
Abstract
Traumatic brain injury (TBI) is the main cause of death in trauma victims and causes high rates of disability and neurological sequelae. Approximately 38–65% of traumatic brain contusions (TBC) demonstrate hemorrhagic expansion on serial computed tomography (CT) scans. Thus far, however, no single variable can accurately predict the hemorrhage expansion of a TBC. Our purpose was to evaluate contrast extravasation (CE) as a predictor of expansion, mortality, and poor outcome in TBC in a Brazilian cohort. After Institutional Review Board approval, we used multidetector CT angiography (MDCTA) to study 121 consecutive patients (106 men, 87.6%) with ages varying from 10 to 85 years. Informed consent was obtained from all subjects. The clinical and imaging findings were correlated with the findings on the initial MDCTA using either the Fisher exact test or Student t test and a multivariate logistic regression model. Of the persons who presented CE in TBC, 21.8% died (in-hospital mortality), whereas in the absence of this sign, the mortality rate was 7.6% (p = 0.014). In addition, expansion of the hemorrhagic component of the TBC was detected in 61.1% of the CE-positive patients, whereas expansion was only observed in 10% of the CE-negative patients (p < 0.001). Poor outcome was observed in 24.2% of the patients in the CE-negative group, but in the presence of CE, 72.7% evolved with poor outcome (p < 0.001). The CE was a strong independent predictor of expansion, poor outcome, and increased risk of in-hospital mortality in our series of patients with TBC.
Introduction
T
Several factors such as concomitant coagulopathy, the need for cardiopulmonary resuscitation, old age, multiple hematomas, midline shift, surgical decompressive procedures, initial TBC size, and the presence of subdural hematoma have been associated with radiological expansion of the hemorrhagic component of the TBC. 7,10,13,15 –17 Thus far, however, no single variable accurately predicts this serious progression. 8,10,11
Active contrast extravasation (CE) on computed tomography angiography (CTA) has been intensively studied in primary 17 –24 and secondary intracerebral hemorrhage (ICH). 25,26 In nontraumatic ICH, CE on CTA has been confirmed to predict hematoma expansion, poor outcome, and high mortality. 17 –24 Despite some reports on CT identification of CE in head trauma, 14,27,28 there are only a few studies on this topic. 14,27 Further, it remains necessary to reproduce the CTA results and evaluate the prognostic implications of the CE in this population of patients with TBI in a larger series.
Our main aim is to study the CE characteristics on CTA-source images (CTA-SI) and estimate their relationship with expansion of the hemorrhagic component of the TBC, poor outcome, and mortality rate in a Brazilian cohort of patients with TBI. The relevance of this study derives from the potential reproducibility of CTA technique as a daily routine to evaluate this not uncommon scenario, which often demands intensive care and determines serious neurological sequelae in economically active persons around the world.
Methods
Patients
After Institutional Review Board approval, we prospectively analyzed patients of any age or sex who presented to the emergency department with a clinical history of TBI wherein the hemorrhagic component of TBC measured ≥2.0 cm on any axis, demonstrated on NCCT, from August 2011 to October 2014. Informed consent was obtained from all subjects (signed personally or by their guardians). CTA with comparable imaging parameters was performed on patients who arrived at the hospital within the first three days after brain trauma. We excluded patients with contraindications to the administration of the intravenous iodine contrast agent, patients who refused to participate in the study, and patients whose examination quality was considered inadequate or contained technical artifacts.
Clinical history and laboratory results were reviewed to identify arterial hypertension diagnosis or diabetes mellitus and to confirm coagulation disorders. A coagulation disorder was defined as any disturbance in a patient's coagulation parameters, including prolongation of the prothrombin time (PT), (PT <70%), elevation of the International Normalized Ratio (INR), (INR ≥1,4), elevation of the activated partial thromboplastin time (aPTT), (aPTT >38 sec), or a decrease in the platelet number (PLT), (PLT <100,000). All patients were monitored in the intensive care unit or emergency department and treated according to the current guidelines for the management of brain contusion. 29
All imaging examinations were conducted using a 64-slice CT scanner (Brilliance CT 64 Channel, Philips Medical, Eindhoven, North Brabant, The Netherlands), adding CTA to the first requested NCCT. The CTA examination was performed using 120 kilovolts and 185 milliamperes, a 450 mm field of view, 0.6 mm section thickness, and a pitch of 0.673. The first acquisition (arterial phase) was performed after a time delay of 20 sec by injecting iodine contrast at 4–6 mL/sec in a dual-head power injector (Medrad, Warrendale, PA) with an appropriate intravenous access, which was generally 18-gauge in adults and 22-gauge in children, located in a peripheral vein, at a dose of 1.0 mL/kg. The additional acquisition of CTA (venous phase) was obtained using identical parameters 60 sec after the beginning of the contrast administration.
