
Abstract
Traumatic brain injury (TBI) has long been associated with coagulopathy; however, the time course of coagulation/fibrinolytic parameters in the acute phase of TBI remains unclear. The purpose of the study was to analyze the time course of coagulation/fibrinolytic parameters in the acute phase of TBI and to elucidate parameter relationships to prognosis. We retrospectively evaluated 234 patients with severe isolated TBI with initial blood samples obtained no more than 1 h after injury. Platelet count, prothrombin time, activated partial thromboplastin time (aPTT), plasma levels of fibrinogen, and D-dimer were measured on arrival in the emergency department and 3, 6, and 12 h after injury. Multivariate logistic regression analysis was performed to identify risk factors for poor prognosis at each time point. From hospital admission to 12 h after injury, an elevated D-dimer level was a significant negative prognostic indicator (admission: p < 0.0001; 3 h after injury: p = 0.0005; 6 h after injury: p = 0.005; 12 h after injury: p = 0.0009). An upward trend of aPTT on admission and 3 h after injury was also a significant negative prognostic indicator (admission: p = 0.0011; 3 h after injury: p = 0.013). On multivariate logistic regression analysis, which included all initial variables, independent risk factors for poor prognosis included older age (p = 0.0005), low Glasgow Coma Scale score (p < 0.0001), high Abbreviated Injury Score (p = 0.015), aPTT >30.2 sec (p = 0.019), and elevated D-dimer level (p = 0.0005). We concluded that D-dimer is the best coagulation/fibrinolytic parameter to monitor for prediction of outcome.
Introduction
T
Coagulopathy after TBI includes hypercoagulable and hypocoagulable states that can lead to secondary injury from either microthrombi or hemorrhage. 4 –6 In particular, hemorrhagic lesions because of hypocoagulability are a critical and often fatal complication of TBI. 2,7 –9 Several reports have observed that the brain contains high concentrations of tissue factor that, if released into the circulation, trigger activation of the extrinsic coagulation pathway. 4,5,10 –12 These results suggest that the extent of activation of the coagulation system, which is determined by the amount of tissue factor released from damaged brain tissue, could be a reliable marker of the extent of brain damage. 13
Meanwhile, the results of the International Mission on Prognosis and Analysis of Clinical Trials in TBI (IMPACT) study suggest that alterations in coagulation parameters, manifested by elevations in prothrombin time (PT) and decreased platelet count, may be reliable markers of TBI outcome. 14 Other investigators have found that fibrinolytic parameters such as D-dimer are more reliable markers than coagulation parameters. 13,15 –17
Overall, most studies have shown a mixture of early and delayed coagulopathy in TBI. 18 Thus, a deeper understanding of the prognostic value of coagulopathy in the acute phase of TBI is needed, 17,18 because the time course of fibrinolytic parameters such as D-dimer in the acute phase of TBI, particularly within the first 12 h after injury, remains unclear.
An important priority in the early phase of care for patients with TBI is to evaluate the severity of brain injury and to predict the outcome. 19 –21 With this in mind, we evaluated the time course and role of coagulopathy in the acute phase of TBI by focusing on coagulation and fibrinolytic parameters, as well as other clinical variables, to assess which factor or combination of factors could best predict the outcome of TBI.
Methods
Setting
The Emergency and Critical Care Center of Kawaguchi Municipal Medical Center (Saitama, Japan) is a top-level critical care center in Saitama Prefecture. Approximately 1000–1200 patients are treated per year, with severe trauma cases amounting to 300–350 patients per year.
Patients
We retrospectively studied the demographic, clinical, and radiologic data on all patients with TBI who were admitted to our center from April 2007 to March 2014. Patients were eligible if the diagnosis was severe isolated TBI. Severe isolated TBI was defined as an intracranial Abbreviated Injury Score (AIS) ≥3 with an extracranial AIS <3, as described previously. 1,2,22 –24 A diagnosis of TBI was established from the findings on computed tomography (CT) scans and magnetic resonance (MR) images. Intracranial and extracranial AIS, CT scans, and MR images were independently evaluated by study intensivists and neurointensivists (R.N., Y.T., K.K., and Y.N.).
