, and prevention subjects. These articles were screened to identify those that fulfilled the criteria of a full economic evaluation using descriptions by Drummond MF et al., as summarized in Table 1. 17
The inclusion criteria used to define the sample of articles were: (1) Subject: all original quantitative economic evaluation studies in TBI-related studies; (2) Analysis: only complete cost-benefit, cost-effective, and cost-utility analyses. The exclusion criteria were: (1) Subject: reviews or commentaries of economic evaluations; (2) Analysis: evaluations that did not include full considerations of outcomes or costs or used cost-minimization approaches because cost-minimization only evaluates the costs and compares alternatives with the same outcomes.
Based on the defined eligibility, two authors (J.L. and N.A.) independently screened titles of all reports captured by the search (n=613) and eliminated those (n=506) that were unrelated to the study interest. Both authors then independently evaluated the remaining 107 abstracts and further excluded articles (n=66) that did not meet the study inclusion criteria. The resulting 41 articles were subject to full-text review to determine final inclusion. Through the full article review, 13 articles were further excluded. Of the excluded studies, 10 studies used approaches other than CBA, CEA, or CUA; two studies assessed cost only, and one did not use original data. Therefore, a total of 28 articles were included in this review for data extraction. Figure 1 depicts our article identification process.
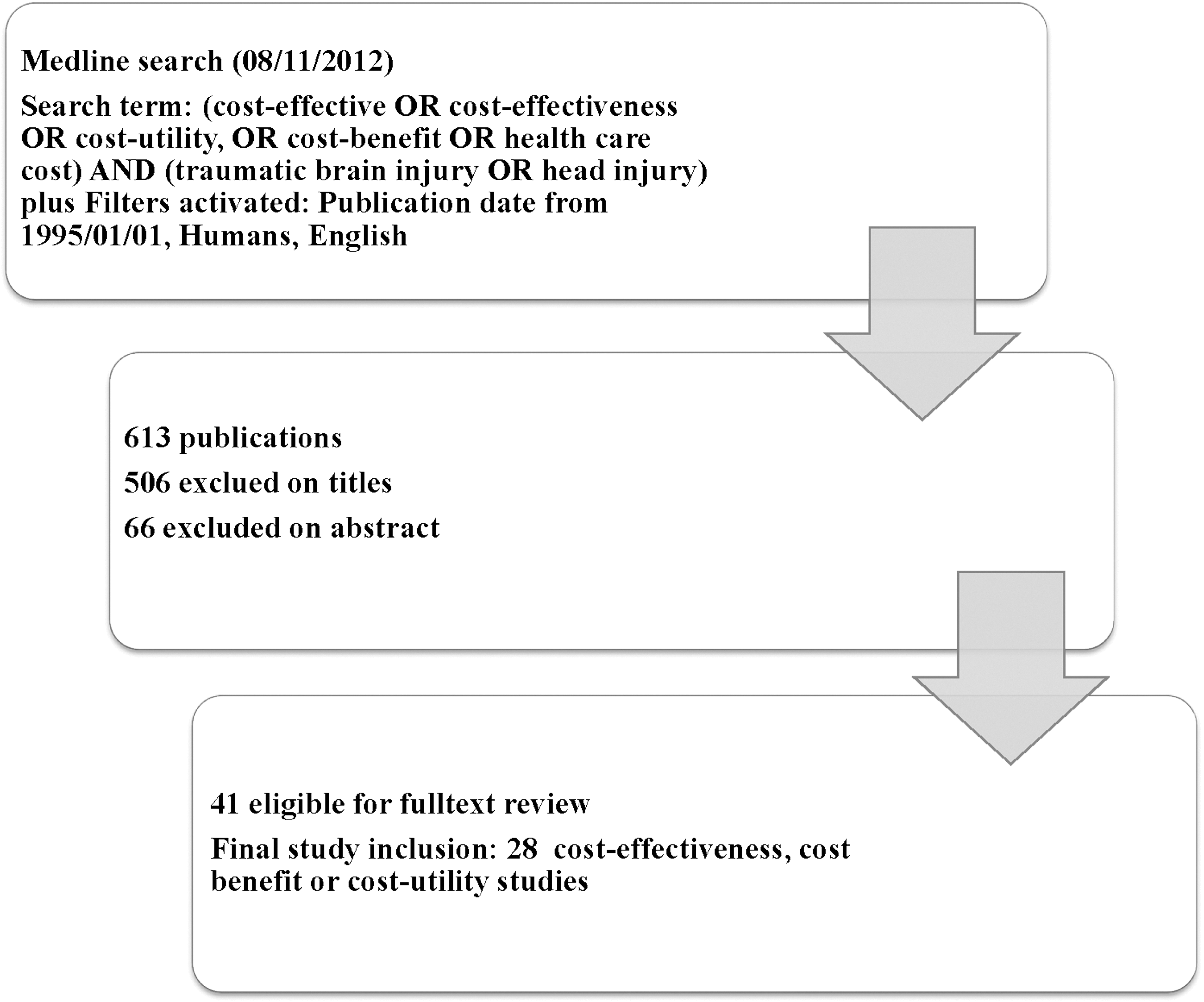
Search methodology and article identification process.
