
Abstract
Repetitive brain injury, particularly that occurring with sporting-related injuries, has recently garnered increased attention in both the clinical and public settings. In the laboratory, we have demonstrated the adverse axonal and vascular consequences of repetitive brain injury and have demonstrated that moderate hypothermia and/or FK506 exerted protective effects after repetitive mild traumatic brain injury (mTBI) when administered within a specific time frame, suggesting a range of therapeutic modalities to prevent a dramatic exacerbation. In this communication, we revisit the utility of targeted therapeutic intervention to seek the minimal level of hypothermia needed to achieve protection while probing the role of oxygen radicals and their therapeutic targeting. Male Sprague-Dawley rats were subjected to repetitive mTBI by impact acceleration injury. Mild hypothermia (35°C, group 2), superoxide dismutase (group 3), and Tempol (group 4) were employed as therapeutic interventions administered 1 h after the repetitive mTBI. To assess vascular function, cerebral vascular reactivity to acetylcholine was evaluated 3 and 4 h after the repetitive mTBI, whereas to detect the burden of axonal damage, amyloid precursor protein (APP) density in the medullospinal junction was measured. Whereas complete impairment of vascular reactivity was observed in group 1 (without intervention), significant preservation of vascular reactivity was found in the other groups. Similarly, whereas remarkable increase in the APP-positive axon was observed in group 1, there were no significant increases in the other groups. Collectively, these findings indicate that even mild hypothermia or the blunting free radical damage, even when performed in a delayed period, is protective in repetitive mTBI.
Introduction
R
In the current communication, we follow upon these important findings in the context of repetitive brain injury, now seeking to better understand the range of therapeutic options available as well as the utility of other established post-traumatic neuroprotective strategies. To this end, we revisit the utility of hypothermia, now moving from the moderate hypothermia used in our previous studies to mild hypothermia (35°C) to determine whether a relatively modest drop in temperature can exert any protective effects, which, obviously, could prove of clinical utility. 25 –27 Additionally, to better understand the potential involvement of damaging oxygen radicals in the process of repetitive injury and the benefits of their therapeutic attenuation, we revisit our previous studies, 22,23 now using postrepetitive administration of either superoxide dismutase (SOD) or Tempol, based upon the recognition that SOD will dismutate the superoxide anion, whereas Tempol serves as a nitroxide antioxidant that decomposes both the superoxide radical and the peroxynitrite-derived radical species, all of which have been implicated in the pathogenesis of various forms of axonal and vascular change after TBI. 28 –33 In the current communication, we report that the use of even mild hypothermia (35°C) exerts significant axonal and vascular protection when the hypothermia is initiated relatively late (1 h) after repetitive injury, with both SOD and Tempol providing comparable protection when administered in the same time frame. Collectively, these studies reaffirm the concept that the adverse consequences of repetitive mTBI can be attenuated by targeted therapeutic interventions, some of which may prove applicable to traumatically brain-injured humans.
Methods
General preparation
All experimental procedures were performed using a protocol approved by the institutional animal care and use committee at Virginia Commonwealth University (Richmond, VA). Five adult male Sprague-Dawley rats were assigned to each group. Animals were housed in individual cages on a 12-h light/dark cycle with free access to water and food.
Animals were intraperitonally anesthetized with sodium pentobarbital at 60–65 mg/kg. After completion of a tracheotomy, they were mechanically ventilated with room air (Harvard Apparatus, Holliston, MA). Then, the femoral artery and vein were cannulated with a PE50 catheter (Becton Deckinson, Spark, MD). An arterial catheter was used for continuous monitoring of arterial pressure (PowerLab; AD Instruments, Colorado Springs, CO) and periodic blood sampling. Arterial blood partial oxygen pressure (PaO2), partial carbon dioxide pressure (PaCO2), and pH value were maintained within a normal range. PaCO2 was controlled between 35 and 40 mmHg by adjusting respiratory volume and/or rate (Stat Profile® pHOx; Nova Biomedical, Waltham, MA). A venous catheter was used for administration of medication. To maintain an adequate level of anesthesia, diluted pentobarbital solution (24 mg/mL) was given intermittently by the femoral venous catheter while checking the toe pinch response. Rectal and temporalis temperatures were monitored continuously and controlled to maintain a level of 37°C using a heat lamp and/or pad throughout the experiment, except during the hypothermic period. These two respective temperatures moved in parallel. Postinjury, pancronium bromide (3 mg/kg) was administered intravenously to produce muscular blockade after the repetitive mTBI and thereby optimize our vascular assessments with controlled ventilation.
