
Abstract
Inflammation of the spinal cord after traumatic spinal cord injury (SCI) leads to destruction of healthy tissue. This “secondary degeneration” is more damaging than the initial physical damage and is the major contributor to permanent loss of functions. In our previous study, we showed that combined delivery of two growth factors, vascular endothelial growth factor and platelet-derived growth factor, significantly reduced secondary degeneration after hemisection injury of the spinal cord in the rat. Growth factor treatment reduced the size of the lesion cavity at 30 days, compared to control animals, and further reduced the cavity at 90 days in treated animals, whereas in control animals the lesion cavity continued to increase in size. Growth factor treatment also reduced astrogliosis and reduced macroglia/macrophage activation around the injury site. Treatment with individual growth factors alone had similar effects to control treatments. The present study investigated whether growth factor treatment would improve locomotor behavior after spinal contusion injury, a more relevant pre-clinical model of SCI. The growth factors were delivered for the first 7 days to the injury site by osmotic minipump. Locomotor behavior was monitored at 1–28 days after injury using the Basso, Beattie and Bresnahan (BBB) score and at 30 days using automated gait analysis. Treated animals had BBB scores of 18; control animals scored 10. Treated animals had significantly reduced lesion cavities and reduced macroglia/macrophage activation around the injury site. We conclude that growth factor treatment preserved spinal cord tissues after contusion injury, thereby allowing functional recovery. This treatment has the potential to significantly reduce the severity of human spinal cord injuries.
Introduction
M
We recently reported significantly reduced secondary degeneration after spinal cord lateral hemisection in the rat with a combination of vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF). 2 This combined growth factor treatment significantly reduced the size of the lesion cavity at 30 and 90 days postinjury and eliminated the expansion in cavity size observed over this period in control animals. Treatment with either growth factor alone was deleterious; individually, both growth factors increased the lesion cavity size at 30 days, compared to controls. 2 Combined growth factor treatment was most effective when infused at the injury site continuously for 7 days from the time of injury. The cellular mechanisms of this combined growth factor treatment are unknown, but histological analysis of the spinal cords at 30 days revealed significant reductions in astrogliosis and in microglia/macrophage activation surrounding the lesion cavity. 2 These observations indicate that the growth factors intervene in the early inflammatory events after spinal cord injury (SCI). Consistent with this conclusion are observations that similar reductions in gliosis were observed with combined growth factor treatment of a stab injury in the brain. 3 The aim of the present study was to investigate whether combined growth factor treatment is able to improve locomotion after a thoracic contusion injury of the spinal cord. Our hypothesis is that the growth factors, by intervening early in the inflammatory process and preserving spinal cord tissue, will also preserve locomotor function.
Methods
Overview of experiment
Animals were subjected to contusion injury with treatment for 7 days (control, 0.09% saline; treated, VEGF+PDGF) commencing at the time of injury. At 28 days, animals were tested for their locomotor behavior (Basso, Beattie and Bresnahan [BBB] score and automated footprint analysis). At 30 days, animals were killed for histological analysis of the spinal cord to assess the effect of treatment on lesion size and macrophage/microglia. The experiments were conducted in two independent cohorts of 6 animals per group (control and treated), for a total of 12 animals per group.
Animals
Adult female Wistar rats (study 1: n=12, 300 g, 20–25 weeks; study 2: n=12, 210–270 g, 12–16 weeks) were anesthetized with 5% isofluorane (Forthane; Abbot Laboratories, Abbot Park, IL) in oxygen. All procedures were approved by the animal ethics committees of the Queensland University of Technology (Brisbane QLD, Australia) and Griffith University (Brisbane QLD, Australia), according to the guidelines of the National Health and Medical Research Council of Australia.
