
Abstract
The aim of this study was to examine the rate and causes of mortality following mild to severe traumatic brain injury (TBI) rehabilitation and to develop a multivariate prognostic model of mortality. We conducted a cohort study of 3341 individuals with mild to severe TBI followed-up from a post-acute inpatient rehabilitation center. Rate of death and survival between one and 26 years following injury were examined using standardized mortality ratios (SMRs) and prognostic models developed using Cox regression. A mortality rate of 9.3% was observed and an overall SMR of 1.04 (95% confidence interval [CI]=1.04–1.05). A statistically significant elevated SMR of 1.20 (95% CI=1.06–1.37) was observed for males, and both males and females had an elevated risk of death from external causes. Females also were found to have a significantly elevated SMR of 5.02 (95% CI=1.36–12.80) for intentional self-harm. Individuals ages 15-44 had a two-fold increase in mortality, compared with the general population. The multivariate Cox model indicated that increased risk of mortality was associated with older age, being male, being unemployed prior to injury, having a history of stroke, alcohol use, mental health issues, and back injury sustained in the accident. Premorbid lifestyle factors exerted a greater influence on mortality following TBI, compared with injury-related factors. This risk was especially prominent for younger individuals, who died primarily due to external causes. These findings highlight the need for interventions that address premorbid issues, such as substance abuse and mental health issues.
Introduction
T
Significantly higher rates of mortality have been reported within the first year following TBI, in comparison with the general population. 7 –10 Although mortality rates show a steep decline thereafter, they remain elevated, compared with the general population for many years post-injury. 9,11,12 Increased mortality rates have been most consistently related to older age at injury, worse severity of injury, and being male. 7 –10,12 –16 Nevertheless, Harrison-Felix and colleagues 15 found that when considering mortality risk across age groups, younger individuals showed the highest risk of death following TBI. Other risk factors for mortality include lower functional independence at admission and discharge, presence of comorbidities, discharge destination, comorbid psychiatric disorder, substance abuse, injury mechanism, level of education, marital status, and being unemployed at the time of injury. 7,11,12,14,15,17,18
Three Australian studies have examined mortality in patients admitted to inpatient rehabilitation with severe TBI only, reporting a mortality rate as high as 36% when restricting their sample to individuals who were functionally dependent at discharge from rehabilitation. 7,8,17 More recently, Baguley and colleagues 7 reported a mortality rate of 10.2% and a standardized mortality ratio (SMR) of 3.19 in a larger sample with severe TBI over a 20-year period. A recent study in the U.S. comprising a cohort of individuals with moderate to severe TBI who had completed inpatient rehabilitation and survived to one year reported an overall SMR of 2.25. 15 Mortality rates remained elevated 10 years after injury for all causes of death, with life expectancy shortened by a mean of 6.7 years. Risk of death was especially elevated for teenagers, young adults, and middle-aged adults. Causes of death also varied across age groups, with external causes of death (e.g., vehicular injuries, suicide) most common in the younger age groups, and chronic medical conditions (such as cardiovascular and respiratory disease), falls, and neurodegenerative disease more common in older age groups. 15
Studies from Glasgow, including mild as well as moderate-to-severe TBI cases, also reported higher risk of death relative to other trauma and healthy control samples, which was particularly elevated for younger individuals. 10,16,19 Pre- and post-injury lifestyle factors, such as substance abuse, mental and physical health problems, and subsequent head injuries were associated with higher death rates. The groups in these studies had higher rates of falls and assaults than other samples. These studies indicate that younger, rather than older, individuals may be more at risk of mortality following TBI.
In the current study, we examined the rate and causes of mortality following mild to severe TBI while also developing a multivariate prognostic model of mortality. We expected rates of mortality to be highest within the first year and to decline thereafter. Being younger, as well as older, being of male gender, and having lower education, pre-morbid medical complications, pre-morbid mental health issues, and pre-injury alcohol misuse were expected to increase the risk of death. We predicted that injury-related factors, including cause of injury, physical injuries sustained in the accident, and an abnormal computed tomography (CT) scan, would be associated with increased risk of death. We expected external causes of death to be more common in younger age groups and chronic causes of death more common in the older age groups.