Experimental design
In this study, we investigated the effect of multiple therapeutic interventions employed after repetitive mTBI using an impact acceleration injury device. The injuries used were defined as mild based upon previous studies, 10,19 in which we recognized that a singular impact from 1 meter evoked no contusional, hemorrhagic, axonal, or microvascular change. Animals were arbitrarily divided into the four groups specified below, with each group containing 5 animals each. The experimental time course in each group is shown in Figure 1. In group 1, which constituted the control group, animals were exposed to repetitive mTBI at 3-h intervals. In the other groups, multiple therapeutic interventions, including mild hypothermia (group 2), SOD (group 3), and Tempol (group 4), all were applied 1 h after the second/repetitive insult. The dose of SOD and Tempol were based on our previous experience with these agents and the doses needed to achieve axonal and/or microvascular protection. 22,23 Pial vascular function was assessed by measuring the vascular diameter after topical acetylcholine (ACh) application at 3 and 4 h after the repetitive insult. The burden of intraparenchymal axonal damage was assessed by quantifying the number of amyloid precursor protein (APP)-positive axons in the brainstem after euthanization and fixation. Animals were anesthetized and mechanically ventilated throughout the experimental time course in this study. Macroscopic observation confirmed the absence of skull fracture and brain contusion.

This chart shows the time course for each experimental group. All animals were exposed to twice repetitive impact acceleration insults at 3-h intervals. In group 1, no intervention was administered to animals. In group 2, mild hypothermia (35°C) was initiated 1 h after repetitive mTBI and rectal temperature was maintained at 35°C for 1 h, followed by gradual rewarming. In group 3, superoxide dismutase (SOD; 60 U/mL) was administered into artificial cerebrospinal fluid (aCSF)-containing space underlying the cranial window 1 h after repetitive mTBI. Cerebral vascular was exposed to SOD solution for 3 h in total. In group 4, Tempol (10 mg/kg) was administered by the catheter placed in the femoral vein 1 h after repetitive mTBI. Vascular reactivity to acetylcholine was assessed at 3 and 4 h after repetitive mTBI. mTBI, mild traumatic brain injury; IAI, impact acceleration insult.
Group 1: Repetitive mild traumatic brain injury without intervention
Consistent with previous reports from our lab using an impact acceleration injury, 10,19 a 450-g brass weight was dropped from a height of 1 m to produce an impact without contusion, hematoma formation, impaired vascular reactivity, or axonal alteration consistent with what we believe to be a mild impact. Three hours later, another 1-m impact was employed to mimic repetitive mTBI (Fig. 1). During all procedures, basic physiological parameters, including mean blood pressure, body temperature (rectal and temporalis), and blood gases, were monitored continuously and controlled at a constant level. After the repetitive insult, a cranial window was installed and cerebral vascular reactivity to topical ACh administration was evaluated 3 and 4 h after the repetitive mTBI. In each animal, a minimum of four medium-sized (40–60-μm) arterioles were assessed.
Group 2: Repetitive mild traumatic brain injury with mild hypothermia
Animals were exposed to the same repetitive mTBI used in group 1 (Fig. 1) and again, with the exception of the rectal and temporalis temperatures, basic physiological parameters were maintained at constant levels throughout all experimental procedures. One hour after the second/repetitive mTBI, mild hypothermia (35°C) was initiated by placing an ice pack under the animal's body. Rectal and temporalis temperatures were maintained at 35°C for 1 h. As described in a previous report, 34 the rewarming rate was adjusted not to exceed 1°C per 20 min. Cerebral vascular reactivity to ACh in a minimum of four medium-sized (40–60-μm) arterioles was evaluated at the same time points as in group 1.
Group 3: Repetitive mild traumatic brain injury with superoxide dismutase administration
Animals were exposed to the same repetitive mTBI used in group 1 (Fig. 1). Basic physiological parameters were also maintained at constant levels throughout the experiment. One hour after the second/repetitive mTBI, SOD diluted in artificial cerebrospinal fluid (aCSF) at a concentration of 60 U/mL was infused into CSF-containing space underlying cranial window through the same inlet used to monitor intracranial pressure (ICP). In this fashion, the topically applied SOD bathed the cerebral arterioles. The SOD solution was allowed to remain in place for 2 h until the first vascular measurement (3 h after the repetitive mTBI). After measurement at resting state, the SOD solution was washed out and replaced by aCSF containing a predetermined concentration of ACh. Thereafter, SOD was applied again (Fig. 1) and allowed to remain under the cranial window. Then, 1 h later, at the second measurement (4 h after the repetitive mTBI), the SOD was again washed out and replaced by aCSF containing ACh. Pial arteriolar diameters were again measured before and after ACh administration. As in the other groups, four medium-sized (40–60-μm) arterioles were assessed in each animal.
Group 4: Repetitive mild traumatic brain injury with Tempol administration
Animals were exposed to the same repetitive mTBI used in group 1 (Fig. 1). Basic physiological parameters were maintained at constant levels throughout the experimental process. One hour after the repetitive mTBI, Tempol (10 mg/kg) was administered over a 20-min period, through the femoral vein, with careful monitoring of basic physiological parameters. Cerebral vascular reactivity to ACh in four different medium-sized (40–60-μm) arterioles was evaluated at the same time points as in group 1.
