
Abstract
Sexuality is an integral part of the human experience and persists in health and disability. The cardiovascular system is crucial to sexual function and can be affected profoundly by spinal cord injury (SCI). The effects of sexual activity on the cardiovascular system in SCI have not been summarized and compared with sexual activity in able-bodied individuals. A keyword search of Embase, PubMed, and Medline was conducted. From 471 retrieved studies for able-bodied individuals, 11 were included that met the strict criteria of medically uncomplicated participants. In the SCI literature, 117 studies were screened, with 18 meeting criteria. In able-bodied persons, sexual activity resulted in modest increases in systolic blood pressure peaking at orgasm (males of 163 mm Hg and females of 142 mm Hg) and returning to baseline shortly afterward. In persons with SCI, results varied from minimal changes to significant elevations in systolic blood pressure because of episodes of autonomic dysreflexia, especially in those with high thoracic and cervical lesions. Peak systolic blood pressure in these individuals was measured to be as high as 325 mm Hg. In the SCI population, more intense stimuli (including penile vibrostimulation and electroejaculation) tended to result in a greater increase in systolic blood pressure compared with self-stimulation. Studies that used continuous versus intermittent monitoring were more likely to report greater changes in systolic blood pressure. In able-bodied persons, sexual activity results in modest increases in blood pressure. In those with SCI, intense stimulation and higher injury levels result in a higher likelihood of autonomic dysreflexia and elevated blood pressure. Because of rapid changes in blood pressure, continuous monitoring is more advantageous than intermittent measurement, because the latter may miss peak values.
Introduction
S
Sexual activity involves the coordination of many organ systems and is vulnerable to dysfunction. 5 The cardiovascular system is particularly important and is responsible for blood flow shifts to genital tissue and delivering oxygen to metabolically active areas. Sexual activity is known to be associated with changes in blood pressure (BP) and heart rate (HR) and is known to produce an additional demand on the cardiovascular system. 6
A common question asked by patients to healthcare providers after a significant health event like stroke or myocardial infarction is: “When is it safe to have sex at all?” Most practitioners would point to the latest evidence stating that if the patient's cardiovascular condition is stable and there is no evidence of ischemic changes during the metabolic equivalents of being sexual, then it is “safe” to have sex, either with one's self or partners. 7 There is still ongoing discussion among clinicians and scientists, however, on the exact variability of the cardiovascular responses during the sexual activities in both able-bodied persons and in persons living with various disabilities. 8
Individuals living with spinal cord injury (SCI) are vulnerable to both sexual dysfunction and alterations in cardiovascular control. 3,9,10 When surveyed about the priority of various body functions to quality of life, men and women with SCI reported that restoration of sexual function was either the first or second highest priority, even above the return of walking, sensation, and normal bladder and bowel function. 4
Common fertility interventions to assist the SCI population include vibrostimulation and electroejaculation procedures available in specialized centers. 11 These procedures can be dangerous because of the possibility of cardiovascular side effects even when conducted under medical supervision. 12 The same is true of urological procedures such as cystoscopy and lithotripsy. 13 To help a patient make an informed decision before the procedure, the clinician must be knowledgeable about which factors make a patient prone to these risks, and what measures can be used to prevent such risks.
One unique aspect of the cardiovascular response related to sexual activity in the SCI population is autonomic dysreflexia (AD). 14 This is a potentially life-threatening complication of SCI and occurs most commonly in those who have sustained an injury at or above the sixth thoracic spinal cord segment. 15 Episodes of AD occur when a noxious, or nonnoxious stimulus, triggers peripheral afferents below the level of the SCI, stimulating spinal circuits and resulting in massive activation of spinal sympathetic neurons. This results in the release of catecholamines and peripheral vasoconstriction, causing a rise in BP.