Data extraction and data analysis
The data were extracted using the structured data extraction sheet as described below. Two authors (J.L. and N.A.) independently audited each study on the methodological and reporting practices used and evaluated adherence to the recommended methodological principles based on the 10 criteria presented in Table 2. The articles were graded for the presence or absence of each of the methodological criteria (1=yes and 0=no). Descriptive analysis was used to summarize the data. The types and methods of cost analysis were summarized by type of analysis (i.e., CEA, CUA, CBA), as well as across all analyses. The discrepancies between the two authors were re-reviewed and consensus was used for final results. Inter-rater reliability was assessed via Kappa statistics. 24 In general, the strength of agreement could be described by Kappa statistics as poor (<0.2), fair (>2 to ≤0.4), moderate (>0.4 to ≤0.6), good (>0.6 to ≥0.8), and very good (>0.8 to ≤1). 25 Overall agreement between two independent authors for all criteria was 95% and simple kappa=0.88 (95% Confidence interval=0.82–0.94), indicating very good agreement.
Methodological standards
Ten methodological principles recommended by Blackmore et al. 19 and used by Kruper et al. 21 were used to evaluate the articles (Table 2). These principles are consistent with the general economic evaluation guidelines. 17,18,23,26 –28 We intend to use these principles as the cross disciplinary minimum requirements for assessing the quality of TBI-related economic evaluation studies and for facilitating standardized methodology in the field. For the purpose of this review, we slightly adapted description of the principles in order to be consistent with the TBI literature.
Results
A total of 28 studies met the inclusion criteria. Table 3 shows the characteristics of these studies, including 18 (64%) cost-effective, 29 –46 7 (25%) cost-benefit, 2,35,47 –51 and 3 (11%) cost-utility 52 –54 analyses. Nine (32%) studies are retrospective design using existing data from registry, surveillance, or other resources; seven (25%) are prospective design, and five (18%) survey or cross-sectional studies. Other designs include clinical trial (one study), cohort (two studies), case-control (one study), and other approaches (three studies). Various subjects were assessed by these economic evaluations, including six (22%) on injury preventions (e.g., helmet use), seven (25%) on diagnostic strategies (e.g., routine serial computed tomography screening of TBI patients), four (14%) on rehabilitation programs, and two (7%) on social/community support programs, three (11%) on surgical, two (7%) on drug treatments, two (7%) on other treatments, and two (7%) on overall TBI related healthcare costs. In addition, 10 out of 28 studies (36%) used decision analytic modeling approach to predict outcomes and economic costs associated with TBIs.
Table 4 displays studies that met the inclusion criteria in compliance with 10 major methodological criteria. The mean number of criteria met by all 28 articles was 6.3 out of the possible 10. Two articles met all 10 criteria. The range of compliance with individual criteria was as high as 96% and as low as 39%. It is noticeable that most of studies were able to (1) give a description of comparative options (93%), (2) give a statement of perspective analysis (96%), (3) define study outcome measures (93%), (4) provide definitions of cost data (96%), and (5) give explicit examination of sources of such cost data (93%). Conversely, it is also evident that half or more than half of the studies failed to (1) include long-term costs in their economic evaluations or provide explanation of why long-term costs were not included (39% compliance), (2) discount future costs or provide explanation of why discounting was not used (50% compliance), (3) include summary measure (50% compliance), (4) provide incremental analysis of cost-effectiveness (46% compliance), and (5) apply sensitivity analysis (55% compliance) to deal with the uncertainties of the cost evaluations.