Spinal cord contusion injury and microinfusion surgery
Animals were anesthetized with 5% isofluorane (Forthane; Abbot Laboratories) in oxygen. Complete laminectomy was made at T10 for the site of injury. After laminectomy, spinal cords were exposed surgically by careful dissection and parting of the meninges. Contusion injury was induced at this site using the Infinite Horizons Impactor (Precision Systems and Instrumentation, Lexington, KY) with a force of 150 kdyne. 4 The Infinite Horizons Impactor is validated for histological and behavioral recovery for the month after injury. 4,5 The impactor was set up to have no dwell time; the tip was removed from the surface of the spinal cord immediately after impact. The force and dynamics of the impactor were measured by the instrument. The measured impact force (kilodynes) delivered to the two groups was (mean±standard error of the mean [SEM], range): control, 158+1.1, 6; treated 155±2.0, 13. The measured impactor displacement (mm) delivered to the two groups was (mean±SEM, range): control, 1264+74, 365; treated 1314±68, 388. The measured impact velocity (mm/sec) delivered to the two groups was (mean±SEM, range): control, 124+1.3, 7; treated 121±1.0, 7. All impacts were within expected limits, and no animals were excluded on the basis of force and dynamics measurements. The growth factor treatments were then applied by an osmotic minipump through a catheter whose tip was placed adjacent to the site of injury, effectively bathing the dorsal surface of the spinal cord. The miniosmotic pump (Alzet model 2001; 1 μL/h for 7 days; DURECT Corporation, Cupertino, CA) was weighed before loading and then filled with 15 μg of VEGF (catalog no.: PMG0041; Life Technologies, Invitrogen, Carlsbad, CA) and 15 μg PDGF-BB (catalog no.: PHC9391; Life Technologies, Invitrogen) dissolved in 168 μL of phosphate-buffered saline (PBS), using a blunt-tipped 27-gauge filling tube provided by the manufacturer. The filled pump was weighed, and the net weight of the growth factor solution loaded was recorded. A catheter (Rat Intrathecal Catheter, 15 cm, Alzet; DURECT Corporation) was then connected to the pump, which was primed with 0.9% sterile saline solution at 37°C overnight before the pump was implanted. An additional laminectomy was performed at T12, and the catheter was passed under the T11 lamina. The tip of the catheter was carefully placed on top of the lesion and sutured to the muscle to keep it in place. Animals were then randomly assigned to treatment groups (control, saline vehicle only, n=12; treated, VEGF and PDGF, n=12), with the surgeons blinded to treatment. Miniosmotic pumps were implanted in a subcutaneous pouch over the right flank. The laminectomies were covered by suturing muscle and skin layers above them. The deep and superficial muscles were sutured, and animals were given prophylactic cephalothin and buprenorphine. Animals received manual bowel and bladder expression twice-daily until they recovered.
Locomotor behavior
Open-field locomotor behavior was scored according to the BBB scale. 6 Animals were scored at 1, 7, 14, 21, and 28 days after injury. To avoid observer bias, animals were filmed at high resolution with a hand-held camera at a range of focal distances and relative positions, including close-ups on both sides, in order to record joint movements, posture, and weight bearing. The BBB score was then scored independently by two observers who were blind to the treatment group. The average scores of the two observers are presented as the assessed BBB score.
Automated footprint analysis of gait parameters was quantified using motorized treadmill system and analysis software (Digigait). This analysis uses a video camera mounted beneath a transparent treadmill to record the paw placement of the animal when put through a forced gait cycle. Algorithms in the software automatically digitize the ventral view of the rat and identify the individual footprints on the treadmill. The resultant images are used to define the contact area of each paw during walking to generate a set of periodic waveforms that describe the advance and retreat of the four limbs, including stride length, stepping frequency, and stance width. From these, the percentage of time spent in stand, stride, and swing phases were calculated as well as hindlimb stance width. Thoracic spinal cord injury leads to an unstable gait with an increased hindlimb stance width (hindlimb base of support). 7,8 These gait parameters were quantified for the first cohort of 6 animals per group 30 days after injury. An equal number of steps was analyzed per group so as not to bias the data toward any individual.
Tissue preparation and immunofluorescence histology
Thirty days after the injury, animals were killed with an injection of 1.5 mL of sodium pentobarbital (60 mg/kg, intraperitoneally) and perfused transcardially with 200 mL of PBS, followed by 200 mL of Zamboni's fixative solution (pH 7.2). The spinal cord in the region of the lesion was dissected out and postfixed in Zamboni's solution overnight at 4°C. The spinal cord was then dehydrated serially in 50%, 70%, and 100% ethanol solutions (1 h each) and embedded in polyethylene glycol, after which 40-μm sections were cut with a Leica RM2255 rotary microtome (Leica Microsystems GmbH, Wetzlar, Germany).