The control imaging study was performed according to clinical judgment, using only a standardized NCCT, within the first three days after admission, without interference from this study. Therefore, if some of our patients did not undergo the control CT, we decided anyway to keep them in the study to examine their mortality, because it would not be possible to study the expansion of hemorrhage.
Imaging analysis
The imaging interpretation included analysis of the NCCT and CTA-SI, as well as the maximum intensity projection (MIP) and three-dimensional (3D) post-processed views of CTA. All data were post-processed using commercially available software on a workstation (Extended Brilliance Workspace v3.5.0.2250, Philips Medical Systems Nederland B.V., PC Best, The Netherlands). All images were evaluated by two neuroradiologists with 19 and 4 years of experience in the diagnosis of TBC and in the interpretation of CTA. Differences in reader interpretation regarding the presence or characteristics of CE were decided by consensus.
The CE is a bright spot on CTA-SI, which is predictive of hemorrhage progression. 14,17 –24,27 It was considered to be present or absent on CTA-SI adapted according to previously reported criteria proposed for primary ICH: 19 one or more foci of contrast pooling within a TBC (of any size and morphology), discontinuity from normal or abnormal vasculature adjacent to the TBC (to distinguish of vessels in the interior of the TBC), and presenting attenuation ≥120 Hounsfield units (HU) in the post-contrast phases of CTA (to distinguish hyperattenuating foci of heterogeneous hemorrhage).
To comparatively categorize our cohort of subjects, we considered the number of foci of CE within the TBC, the largest dimension of focus and attenuation in HU to build a contrast extravasation score (CES), as previously proposed for primary ICH, 19,30 no matter in what phase of the CTA they appeared.
The volume of the hemorrhagic component of the TBC was calculated on the first NCCT scan, estimating its three major axes and multiplying the result by 0.5. The perilesional areas of vasogenic edema and extra-axial hemorrhage were not considered in the volume measurement. NCCT data were also assessed for subarachnoid hemorrhage, subdural hematoma, intraventricular hemorrhage, and midline shift. Midline shift was measured at the level of the foramen of Monro.
Expansion of the hemorrhagic component of the TBC was defined at the follow-up NCCT by an absolute growth greater than 6 mL or a relative growth of more than 33% from the initial NCCT, in accordance with other ICH studies. 18,24 A poor outcome was defined when an expansion of the hemorrhagic component of the TBC occurred at the follow-up NCCT, when the patient died by neurological damage, or when surgery was necessary to treat the TBC.
Statistical analysis
Univariate analysis using either the Fisher exact test or Student t test was performed to determine the relationship between the presence of CE within the TBC and expansion, poor outcome, and in-hospital mortality. We also used a multivariate logistic regression model to identify the independent predictors of TBC expansion, the presence of CE, and in-hospital mortality. The results were considered to be statistically significant when p ≤0.05. The data were analyzed by using the Statistical Package for Social Sciences (SPSS) statistical software, version 14.0 (SPSS Inc., Chicago, IL).
Results
According to the inclusion criteria, 188 subjects were consecutively selected during the defined period. A total of 67 patients (67/188–35.6%) were subsequently excluded: 16 subjects (16/188–8.5%) with a diagnosis of TBC less than 2.0 cm along the longest axis, 6 additional subjects (6/188–3.2%) with a diagnosis of TBC but not within the first 3 days of the trauma, 34 (34/188–18.1%) excluded because of unavailable peripheral venous access to obtain CTA images, and 11 (11/188–5.8%) excluded because of artifacts in the images.