Elevated BP is detected by the intact carotid and aortic baroreceptors, but compensatory inhibitory control to the spinal sympathetic neurons is inadequate because these tracts are interrupted by the person's SCI. This process is often accompanied by bradycardia, because intact parasympathetic neurons carried within the vagus nerve remain intact and will try to compensate for high BP. 14
Episodes of AD are often associated with headache, sweating, piloerection, flushing, visual changes, nasal congestion, and feelings of apprehension. 16 Symptoms resulting from AD can cause significant discomfort and can have a negative impact on the quality of life of an individual living with SCI, including refraining from sexual activity if AD is triggered. Further, this uncontrolled, sudden increase in BP can lead to debilitating complications such as myocardial infarction, 17 seizures, 18 retinal or cerebral hemorrhage, 19,20 or even death. 18
AD resulting from sexual stimulation has been described in various reports of ischemic symptoms, emergency department visits, and urgent administration of antihypertensive medications: the discomfort and risks of AD can sometimes cause avoidance of sexual stimulation altogether. 21 –23 In addition, cardiovascular disease is often cited as a leading cause of mortality in the SCI population. 24 Uncontrolled BP may pose an additional and cumulative risk should a patient experience repeated bouts of AD. 25
This systematic review will focus on characterizing the cardiovascular responses to sexual activity in able-bodied individuals and persons living with SCI. In addition, this review identifies gaps in the evidence that can help direct clinical management and research efforts in the areas SCI, sexual health, and rehabilitation of persons with SCI and other disabilities.
Methods
A key word literature search of English language published articles from 1948–2012 in Embase; PubMed and Medline databases were conducted to source original articles, practice guidelines, and review articles. Two investigators developed a set of key words that were used in a search for the review. Two independent reviewers (RD and AK) applied inclusion and exclusion criteria and evaluated the quality of each study to be included.
The first search used two sets of key words including “sexuality, orgasm, ejaculation, sexual arousal, and masturbation” and “cardiovascular measures, blood pressure, arterial pressure, cardiovascular, and hypertension.” Studies were included if the population included healthy, able-bodied individuals. Studies were excluded if subjects had significant comorbidities, if medications were involved as a part of the study, or if the BP and HR measurement method or interval was unclear (Fig. 1).
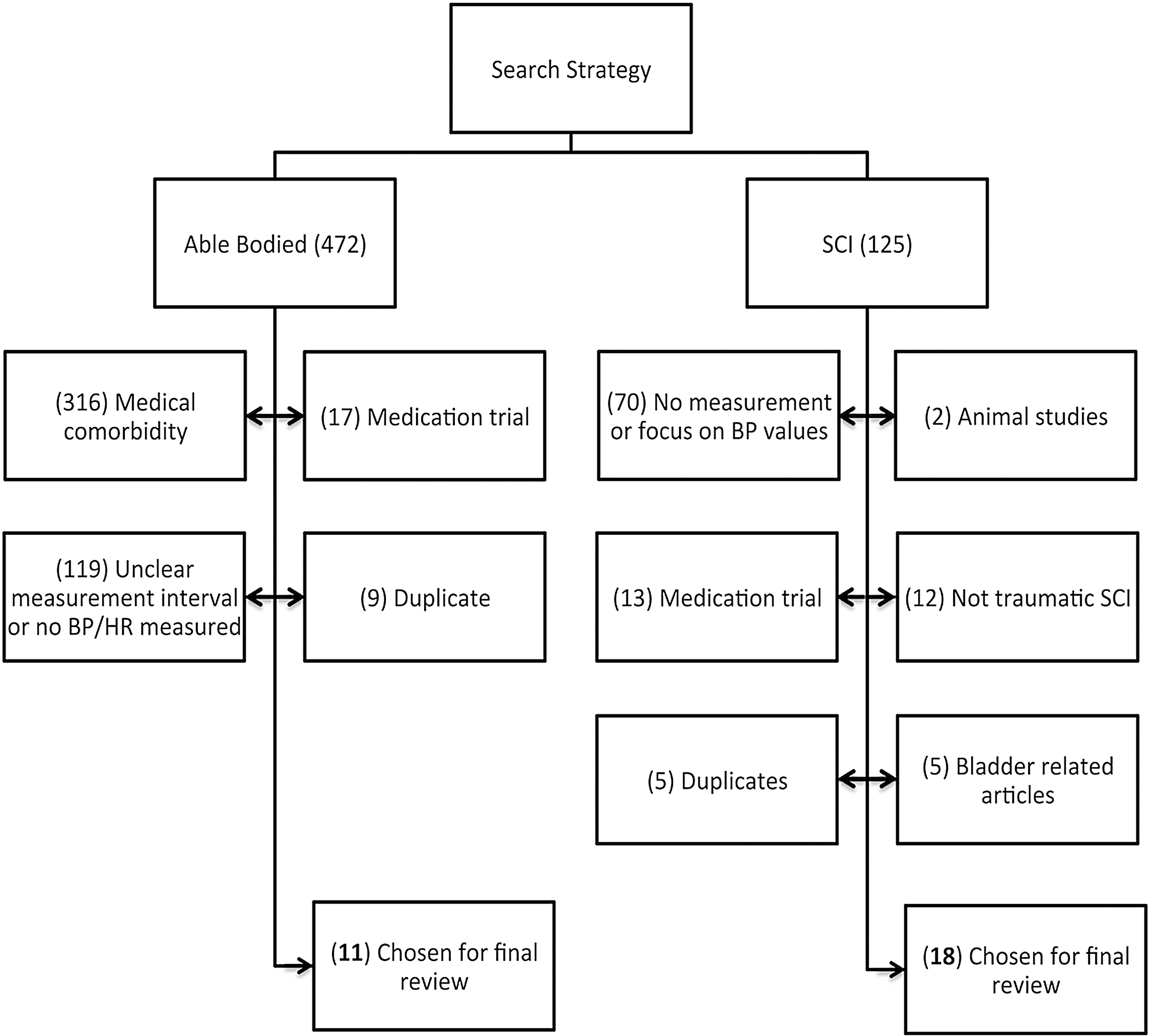
Flow chart describing the study search strategy, studies excluded and included. SCI, spinal cord injury; BP, blood pressure; HR, heart rate.