Sections from the mid-line area of the lesion site were selected by the presence of the central canal as well as by measurement of half thickness of the tissue specimen at the injury level. Sections were washed with 0.1% Triton X-100 in PBS for 10 min, permeabilized in dimethyl sulfoxide for 20 min, washed three times in PBS-Triton for 15 min, and then blocked with 10% donkey serum (Sigma-Aldrich, St. Louis, MO) 0.1% Triton X-100 in PBS for 1 h. The sections were incubated with the following antibodies (Abs) overnight at room temperature in the same blocking solution: anti-Neurofilament-200 (mouse monoclonal Ab, 1:400; Chemicon, Temecula, CA), anti–glial fibrillary acidic protein (GFAP; rabbit polyclonal Ab, 1:1000; Dako North America, Inc., Carpenteria, CA). To study macrophages/microglia, sections from an area with the largest lesion cavity were chosen and immunostained for anti–ionized calcium binding adaptor molecule 1 (IBA-1; rabbit polyclonal Ab, 1:2000; Wako Chemicals USA, Inc., Richmond, VA). Sections were then washed three times in PBS-Triton and incubated with the Alexa Fluor 594–labeled donkey anti-mouse or Alexa Fluor 488–labeled donkey anti-rabbit secondary Abs (Molecular Probes, Eugene, OR) for 3 h at room temperature. Sections were washed three times in PBS-Triton and mounted with Vectorshield mounting media with 4′,6-diamidino-2-phenylindole (Vector Laboratories, Burlingame, CA).
Mounted sections were analyzed on a Zeiss Z1 microscope with ApoTome with a digital image capture (Carl Zeiss GmbH, Jena, Germany), which was used to outline and measure the lesion cavity. For quantification of the IBA-1-positive macrophages/microglia, Z-stack images (20×objective) were taken at a distance of 200 μm from the edge of the GFAP-defined lesion (n=4 fields per animal, 5 animals per group, 1152 cells in total). In each field, the total number of IBA-1-immunopositive cells was counted and the morphologies of the IBA-1-immunopositive cells were classified based on the largest cell body cross-section area into three categories: resting, a cell body cross-sectional area of 20–30 μm2; primed/activated, cell body cross-sectional area of 30–150 μm2; and phagocytic, cell body cross-sectional area greater than 150 μm2. The percentage of IBA-1-positive cells in each of the three subclasses was calculated for each animal.
Statistical analysis
The experiments were carried out in two independent studies of 12 animals each, and the BBB locomotor scores from these studies were combined. The first study also included automated footprint analysis and lesion cavity measurement. The second study also included quantification of the IBA-1-immunoreactive cells in the lesioned spinal cord. All data are presented as mean±SEM. Analysis of variance (ANOVA) and post-hoc multiple comparisons tests were performed using GraphPad Prism software (v6; GraphPad Software Inc., La Jolla, CA).
Results
Vascular endothelial growth factor plus platelet-derived growth factor improved locomotor behavior after injury
Locomotor behavior was assessed using the BBB score at 1, 7, 14, 21, and 28 days after injury and treatment. Beginning at 7 days, the behavior of the VEGF+PDGF treatment group diverged from the control group, reaching a higher maximal score at 21 days (Fig. 1). Two-way ANOVA indicated significant effects of treatment (F 1,92=18.25; p<0.0001) and time (F 4,92=17.91; p<0.0001). Post-hoc Sidak's multiple comparisons tests indicated significant differences in BBB scores between the treatment groups at 21 and 28 days (p<0.05). The early recovery of locomotion indicates that the treatment may be neuroprotective during the first days after injury. Treatment appeared to advance, by 7 days, the time course of recovery observed in controls (compare the treated and control BBB scores at 7 and 14 days, respectively; Fig. 1). The combination of these factors brings the BBB score to 18. In contrast, controls recovered only to a BBB score of 11 after receiving the same contusion injury.