We finally enrolled 121 subjects (121/188–64.4%) with a diagnosis of TBC into the current study. Demographic data, the initial volume of the hemorrhagic component of the TBC, and the elapsed time between the trauma and the first CTA were all analyzed (Appendix 1; see online supplementary material at
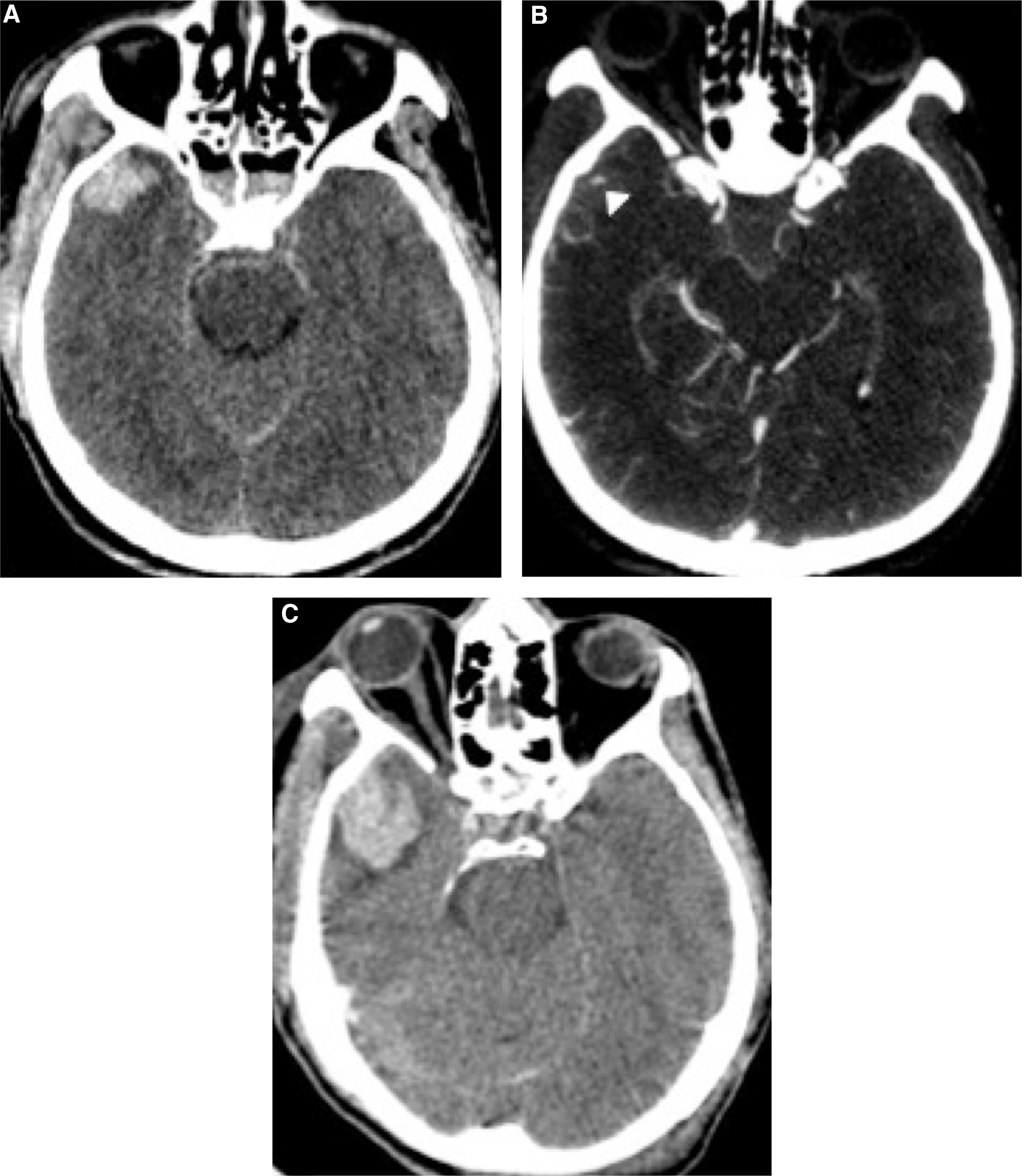
The CE on CTA-SI was documented in 55 subjects (55/121–45.4%) (Fig. 1). All cases of CE (55/55–100%) were detected during the venous phase of CTA-SI in our series. Conversely, this imaging sign was only detected in 44 subjects during the arterial phase of CTA-SI (44/55–80.0%).