Method
Participant characteristics
This study included 3341 individuals with mild-to-severe TBI (2407 male, 72%) admitted to the inpatient head injury rehabilitation program at Epworth HealthCare between 1983 and 2012. Individuals were admitted to a TBI rehabilitation center in the context of a no-fault accident compensation system administered by the Transport Accident Commission or Worksafe at the time of inpatient admission. The inpatient rehabilitation program provides an average of 5 h per day of physiotherapy, occupational therapy, speech therapy, and neuropsychology according to individual needs for an average period of approximately five weeks, but ranging between a few days and two years. This is followed by outpatient or community-based therapies and vocational support as required over an extended period, averaging nine months. Participants had a mean age of 35.7 years at injury (standard deviation [SD]=17.55; range=15-91), mean education of 11.2 years (SD=2.47; range=0-23), and mean days of post-traumatic amnesia (PTA) of 28.3 (SD=34.07; range=0.0-270.0). This sample comprised 8.5% mild (0-1 d PTA), 21.7% moderate (>1 to≤7 d PTA), and 69.9% severe (>7 d PTA) participants. 20 A total of 29.5% had a worst Glasgow Coma Scale (GCS) score of 13-15, 15.1% had a GCS score of 9-12, and 55.4% had a GCS score of 3-8. Abnormality on acute CT scan was evident for 80.9% of the sample. Participants in the mild range, as defined using duration of PTA, were also likely to be admitted to inpatient rehabilitation due to polytrauma. Specifically, 86.1% of those with mild TBI also had some form of moderate or severe physical injury: 28.4% had a back injury, 38.8% a chest injury, 23.3% abdominal injury, 64.9% limb injury, and 49.6% facial injury. The majority of participants (60%) were 15 to 34 years of age, male (72%), and had been injured in a motor-vehicle accident (86%). Following rehabilitation hospital admission, 90.2% of participants were discharged home, 5.5% to further rehabilitation or medical care, and 1.2% to a nursing home, while discharge destination was “other” for 3.0% of participants. For the current study, the mean risk exposure, or time between time of injury and follow-up, for the cohort was 13.2 years (SD=8.06; range=0.67-29.65 years).
Measures
Demographic and injury-related variables
Demographic and injury-severity variables were collected at the time of admission to the rehabilitation hospital. Demographic variables included: gender, age at injury, years of education, premorbid marital status (married/de facto vs. widowed/divorced/never married/single/separated), premorbid living location (metropolitan vs. country/interstate), premorbid employment, non-English speaking background, and premorbid medical history (psychological treatment or diagnosis, excessive or problem drinking, head injury, stroke). Injury-related variables included: cause of injury, GCS score, duration of PTA, inpatient CT scan findings (normal vs. abnormal), injury-related physical injuries (back, chest, abdomen, limb, or facial), and rehabilitation discharge destination. PTA duration was determined from daily administration of the Westmead PTA scale. Injury-related physical injuries were categorized as “No/minor” versus “Moderate/severe,” whereby the “Moderate/severe” injuries were those resulting in fractures or requiring surgery. CT scan abnormality was based on clinical ratings made by a neuroradiologist.
Procedure
This study was approved by Epworth HealthCare, Monash University, the Australian Institute of Health and Welfare, and the National Coronial Information System (NCIS) ethics committees. This study included individuals aged older than 15 years whose primary diagnosis was TBI. Patient demographic and injury-related information was retrieved from medical files. For matching purposes, the TBI database was provided to the National Death Index (NDI), which monitors Australian deaths since 1980, and the NCIS, which monitors external causes of death since 2000. All patient names were cross-checked between the study database and hospital medical records to ensure accuracy of data linkage. Matching with NDI and NCIS was based on participant surname, given name, date of birth, and gender. Once obtained, linkage results were inspected for accuracy. Causes of death were coded using the International Statistical Classification of Diseases and Related Health Problems, Ninth Revision for deaths from 1980 to 1996, and the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision for deaths occurring from 1997. The specific causes of death were unknown for 51 individuals who had only recently died or were still being investigated by the NCIS.
