
Abstract
Rest is commonly prescribed following a mild traumatic brain injury (mTBI). There is concern that cognitive exertion by an acutely or sub-acutely injured brain may negatively alter outcome. The objective of this study was to determine if computerized cognitive testing in the emergency department alters symptom outcome from mTBI. Participants included 77 youth with mTBI who underwent computerized cognitive testing (mean age, 13.6; 95% confidence interval [CI] = 13.0–14.2) and were matched to 77 youth with mTBI who did not participate in cognitive testing (mean age, 13.5; 95% CI = 12.9–14.0). Participants who underwent cognitive testing did not differ from those who did not undergo acute cognitive testing on mean symptom ratings or the proportion who were not recovered at 7–10 days, 1 month, 2 months, or 3 months. There also was no difference in symptom outcome for those who underwent a shortened (four subtests, mean time = 16 min) or full-length (seven subtests, mean time = 28 min) version of the computerized test. Brief cognitive exertion using a computerized cognitive assessment after mTBI in youth does not result in worse symptoms at these follow-up periods, does not prolong symptom recovery, should not be considered contraindicated to recovery, and could be considered as another tool to aid in the management of these injuries. Further research with different samples is warranted.
Introduction
E
Rest following mTBI is based on the premise that cognitive exertion (any amount, whether brief or prolonged) may have pernicious consequences on recovery due to the physiological vulnerability created by a neurometabolic crisis 13 –15 and alterations in cerebral blood flow. 16 The American Academy of Pediatrics 7 advises that cognitive rest is needed “[t]o prevent exacerbation of the athlete's symptoms and allow for continued recovery.” Brown and colleagues 17 reported that engaging in normal levels of cognitive and academic activity (no limitations) post-mTBI is associated with longer time for symptom resolution (retrospectively recalled), compared with those who had reduced levels of activity (i.e., ranging from no activity to “significant cognitive activity”). Prescribing 7–10 days of rest, regardless of the duration of time since the mTBI, has resulted in improvements in cognitive performance and symptom reporting for slower-to-recover high school and college athletes. 18 –20
There also is some evidence that rest may not positively influence outcome after mTBI, particularly extended periods of rest. 21 –24 de Kruijk and colleagues 22 randomized adults with mTBI who presented to the emergency department (ED) into either no bed rest or full bed rest for 6 days. When following up at 2 weeks, 3 months, and 6 months post-injury, there were no differences in their ratings on a health survey. Gibson and colleagues 23 reported that rest in athletes (children, adolescents, and young adults) who sustained mTBI was not associated with a shortened duration of post-concussive symptoms. Thomas and colleagues 24 also suggested that prescribing 5 days of cognitive rest resulted in no benefit, compared with 1–2 days of rest for cognitive or balance testing, and in turn resulted in more symptoms being reported up to 10 days post-mTBI.
Although cognitive rest is a prudent recommendation following mTBI in children, a recent systematic review 12 suggests that the existing literature base is insufficient to fully support this recommendation. It may be that a moderate amount of cognitive activity is best for recovery, with no activity or full activity being problematic. When cognitive rest is recommended by healthcare clinicians, families will follow this advice to help minimize the duration needed for their child's recovery. As a result, they may be reluctant to engage in any activities that require intense cognitive exertion, including only short durations of cognitive exertion through brief cognitive testing in the ED. 25 There is recent evidence that computerized cognitive testing in the ED can detect early cognitive problems 26 and can help to prognosticate longer-term outcome 27 ; therefore, the benefits of cognitive testing need to be balanced with any potential adverse effects on recovery.
The objective of this study was to examine whether engaging in cognitive testing in the ED following mTBI would alter outcome. It was hypothesized that youth with mTBI who underwent cognitive testing in the ED, which requires a brief period of cognitive exertion, would have worse recovery, compared with those youth with mTBI who did not undergo cognitive testing in the ED.