Overall agreement 95% (Kappa=0.88; 95% confidence interval=0.82 – 0.94)
Similar trends regarding the compliances with individual methodological criteria were observed across CEAs, CBAs, and CUAs. As shown in Table 5, all approaches showed high compliance with the criteria of (1) description of comparative options, (2) statement of perspective of analysis, (3) definition of outcome measures, and provide (4) cost data and (5) sources of cost data. Cost-benefit studies had the best compliances in the above-mentioned items among all studies. However, all approaches displayed low compliance with the criteria of (1) inclusion of long-term costs, (2) discount of future costs, (3) inclusion summary measures, (4) providing incremental analysis of cost-effectiveness, and (5) applying sensitivity analysis. Inclusion of long-term costs (compliance, 6 out of 18 studies) was the most problematic criteria to comply for CEAs, and inclusion of summary measures (compliance, 3 out of 7 studies) is the least problematic criteria to fulfill for CBAs.
Two cost-benefit studies also presented the cost effectiveness estimates.
In addition to the trend observed related to compliance with major methodological standards, the trend also indicates that the published reports in assessments of TBI related healthcare costs increased substantially over the years. Figure 2 presents the number of articles with TBI-related economic evaluation studies for specific publication periods. Between 1995 and 1999, only two reports were eligible for this study. However, between 2000 and 2004, and 2005 and 2009, the number of reports doubled and increased to six and 12, respectively. Since 2010 to August 11, 2012, eight reports were eligible for this review and still the number of reports is expected to grow.
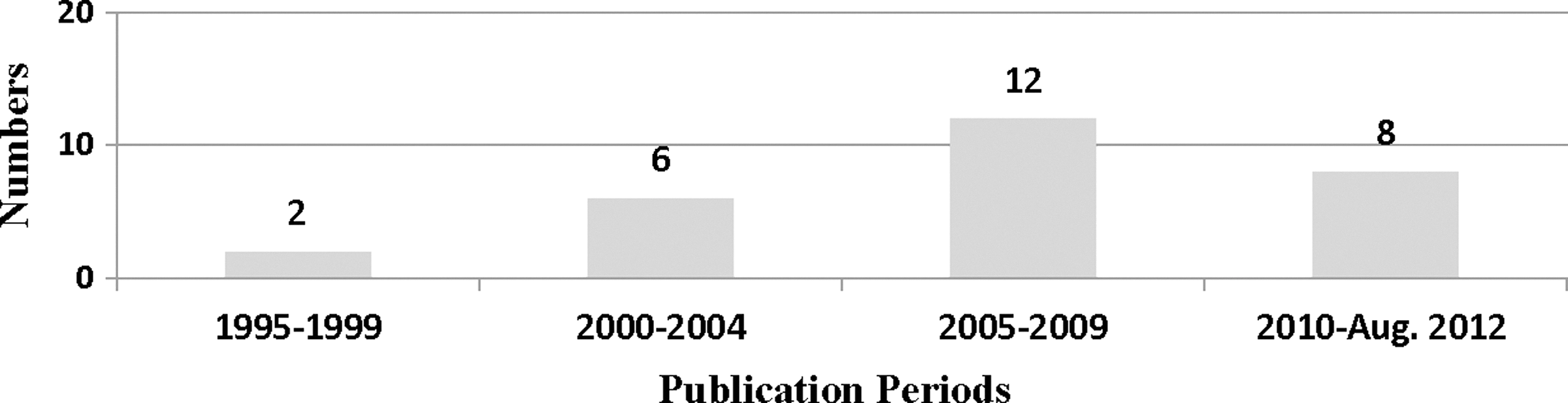
The number of articles with traumatic brain injury-related full economic analysis versus four publication periods. The results showed a rapid growth in the number of published articles on the economic impact of TBI since 2000.
Along with the increased reports, the quality of these reports has also improved in certain aspects, particularly in recent years. Figure 3 shows the percentages of studies compliant with 10 major methodological criteria versus the publication periods. While maintaining high compliances of the previously mentioned five methodological standards, the compliances also improved with the criteria of inclusion of incremental summary measures and/or summary measures, as well as application of sensitivity analysis to address uncertainties of the economic assessments. Nevertheless, low compliances with the criteria of inclusion of long-term costs and providing discount measures remained unchanged.