Statistical analysis
Mortality rates obtained from the Australian Bureau of Statistics (ABS) were used to calculate SMRs for males, females, and the overall TBI cohort. 21,22 Rates for 1994-1996 were chosen as a reference for the current study as this year was the mid-point, based on the dates of injury, for the TBI cohort. Mortality rates were also presented for the years 2009-2011 for a sensitivity analysis. Yearly SMRs were calculated using gender and age distributions specific to each of the follow-up years. Confidence intervals for the yearly and age-group based SMRs were calculated using the steps outlined by Ulm 23 and Dobson and colleagues. 24 Exact Poisson confidence intervals were calculated for causes of death. 25
Univariate Cox proportional hazard models were initially computed for each of the pre-morbid, demographic, and injury-related factors to explore risk of survival following TBI. 26 These factors were included in the current study, as they had been associated with mortality in previous studies. The assumption of proportional hazards (i.e., that for any two cases, the ratio of the estimated hazard is constant across time) was met through graphical and more formal methods of investigation using model interaction terms. In an attempt to create a model that included the necessary and influential predictors of mortality, only the factors that significantly influenced survival time in the univariate Cox hazard models were considered for subsequent multivariate models. Multivariate Cox proportional hazard regression models were performed in a hierarchical or sequential manner. Factors were grouped into theoretically and practically meaningful categories. Pre-morbid demographic factors were entered first, followed by pre-morbid medical factors, and lastly injury-related factors. The appropriateness of each factor to the multivariate model was evaluated using the log-likelihood model statistic. Factors that did not result in a significantly superior model were excluded from subsequent multivariate models. The Akaike Information Criterion corrected for small samples (AICc) of each multivariate model was used to simultaneously compare each of the models against one another, to determine their consistency with the observed data, using the steps outlined by Johnson and Omland. 27
Results
Participant mortality characteristics
There were 311 deaths for the total sample of 3341, equating to a mortality rate of 9.3%. The mean number of years until death following injury was 8.3 years (median=6.85; SD=6.22; interquartile range=8.76, range=0.04 to 25.70 years). SMRs for TBI participants were most pronounced between seven and 14 years following injury, compared with the general population rates. The average SMR over the entire follow-up period was 1.04 (95% CI=1.04-1.05) using 1994-1996 rates and 1.52 (95% CI=1.51-1.53) using 2009-2011 rates (Fig. 1). Using earlier general population death rates resulted in more conservative SMR estimates, compared with more recent death rates. All subsequent analyses were conducted using 1994-1996 death rates. Males showed a significantly increased all-cause SMR (1.20; 95% CI=1.06-1.37). All-cause SMR was not significantly different for females (0.99; 95% CI=0.79-1.23).