Exclusion criteria were a first blood sample collected more than 1 h after injury, incomplete information about injury time, age less than 16 years, liver failure, hematological disease, infection, malignancy, pregnancy, use of anticoagulants or antiplatelet agents, hypotension (systolic blood pressure <90 mm Hg) or hypoxemia (PaO2 <60 mm Hg) on admission, cardiopulmonary arrest before or on arrival at the hospital, transfusion of fresh frozen plasma (FFP) or platelets, death caused by conditions other than TBI, and incomplete information about outcome at 3 months after injury.
Of 345 patients with isolated TBI treated from April 2007 to March 2014, 12 were excluded because of a first blood sample collected more than 1 h after injury, and 6 were excluded because of incomplete information about injury time. Subsequent exclusions included 25 because of age less than 16 years, 4 because of liver failure, 1 because of hematological disease, 2 because of infection, 2 because of malignancy, 1 because of pregnancy, 8 because of use of anticoagulants or antiplatelet agents, 9 because of hypotension or hypoxemia on admission, 6 because of cardiopulmonary arrest before or on arrival at the hospital, 3 because of death caused by conditions other than TBI, and 15 because of incomplete information about outcome at 3 months after injury (some patients had more than one of the above exclusion criteria).
Moreover, we excluded 25 additional patients who received transfusion of FFP or platelets from this study population. Finally, 234 patients were included in this study. Informed consent to this study was obtained from the patient or from a legal representative. This study was approved by the hospital's Institutional Review Board.
Information on factors considered important to the outcome was collected, including age, 3,7,18,25 –27 sex, admission Glasgow Coma Scale (GCS) score, 3,17,23,24 and the AIS-head. 3,7,23,28 In all patients, blood samples for the initial (within 1 h after injury) platelet count, PT-international normalized ratio (INR), activated partial thromboplastin time (aPTT), and plasma levels of fibrinogen and D-dimer were drawn on arrival at the emergency department. Tests were routinely repeated 3, 6, and 12 h after injury.
Admission and follow-up CT scans and MR images were independently evaluated, and the type of head injury based on the radiologic findings was classified into acute subdural hematoma (ASDH), acute epidural hematoma (AEDH), intracerebral hematoma/contusion (ICH), and traumatic subarachnoid hemorrhage (TSAH).
Management of TBI
Immediately on arrival at the emergency department, treatment was given in accordance with guidelines for the management of TBI by the Japan Society of Neurotraumatology. 29 All patients underwent brain CT after detailed neurological evaluation and initial resuscitation. A second CT scan was routinely obtained no more than 3 h after admission, as well as whenever indicated by clinical deterioration or signs of increased intracranial pressure. When CT scans showed no significant abnormality but TBI was suspected, MR imaging was obtained immediately.
Assay of coagulation/fibrinolytic parameters:
Blood samples were drawn in ethylenediaminetetraacetic acid (EDTA) plasma and citrate. Platelet count was determined by the DC sheath flow detection method (Cellpack II® and SE sheath II,® Sysmex Corp., Kobe, Japan). PT was measured by the coagulating time method (Dade Innovin,® Sysmex Corp.). APTT was quantified by the coagulating time method (Thrombocheck APTT-SLA,® Sysmex Corp.). Fibrinogen was determined by the thrombin coagulating time method (Thrombocheck Fib (L),® Sysmex Corp.). D-dimer was measured by the latex immunoassay method (LIAS Auto D-dimer Neo,® Sysmex Corp.).
Statistical analysis
Analysis of data was performed using commercial software (SPSS Version 20.0®; IBM Corp., Armonk, NY). Patients were divided into two groups according to Glasgow Outcome Scale (GOS) 30 at 3 months post-injury. The good outcome group (group 1) included patients with good recovery or no more than moderate disability. The poor outcome group (group 2) had severe disability, vegetative state, or death. The GOS were independently evaluated by study neurointensivists (R.N. and Y.T) using in-person contact or telephone and mail communications to the hospital where patients were transferred from our hospital after discharge.