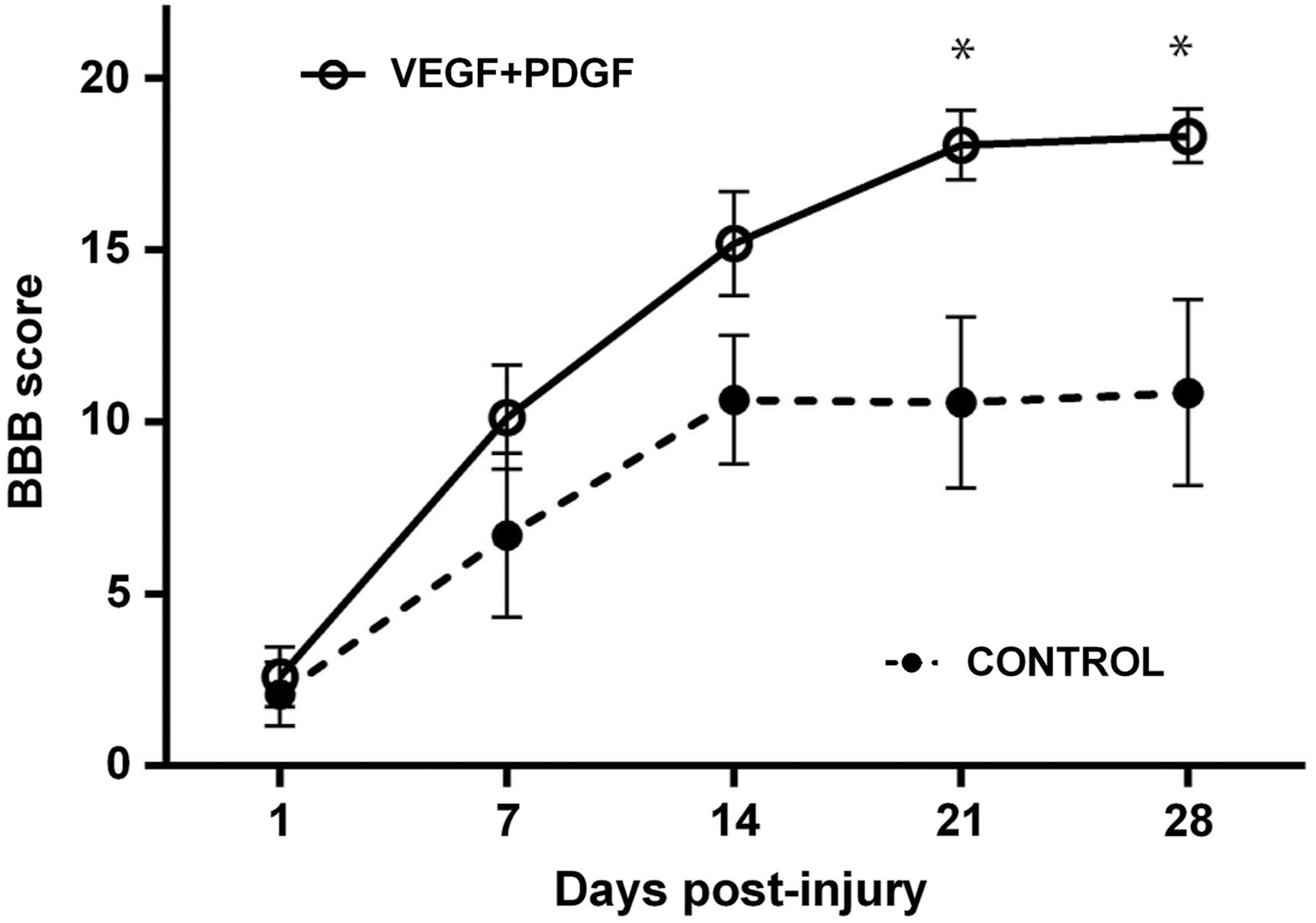
VEGF+PDGF treatment improved hindlimb motor function after spinal cord contusion. Locomotor behavior was assessed using the BBB scale. VEGF+PDGF treatment significantly improved BBB score (analysis of variance, p<0.0001) with the BBB scores significantly different between the groups at 21 and 28 days (*p<0.05). All data are mean±standard error of the mean. BBB, Basso, Beattie and Bresnahan; VEGF, vascular endothelial growth factor; PDGF, platelet-derived growth factor.
Automated footprint analysis at 30 days postinjury revealed that control animals showed impairments in several gait parameters, which were restored toward prelesion levels by VEGF+PDGF treatment (Fig. 2). ANOVA indicates significant effect of treatment on hindlimb base of support (F 2,1342=7.108; p=0.0009) with post-hoc Tukey's multiple comparisons test, indicating that untreated controls were significantly different from prelesion measurements (p<0.01) and treated animals (p<0.01). There was no difference between treated animals and prelesion levels (Fig. 2A). ANOVA indicates significant effect of treatment on percent of time in stride phase (F 2,946=30.78; p=0.0001) with post-hoc Tukey's multiple comparisons test, indicating that untreated controls were significantly different from prelesion measurements (p<0.0001) and treated animals (p<0.0001). There was no difference between treated animals and prelesion levels (Fig. 2C). ANOVA indicates significant effect of treatment on percent of time in stand phase (F 2,946=18.24; p=0.0001) with post-hoc Tukey's multiple comparisons test, indicating that untreated controls were significantly different from prelesion levels (p<0.0001), but not treated animals. There remained a small difference between treated animals and prelesion levels (p<0.05; Fig. 2B). ANOVA indicates significant effect of treatment on percent of time in swing phase (F 2,946=23.81; p=0.0001) with post-hoc Tukey's multiple comparisons test, indicating that untreated controls were significantly different from prelesion measurements (p<0.001) and treated animals (p<0.0001). Treated animals recovered past prelesion levels (p<0.0001; Fig. 2D).