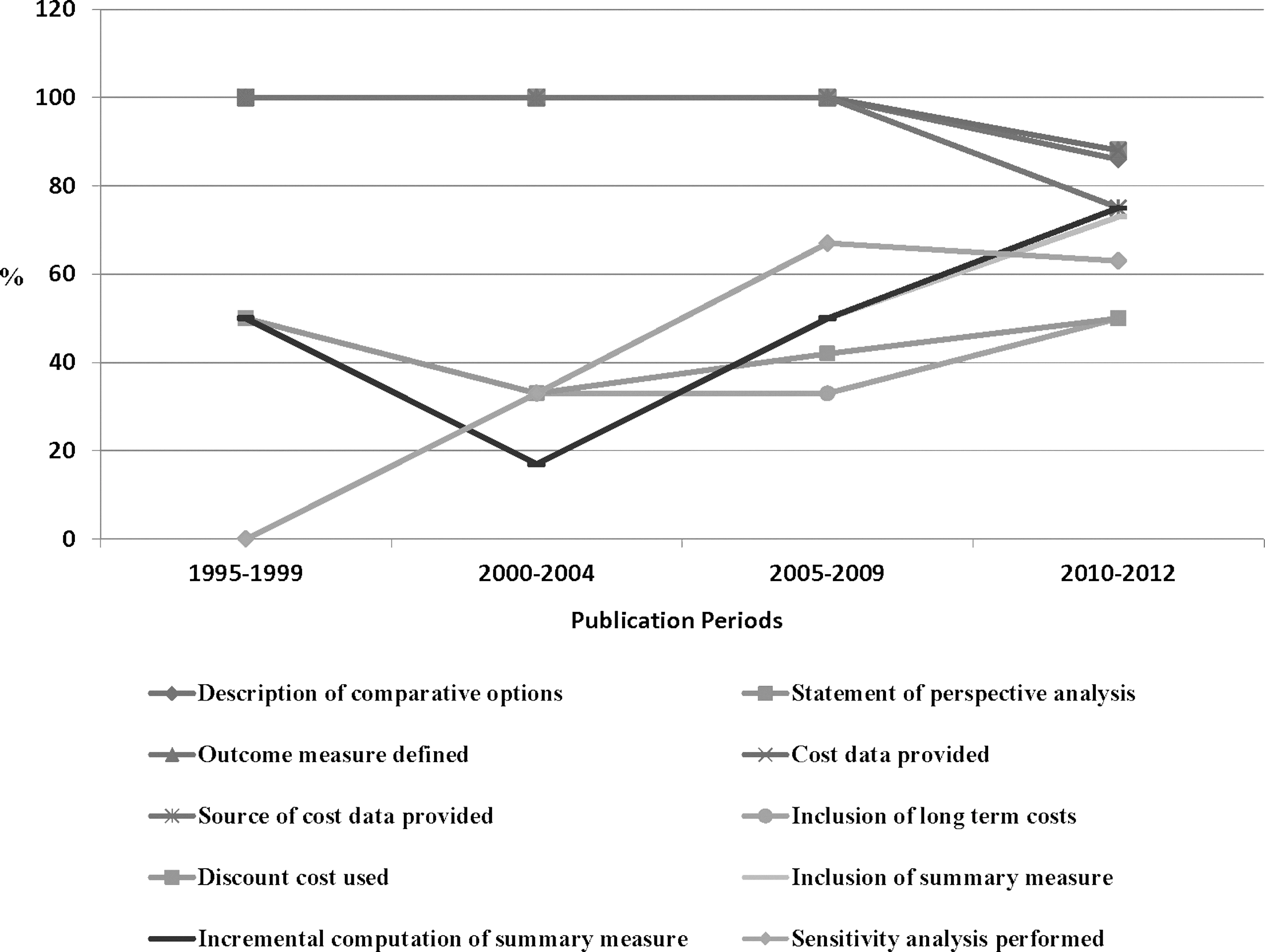
Percentages of studies compliant with 10 major methodological criteria as a function of publication periods. The results indicated that there is an improvement in the compliance with the inclusion criteria of incremental summary measures and/or summary measures, as well as application of sensitivity analysis to address uncertainties of the economic assessments. However, low compliances with the criteria of inclusion of long-term costs and providing discount measures remained unchanged.