The second search was conducted using the three separate sets of search key words “sexuality, orgasm, ejaculation, infertility, sperm retrieval, penile vibratory stimulation, electroejaculation, sexual arousal, masturbation” and “spinal cord injury, tetraplegia, paraplegia” and “cardiovascular measures, blood pressure, arterial pressure, cardiovascular, hypertension, arrhythmia, and autonomic dysreflexia.” Studies were included if the subjects had an SCI. In study protocols using a pharmacological intervention, placebo group results were included if they met inclusion/exclusion criteria. Studies were excluded if no BP or HR measurement methods were specified, or if no measurement interval was identified (Fig. 1).
Using this criterion, the initial search provided us with a total of 471 studies for able-bodied individuals. Only 11 satisfied the strict inclusion criteria and were included for the final analysis. In the SCI literature, of the 117 studies screened, 18 studies met criteria and were included in this review.
Results
Eleven articles in the able-bodied population met criteria and were included into the review. Two major types of stimuli were identified in these studies: self-stimulation, 6,26 –28 and sexual intercourse. 6,29 –34 The range of average maximal systolic BP (SBP) for all participants in these studies varied from 120 to 200 mm Hg (Table 1).
F, female; avg, average; BP, blood pressure; mm Hg, millimeters of mercury; HR, heart rate; bpm, beats per minute; SBP, systolic blood pressure; CV, cardiovascular; M, male; RR, respiratory rate; RPP, rate-pressure product; VO2, oxygen uptake; MET, metabolic equivalent; ECG, electrocardiogram; MOT, man on top; MOB, man on bottom.
Four studies reviewed conducted an observation of cardiovascular changes during self-stimulation in able-bodied individuals, two including data for males, 6,27 one for females, 28 and one for both sexes (no HR data). 26 The overall average change in SBP from baseline in these studies was 22.5 ± 12 mm Hg for men and 25.5 ± 26.9 mm Hg in women. The average maximal SBP was slightly higher in men ranging from 137–181 mm Hg, and lower in women, ranging from 120–158 mm Hg, while the increase from baseline was similar in both groups. HR elevations occurred in both men and women during self-stimulation as well, averaging 30.3 ± 12 bpm above baseline for men and ±11 bpm for women (only one study). 28
The average peak SBP during sexual intercourse in able-bodied persons was higher in men (37 ± 21 mm Hg) compared with women (27.75 ± 49 mm Hg), although with considerable overlap. Average peak SBP reported in these studies ranges between 141–188 mm Hg for men and 120–200 mmHg in women. There was a universal increase in HR during intercourse that was reported to average 54.3 ± 11 bpm in men (range 44–65 bpm), and averaged 18.5 ± 21 bpm in women (range 4–33 bpm).