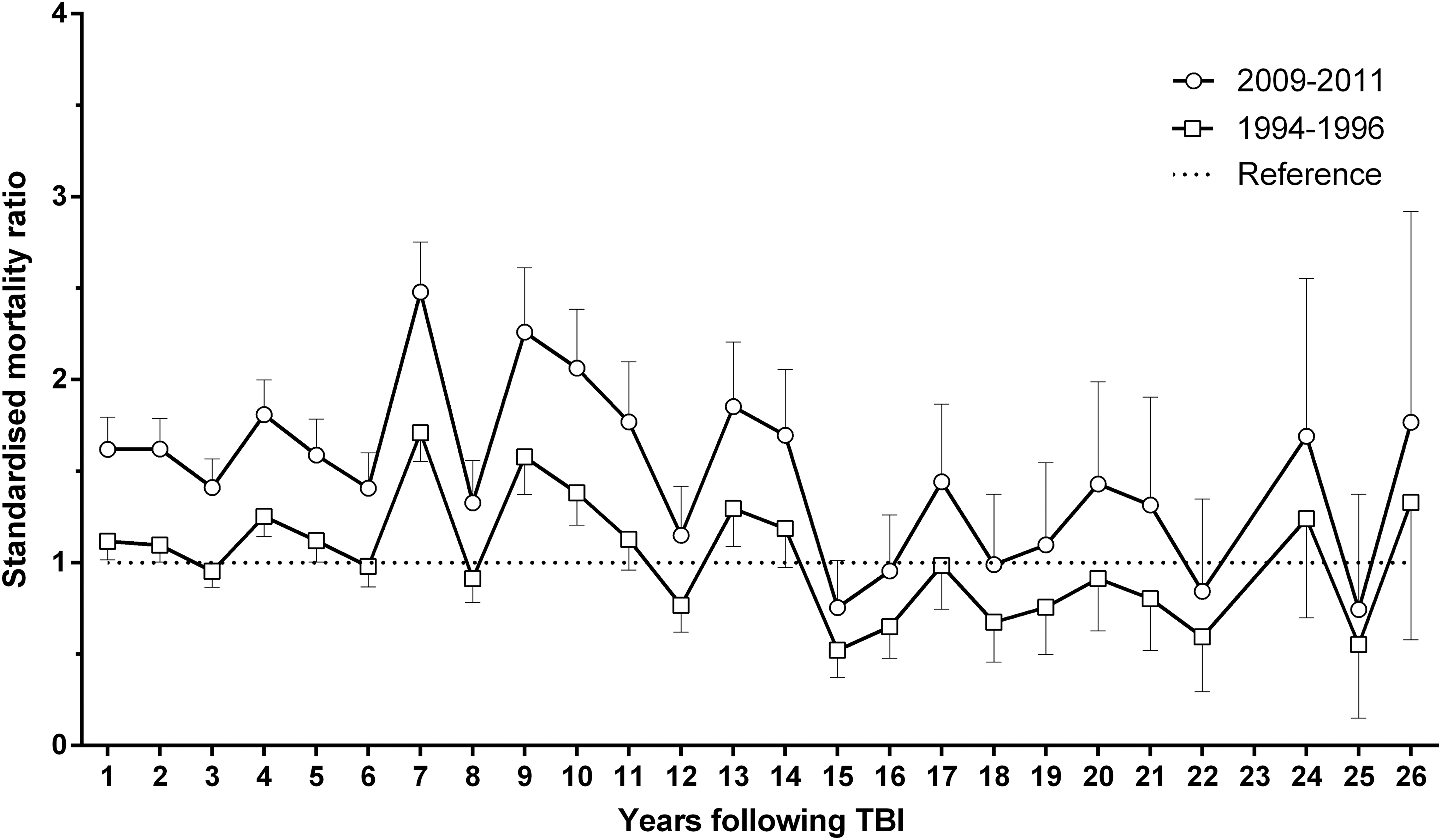
Yearly standardized mortality ratios and 95% confidence intervals over each follow-up year. The reference line indicates the population death rate.
Both males and females displayed a lower SMR for neoplasms, compared with the general population, and a significantly higher SMR for external causes and accidents (Table 1). Females also displayed a significantly elevated SMR for intentional self-harm. All of these deaths occurred at home, with three due to drug poisoning and the fourth due to the toxic effect of carbon monoxide. The average age of these four females at injury was 33.8 years. Three of the four were unemployed prior to the injury and had some form of moderate or major physical injury following their accident. Three of these participants had a complex premorbid social history. One was unemployed for many years pre-injury and had multiple previous suicide attempts, as well as a borderline personality disorder. Another had premorbid depression, anxiety disorder, and a previous suicide attempt. A third participant was in a long-term abusive relationship. Participants ages 15 to 44 were found to have about a two-fold risk of death, compared with the general population (Table 2). SMRs for participants older than age 44 were found to be no different from the general population. Individuals dying from external causes of death were also found to be significantly younger (mean [M]=35.21; SD=17.93) than those dying from other causes (M=61.17; SD=35.21). Conversely, individuals dying from chronic medical disease were significantly older (M=62.09; SD=18.00) than those dying from other causes (M=39.29; SD=20.54).