VEGF+PDGF treatment improved hindlimb gait after spinal cord contusion. Locomotor behavior was assessed using a motorized treadmill. (
Vascular endothelial growth factor plus platelet-derived growth factor treatment reduced lesion size
At 30 days, there were significant differences in lesion sizes in treated and control animals (Fig. 3). The size of the lesion cavity was quantified at its widest point in mid-cord, using the boundaries of NF200 and GFAP immunoreactivity, as previously described. 2 Lesion cavity size measured by GFAP immunoreactivity in control animals was significantly larger that in treated animals (control: 0.84±0.10 mm2, n=5; treated: 0.11±0.03 mm2, n=5; t=7.019, df=4.919, p<0.001; Fig. 3A,B,E). Lesion cavity size measured by NF200 immunoreactivity in control animals was significantly larger that in treated animals (control: 0.60±0.07 mm2, n=5; treated: 0.06±0.02 mm2, n=5; t=7.417, df=4.556, p=0.001; Fig. 3C,D,F).

VEGF+PDGF treatment reduced lesion cavity size after spinal cord contusion injury. (
Vascular endothelial growth factor plus platelet-derived growth factor treatment modulated macrophage/microglia response to injury
At 30 days, there were significant differences in the proportions of IBA-1-positive macrophages/microglia classified by cell body size into resting, active, and phagocytic stages. In control spinal cords, most of the IBA-1-positive cells had small cell bodies with ramified dendritic processes (Fig. 4A). In treated spinal cords, the predominant impression is of large globular cells without cellular extensions (Fig. 4B). Growth factor treatment shifted the proportion of cells from the active to the phagocytic classification (Fig. 4C). ANOVA on the proportions of cells in the different classes indicated significant differences between cell categories (F 2,24=3988; p<0.001) and a significant interaction between treatment and cell category (F 2,24=787.2; p<0.0001), with post-hoc Sidak's multiple comparisons test indicating that controls and treated animals differed significantly in the proportions of active and phagocytic cell categories (Fig. 4C; p<0.001).
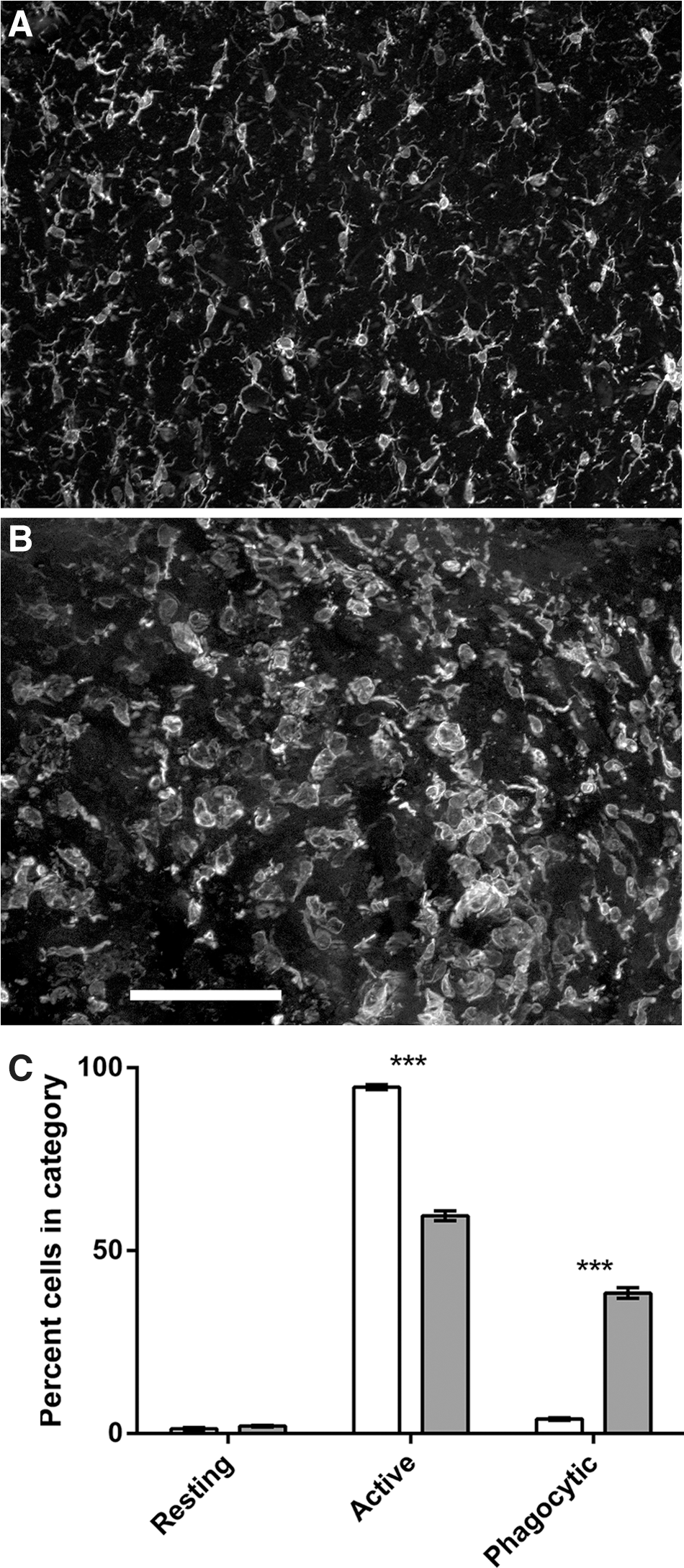
VEGF+PDGF treatment altered the inflammatory cell population after spinal cord contusion injury. (
Discussion
We show here that infusion with a combination of VEGF and PDGF for 7 days after thoracic spinal cord contusion significantly improved locomotor behavior indicated by weekly BBB scores and automated footprint analysis at 30 days. After injury, locomotor behavior of treated animals began improving more quickly than control animals, with differences beginning to emerge after a week. In the spinal cord at 30 days postinjury, lesion cavity size in treated animals was significantly smaller than in control animals, assessed by the boundary of the glial scar (GFAP immunoreactivity) and the boundary defined by axons (neurofilament immunoreactivity). VEGF and PDGF treatment in the contused spinal cord changed the morphologies of IBA-1 inflammatory cells to reduce the proportion of activated microglia/macrophages and increase the proportion of postphagocytic cells. A similar observation was made with the same treatment after a hemisection injury. 