Discussion
The review of economic evaluation studies in TBI-related research indicated that adherence to methodological criteria for reporting results was deficient. On average, about six of the 10 criteria were followed in the 28 CEA, CBA, and CUA publications reviewed. Only two articles met all 10 criteria. However, the overwhelming majority (>90%) of the studies were able to describe the comparative options, provide a statement of perspective analysis, define study outcome measures, provide definitions of cost data, and give explicit examination of sources of cost data. The most frequently neglected criteria were inclusion of long-term costs, discount of future costs, inclusion summary measures, incremental analysis of cost-effectiveness, and applying sensitivity analysis. The results showed that there has been rapid growth in the number of published articles on this topic since 2000, and the methodological quality of these articles has also improved. Nevertheless, low compliance with the criteria of inclusion of long-term costs and providing discount measures remained unchanged.
Methodological considerations
Consistent with other healthcare sectors, there has been increased emphasis on the importance of economic evaluations in healthcare programs and its dominance in influencing allocation of healthcare resource decisions in TBI. Methodological standards have also been established to reduce bias and improve the validity of economic analyses. 13,15 –18,55 Despite the long-standing effort to establish methodological standards in economic evaluations in general, this literature review has shown that few methodologically robust and comparable studies have been undertaken in the field of TBI.
The findings indicate that researchers and journal reviewers pay insufficient attention to methodological principles of economic evaluations. Furthermore, variations in methodological approaches were used also contributed to the difficulties in comparisons between the studies, including choice of the types of the economic evaluations, research perspectives and designs, health outcomes and related cost categories, adjustment for time horizon and uncertainty extrapolated.
There were several limitations to this structured review. First, our search technique relied on MeSH key words and terms and search was done in MEDLINE database only, which may not have been comprehensive to include all published economic evaluations during the search period on the combined subject of traumatic brain injury and related economic evaluations. However, studies include in the review allowed us to fulfill our primary aim to describe methodological quality of the performed studies rather than advice on allocation resources to maximize the returns on investment. Second, our study evaluated each article for adherence to the 10 basic methodological principles recommended by previous studies. 19,21 We did not evaluate adherence to more rigorous checklists about strength of theoretical frameworks, quality of data sources, reporting of model assumptions, methods of obtaining estimates, or subjects of evaluations. It is important to address the basic principles first in each cost analysis. Other aspects and meta-analyses will follow once sufficient rigor is evident in high-quality studies with comparable results. Third, the reviewers were not blinded to authors or year of publications. However, the reviewers did not co-author any of the evaluated studies.
As the main focus of this review was to compare methodological approaches that were applied to the economic evaluations in TBI research with existing guidelines, we did not provide an overview of the outcomes from the reviewed studies. It may be of interest to conduct a subsequent study to comparatively summarize the actual outcomes.
Current literature on other areas of medicine
The methodological criteria of economic evaluation used in this review are parallel to those used in some other disciplines. Blackmore and Magid 19 and Blackmore and Smith 56 evaluated the methodological quality of cost-effectiveness and cost-benefit analyses in the radiology literature reported between 1989 and 1995. They also reviewed the nonradiology literature between 1990 and 1995. In accordance with our findings in TBI, adherences to the methodological criteria were low, with below 10% of the articles adhering to all the criteria. The cost data and comparative options criteria showed high compliance, while the perspective of analysis and discounting had low compliance. The authors concluded that cost-effectiveness and cost-benefit analyses reported in both radiology and nonradiology literatures are frequently deficient in adherence to basic methodological standards.
In 2007, Kruper et al. 21 evaluated the methodological quality of economic analyses of surgical procedures in the literature published from 1995 to 2004. Among 110 identified articles, the average number of criteria met was 4.1 out of 10 with 10 articles meeting all the methodological standards. The five most frequently neglected criteria: long-term costs, discounting costs, summary measures, incremental analysis, and sensitivity analysis, reported in this review is consistent with our findings. The authors concluded that an increased awareness of methodological standards in economic evaluations in surgical areas is needed.