SMRs and 95% CIs were calculated using 1994-1996 general population death rates. This table does not comprise the 51individuals with unknown causes of deaths.
SMRs significantly elevated in the current TBI sample, compared with 1995-1996 cause-specific death rates in the general population.
SMRs significantly lower in the current TBI sample, compared with 1995-1996 cause-specific death rates in the general population.
Exact Poisson confidence intervals for small numbers calculated.
SMR not calculated due to extremely small count number.
ICD-10, International Statistical Classification of Diseases and Related Health Problems, Tenth Revision; SMR, standardized mortality ratio; CI, confidence interval; TBI, traumatic brain injury.
SMR, standardized mortality ratio; CI, confidence interval.
Univariate risk factors of mortality
Older age at injury, being unemployed prior to injury, being in a married or de facto relationship prior to injury, prior head injury, previous stroke, pre-injury alcohol use at excessive levels, and receiving treatment for a mental health problem prior to injury were significant univariate risk factors of mortality (Table 3). Individuals in a relationship pre-injury (M=45.0; SD=16.16; range=15-89) were significantly older than individuals who were single (M=30.4; SD=16.06; range=15-91; p<0.001). Gender was not a statistically significant risk factor. The effect of gender, however, may be masked by the association of older age with increased mortality. Gender differences may occur in younger age groups. Therefore, gender was still considered in multivariate modeling, which controlled for age.
<High school=less than 12 years of education; >High school=12 years of education and more.
CI, confidence interval.
Duration of PTA did not emerge as a statistically significant risk factor for mortality (Table 4). Having sustained the TBI as a pedestrian, due to a fall, or due to assault increased risk of mortality, while car accidents were associated with a reduced mortality risk. Pedestrians (M=40.9; SD=20.54; range=15-91) and individuals injured in falls (M=43.4; SD=17.64; range=17-82) were older than those injured due to other causes (M=34.0; SD=16.36; range=15-89; p<0.001). Those injured in car accidents (M=33.6; SD=16.90; range=15-89) were significantly younger than individuals injured due to other causes (M=38.3; SD=18.08; range=15-91; p<0.001), likely explaining the apparently reduced mortality due to motor vehicle accidents. No statistically significant difference in age was found between those who did (M=36.7; SD=12.84; range=19-63) and did not (M=35.6; SD=17.58; range=15-91) sustain injury due to assault. Accompanying back and chest injuries also were statistically significant risk factors for mortality. Being discharged to another hospital offering either rehabilitation or other forms of medical care or to a nursing home was related to an increased risk of death. Individuals discharged to a nursing home (M=57.9; SD=23.10; range=19-89) or another hospital for further rehabilitation or medical care (M=39.39; SD=19.02; range=15-90) were significantly older than individuals discharged home (M=35.06; SD=17.09; range=15-91; p<0.001), likely explaining the association of discharge destination with mortality.
Mild=0-1 d of PTA; Moderate=up to 7 d of PTA; Severe=more than 7 d of PTA.
CI, confidence interval; CT, computed tomography; PTA, post-traumatic amnesia.