General experimental preparation
Repetitive mild traumatic brain injury
The procedure of repetitive mTBI was the same as we have previously reported on for impact acceleration injury. 10,19 Briefly, an incision was made to expose the skull between the coronal and lambdoid suture. After cleaning and drying the bone surface, a 10-mm circular stainless steel helmet was fixed on the mid-line skull between the bregma and lambda with dental acrylic. Animals were placed prone on the foam bed and the head was placed under a 2.5-m Plexiglass tube, with the metallic disc centered under the lower end of the tube. A 450-g brass weight within the tube was dropped from a height of 1 m onto the metallic disc. After impact, rats were quickly removed from the foam bed and placed on a ventilator. A second insult, using the same preparation and 1-m insult, was performed employing the same level 3 h later.
Visualization and assessment of the cerebral vascular reactivity
After completing the repetitive mTBIs, the metal disc was removed. A rectangular 2×4 mm2 craniotomy was made on the left or right side of parietal bone. The underlying dura was cut and removed from the surgical field. Next, a cranial window was placed over the craniotomy, fixed in place with bone wax, and cemented with dental acrylic. As described previously, the window consisted of a cover glass and metallic frame with three outlets that permitted infusion of various agents. Two of the outlets served as in- and outflow paths for perfusion and clearance of the employed vasoactive agents, whereas the free end of the other outlet was set at a predetermined height to maintain an ICP of 5 mmHg. The space under the cranial window was filled with aCSF, with its pH adjusted to approximately 7.35 by equilibration with 6% O2 and 6% CO2 gas mixture balanced with N2. Next, the pial microcirculation was visualized and pial arteriolar diameters were measured using a Vickers image-splitting device (Vickers Instruments, Maiden, MA). As noted previously, in each window preparation, a minimum of four individual arteriolar segments were evaluated. The vasodilator, Ach, was used in two different concentrations to assess vascular responses after topical application through the cranial window. ACh (Sigma-Aldrich, St Louis, MO) is well known to elicit endothelial-dependent vasodilatation. It was dissolved in aCSF to achieve final concentrations of 10−7 and 10−5 mol/L. After topical application of ACh, vessel diameter was measured 2–4 min later. Vascular reactivity to ACh was expressed as a percent change from the baseline diameter at each measurement time.
Tissue preparation
To evaluate the burden of axonal damage after repetitive mTBI, we analyzed the medullospinal junction, which we have previously shown to contain significant axonal injury in this animal model after repetitive 1-m injury. 10,19 At 4 h after the second insult, and after the evaluation of cerebral vascular reactivity, animals were euthanized with sodium pentobarbital (Euthanasia-6; Veterinary Laboratories Inc., Lenexa, KS). Animals were then perfused with 1 L of saline and fixed with 4% paraformaldehyde and 0.1% glutaraldehyde in 0.1 mol/L of Milloning's phosphate buffer. Each brain was divided into cortex and brain stem. The brain stem was sagittally blocked into 4-mm sections containing the corticospinal tract. For tissue sectioning, the brain stem was attached to a metal plate with cyanoacrylate. The brain stem was sagittally sectioned at 40 μm in 0.1 mol/L of phosphate buffer using a vibratome (Leica Biosystems, St. Louis, MO). Sagittal sections were serially collected in alternating wells, with each well containing adjacent sections. Systematic uniform sampling of sagittal sections was initiated from a random starting well, with every third section collected for a total of 20 sections per animal.
Immunocytochemistry for axonal damage
These sections were processed for visualization of antibody targeting the APP, a marker of impaired axonal transport and axonal damage, using a previously reported protocol. 10,19,23,24 In brief, sections were reacted with 0.3% H2O2 in phosphate-buffered saline (PBS) for 30 min to block endogenous peroxidase and microwaved twice in citric acid buffer while maintaining a 45°C maximum temperature for 5 min. Sections were then allowed to cool for 20 min. Sections were preincubated for 1 h in 10% normal goat serum (NGS) with 0.2% Triton X in PBS and then incubated for 18 h with rabbit anti-β-APP (Invitrogen, Carlsbad, CA) diluted to 1:700 in 1% NGS in PBS. Next, the sections were incubated for 1 h with biotinylated goat anti-rabbit immunoglobulin G (Vector Laboratories Inc., Burlingame, CA) diluted to 1:1000 in 1% NGS in PBS. The reaction product was visualized by incubation for 1 h in avidin-biotinylated enzyme complex (Vectastain® ABC kit; Vector Laboratories), followed by 0.05% diaminobenzidene, 0.01% H2O2, and 0.3% imidazole in 0.1 mol/L of sodium phosphate buffer for 15 min. Sections were mounted on 0.5% gelatin-coated glass slides, serially dehydrated, and cover slipped.