In the SCI population, 18 articles qualified and were included into the final review (Table 2). 23,35 –51 Three major types of stimulation were identified including self-stimulation, 35 –39 penile vibrostimulation (PVS), 23,41 –47,51 and electroejaculation (EEJ). 48 –50
F, female; BP, blood pressure; SCI, spinal cord injury; mm Hg, millimeters of mercury;
SBP, systolic blood pressure; AD, autonomic dysreflexia; HR, heart rate; RR, respiratory rate; CV, cardiovascular; bpm, beats per minute; UMN, upper motor neuron; LMN, lower motor neuron; M, male; PVS, penile vibrostimulation; AIS-A, complete SCI; EMG, electromyography; ECG, electrocardiogram; MAP, mean arterial pressure; DBP, diastolic blood pressure.
The average maximal SBP found in the SCI studies varied widely from 121 to 325 mm Hg (Table 2). It was noted that the high BP values (more pronounced episodes of AD) were more likely to be reported if one or more of three conditions were true. If the stimulus applied was either very intense (as in PVS or EEJ procedures), peak SBP was higher. If the study subjects had a level of injury above the T6 spinal segment, peak SBP tended to be higher. Finally, if the study recorded BP values using a continuous versus intermittent method of BP readings (Table 3), 23,42 –44,48,49,51 peak SBP was higher because continuous measurement is likely to catch the higher, fleeting measurements.
SBP, systolic blood pressure; M, male; C, cervical; T, thoracic; L, lumbar.
In the SCI group, the average change in HR in response to sexual stimulation also varied widely from declining by 17.5 bpm below baseline 41 to increasing by 13 bpm above baseline. 51 Bradycardia was most commonly described with the very high BP elevations indicative of AD. 23,43,51
Discussion
Cardiovascular responses during sexual activity in able-bodied individuals
Various models of sexual function exist to describe the stages that humans traverse during sexual arousal. 52,53 The classic model published by Masters and Johnson describes excitement, plateau, orgasm, and resolution phases based on laboratory observations of physiologic parameters they observed in more than 600 healthy subjects of varying ages. They noted that men generally progress through the four phases more quickly than women, often with a very short plateau phase, and achieve only one orgasm per cycle because of a refractory period. In contrast, women have the potential to achieve single or multiple orgasms per cycle. Both sexes had the potential to fluctuate between excitement and plateau without carrying on to orgasm.
Original data from Masters and Johnson indicated a rise in both HR and BP in men and women during the excitement and plateau phase, peaking at, or slightly after, orgasm. Of all phases, the orgasmic phase was the shortest, lasting only 10–15 sec for men, and for women, 20–60 sec. 52 During this time, HR and BP were noted to be at their peak. Other early studies report a maximal SBP of 180–200 mm Hg in young healthy adults. 30,31 Later studies find generally lower BP and HR, with significant individual variability.
Cardiovascular changes during self-stimulation in able-bodied adults
The studies reviewed revealed mild-modest increases in HR and BP in able-bodied persons in response to self-stimulation. 6,26 –28 For men, intermittent noninvasive BP recordings of self-stimulation resulted in BP elevations of 7–30 mm Hg above baseline and HR changes of 9–38 bpm. 27 In women with continuous cardiovascular recordings during self-stimulation, average SBP elevations of 38 mm Hg above baseline 28 with mild average elevations in HR 11 bpm above baseline were observed. 28
One study looked at oxygen uptake and metabolic expenditure in relatively young men during self-stimulation to orgasm, finding that this activity required a peak oxygen uptake of 6.3 mL/kg/min, equating to a metabolic expenditure of 1.8 METS. 6 This is not a significant physical or cardiovascular stress and is approximately equivalent to the energy that we would spend during cooking or dressing activities (∼ 2.0 METS). 54
Cardiovascular responses during intercourse in able-bodied adults
In able-bodied individuals during intercourse, the cardiovascular response in both men and women followed a similar pattern to that described during self-stimulation, but with higher peak HR and BP values. These parameters tended to rise slowly throughout intercourse, peaking for a short period at or around orgasm, and then quickly returning to baseline, usually within 1 or 2 minutes.