Methods
Participants
Participants included children and adolescents who presented to the ED of a tertiary care pediatric hospital following mTBI. Inclusion criteria were 8–17 years of age, sustained an external force to head or body leading to neurological symptoms, at least one reported symptom attributed to the injury (e.g., dizziness, confusion, headache, balance issues, nausea), and a diagnosis of mTBI or concussion by the emergency physician. Exclusion criteria included loss of consciousness exceeding 30 min, Glasgow Coma Scale (GCS) score <13/15, abnormal neuroimaging attributed to the traumatic injury, suspected child abuse, alcohol or drug use at the time of injury, the administration of analgesics that can potentially alter cognition (e.g., codeine, morphine, ketamine), English as a second language, or an upper extremity injury that would have prevented responding on the computerized tests. Data collection was granted ethical clearance by the Conjoint Health Research Ethics Board.
Measures
The primary outcome measure was the Post-Concussion Symptom Inventory (PCSI). 28,29 The PCSI takes approximately 5 min to complete. The PCSI is a 26-item scale with somatic, cognitive, and emotional symptoms that often are reported following mTBI. Each symptom is rated on a 5-point scale of severity, ranging from “never” (0) to “almost always” (4; total severity score range = 0–104). Psychometric properties of the PCSI have been reported as adequate to strong 28 for this instrument that is recommended as a supplemental measure for the common data elements in pediatric TBI research. 30
Cognitive testing included the CNS Vital Signs computerized battery. 31 This battery is designed to rapidly screen cognitive abilities, has been normed for use in children and adults between 7–90 years, has adequate to high test–retest reliability in children and adolescents (Pearson's r = 0.63–0.82), has adequate concurrent validity with traditional paper-and-pencil measures, 31 and has been validated for use with children and adolescents with psychological disorders, 32,33 neurological disorders, 34,35 and in the ED following mTBI. 26,27 The first 50 participants completed a seven-subtest version, 31 but the remaining 27 participants completed a four-subtest version due to concerns with enrollment. 25 The seven subtests were: 1) verbal memory (i.e., recognition memory for words); 2) visual memory (i.e., recognition memory for designs); 3) symbol digit coding (i.e., visual-processing speed); 4) finger tapping (i.e., speeded fine motor speed in both the right and left hands); 5) Stroop (i.e., inhibition); 6) shifting attention (i.e., rapid mental flexibility); and 7) continuous performance test (i.e., sustained visual attention). The four-subtest version included verbal memory, finger tapping, Stroop, and shifting attention, which were selected based on having the highest effect sizes in a pediatric neurology sample. 35
Procedures
Participants were recruited and tested within the ED. After presenting to triage, eligible study participants were identified by research assistants who completed informed consent/assent. Parents completed the PCSI in the ED to indicate their child's baseline (pre-injury) level of functioning. Adolescents did not complete ratings of pre-injury functioning in the ED; therefore, any follow-up ratings were not included because of the potential for a “good old days” bias without true baseline ratings 36 and because parent and child ratings correlate strongly following mTBI (i.e., r = 0.65 between parent and adolescent PCSI ratings following mTBI). 28 Cognitive testing in the ED was introduced for the final phase of a larger study's data collection on epidemiological outcome from mTBI. 3 Cognitive testing was offered to all participants from this point forward, so those who agreed were not randomly assigned. Computerized cognitive testing was completed with the research assistant in a designated room in the ED. Due to the relatively higher level of noise within an ED environment, compared with a typical neuropsychological testing laboratory, all participants who participated in the cognitive testing wore noise-dampening ear muffs while being tested (3M Optime 105 Earmuff, Model H10B; noise reduction rating, 29 decibels). Follow-up ratings of post-concussive symptoms, which serve as an indicator of outcome and recovery from mTBI, 4,37,38 were completed over the phone using the PCSI as a semi-structured interview at 7–10 days, 1 month, 2 months, and 3 months post-injury.