A 19-year-old man presented with head trauma after falling 4 meters. (
The initial average volume of the hemorrhagic component of the TBC was 16.4 mL (range 1–187 mL). The average volume was 24.7 mL in the CE-positive group (range 1.6–187 mL) and 9.5 mL in the CE-negative group (range 1–105 mL). The initial median volume of the hemorrhagic component of the TBC was 6.1 mL (interquartile range [IQR] 2.45–14.5 mL). The median volume was 10.6 mL in the CE-positive group (IQR, 4.1–32.1 mL) and 5.2 mL in the CE-negative group (IQR 2.25–8.625 mL). The median volume of the hemorrhagic component of the TBC was 5.2 mL (IQR 2.25–8.625 mL) in patients with CES 0; 6.5 mL (IQR 2.2–21.8 mL) in CES 1; 14.55 mL (IQR 4.25–48.475 mL) in CES 2; 7 mL (IQR 4.45–10.15 mL) in CES 3; 26.1 mL (IQR 7.5–187 mL) in CES 4 (Table 1).
CES, contrast extravasation score; N, total number of patients; N2, total number of patients with CT control; IQR, interquartile range; AUC, area under the curve; CI, confidence interval.
Adapted from spot sign score. 30
The CE was documented up to 72 h after trauma, with a mean of 11 h (range, 1–72 h) and a median of 6 h (IQR, 4–14 h).
When categorizing patients according to the CES, we found 25 patients with CES 1 (25/55–45.4%), 22 with CES 2 (22/55–40.0%), 5 with CES 3 (5/55–9.1%), and 3 additional patients with CES 4 (3/55–5.5%) (Table 1).
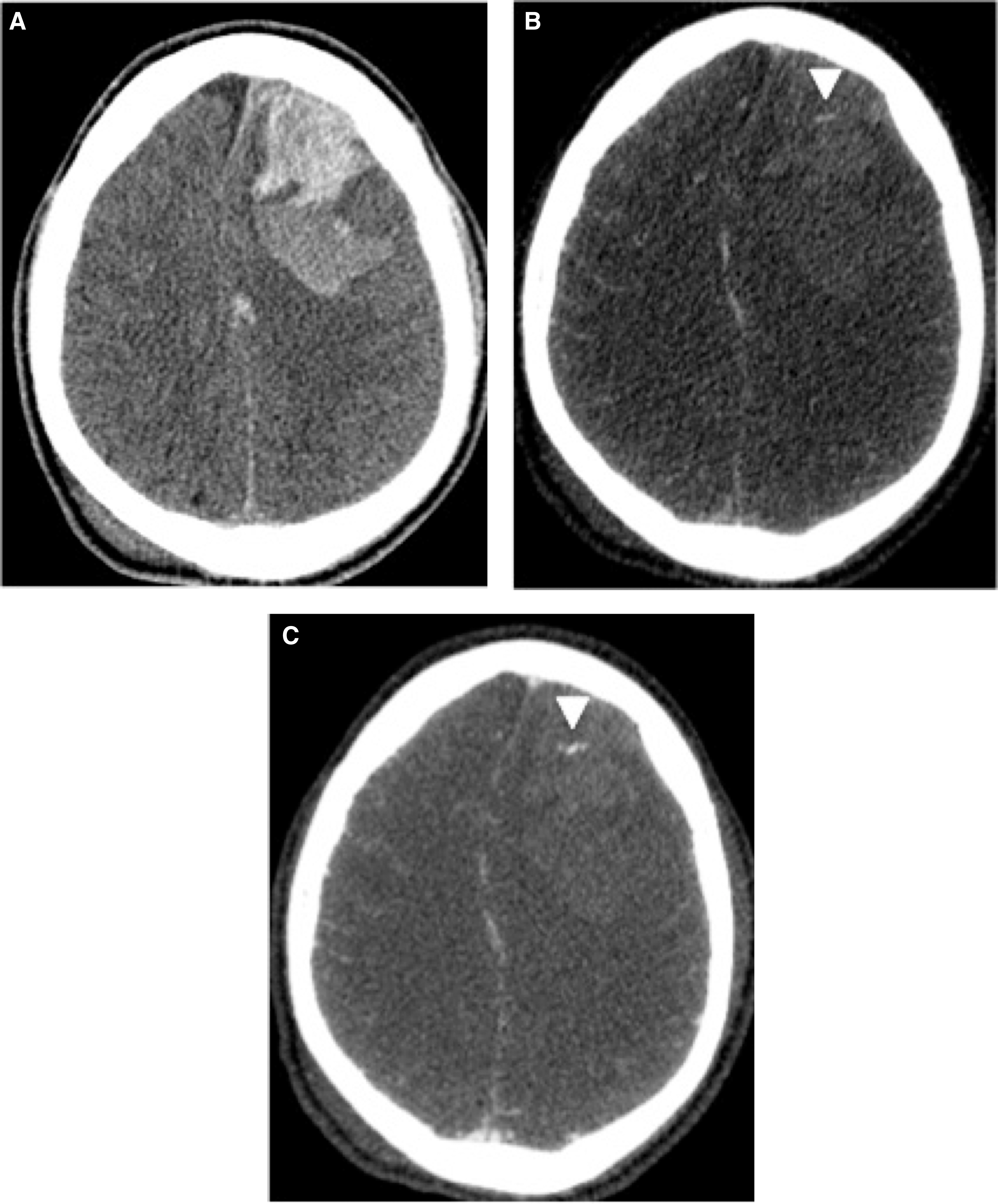
Hemorrhagic expansion of a TBC was documented in 10.0% (6/60) of patients in the CE-negative group and in 61.1% (22/36) (p < 0.001) of the CE-positive group (Fig. 2). A poor outcome was registered in 24.2% (16/66) of the patients in the CE-negative group and in 72.7% (40/55) of the patients in the CE-positive group (p < 0.001). A mortality rate of 7.6% (5/66) was documented in CE-negative group, whereas the CE-positive group exhibited 21.8% (12/55) in-hospital mortality (p = 0.014) (Table 1).