In healthy able-bodied men, the literature reported a range of average peak SBP of 141–188 mm Hg and average peak HR between 96–170 bpm. 6,29 –34 This wide variability likely reflects a number of factors. First, there is a normal variation in the effort expended during intercourse across individuals. Second, a stressful laboratory environment may artificially increase BP given the observation that laboratory experiments in men tend to report a higher peak SBP than ambulatory studies. Third, with advancing age, general fitness and health levels, frequency of regular sexual activity and effort of exertion change. It has been shown that sexual and cardiovascular pathology may be linked and may also influence the cardiovascular responses during sexual activity given the observation that younger persons tend to have higher peak BP than older persons during sexual activity. 55
One study by Bohlen and associates 6 recorded oxygen uptake (VO2) from men during intercourse, finding an average peak in VO2 of 11.7 ± 3.8 mL/kg/min for a short time during orgasm. This equates with a metabolic expenditure of 3.3 ± 1.08 METs, which is equal to a mild-moderate metabolic demand. This is comparable to activities such as very light jogging, light dancing, light yard work, tai-chi, walking at 4 kilometers per hour, or walking slowly up a flight of stairs. 54 This assertion has met criticism, however, because some authors regard it as an “oversimplification.” 56
In healthy able-bodied women, the literature reported a similar variability in cardiovascular parameters with an average peak SBP ranging from 120–136 mm Hg 29 –31,33,34 and average peak HR of 75–180 bpm. Similar to men, this range represents variation in the effort expended during intercourse across individuals. Similar to men, women tended to show a peak in BP occurring at orgasm, returning to baseline shortly afterward. In contrast to men, women tended to have lower peak SBP and HR than men during intercourse, which may represent lower average resting BP values in women.
In able-bodied persons, sexual activity normally results in mild to modest increases in BP and HR that rise during the excitement phase, peaking at or around the time of orgasm, and return to resting values shortly after. This is regardless of whether this activity is in the form of self-stimulation, foreplay, or intercourse. This is equivalent to 3–4 METS of metabolic demand.
Cardiovascular responses during sexual activity in persons with SCI
In contrast to able-bodied persons, cardiovascular responses to sexual activity follow a less predictable and more labile pattern in persons living with SCI. Individuals living with lesions at or above the T6 spinal level are predisposed to episodes of AD, 14 and sexual stimulation can be a potent trigger of this phenomenon. 57 The next section of this review will discuss changes in cardiovascular parameters during specific sexual stimuli in individuals with SCI.
Cardiovascular responses during self-stimulation in persons with SCI
The cardiovascular responses to self-stimulation in men and women living with SCI have been investigated. 35 –38 In one study performed by Sipski and colleagues, 35 45 men with a variety of SCI levels and completeness of injury were investigated using intermittent BP monitoring every 3 min during a self-stimulation protocol. For these individuals, it was reported there were no significant changes in either SBP or HR values as subjects progressed from the excitement, plateau, and orgasm phases measured with a visual scale of subjective arousal. None of the subjects described symptoms of AD in this study.
Using a similar protocol, with intermittent BP recordings, Sipski and coworkers 37 studied the cardiovascular responses to manual self-stimulation in 13 women with incomplete SCI above the T6 level. This group found nonsignificant, modest increases in SBP and HR with no person reporting typical AD symptoms during the study. Given previous findings that peak BP tends to dissipate within 1–2 min, and because intermittent BP measurements were being taken only every 3 min, it is possible that maximum peak BPs may have been missed during both of these studies, and consequently not reported.
Cardiovascular changes during intercourse in individuals with SCI
The literature did not report any home-based studies that directly measure BP and HR changes in response to sexual intercourse in persons with SCI. A case report by McBride and colleagues 40 measures an episode of severe AD and arrhythmia with a maximum SBP of 325 mm Hg in a man with long-standing tetraplegia in response to stimulation by his partner. Another more recent report describes AD in one subject who had its onset in response to sexual activity with a partner in the community. 23
These, other reports, and numerous anecdotal patient testimonials confirm that AD as the result of sexual activity occurs in the community. Bolstering the evidence of this, a survey of women with SCI conducted by Charlifue and coworkers 58 found that AD is an unwanted consequence of sexual activity in up to 27% of women living with SCI. Numerous studies including Anderson and associates 59,60 describe that AD during sexual activity is interpreted negatively by many individuals with SCI and can interfere with sexual activity. This report also highlights that the occurrence of AD during typical bladder or bowel care is a significant variable predicting the occurrence and distress of AD during sexual activity. In addition, AD can be asymptomatic in nature, 61 and it is likely that these surveys underestimate the number of persons living with SCI who have AD in response to sexual activity for this reason.
Cardiovascular responses during PVS procedures in persons with SCI
Vibrostimulation is a fertility procedure that involves placing a specially designed vibrating device on the glans penis with the ability to change the frequency and amplitude of the stimulus delivered to accomplish ejaculation. 43 In the literature, studies used comparable device settings proven to provoke ejaculation. 62 The duration of application of the device during these protocols differed slightly, ranging between 3- and 5-min intervals with multiple attempts if needed.