In 1999, Chang and Beverly 20 evaluated the methodological principles of cost analysis in nursing, medical, and health services literature (1990–1996) using six principles recommended by Udvarhelyi et al. 23 (e.g., analytic perspective, beneficial effects, cost components, discounting, sensitivity analysis, and efficiency measurement). Adherence to all six principles was found in 19 of 88 articles, including 15 medical studies, four health services studies, and none of nursing studies. The authors concluded that the presented methodological principles could be useful for future nursing education and cost-analysis research designed to control cost and increase the quality of health care.
Bozic et al. 57 assessed type and quality of economic evaluation in total hip arthoplasty literature published from 1966 to 2002, using the above-mentioned methodological criteria. 23 The large number of the reviewing studies did not explicitly state perspective of the analysis or the types of cost. Only six of 81 studies adhered to all six methodological criteria. The authors pointed out that the methodological quality of future studies should be improved and recommend prospective collection of costs and outcomes data and inclusion of the economic variables in the databases of the national total joint arthroplasty.
More recently, Polinder et al. 58 reviewed and assessed the quality of economic evaluation studies on injury prevention measures published from 1998 to 2009. Study quality was evaluated using the criteria recommended by the panel on cost-effectiveness in health and medicine 26 and on guidelines developed for economic evaluation for submissions to the British Medical Journal (BMJ). These methodological standards closely parallel the methodological criteria used in this study. The majority of the 48 included studies were related to fall prevention interventions. A wide variety of methodological approaches across studies were found. Most studies have not adopted the societal perspective and not included all relevant costs and incremental analysis. The authors recommended the establishment of international guidelines on economic evaluation for injury prevention interventions, based on the established economic evaluation checklists.
This review is similar to those in other areas of medicine in its attempt to evaluate quality of economic evaluations and the presence or absence of the methodological standards in the field of TBI. Compared with the other areas of medicine, it appeared that there were a fewer numbers of full economic evaluations published in the field of TBI in the past. However, comparable with other disciplines, the economic evaluations in our review are deficient in adherence to established methodological standards. Hence, there is need of improvement in the future TBI studies.
Implications for TBI research and management
It is well known that TBI poses unique challenges to its intervention. Great advancements have been achieved over the past decades, yet, advances in basic science have not led to new treatment of clinically proven benefit. 59 –64 Similar to acute phase interventions, many post-acute rehabilitation interventions and community programs have shown effective treatment effect of TBI, but the components and effectiveness of these methods need to be further explored. 65,66 Currently, much of the treatment of TBI has moved towards standardized management that follows national and international guidelines. 67 –69 The value of economic evaluation studies for intervention in TBI would increase if the methodological approaches were in line with recommended methodology guidelines and principles. The achievement of alignment of methodological approaches will improve our understanding of key factors in cost and care of persons with TBI, and enhance the ability of policy-makers to base their decisions on objective information to maximize the effectiveness of their management and resource allocation policy in terms of TBI outcome.
Economic evaluations are among the most important outcome research in TBI. To our knowledge, this is the first study that critically examined the methodological quality of published economic evaluation studies in the TBI field. Based on this review, it is recognized that there is significant increase in utilizing economic evaluations in TBI outcome research in recent years. The methodological quality of these evaluations is improving, particularly in the area of inclusion of incremental measures and using sensitivity analysis to extrapolate uncertainties of the economic assessments. However, the overall compliance to recommended methodological principles of TBI-related economic evaluations has been insufficient in the past 15 years. The observed differences in the design and description of perspectives, outcome measures, data definition and estimation, long-term costs, discount rates, summary of the incremental measures, and sensitivity analysis performed limit the ability to make head-to-head comparisons of the most effective and efficient intervention programs in TBI. Therefore, it is important to call for an increased awareness of the methodological standards that should be followed by investigators performing economic evaluation and reviewing such reports for publication. The data also suggest that all economic evaluations should be made by following the guidelines within a conceptual framework in order to facilitate evidence-based practices in the field of TBI.
Footnotes
Acknowledgments
This study was supported by funds from Institute of Clinical Medicine and Institute of Health and Society, Research Centre for Habilitation and Rehabilitation Models and Services (CHARM), University of Oslo, Oslo, Norway.
Author Disclosure Statement
No conflicting financial interest for all authors.