A 52-year-old man presented with head trauma after falling 7 meters. (
In the univariate analysis, it was important for the occurrence of the CE: hemorrhage volume >50 mL (p = 0.008), the presence of subarachnoid hemorrhage (p = 0.006), subdural hematoma (p = 0.002), and ventricular hemorrhage (p = 0.003). Mortality was primarily influenced by: blood glucose ≥170 mg/dL (p = 0.02), the presence of coagulation disorder (p = 0.04), the hemorrhage volume >50 mL (p = 0.01), admission GCS ≤8 (p < 0.001), the presence of subarachnoid hemorrhage (p = 0.08), subdural hematoma (p = 0.02), ventricular hemorrhage (p = 0.04), and CE (p = 0.014). It was relevant for the expansion of the TBC in the univariate analysis: the presence of coagulation disorder (p = 0.03), subarachnoid hemorrhage (p = 0.03), subdural hematoma (p = 0.01), and CE (p < 0.001) (Table 2).
Only patients with control CT.
Univariate analysis.
×, multivariate logistic regression analysis.
CD, coagulation disorder; ICH, intracerebral hemmorhage; GCS, Glasgow Coma Scale.
Multivariate logistic regression was used to analyze certain additional features, including age, sex, TBC location and volume, CE, midline shift, subarachnoid hemorrhage, subdural hematoma, ventricular hemorrhage, and Glasgow Coma Scale Score (GCS). Mortality was primarily influenced by GCS ≤8 (odds ratio, 15.2; 95% confidence interval, 2.90–79.56; p < 0.001) and CE (odds ratio, 4.2; 95% confidence interval, 1.21–15.18; p = 0.024), whereas expansion of the hemorrhagic component of the TBC was influenced by CE (odds ratio, 14.14; 95% confidence interval, 4.82–41.53; p < 0.001), in multivariate logistic regression.