Quantitative analysis of the axonal damage
After completion of APP immunocytochemical procedures, slides were transferred in a blinded manner to an Eclipse 800 microscope (Nikon, Tokyo, Japan) and interfaced using a computer-assisted imaging system DP Controller (version 3.2; Olympus Corporation, Tokyo, Japan). Consistent regions of medulla at the medullospinal junction were enlarged to a magnification of 10×and saved as a tagged image file format. Based on our previous experience, the image was viewed on a monitor using the image analysis software, IPLab (version 3.7; BD Biosciences Bioimaging, Rockville, MD), and changed to grayscale. APP-immunoreactive axonal profiles were outlined and overlaid with cyan color to suppress background immunoreactivity. The sampling area in the medullospinal junction was delineated by a rectangle (measuring 500×200 μm2) that was superimposed over the specified region. Within these rectangles, the number of damaged APP-immunoreactive axonal profiles that exceeded 0.968 μm2 in size was then counted. This number is expressed as the density of damaged axons per unit area. For the corticospinal tract, eight alternate serial sections from the same tissue block were analyzed in this fashion, together with the use of investigator blinding.
Statistical analysis
Statistical analysis was performed using the statistical software, PASW Statistics (17.0; SPSS Inc., Chicago, IL). All data are presented as mean±standard error of the mean. All values were tested for distribution normality using Kolmogorov-Smirnov's test. Physiological parameters and laboratory data, which were normally distributed, were analyzed by one-way analysis of variance. When a significant difference was found, differences among time points in the same group and among groups at each time point were determined by using Bonferroni's correction and Tukey's test, respectively. The data of vascular reactivity to ACh and axonal injury were analyzed by Kruskal-Wallis' test because these data were not normally distributed, and post-hoc multiple comparisons were made by Mann-Whitney's U test and Bonferroni's correction. A value of p<0.05 was considered to be statistically significant.
Results
General physiological findings
A total of 20 rats were included in this study. There were no significant differences in baseline body weight and hematocrit between groups. Table 1 shows time-course measurements of mean arterial pressure (MAP) and blood-gas analysis. There were no significant differences in these physiological parameters, including MAP, PaO2, PaCO2, and pH value at each measurement time, with the exception of the MAP at 1 and 6 h after the first insult (group 1 vs. group 4, p=0.042; group 2 vs. group 4, p=0.033, respectively), although the blood pressure for each group was not below autoregulatory levels. Because a tendency for a decrease in PaO2 value over time was observed, we employed oxygen supplementation midway in the experimental series. Although the values of PaO2 appeared relatively lower, no statistical difference was found for the PaO2 at any time point or experimental group. Rectal temperature was maintained at approximately 37°C throughout the experiment, except during the use of therapeutic hypothermia (Fig. 2). During induction of therapeutic hypothermia, rectal and temporalis temperatures dropped quickly (within 10–20 min) to reach 35°C in group 2. Rewarming rates in hypothermia groups were approximated 1°C/20 min.
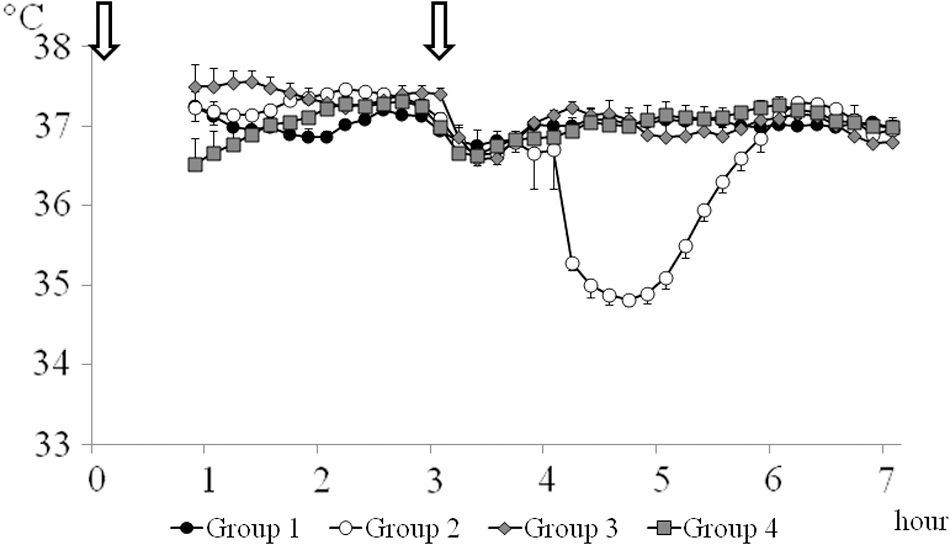
This figure illustrates changes of mean rectal temperatures throughout the duration of the study. A parallel temperature response was observed with the use of a temporalis muscle probe, with the caveat that this temperature slightly trailed the rectal temperature by approximately 0.5°C. Rectal temperature in group 2 was decreased quickly and maintained at 35°C for 1 h. Rewarming was performed gradually and temperature achieved the targeted range 1 h later. Arrow indicates the time of each insult. Data points represent 10-min intervals. Timeline represents the time course after the first insult. Values are expressed as mean±standard error of the mean.
Values are expressed as the mean±standard error of the mean.
Significant difference at p<0.05 versus group 4 (one-way analysis of variance).
MAP, mean arterial pressure; PaCO2, partial arterial oxygen pressure; PaCO2, partial arterial carbon dioxide pressure.