Modeling risk of mortality using multivariate Cox regression
Model A indicated that older age was associated with increased risk of death. Model B resulted in a statistically superior model, indicating that males had a higher likelihood of dying (Table 5). Model C also resulted in a superior model, suggesting that those unemployed or not in the labor force, as well as those who were single prior to injury, had a greater likelihood of dying. Premorbid history of stroke, excessive pre-morbid use of alcohol, and treatment for mental health problems were entered in Model D. Only those with premorbid history of problem alcohol use or mental health problems had a greater likelihood of mortality following TBI. Entering causes of injury did not statistically improve the multivariate model using the log-likelihood, and so this factor was excluded from subsequent models. Including physical injuries in Model F did not result in a statistically superior model, compared with Model D. Sustaining a back injury did, however, increase risk of mortality. Lastly, discharge destination in Model G was not found to improve the model. Simultaneous comparison of all multivariate models using the AICc estimates indicated that Model F—which included age, gender, premorbid employment status, premorbid relationship status, stroke, excessive alcohol use history, history of psychological treatment, back and chest injury—was the best model of the candidate set.
=p<0.05; b=p<0.01; c=p<0.001
Lower −2 Log Likelihood and AICc model fit statistics indicate a better fit. Model comparisons were undertaken using the log likelihood model fit statistic.
CI, confidence interval; AICc, Akaike Information Criterion corrected for small samples.
Discussion
This study examined the rates and risk factors of mortality in a cohort of 3341 individuals with mild to severe TBI injury admitted for rehabilitation between 1983 and 2012. A mortality rate of 9.4% was observed. The rate of death was not elevated in the first year after injury and rates of observed deaths were highest between seven and 14 and more than 24 years following injury.
The mortality rate observed in the current study is similar to that reported by Baguley and colleagues, 7 who noted a death rate of 10.2% in their follow-up over an 18-year period. The current cohort exhibited a small but statistically significant increase in mortality rate, compared with the general population, with the SMR ranging between 1.0 and 2.0 for the first year following TBI, and being 1.04 overall. In contrast, Baguley and colleagues 7 reported an SMR of 12.0 over the initial year and an overall SMR of 3.2. This difference is likely due to the more severely injured cohort followed-up by Baguley and colleagues, 7 which excluded moderate and mild injuries. Conversely, 30% of participants in the current study had a mild or moderate TBI, as classified by PTA duration, and 45% had mild or moderate injuries, based on GCS score. Ninety-percent were discharged home, compared with 74% of those in Baguley and colleagues' cohort. 7
The sample in the present study was more similar in its composition to the rehabilitation sample studied by Harrison-Felix and colleagues, 15 who noted a mortality rate of 9.8% up to 21 years post-injury. However, the SMR in their study was 2.25, suggesting a death rate more than double that of the general population. This most likely reflects the higher proportion of elderly falls victims in their sample, given their finding that older age and being injured due to a falls were more common in those who had died. Consistent with both these previous studies, males had a higher overall SMR than females. In the present study, the overall mortality rate in females did not differ significantly from that in the general population.
Although injury severity and age may underpin the differences in SMR across these studies, one other factor to consider is the management of the patients. As already mentioned these patients had access to comprehensive individualized rehabilitation as needed across their lifetime. Although the patient cohort followed-up by Baguley and colleagues 7 had received inpatient and community-based rehabilitation, they were not treated under a lifetime care and support scheme. In addition, cohorts followed-up in Glasgow and in the U.S. likely had variable and more limited access to rehabilitation, which in the case of the U.S. depended on their insurance.
Examination of the SMRs across age groups revealed that participants aged 15-44 had a two-fold risk of death, relative to the general population, whereas SMRs for participants age older than 44 did not differ from the general population. This finding is largely consistent with the results reported by McMillan and colleagues in patients with mild to severe TBI as well as in patients with moderate to severe TBI. 10,16, 28 These findings suggest that while older age is a risk factor for mortality as it is in the general population, in the TBI population younger people are at disproportionately higher risk.
Males were three times more likely and females were 4.5 times more likely than the general population to die from external causes—which include accidents and intentional self-harm. In addition, females were five times as likely to die as a result of intentional self-harm, whereas the difference for males was not statistically significant. Thus, it would appear that in this sample, younger females were at high risk of self-harm or suicide after TBI. These females tended to have histories of premorbid substance use, mental health issues, as well as previous self-harm. The study by Harrison-Felix and colleagues 15 in the U.S. also reported an elevated risk of intentional self-harm, especially in individuals aged 15 to 24. 10,15 McMillan and colleagues 28 found elevated risk of death from external causes in young people, as well as a potentially increased risk of self-harm, but did not conduct significance tests due to small group numbers.