Discussion
Recent studies have shown that 38–65% of TBCs present expansion of the hemorrhagic component. 6 –13 In our series, the expansion of the hemorrhagic component of the TBC was observed in 29.1% of our patients, somewhat lower than previously reported in the literature, probably because of our restricted selection criteria, which selected patients within up to 72 h after injury. This criterion probably included a comparative bias to select patients who had less severe TBI. Most reports limit the selection to 6 h or 24 h after injury. 14,27
The hemorrhagic lesion in TBI often progresses during the first hours after trauma, either expanding or developing new hemorrhagic lesions. 6 Usually the hemorrhagic expansion of TBC has been attributed to continued bleeding of microvessels fractured at the time of primary injury, and classically two factors are involved in this expansion: the presence of coagulation disorder and the recently described progressive microvascular failure initiated by the impact. 6
Although some studies in the literature do not support a simple relationship between coagulopathy and expansion of TBC, 6 our study found a positive association between coagulopathy and expansion of TBC. A large percentage of patients in whom hemorrhagic expansion of a TBC develops may not have coagulation abnormalities, however, and, conversely, hemorrhagic expansion will not develop in many patients with coagulopathy. 6 Thus, the relationship between hemorrhagic expansion of TBC and coagulopathy is not simple.
Therefore, Kurland and associates 6 recently showed in their review a novel mechanism account for hemorrhagic expansion of TBC that involves delayed, progressive microvascular failure initiated by the impact. 6 For delayed hemorrhage or expansion of TBC to occur, either microvessels must have been fractured at the time of impact, even though they showed no evidence of bleeding initially, or microvessels not fractured at the time of impact must finally be opened, hours after the impact, to allow extravasation of blood. 6 This latter mechanism would occur by cellular and molecular events in microvessels after impact injury 6 and have been studied in the cortex in animal models of contusive injury that accurately replicate hemorrhagic expansion of TBC. 6,31,32 These findings could explain the predictive utility of evaluating CE in TBC.
The expansion of the hemorrhagic component of the TBC is relevant because it worsens the prognosis of patients, because it might promote increased mass effect and higher intracranial pressure. 6 No single variable can yet accurately predict the expansion of the hemorrhagic component of the TBC; however, several features have been studied as possible predictors of expansion, including coagulopathy, the need for cardiopulmonary resuscitation, old age, multiple hematomas, midline shift, surgical decompressive procedures, initial size of the TBC, and presence of subdural hematoma. 6 –16
Alahmadi and colleagues 7 found that the presence of subdural hematoma and initial hemorrhage volume are predictors of expansion of the TBC. Our data enlarge this knowledge to include coagulopathy, subarachnoid hemorrhage, and mainly CE as predictors of expansion of the TBC. The CE was an independent predictor of expansion of the hemorrhagic component of the TBC in multivariate logistic regression. Similar to previous TBC studies, 14,27 our results demonstrate the prognostic value of CE in TBI. Compared with previous reports, 14,27 however, the current one included a larger population. Magnetic resonance imaging series have evaluated the focal enhancement of traumatic hematomas 33,34 and CE in nontraumatic ICH, 35 similarly suggesting a predictive value of CE in these settings.
The inconsistent definition for hematoma expansion has been debated in the current literature. 18,19 Several expansion thresholds have previously been proposed, including any increase in the hemorrhage or 20%, 25%, 30%, or 33% growth to define expansion of the hemorrhage; other studies have used an increase of 5 mL, 6 mL, or 12 mL to define expansion. To ensure the clinical significance of our results, we decided to use a stricter threshold in accordance with other ICH studies. 18,24
The occurrence of CE in our series was 45.4%, agreeing with previous studies, which have reported values varying from 40.9–50%. 14,27 It is known that early arrival to the hospital is related to a higher frequency of CE within the TBC. 27 Our results are consistent with this tendency, although the findings most strongly associated with the occurrence of the CE were the presence of subdural hematoma and ventricular hemorrhage rather than time of arrival at the hospital. Because subdural hematoma and ventricular hemorrhage are predominantly determined by venous bleeding, early imaging acquisition and the presence of subdural hematoma and ventricular hemorrhage are likely intrinsically correlated. The presence of CE was more frequent in our series in patients who came to the hospital sooner but also occurred in patients who arrived later, likely as a marker of more severe parenchymal laceration in the latter case.