Demographic, clinical, and radiological parameters for the two groups were analyzed with the Student t test, the Mann-Whitney U test, or a chi-square test for continuous normally distributed, continuous non-normally distributed, and dichotomous data, respectively. Statistical significance was accepted at p < 0.05.
Multivariate logistic regression analysis was used to analyze coagulation/fibrinolytic parameters on arrival (within 1 h after injury) and at 3, 6, and 12 h after injury. This was to identify reliable prognostic markers after TBI, with the odds ratio (OR) and 95% confidence interval (CI) being calculated for each variable. To assess independent risk factors associated with poor prognosis at the time of admission, multivariate analysis was performed by the stepwise logistic regression method including all initial variables. Factors with p < 0.2 from the bivariate analysis were included in this model. For continuously distributed data, the threshold value of each variable that best discriminated between good and poor outcome was identified by receiver operating characteristic (ROC) curve analysis, and the area under the curve (AUC) and 95% CI were calculated.
Results
Demographic, clinical, and radiologic characteristics are summarized in Table 1. ASDH was observed in 148 (63.2%) patients, AEDH in 44 (18.8%), ICH in 176 (75.2%), and TSAH in 192 (82.1%) (some patients had more than one diagnosis). Overall, group 1 was composed of 164 (70.0%) patients and group 2 of 70 (30.0%) patients. Median age was 49 years in group 1 (25th–75th percentiles: 31–66) and 69 years in group 2 (25th–75th percentiles: 62–74), with this difference being significant (p < 0.0001). The two groups did not differ by sex. The clinical variables showing significant differences between the two groups were admission GCS score (p < 0.0001), the AIS-head (p < 0.0001), and the presence of ASDH (p < 0.0001), AEDH (p = 0.018), or ICH (p = 0.004).
Group 1, patients with a good outcome; Group 2, patients with a poor outcome.
GCS, Glasgow Coma Scale; AIS, Abbreviated Injury Score; ASDH, acute subdural hematoma; AEDH, acute epidural hematoma; ICH, intracerebral hematoma/contusion; TSAH, traumatic subarachnoid hemorrhage.
Blood samples for coagulation and fibrinolytic parameters were collected at 0.65 ± 0.19, 3.04 ± 0.12, 6.06 ± 0.17, and 12.05 ± 0.22 h after injury for the first, second, third, and fourth sets of laboratory values, respectively.
Time course of coagulation/fibrinolytic parameters
Figure 1 shows the time course of coagulation and fibrinolytic parameters of all patients on admission and at 3, 6, and 12 h after injury. Platelet count (normal range: 120–400 × 109/L) decreased significantly from admission (median: 222 × 109/L, interquartile range: 184–256 × 109/L) to 3 h after injury (p < 0.0001) (median: 196 × 109/L, interquartile range: 151–227 × 109/L), and then decreased insignificantly from 3 to 12 h after injury.
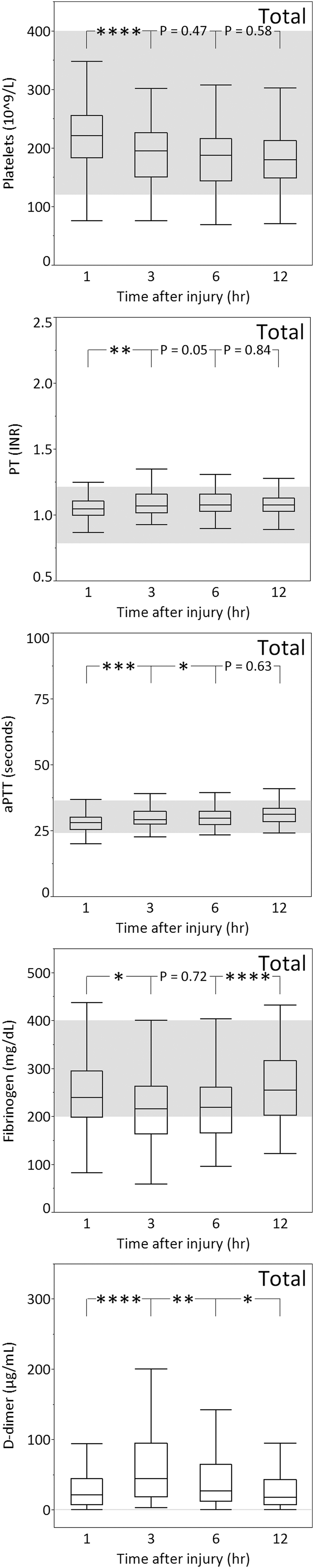
Platelet count, prothrombin time (PT,) activated partial thromboplastin time (aPTT), and plasma levels of fibrinogen and D-dimer of all patients on admission and at 3, 6, and 12 h after TBI. The gray zones represent the normal ranges for each parameter. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001.