Statistical analysis
Alpha was set a priori at p < 0.05 for all analyses and Cohen's d was used to examine the effect sizes (e.g., d ≥ 0.2 considered to be small, d ≥ 0.5 considered to be medium, and d ≥ 0.8 considered to be large). All statistical analyses were completed with the IBM Statistical Package for the Social Sciences (SPSS) version 19.0. 39
Comparisons of demographic and injury data across the groups were completed using analyses of variance (ANOVAs) for continuous variables and chi-square (χ2) tests for categorical variables. Groups were compared on the post-concussion symptom scores (dependent variable) using repeated measures multi-variate analyses of covariance (R-MANCOVAs) with baseline symptom ratings as the covariate. Interpretation of the R-MANCOVAs was dependent on equal covariance matrices (non-significant Box's M test) and the assumption of sphericity (if sphericity not assumed, interpretation used Greenhouse-Geisser). Pending a significant effect at the multi-variate level, group comparisons for each time-point (7–10 days, 1 month, 2 months, and 3 months) were completed using ANOVA when there was equal homogeneity of variance (non-significant Levene's test), but otherwise were completed using Mann-Whitney U tests if there was unequal homogeneity of variance (significant Levene's test).
The proportion of participants in each group who were deemed to have recovered at follow-up also was considered for this study. Examination of individual change over time was completed using reliable change calculations, 40 with values obtained from a prior study of PCSI scores with orthopedically-injured adolescents. 27 To compute change, the differences between each follow-up and the baseline total scores were computed using parent PCSI ratings (youth did not complete baseline ratings in the ED). Those youth with difference scores that exceeded the reliable change score (with an 80% confidence interval) were deemed to have not yet recovered. Those youth with a difference score that did not exceed the reliable change score (80% confidence interval) were deemed to have recovered. Comparisons of the proportions of recovered and not recovered for the two groups used chi-square analyses.
Results
Participants included 77 youth with mTBI who did not complete cognitive testing in the ED (“mTBI without cognitive testing”) and 77 youth with mTBI who completed cognitive testing (“mTBI with cognitive testing”; Table 1). Due to the close matching of the two groups based on pre-injury functioning, there were no significant differences in age (p = 0.72), sex (p = 1.0), family income (p = 0.96), past history of headaches (p = 0.83), number of prior concussions (p = 0.65), or pre-injury ratings of post-concussion symptoms (p = 0.17). With regard to injury factors (these were not matched), there were no significant differences in the presence of positive loss of consciousness (p = 0.79), the presence of positive post-traumatic amnesia (p = 0.43), acute pain ratings (p = 0.17), or the time between injury and triage (p = 0.41).
All group comparisons on sample and injury characteristics are p > 0.05.
mTBI, mild traumatic brain injury; CI, confidence interval.
Total parent-reported PCSI scores at baseline, 7–10 days, 1 month, 2 months, and 3 months post-injury are presented in Figure 1. Attrition rates for this study were minimal, with only 2.6% dropping out between the ED and the 3-month follow-up. There was no significant group difference in PCSI scores based on the length of cognitive testing (F[8.155, 380.582] = 1.41; p = 0.19), supporting that those who underwent either the seven-subtest (mean = 28 min, 95% confidence interval [CI] = 25.8–30.2) or the four-subtest (mean = 16 min; 95% CI = 13.7–18.3) versions of cognitive testing did not differ in their symptom outcome and subsequently could be grouped together for the analyses. When considering total parent PCSI scores at the four follow-up time-points (co-varying for baseline symptoms), there were not statistical differences between those who did and those who did not participate in cognitive testing (F[2.739,388.939] = 1.90; p = 0.14). Box's M was significant (p < 0.001) for the omnibus R-MANOVA, suggesting caution when interpreting these multi-variate results. Follow-up univariate comparisons at each time period also did not reveal groups differences in total parent PCSI scores at 7–10 days (F[1,152] = 0.09; p = 0.77), 1 month (Mann-Whitney U = 2918, Z = −0.08, p = 098], 2 months (F[1,147] = 0.33; p = 0.57), or 3 months (F[1,148] = 0.22; p = 0.64) post-injury. Effect sizes for comparisons of total parent PCSI scores between the two groups were small at 7–10 days (d = 0.02), 1 month (d = 0.05), 2 months (d = 0.12), and 3 months (d = 0.15) post-injury. Similar results of no significant group differences at the follow-up periods were found when considering the adolescents' self-reported PCSI scores (F[2.037, 414.729] = 2.10, p = 0.12).