Effect of mild hypothermia on cerebral vascular responsiveness after repetitive mild traumatic brain injury
Mean baseline vascular diameter was not significantly different between groups 1 and 2 (44±3 vs. 42±2 μm and 45±3 vs. 50±3 μm at 3 and 4 h after the repetitive mTBI, respectively). Cerebral vascular responses to different concentration of ACh (10−7 and 10−5 M) were evaluated at 3 and 4 h after the repetitive mTBI (Fig. 3). Response to ACh was expressed as the percent change from the baseline diameter after ACh exposure. Consistent with previous reports, cerebral vascular responses to ACh in group 1 were completely suppressed at both ACh concentrations and at both measurement time points (10−7 M ACh, −0.4±0.7% and 0.1±0.6% at 3 and 4 h after the repetitive mTBI, respectively; 10−5 M ACh, 1.3±1.1% and 1.1±1.0% at 3 and 4 h after the repetitive mTBI, respectively). In group 2, after use of hypothermia, rectal temperatures returned to normal levels at both measurement time points (Fig. 2; 37.1±0.1 and 37.0±0.1°C, respectively). In this hypothermic-treated group, the percent increase in cerebral vascular diameters was significantly higher than in group 1 at both ACh concentrations and at both measurement time points (10−7 M ACh, 7.9±1.0% and 5.1±1.0% at 3 and 4 h after the repetitive mTBI, respectively, P<0.001; 10−5 M ACh, 12.5±1.8% and 11.7±1.7% at 3 and 4 h after the repetitive mTBI, respectively, P<0.001).
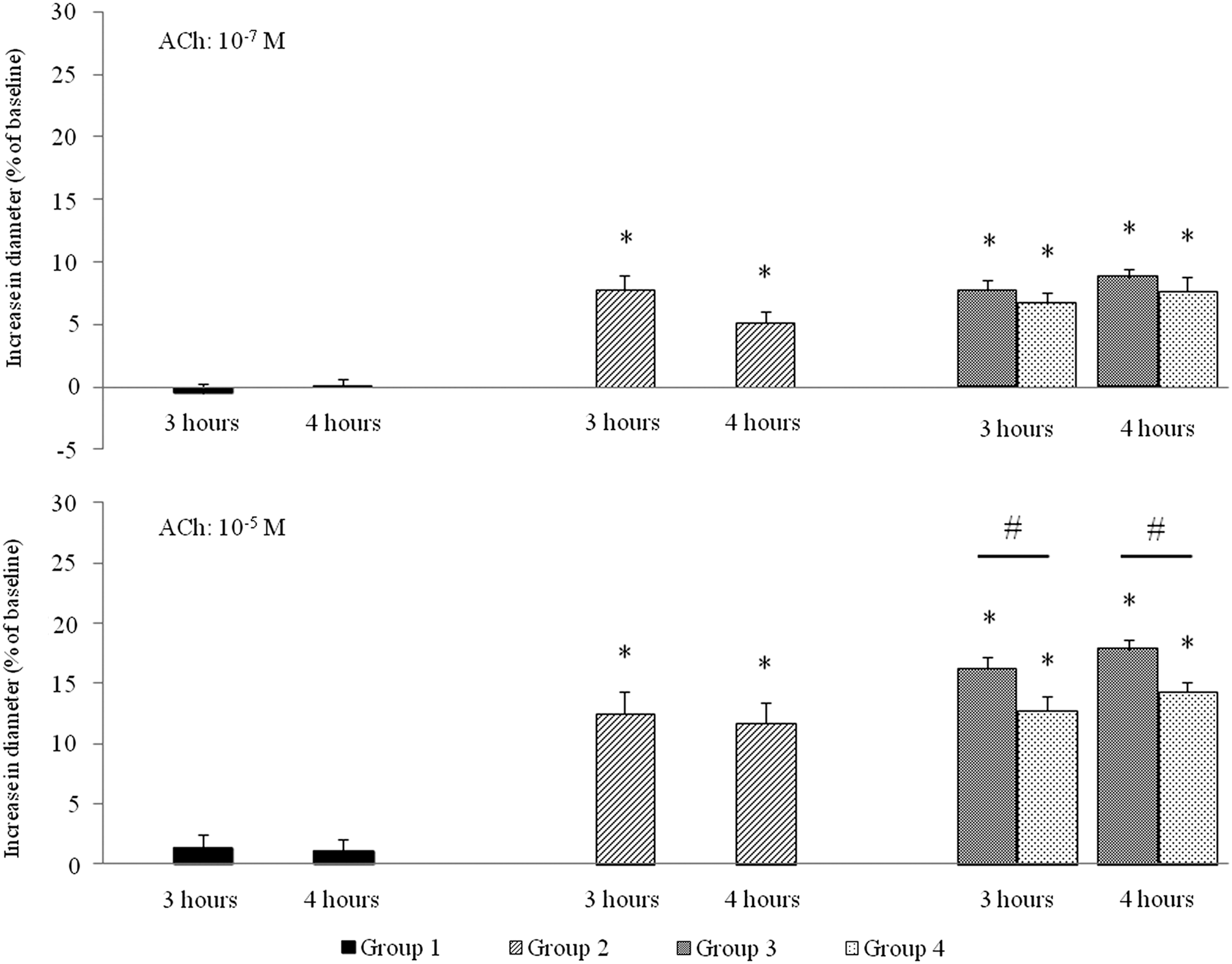
These bar graphs show cerebral vascular reactivity to 10−7 and 10−5 M ACh 3 and 4 h after repetitive mTBI. Bars express percent changes from baseline cerebral vascular diameter after exposure to ACh in each measurement time point. In group 1, cerebral vascular responses were significantly suppressed at all measurement points (left panel). In group 2, cerebral vascular responses were significantly higher than in group 1 in all measurement points (center panel). In groups 3 and 4, cerebral vascular responses were also significantly higher than group 1 in all measurement points (right panel). Vascular responses to 10−5 M ACh at 3 and 4 h after the repetitive mTBI in group 3 were significantly higher than group 4. All values are expressed as mean±standard error of the mean. Statistical difference was analyzed by Kruskal-Wallis' test followed by Bonferroni's test for multiple comparisons. *Significant difference at p<0.001 versus group 1; #significant difference at p<0.05. ACh, acetylcholine.