PT (normal range: 0.8–1.2 INR) and aPTT (normal range: 24–36 sec) increased significantly from admission (median: 1.05 INR and 28.1 sec, interquartile range: 1.00–1.11 INR and 25.6–30.2 sec, respectively) to 3 h after injury (p < 0.01 and p < 0.001, respectively) (median: 1.07 INR and 29.2 sec, interquartile range: 1.02–1.16 INR and 27.5–32.4 sec, respectively). After 3 h, the median values remained within normal limits, but by that time, some were in the abnormal range.
Plasma fibrinogen concentration (normal range: 200–400 mg/dL) decreased significantly from admission (median: 240.0 mg/dL, interquartile range: 199.3–296.0 mg/dL) to 3 h after injury (p < 0.05) (median: 216.0 mg/dL, interquartile range: 164.5–263.3 mg/dL), subsequently increased insignificantly from 3 to 6 h after injury, and increased significantly from 6 (median: 220.0 mg/dL, interquartile range: 166.0–262.0 mg/dL) to 12 h after injury (p < 0.0001) (median: 255.0 mg/dL, interquartile range: 203.5–316.8 mg/dL).
The most dynamic changes were detected in the plasma level of D-dimer (normal range: 0.0–1.0 μg/mL): the median plasma level of D-dimer was already abnormal on admission (median: 21.6 μg/mL, interquartile range: 8.2–44.8 μg/mL), increased further from admission to 3 h after injury (p < 0.0001) (median: 45.3 μg/mL, interquartile range: 18.8–95.6 μg/mL), and then subsequently significantly decreased.
To evaluate the relationship of coagulation/fibrinolytic parameters to outcome, we compared values between group 1 and group 2 (Fig. 2). The PT, aPTT, and D-dimer levels in group 2 were significantly higher than in group 1 at all time points from admission to 12 h after injury, except for the fourth aPTT level. Meanwhile, platelet count and plasma fibrinogen concentration in group 2 were significantly lower than in group 1, except for the first and second fibrinogen levels. The most marked difference between group 1 and group 2 at all time points from admission to 12 h after injury was in the plasma level of D-dimer (p < 0.0001 at all time points).