Our study also showed that the initial average volume of the hemorrhagic component of the TBC was higher in the CE-positive group, suggesting that it may represent a marker of more severe parenchymal laceration in these persons. Despite the initial volume of hemorrhage, it has been important in predicting mortality in univariate analysis; in the multivariate analysis, the most important findings for mortality were GCS ≤8 and the presence of the CE. The initial volume of TBC was not a predictor of expansion either in univariate or multivariate analysis. Our results show that CE is an important predictor of expansion and mortality in TBC. Once even in patients with CES 3, which showed comparable TBC volumes, those patients with CES 0 and 1, and smaller volumes than patients with CES 2, showed higher rates of expansion and mortality than previous.
The venous phase of CTA has been reported to increase the detection of CE by 8–23% in primary ICH. 19 Similarly, the venous phase of CTA was also the most important for the detection of CE in our series of patients with TBC, allowing for additional detection in 20% of the patients compared with the arterial phase of CTA. No patients were suspected of traumatic vessel injury, and the arterial phase of CTA did not show any unsuspected lesions in either the large or middle arteries. Thus, we argue that in this setting, the venous phase of CTA (60 sec delayed) is sufficient to detect CE and to estimate the expansion of the hemorrhagic component of the TBC. It is important to reduce radiation exposure, primarily in young patients, when arterial traumatic lesions are not suspected. More studies are needed, however, to determine the real importance of the arterial phase of CTA in this setting.
To the best of our knowledge, this work is the first MDCT study of TBC to apply the CE score proposed by Delgado-Almandoz and coworkers 30 in primary ICH to TBI. We found that the higher score (CES) is significantly correlated with the expansion of the hemorrhagic component of the TBC, with a higher mortality rate and with a worse prognosis of these patients. Verification of the reproducibility of this score, however, remains necessary in this setting.
Coagulopathy is reported to occur in patients with TBI on admission with some variability, 36 but Harhangi and colleagues 37 reported an overall prevalence of 32.7%. Coagulopathy was observed in 28.9% of our patients, similar to the findings of Harhangi and colleagues. 37 Although Smith and associates 38 found no association between the presence of coagulopathy and the expansion of the TBC in their studies, we found a statistically significant association between coagulopathy and expansion in 48% of patients, whereas Allard and coworkers 39 found expansion in 80% of patients with coagulopathy compared with the 36% observed for patients without coagulopathy. A recent review of hemostatic drugs for TBI has concluded that there is no reliable evidence from randomized controlled trials to support the effectiveness of hemostatic drugs in reducing mortality or disability in patients with TBI. 40 This issue, however, is important, and additional trials are still required. 41
In agreement with a previous report, 14 we found an association of the CE with in-hospital mortality and poor outcome. Although a poor outcome was observed in 24.2% of patients in CE-negative patients, in the presence of CE, 72.7% of our patients exhibited poor outcomes. The mortality rate was also significantly higher when CE was found on CTA-SI.
Our report has certain limitations, including the delayed arrival of the patients to our center, which may have biased the study toward the inclusion of less severe TBIs. Long-term prognosis was not considered, because the focus of this study was primarily the acute in-hospital course. Another limitation is the volume calculation method. Although computer-aided planimetry shows fewer errors and improved performance for irregularly shaped hematomas, 42 we used the ABC/2 method because it is more routine, easier, and widely used in clinical practice. 43
The authors encourage the use of CTA, particularly the venous phase, in an imaging work-up for TBI, in patients with TBC, even to study patients who arrived at the hospital after the first s6 h of trauma. CTA-SI was shown to be useful for detecting CE, even up to 72 h after trauma, which was positively associated with expansion of the hemorrhagic component of the TBC, poor outcome, and in-hospital mortality. Further studies on this topic remain needed to improve care for this serious neurological effect, particularly with the use of hemostatic procedures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.