Effect of superoxide dismutase and Tempol on cerebral vascular responsiveness after repetitive mild traumatic brain injury
Mean baseline vascular diameter was not significantly different between groups 3 and 4 (47±2 vs. 43±1 μm and 48±2 vs. 42±2 μm at 3 and 4 h after the repetitive mTBI, respectively). Compared to group 1, cerebral vascular responses to both concentrations of ACh were significantly preserved in groups 3 and 4 (Fig. 3), demonstrating that SOD and Tempol exerted vascular protective effects (SOD: 10−7 M ACh, 7.7±0.8% and 8.8±0.6% at 3 and 4 h after the repetitive mTBI, respectively, P<0.001; 10−5 M ACh, 16.3±0.9% and 17.9±0.8% at 3 and 4 h after the repetitive mTBI, respectively, P<0.001; Tempol: 10−7 M ACh, 6.7±0.9% and 7.7±1.1% at 3 and 4 h after the repetitive mTBI, respectively, P<0.001; 10−5 M ACh, 12.7±1.2% and 14.3±0.8% at 3 and 4 h after the repetitive mTBI, respectively, P<0.001). Whereas there was a trend that vascular response was more preserved in group 3 than group 4 after 10−7 M ACh stimulation, there was no statistically significant difference between these groups. However, significantly better response in vascular responsivity was demonstrated in group 3 vs. group 4 after 10−5 M ACh stimulation (3 and 4 h after the repetitive mTBI, P=0.021 and 0.014, respectively; Fig. 3).
Evaluation of axonal injury after repetitive mild traumatic brain injury
Figure 4 shows representative findings of the medullospinal junction in each group. There were many APP-positive axons in group 1, showing axonal truncation and edema, whereas in the other groups, decreased numbers of axonal injuries were observed. Figure 5 shows the result of quantitative analysis of damaged axon in each group. Consistent with our previous reports, 10,19 repetitive mTBI caused significant axonal injury reflected in the appearance of numerous APP-positive axons in group 1 (182±25/mm2). In group 2, the number of APP-positive axons was significantly lower than group 1 (27±5.1/mm2; p<0.001). The antioxidant agents, SOD (group 3) and Tempol (group 4), also significantly reduced the APP-positive axons, in comparison to group 1 (54±13/mm2 and 50±14/mm2, respectively; P<0.001). There were no significant differences in axonal protection observed between group 3 versus group 4.