One counter-intuitive finding relating to injury causes was that of neoplasms being less common in the TBI cohort, compared with the general population. McMillan and colleagues, 10 however, also reported that mild TBI participants displayed elevated risk of death for all causes of death, compared with controls, except for neoplasms. Other common causes of death, such as diseases of the circulatory system, did not differ in frequency from the general population.
Univariate mortality risk factors included older age, being male, being single prior to injury, being unemployed or not in the labor force prior to injury, premorbid history of stroke, history of excessive alcohol use, pre-injury mental health problems, and having a back or chest injury. Similar risk factors are found in previous studies.7-10,12-14 The multivariate model suggests that premorbid/lifestyle factors exerted a significantly greater influence on post-injury mortality than injury-related factors, as was the case in the studies by McMillan and colleagues. 10,28 Younger people with a history of substance abuse, psychiatric problems, and unemployment are disproportionately represented in this population. 29 The high rate of death due to self-harm in younger females is particularly concerning. Elevated risk of suicide has previously been identified in the TBI population. 30,31 There is also a high rate of depressive and anxiety disorders after TBI, with associated suicidal ideation and suicide attempts, which may occur in those with or without any pre-injury history of previous psychiatric disorder. 32 -34
One other consideration highlighted in this study was the choice of community comparison group on which to base TBI mortality rates and the influence on SMRs. More conservative mortality rates were observed using 1994-1996 mortality rates, compared with 2009-2011 mortality rates. This is due to the decreasing mortality rates over time and is likely to affect all studies with follow-up over long time-frames. Although the current study acknowledged this bias and attempted to correct this by using mortality rates at the mean follow-up period in the current sample, caution should be exercised regarding generalization of mortality rates between studies.
Interpretation of the study findings should be undertaken with consideration of the specific rehabilitation context, as well as other sample characteristics. Participants were recruited from a single site and largely included patients who received rehabilitation within the context of a no-fault accident compensation system, and thus victims of motor vehicle and work-related accidents were disproportionately represented. Participants had access to comprehensive lifetime care and support, which may have influenced mortality outcomes. This compensation and support system differs from studies conducted in the U.S., where the amount and level of rehabilitation and long-term care services offered to patients following TBI is limited by insurance. One possible future avenue of investigation would be to examine the influence of various compensation schemes on mortality rate after TBI, as well as causes of death. As mentioned above, this study largely comprised individuals injured in motor vehicle accidents, with relatively few falls and assaults. This differs from sample demographics of other TBI populations, for example, in Glasgow, U.K., or the U.S., with a higher proportion of TBI's due to assaults and falls. These systematic differences also are likely to be associated with other premorbid socioeconomic factors, as well as susceptibility for further morbidity and mortality following TBI. Causes of death are also likely to be systematically biased since motor-vehicle accidents are related to younger age, while falls are associated with older age. Another limitation was that the follow-up schedule of study participants was heterogeneous. While rates of mortality within the first year would have included nearly all participants, rates at longer follow-up periods were based on smaller samples. Appropriate statistical methods were applied but certain causes of deaths had small samples, with a significant proportion of causes missing due to individuals having died relatively recently and should therefore should be interpreted cautiously.
Although confirming the association of mortality with age and pre-injury medical and lifestyle factors, the study also has highlighted the elevated risk of mortality in younger people sustaining TBI. Preventative programs to address psychiatric and substance use issues and risk-taking behavior in this population may represent an important means of reducing mortality in this group.
Footnotes
Author Disclosure Statement
This project is funded by the Transport Accident Commission through the Institute for Safety, Compensation and Recovery Research (ISCRR).