The main variation in technique reported in the studies reviewed was the BP monitoring equipment used and the frequency with which BP was measured. In the literature, the spectrum of BP monitoring was measurements taken as few as three times during the entire protocol to continuous beat-to-beat measurement (Table 2). This measurement variability results in a bias to the reported cardiovascular values observed during PVS.
The observed variability in the frequency of BP readings has an interesting consequence. Table 3 describes the average increase in SBP from baseline during PVS stratified by studies that used continuous versus intermittent monitoring. Those studies that monitor BP intermittently report average peak SBP of 40–50 mm Hg above baseline during procedures, 45 –47,63 whereas studies that monitor continuously reveal peak SBP of 65–107 mm Hg above baseline in individuals susceptible to AD. 23,42 –44,51
This discrepancy can be explained by the nature of SBP, which changes on a beat-to-beat basis, 43 and the nature of intermittent monitoring, which can miss the peak BP depending on whether the reading was observed just before, during, or after ejaculation. Studies using intermittent BP monitoring use an arm cuff that takes 30–45 sec to inflate, deflate, and report a reading. As a result, these studies are more likely to miss the peak in BP, which occurs for a short period at orgasm. In contrast, studies that measure BP using the continuous method (invasively or noninvasively) clearly have an advantage because they have the capability to document beat-by-beat BP changes and will not miss the largest increases in BP during orgasm that occur only for a very short time.
Because of measurement interval variability, the studies reported a wide variability of severity of AD during PVS procedures. The literature reported that an average peak of SBP during the PVS procedure could range between 123 mm Hg 46 to 210 mm Hg. 23 Likewise, the studies also describe a wide variety of HR responses, ranging from an average of 17.5 bpm reduction in HR below baseline during AD 41 to an increase of 13 bpm above baseline. 51 Individuals with injury at or above T6 were more likely to experience more severe episodes of AD during this procedure in all reviewed studies.
The variability in reported peak SBP in the literature has given rise to disagreement regarding how severe SBP increases during PVS can be. Studies performed by Courtois and colleagues 41,46,47 report an average peak SBPs of 156 mm Hg for individuals with cervical SCI. In contrast, studies performed by Brown and associates, 51 Ekland and coworkers, 44 Claydon and associates, 43 Sheel and colleagues, 42 and Elliott and Krassioukovet 23 that record BP continuously report a noticeably higher average peak SBP during PVS ranging from an increase of 10 mmHg up to 107 mm Hg above baseline. The only major difference between these experimental studies was the method of BP monitoring. Because of the variability in BP increases and the associated AD, first time use of PVS for men should be performed under clinical conditions to monitor the severity of the BP rise, irrespective of symptoms. 61
Limited data exist for the incidence of AD during vibrostimulation sperm retrieval trials in which vibrostimulation is less intense, and at home, where commercially available vibrostimulatory devices are used and are, again, less intense. 64 Likely, the incidence of AD in persons with SCI using commercially available vibrators would be less compared with that of PVS, because the intensity of the stimulus is less. Just how much less, however, is not known at this time.
Cardiovascular responses during electroejaculation procedures (EEP)
EEP is a procedure that requires the use of a rectal probe delivering current to the periprostatic nerves to induce an ejaculatory specimen. The procedure is used for fertility purposes in men with SCI. An early report of AD during EEP was published in 1974 when Frankel and coworkers 48 described uncontrolled hypertension brought on during an EEP. It has since been well accepted that this noxious, visceral stimulus can be a potent trigger of AD and associated arrhythmia, requiring cardiac monitoring and pre-treatment with antihypertensive medication. 50 For this reason, EEP is usually performed in a clinical setting or operating room where cardiovascular parameters can be closely monitored and medical assistance with BP applied as necessary.
Future Directions and Limitations
This review was meant to give the clinical community insight regarding what questions have yet to be answered in the area of cardiovascular responses during sexual activity in able-bodied and SCI populations. The studies in this review measure the cardiovascular response to sexual stimulation mainly within the laboratory setting. In this environment, the type, duration, and intensity of stimulation are held as constant as possible. This is in contrast to the community setting where the type, duration, and intensity of sexual play are not constant and vary from encounter to encounter and within each episode.