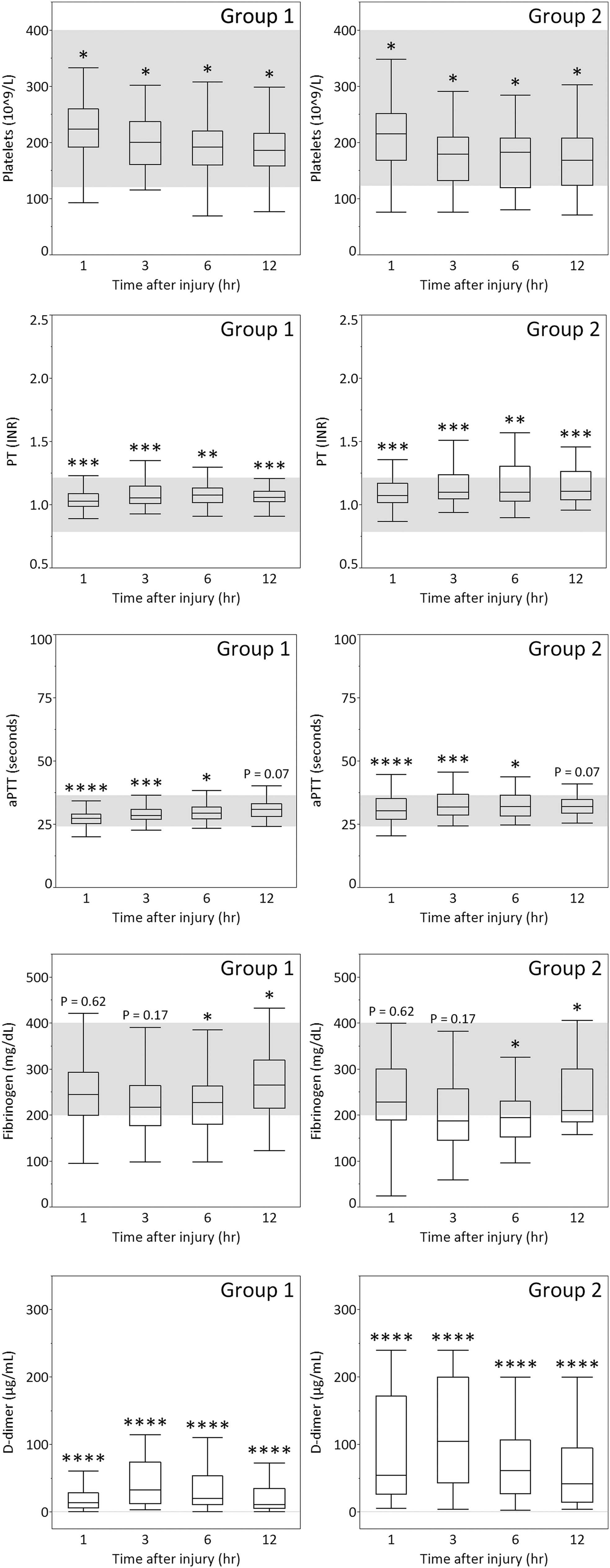
Platelet count, prothrombin time (PT,) activated partial thromboplastin time (aPTT), and plasma levels of fibrinogen and D-dimer of patients with a good outcome (group 1) or poor outcome (group 2) on admission and at 3, 6, and 12 h after TBI. The gray zones represent the normal ranges for each parameter. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001.
Coagulation/fibrinolytic parameters as a prognostic marker of TBI
To identify reliable prognostic markers at each time point after TBI, multivariate logistic regression analysis was performed using platelet count, PT, aPTT, and plasma levels of fibrinogen and D-dimer on admission and at 3, 6, and 12 h after injury (Table 2). From admission to 12 h after injury, elevated D-dimer level was a significant prognostic indicator in this analysis. Prolonged aPTT on admission and at 3 h after injury was also a significant indicator of poor prognosis.
CI, confidence interval; PT, prothrombin time; INR, international normalized ratio; aPTT, activated partial thromboplastin time.
Admission: R2 = 0.40; 3 h after injury: R2 = 0.52; 6 h after injury: R2 = 0.31; 12 h after injury: R2 = 0.30).
Relationship between clinical variables and outcome
To assess independent risk factors at the time of admission associated with poor prognosis, all initial variables with a p < 0.2 by bivariate analysis were included in stepwise logistic regression analysis. As seen in Table 3, this analysis was performed using age, GCS score, AIS-head, presence of ASDH, AEDH, ICH, and TSAH, platelet count, PT, aPTT, and plasma levels of D-dimer. The resulting independent risk factors for poor prognosis included old age, low GCS score, high AIS-head, prolonged aPTT, and elevated D-dimer. Threshold values were 58 years for age, 9 for GCS score, 5 for AIS, 30.2 sec for aPTT, and 32.7 μg/mL for D-dimer. The presence of AEDH was significantly associated with a good prognosis.