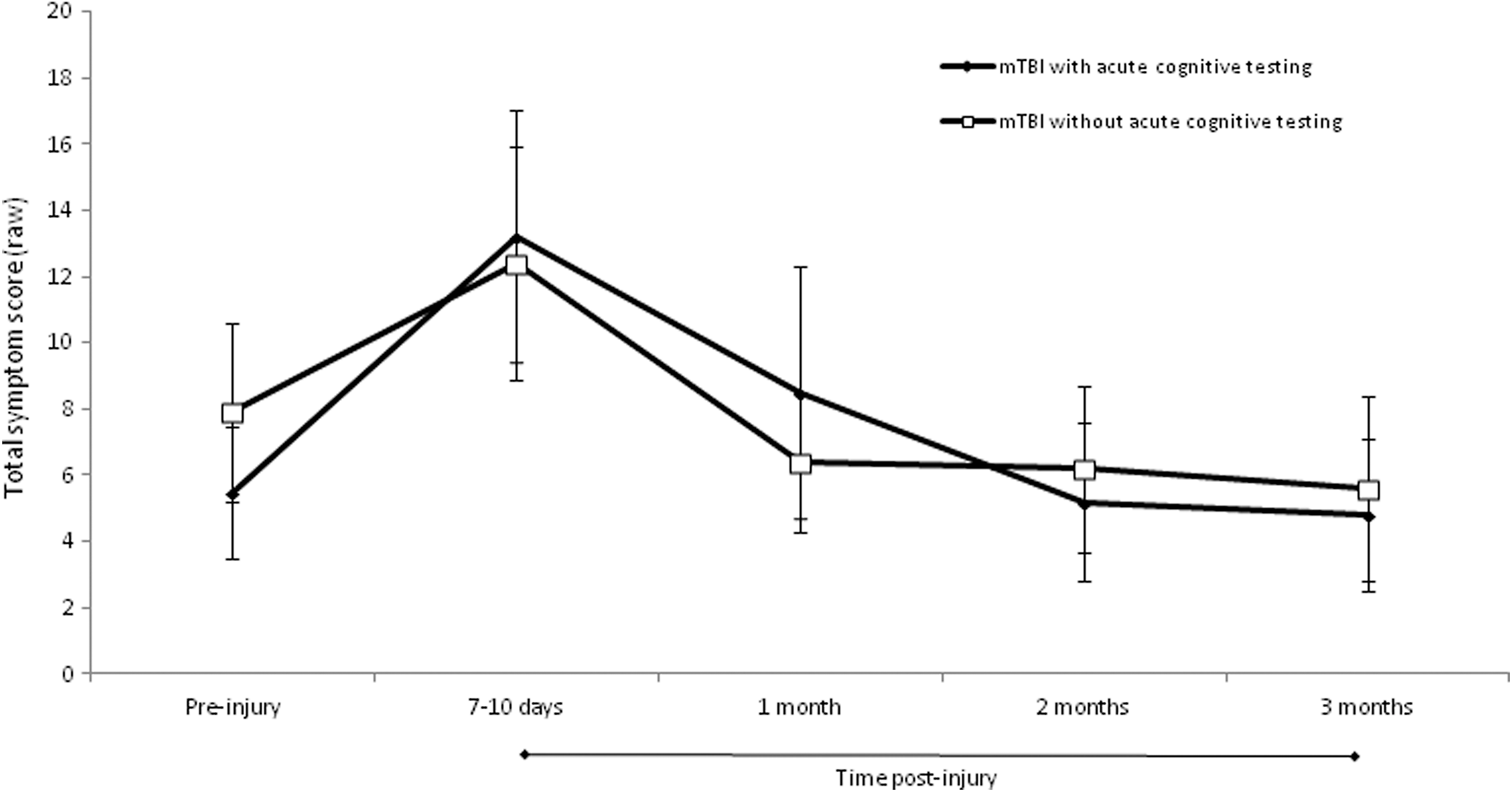
Ratings are obtained from parents. Error bars represent 95% confidence intervals for means. mTBI, mild traumatic brain injury.