Also, in the home environment, there is a lack of clinical/environmental stress, but the assumption is there would be more emotional interplay in personal, private sexual practices. For persons with SCI, it is reported that AD does occur at home during sexual stimulation, and that AD can interfere with sexual pleasure after SCI 58 –60 ; however, the frequency and severity of this in the community has yet to be as well characterized as it has in the able-bodied literature. 33
This review has limitations. The studies reviewed examined a heterogeneous mix of persons living with SCI, and not all studies stratified results based on the level of injury. This could result in an underestimation of peak BP, because persons with higher level injuries tend to have the greatest increase in SBP during sexual activity. Also, the studies discussed use varied experimental methods that may have an impact on experimental results. This makes comparisons between studies challenging, except in the case of PVS procedures in men with SCI, where stimulation protocols were largely similar.
The measurement of BP during vibrostimulation in men and women with SCI is critical because sexual health clinicians cannot rely on the individual's self-report of AD signs and symptoms. This condition can occur and be very severe without the individual experiencing any ominous signs known as “silent AD.” 61
Based on the evidence provided in this review, it is recommended that continuous BP monitoring is chosen when planning PVS procedures because it is clear that intermittent BP monitoring can lead to an underestimation of true BP values. By monitoring BP closely, sexual health clinicians can avoid iatrogenic complications during PVS.
Of clinical importance is the presentation of the patient. In able-bodied persons, the onset of angina during sexual activity is a clear message to stop activity. In a study by Hellerstein and Friedman, 65 it was shown that in one third of the cardiovascular patients studied had ischemia, mostly silent, during intercourse. Further, the study showed that improved fitness consequent to exercise training resulted in a reduction in peak HR achieved during sexual activity. This has not been studied in the SCI population during sexual activity, although it is plausible that similar post-training findings may be seen given lower post-training submaximal HR during exertion known to occur in individuals with after an 8-week exercise program. 36,66
During sperm retrieval procedures, a careful monitor of the patient's symptoms is performed along with BP and HR monitoring. Most persons with SCI are very familiar with their symptoms of AD, which may, aside from the usual feelings of headache, be more typical of visceral information they have recognized over time to be AD. Symptoms should be elicited from the patient during any sperm retrieval or urological procedure. Clinicians should also watch for signs such as blotching skin or facial pallor, and goose bumps.
Many patients with SCI, however, especially over time, have lessened symptoms of AD or are even asymptomatic despite distinctly high BP readings. 61 This can lead to false reassurance of both the patient with SCI and the clinician that the cardiovascular effects of sperm retrieval are not of clinical importance. For private home use, those men and women with AD who have either symptomatic AD or are found to have silent AD can take precautionary measures to prevent the significant rise in BP by the use of antihypertensives before activity. This may include the use of prazosin 38,67 or nitroglycerin paste that can be wiped off 68 and in extreme cases, to have bite and chew nifedipine to use if BP does not reduce within minutes. 35,50,69
Conclusion
In able-bodied persons, sexual activity results in mild-modest increases in BP and HR equivalent to 3–4 METS of cardiac work. The demand of sexual activity is found to be within normal daily activities, and unless there is severe cardiovascular compromise, sexual activity is safe. If there is any question of this, a cardiologist should address further concerns.
Changes to cardiovascular parameters are less predictable in the SCI population and appear more dependent on both subject and stimulus factors than their able-bodied counterparts. Subjects with an injury level above the T6 spinal segment are vulnerable to severe episodes of AD in response to sexual stimulation. It appears, however, that less noxious methods of stimulation such as manual genital stimulation are less likely to cause severe episodes of AD. This is in contrast to vibrostimulation, or EEJ, which can trigger severe AD more frequently in susceptible individuals.
Both clinicians in the area of sexual medicine and researchers in the area of sexual health working with individuals living with SCI should aim to use continuous BP monitoring where possible to ensure that episodes of AD do not go undetected and promoting a false sense of security for cardiovascular safety. Developing steps to prevent or manage hypertension during sexual stimulation in this population presents an opportunity for individuals living with an SCI to participate in this fundamental human activity safely, while minimizing the unpleasant and often serious symptoms and signs of uncontrolled AD.
Footnotes
Author Disclosure Statement
This study was supported by grants from the BC Rehab Foundation Research and Innovation Fund and Rick Hansen Institute.