CI, 95% confidence interval; AUC, area under curve; 95% GCS, Glasgow Coma Scale; AIS, Abbreviated Injury Score; ASDH, acute subdural hematoma; AEDH, acute epidural hematoma; ICH, intracerebral hematoma/contusion; TSAH, traumatic subarachnoid hemorrhage; PT, prothrombin time; INR, international normalized ratio; aPTT, activated partial thromboplastin time.
R2 = 0.72.
Discussion
In this analysis of the time course of coagulation and fibrinolytic parameters in the acute phase of TBI, we found that the median plasma level of D-dimer was already higher than normal on admission, and peaked about 3 h after TBI. We also found that fibrinolytic parameters such as D-dimer differed more strongly between group 1 and group 2 than differences in coagulation parameters such as the platelet count, PT, aPTT, and fibrinogen through the acute phase of TBI. D-dimer was the best coagulation/fibrinolytic predictor of outcome.
Recently, several articles have described the time course of coagulation parameters in the acute phase of TBI. 22,23,31,32 Halpern and associates 22 showed that an early peak in PT occurred between 1 and 6 h after injury, with a subsequent return to normal values at 6 to 12 h. Lustenberger and colleagues 23 revealed that while peaks in PT-INR were seen 6 and 36 h after hospital admission, the most prominent decrease in mean platelet count was most frequently seen 24 h after admission.
On the other hand, only a few studies have reported the time course of fibrinolytic parameters in the acute phase of TBI. 6,33 In an overview article that did not mention actual values, Stein and coworkers 6 demonstrated that the plasma levels of fibrin/fibrinogen degradation products (FDP) and D-dimer were abnormal within minutes of TBI. 6 They also observed that plasma FDP levels peaked about 6 h after injury and that plasma D-dimer levels peaked about 12 h after injury. In a similar review article, Kuo and colleagues 33 also found that increased D-dimer levels occurred within 4 h after TBI.
In the present study, increasing change in aPTT and the plasma levels of D-dimer from admission to 3 h after injury were demonstrated. The prolonged aPTT is caused by the activated coagulation pathway and depletion and/or dysfunction of coagulation factors in the plasma as a result of TBI. 4 –6 If the D-dimer level is elevated, increased plasmin activity secondary to enhanced fibrinolytic activity promotes fibrin degradation 4 –6 ; that is, combined prolonged aPTT and elevated D-dimer level in the early phase of TBI can be considered as simultaneous hypercoagulability and hyperfibrinolysis.
On the other hand, the plasma fibrinogen concentration decreased significantly from admission to 3 h, changed very little from 3 to 6 h, and increased significantly from 6 to 12 h after injury. The decrease in the plasma fibrinogen concentration could be caused by the consumption to make fibrin clot or direct destruction. 34 The tendency of the fibrinogen concentration to increase after 6 h indicates a hemostatic shift, characterized by inhibition of fibrinolysis. This is consistent with the decrease in plasma D-dimer beginning 3 h after injury. The decrease in platelet count from admission to 3 h after injury might be because of the consumption from the formation of crosslink-stabilized platelet-fibrin clot immediately after TBI. 4
We also detected the onset of hyperfibrinolysis within the first hour after injury. Of 234 patients who had D-dimer measured in this study, only three (1.3%) patients had a value within the normal range. Interestingly, MR imaging of these three patients revealed no lesions with mass effect such as ASDH or ICH, but rather small hemorrhagic foci in the corpus callosum or cerebral white matter. This result suggests that fibrinolytic parameters may not increase markedly in patients with small hemorrhagic lesions alone, unlike patients with localized brain injuries with more obvious hemorrhages such as ASDH and ICH.
Yokota and associates 35 showed that the serum level of thrombomodulin, which is released from damaged or activated cerebral endothelial cells and parallels changes in plasma FDP levels, was higher in localized brain injuries than in diffuse brain injury. This result is consistent with our present findings.
It is well known that AEDH, unlike ASDH, is not often associated with parenchymal injury. 36 –38 In other words, there is little activation of the coagulation system, and the outcome of AEDH is generally good. Similarly, we demonstrated that the presence of AEDH conferred a low-risk prognosis, although most patients had two or more diagnoses. Disentangling the independent impact of each TBI type is important and will require large-scale studies with sufficient patient numbers to allow subgroup analysis of patients with single TBI types.