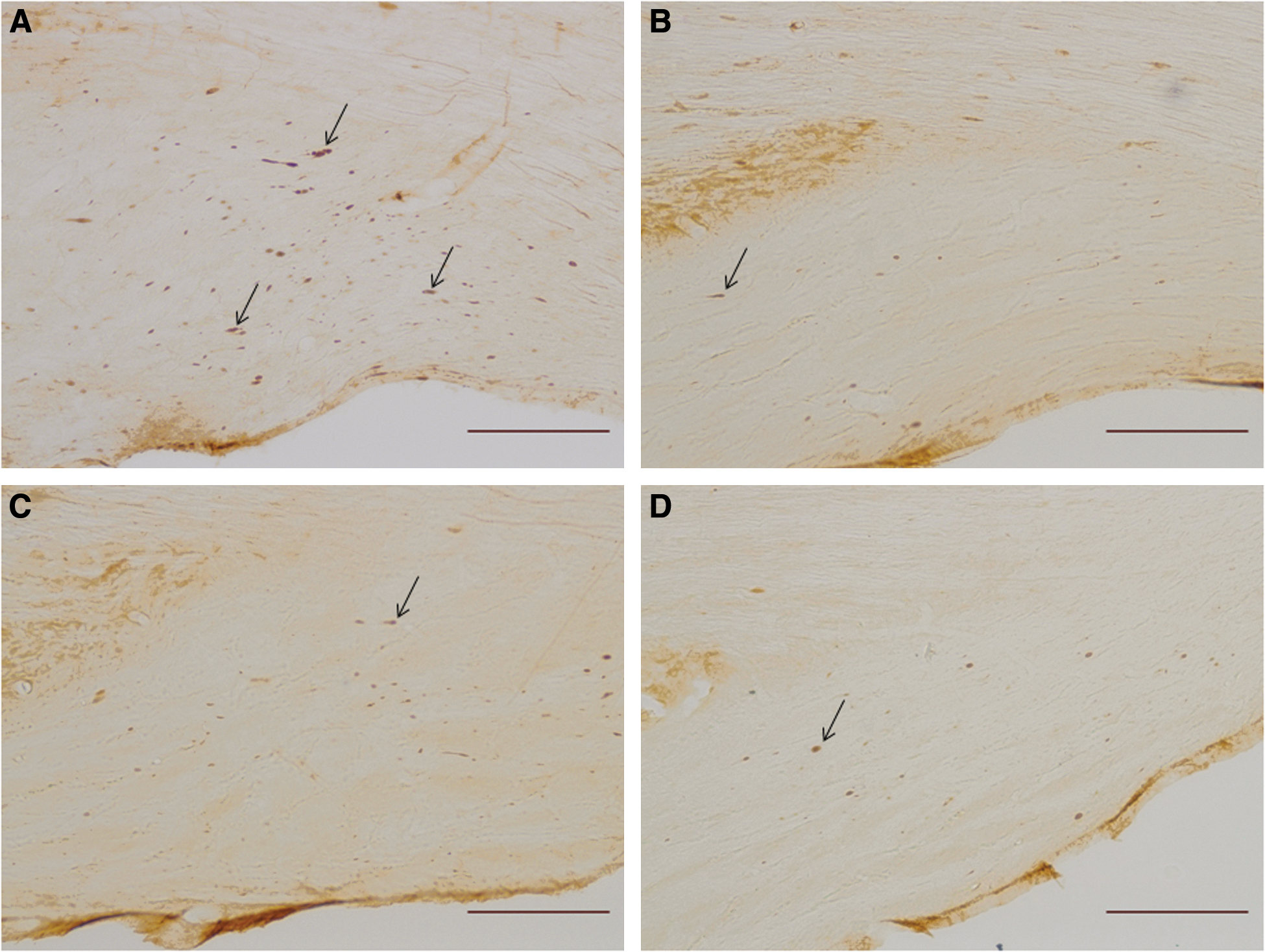
Representative micrographs of medullospinal junction in each group. Brain stem was obtained 4 h after repetitive mTBI. Bulb-shaped black dots (arrows) are amyloid precursor protein (APP)-positive axons, suggesting significant axonal damage and disconnection. Significantly increased APP-positive axons can be observed in group 1 (
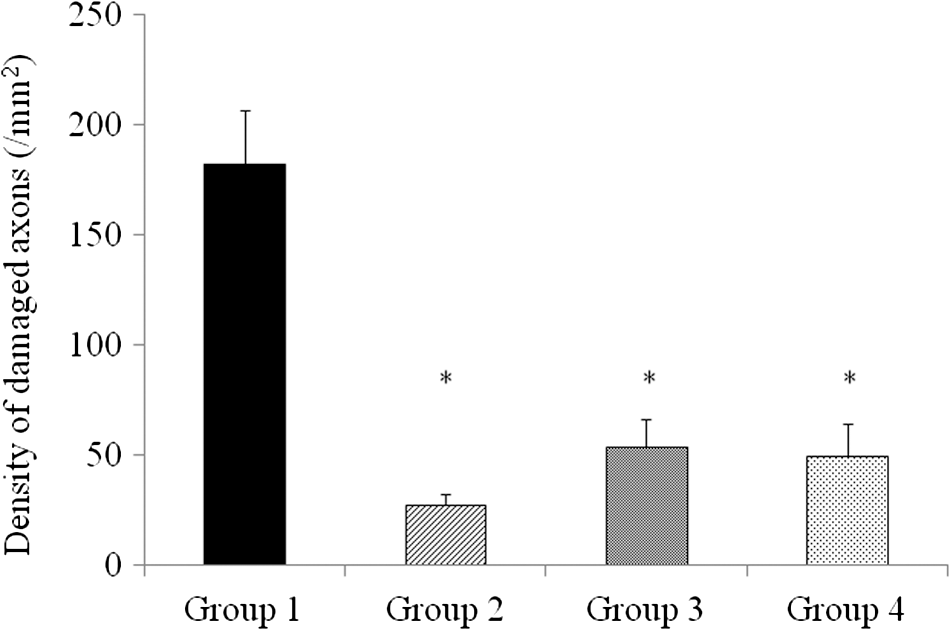
This bar graph shows mean density of APP-immunoreactive damaged axon in the medullospinal tract at 4 h after repetitive mTBI. Significantly increased APP density was observed in group 1. Whereas APP density in groups 2, 3, and 4 were significantly lower than that in group 1, there were no significant differences between therapeutic intervention groups (groups 2, 3, and 4). All values represent the mean±standard error of the mean. Statistical differences were analyzed by the Kruskal-Wallis' test, followed by Bonferroni's test for multiple comparisons. *Significant difference at p<0.001.