2 These observations support our hypothesis that growth factor treatment intervenes early in the inflammatory process to preserve spinal cord tissue and preserve locomotor function.
The behavioral and histological effects of combined treatment with VEGF and PDGF are large, compared to the neuroprotection afforded by other treatments for SCI in the rat, including with several already in human clinical trials. 9,10 This treatment has potential for translation to humans because it could theoretically be delivered to humans after SCI, for example, by implantation of an infusion pump at the time of decompression surgery, 11 but it needs to be optimized. For example, a 7-day treatment period was used here because it was effective previously, 2 but a shorter treatment period may be optimal because growth factors delivered in a hydrogel patch reduced lesion size, even though they were likely available for only 24–48 h. 2 That suggests that, in terms of cellular mechanism, the treatment may act on the earliest stages of inflammation, such as the influx of neutrophils that occurs initially and peaks at approximately 1–2 days. 12 –14 In this respect, it is interesting to note that the BBB scores of the treated and control groups begin to diverge in the first week, indicative of a very early influence on the cellular mechanisms of inflammation.
The identities of the cells upon which VEGF and PDGF act are not known. None of the cells present has receptors for both growth factors. For example, after vascular damage, platelets promote the recruitment and extravasation of neutrophils, 15,16 but they do not have the PDGF receptor (PDGFRβ) for PDGF-BB, the dimer used in the present study, nor would neutrophils, which lack PDGF receptors. 17 On the other hand, after SCI, PDGF-BB stimulates astrocytes to induce monocyte extravasation by releasing monocyte chemoattractant protein 1. 18 Platelets and activated neutrophils have VEGF receptors, 19,20 and VEGF promotes monocyte extravasation. 21 Our working hypothesis is that PDGF-BB acts through astrocytes, whereas VEGF acts through platelets, neutrophils, and monocytes after SCI. Although the cellular and mechanisms through which they work are undetermined, the comparatively large neuroprotective effects of VEGF and PDGF indicates that further exploration of this treatment is warranted.
Footnotes
Acknowledgment
The work was supported by a grant to A.M.S. from the Australian Department of Health and Aging.
Author Disclosure Statement
No competing financial interests exist.