We also observed that D-dimer as a fibrinolytic parameter increased progressively between admission and 3 h after injury and remained elevated for at least 12 h after injury. These results indicate that patients presenting within 12 h after injury, especially within 3 h after injury, have a high risk of hemorrhage expansion because of hyperfibrinolysis. Allard and coworkers 7 observed a four-fold increase in mortality (32% vs. 8%) in coagulopathic patients with hemorrhagic progression on follow-up CT scan. The greatest risk factor for progression of hemorrhagic lesions was coagulopathy within the first 24 h after TBI. 7
We believe that hyperfibrinolysis can cause hemorrhage expansion by degradation of coagulation factors, breakdown of formed fibrin clot, and impaired clot formation because of excess generation of fibrin degradation products. Usually, patients who “talk and deteriorate” (T & D) are defined as those in whom rapidly progressive disturbances of consciousness develop (GCS score of 8 or less) within 48 h after injury. 39 –41 In most cases, GCS score deteriorates within several hours after injury. 42
In our study, there were 107 patients who scored 13 or higher on the GCS score on admission in 10 (9.3%) of whom the clinical picture of T & D developed. Intriguingly, this condition developed within 3 h after injury in 7 of these 10 patients. This finding suggests that hyperfibrinolysis in the acute phase of TBI is more likely to contribute to the phenomenon of T & D through progression of the hematoma. Takahashi and associates 13 also found that in patients in whom T & D went on to develop could be readily identified on admission using fibrinolytic parameters such as α2-plasmin inhibitor-plasmin complex and D-dimer.
Previous reports have revealed that the early hypercoagulable state after TBI is followed by an increase in fibrinolytic activity, with fibrinolytic parameters such as FDP and D-dimer being reliable prognostic markers. 13,15 –17 In our study, plasma levels of fibrinolytic parameters displayed greater differences between group 1 and group 2 than those of coagulation parameters through the acute phase of TBI. In addition, an elevated D-dimer level was an independent risk factor for poor prognosis in this analysis at all time points from admission to 12 h after injury.
Other investigators have cited abnormalities in platelet count, PT, aPTT, and fibrinogen as predictive of the worst outcome in patients with TBI. 7,14,18,23,24,31,43 –47 We consider that the wide variation in indicators of poor prognosis after TBI may originate from a mixture of early and delayed coagulopathies, as described by Greuters and colleagues. 18 Coagulation and fibrinolytic parameters undergo dynamic changes during the acute phase of TBI, so it is important to pay close attention to the elapsed time from injury when they are measured.
Previous studies have emphasized the importance of the aPTT in predicting poor outcomes. 43,44 Oertel and coworkers 44 revealed a 42.3% rate of hemorrhagic progression after TBI on the 24-h follow-up CT scan; risk was highest in patients with elevated partial thromboplastin time (PTT), who showed a 100% progression rate. McLeod and colleagues 43 demonstrated that PTT was a stronger predictor of mortality, with TBI patients who had an abnormal PTT having a 326% increase in all-cause mortality when controlling for other prognostic indicators.
In our present study, aPTT was a significant indicator of poor prognosis only up to 3 h after injury. We propose that the absence of statistical significance of aPTT in determining outcome after 6 h post-injury is because of its small changes over a short time course. Unlike D-dimer, prolonged aPTT usually returned to the normal range in the acute phase, so aPTT is not a reliable prognostic marker 6 h or more after injury. The threshold value of aPTT as a prognostic indicator at the time of admission was 30.2 sec, which is within normal range. This result suggests that patients with TBI whose aPTT is in the high normal range have a poor prognosis.
Indeed, an elevated D-dimer level was the only laboratory measurement that was an independent risk factor associated with poor prognosis at all time points from admission to 12 h post-injury, indicating its value as an indicator over this length of time. We analyzed the relationship between outcome and the degree of elevation in the plasma level of D-dimer from admission to 3 h and the degree of decline from 3 to 6 h after injury, but found no significant association between them (p = 0.19 and p = 0.09, respectively). We consider that a poor prognosis may be associated with high plasma levels of D-dimer, and not the degree of elevation or decline.