Discussion
The results of the current communication both confirm and extend previous observations from our lab as well as others that show that repetitive mild injuries, when administered within a specific temporal framework, can result in an exacerbated burden of both microvascular and axonal damage and dysfunction. 2,4,6 –8,10,19 Equally important, the current studies also extend and confirm previous findings from our lab that the damaging consequences of repetitive mTBI can be dramatically attenuated through the delayed postrepetitive injury use of either mild hypothermia or the oxygen radical scavengers, SOD or Tempol. 22,23 Accordingly, the current communication continues to extend our understanding of the complex pathobiology of repetitive mTBI and its possible therapeutic targeting.
In the current communication, the observation that the use of even mild (35°C) hypothermia exerts significant axonal and vascular protection was an unanticipated observation, given its relatively dramatic suppression of both repetitive injury-induced axonal and microvascular damage and dysfunction. Though the possible mechanisms associated with this mild hypothermia-induced axonal and vascular protection remain unclear, it is most likely that its benefits derive from subtle reductions in brain metabolism and/or oxygen radical production capable of evoking both axonal and microvascular change. 35 –39 Some previous articles that demonstrated reduction of neuronal oxidative damage by induction of mild hypothermia (33–35°C) in TBI, intracerebral hemorrhage, and hypoxic ischemia support our opinion. 40 –42 Whereas it is relatively remarkable that a 2°C temperature drop, which would result in a 14% reduction in brain metabolism, 38 could be capable of effecting such protection, our observation suggests that this is the case and, as such, that the use of mild hypothermia may ultimately prove a rational choice in patients showing adverse consequences of secondary or repetitive injury, particularly those patients manifesting rapid deterioration in second impact syndrome. Though in the context of human TBI, moderate hypothermia in the range of 32–33°C has been used clinically to exert purported neuroprotection, it is important to note that such hypothermic levels can be associated with cardiogenic arrhythmias, 43 –45 plasma and intracellular ionic imbalances, 44 and/or increased susceptibility to infection, 46 all of which increase the risk associated with the use of moderate hypothermia, continuing to blunt clinical enthusiasm for its routine consideration. In this context, the efficacy here demonstrated with the use of mild hypothermia, which is not associated with the above-identified clinical risks, may be a rational strategy for those showing dramatically increased morbidity after repetitive mTBI, particularly those in that unique subpopulation of patients transitioning to the devastating consequences of a second impact syndrome associated with vascular engorgement and rapid neurological deterioration. 47 –49 Whereas, obviously, this issue will mandate detailed clinical investigation, the provocative results in the current communication suggest that this issue merits further study.
Equally important to the observation that mild hypothermia provides axonal and microvascular protection when administered after repetitive mTBI was the observation that both SOD and Tempol provided comparable protection when also administered after repetitive insult. These findings are consistent with the observation that SOD and/or Tempol can exert either microvascular or axonal protection after a singular/nonrepetitive brain injury. 22 Importantly, because their efficacy is observed after repetitive injury, it would suggest that delayed, repetitive injury is capable of eliciting a burst of radial-mediated damage, causing the observed axonal damage as well as the parallel observation of microvascular dysfunction. Clearly, the utility of SOD suggests the involvement of the superoxide anion, whereas the benefit of Tempol is not only consistent with its ability to quench the superoxide anion, but also its ability to quench peroxynitrite-derived free radicals, which could be involved in both the observed axonal structural and vascular functional change. 10,31 As noted, what is of interest here is that although both radical species have been associated with uncomplicated mTBI, these findings unequivocally link their generation to the damaging consequence of repetitive brain injury and thus make them appropriate therapeutic targets. Though the efficacy of both SOD and/or Tempol cannot be disputed after repetitive mTBI, it was somewhat unexpected that topical application of SOD after repetitive mTBI could also exert somewhat remote axonal protection. Though, admittedly, this finding was unanticipated, the observation of both local vascular and remote axonal protection could be related to the relatively long period of time over which the SOD remained in place in the CSF bathing the injured brain, together with its potential to readily diffuse into the basal cisterns where it could have ready access to the descending corticospinal tracts. Obviously, this premise will further additional tracer-linked studies, yet, at the moment, this explanation appears entirely reasonable.
In sum, the present study continues to confirm the damaging consequences of repetitive brain injury while suggesting that some of its damaging consequences can be targeted with relatively innocuous therapeutic approaches that include mild hypothermia and/or use of radical scavengers, such as SOD. It is hoped that, with further preclinical studies, these strategies can be moved to the clinical setting.
Footnotes
Acknowledgments
The authors thank Ms. Lynn Davis and Mrs. Susan Walker for their technical assistance. This study was supported by National Institutes of Health grants NS077657 and NS047463.
Author Disclosure Statement
No competing financial interests exist.