In addition to prolonged aPTT and elevated D-dimer level, stepwise logistic regression analysis showed that old age, low GCS score, and high AIS-head were independent risk factors associated with poor prognosis. Several studies have reported a strong correlation between increasing age and decreasing chance of mental recovery after head injury. 3,7,18,25 –27
A large-scale meta-analysis showed a correlation between increasing age and poorer outcome, revealing that mortality and unfavorable outcomes are seen in 52% and 74% of patients aged older than 55 years, respectively. 25 The association of poorer outcomes such as vegetative state or death with increasing age beyond a certain threshold was previously noted in the United States traumatic coma data bank for age cutoff points of 55 years old, 27 which is consistent with our results for a threshold value of 58 years old. These results support the hypothesis that coagulation/fibrinolytic abnormalities increase in older patients with TBI because of the increased vulnerability of cerebral vessels and high sensitivity of cerebral endothelial cells to trauma. 27,35,48 –51 Further investigation of the physiological and pathophysiological features in the aging brain may aid prevention of the poorer outcomes associated with advanced age.
The results of the present study indicate that the objectives of treatment of TBI should be to combat coagulation and reverse hyperfibrinolysis. May and associates 52 advocated the use of FFP as fluid resuscitation in patients with a GCS score ≤7. Several studies, however, have found no improvement in outcome with the use of FFP. 53,54
Various other approaches have been explored to correct coagulopathy in TBI. Recombinant factor VIIa (rFVIIa) provided a rapid and successful correction of coagulopathy in patients with TBI, which might suggest an alternative strategy for managing coagulopathy in TBI. 55 Interestingly, treatment with rFVIIa within 4 h after the onset of intracerebral hemorrhage limited the growth of the hematoma, reduced mortality, and improved functional outcomes at 90 days. 56 Recently, however, Perel and colleaues 57 reported that there was no reliable evidence from randomized controlled trials to support the effectiveness of hemostatic drugs in reducing mortality or disability in patients with TBI in their review article about the available randomized clinical trials of rFVIIa in TBI.
The Clinical Randomisation of Antifibrinolytic in Significant Hemorrhage (CRASH-2) trial is a large international multicenter randomized placebo-controlled trial of the effects of the antifibrinolytic agent tranexamic acid (TXA) on death and transfusion requirements in adult trauma patients with significant hemorrhage. 58 This study provided more insight into the use of antifibrinolytic agents in trauma patients but could not confirm a benefit on progression of lesions or outcome after TBI. 59 Investigating the beneficial effect of early treatment of coagulation disorders in TBI in well-performed blinded randomized trials should be a priority for future research, and we await the results of the ongoing CRASH-3 trial and the Resuscitation Outcome Consortium (ROC) TXA trial. 60,61
Limitations
This study has several limitations. The data were not designed to evaluate the impact of surgery or hemodilution from osmotic diuretic agents, either of which might have affected coagulation/fibrinolytic parameters after 3, 6, and 12 h post-injury. Differences in the mechanism of TBI between Japan and other nations are most likely attributable to the high average age of the Japanese population, resulting in what might seem to be an overrepresentation of elderly patients with severe TBI. A GOS score taken at 3 months may be somewhat premature in severe TBI. Further investigation and implementation of long-term follow-up studies of these patients is necessary when evaluating recovery after severe TBI.
Conclusions
Coagulation and fibrinolytic parameters undergo dynamic changes during the acute phase of TBI. Routine measurement of fibrinolytic parameters such as D-dimer to predict the occurrence of coagulopathy and the expected outcome is warranted. Future studies should reveal whether early recognition of acute coagulopathy and the prevention of delayed hemostatic disturbances might be associated with improvements in morbidity and mortality in patients with isolated head trauma.
Footnotes
Author Disclosure Statement
No competing financial interests exist.