Recovery on an individual basis also was considered using reliable change scores. 27 At 7–10 days post-injury, there was no significant difference between the two groups in the proportion who had recovered (i.e., symptom recovery was found in 73% of mTBI without cognitive testing and 68% of those with mTBI who did complete cognitive testing; χ2[1] = 0.21, p = 0.65). Similar results were found for the follow-ups at 1 month [i.e., 82% of mTBI without cognitive testing and 78% of mTBI with cognitive testing; χ2[1] = 0.01, p = 0.91], 2 months (i.e., 84% of mTBI without cognitive testing and 81% of mTBI with cognitive testing; χ2[1] = 0.54, p = 0.46), and 3 months (i.e., 86% of mTBI without cognitive testing and 82% of mTBI with cognitive testing; χ2[1] = 0.10, p = 0.76), where there were no significant differences in the proportions of participants who had recovered after their mTBI based on the presence or absence of cognitive testing in the ED.
Discussion
A substantial number of children and adolescents sustain mTBI each year, with cognitive rest being a common recommendation during early management. 6 –10 The nature and duration of cognitive rest is not well supported by research, 12 although some level of cognitive restriction may be prudent for a short period of time following an injury to a developing brain (i.e., the same may not apply regarding restrictions for physical activities or sports that put a child at risk of another injury). Engagement in a brief period of intense cognitive exertion sub-acutely after mTBI using computerized neuropsychological testing may be considered contradictory to the recommendation of cognitive rest, although this methodology has the potential to identify early deficits 26 and predict outcome following pediatric mTBI. 27 It is not known, however, if this level of cognitive exertion is contraindicated for recovery.
Participants who did or did not engage in computerized cognitive assessments while in the ED did not differ in their symptom outcome at 7–10 days, 1 month, 2 months, or 3 months post-mTBI. There were neither group differences in mean symptom scores nor differences in the proportion who were or were not still deemed symptomatic. The absence of a negative impact on symptomatic outcome held true for both the 16-min and a 28-min versions of the computerized test battery. To our knowledge, this is the first study to demonstrate that a brief computerized evaluation of cognition in the ED during the sub-acute recovery period following mTBI does not alter symptom outcome up to 3 months post-injury.
The results of this study have important implications for the assessment, management, and treatment of mTBI in children and adolescents. Following mTBI, it remains prudent to consider a reduction in physical and cognitive activities, to consider this reduction for only a brief period of time, to avoid 100% cessation of activities, to gradually increase activity as part of the recovery process, and to consider return to learn before return to play. 6,17 –20,23,24 However, the prevention of any period of brief cognitive exertion (i.e., computerized cognitive testing) is not supported from the perspective of worsening or protracting outcome. With the current study, it is not contraindicated to consider adding brief and focused cognitive testing acutely or sub-acutely after an injury as part of early management. This testing can rapidly evaluate brain functions, which can be used to determine the extent and type of cognitive disruption to the brain, monitor progress during recovery, and potentially prognosticate outcome.
There are some limitations to this study. First, this study cannot rule out a temporary worsening of symptoms immediately following the brief cognitive testing. That is, although symptoms did not differ by 7–10 days post-injury, it is possible that those who took the test had elevated symptoms immediately after testing. Second, outcome was defined based on symptoms only. It is not known whether other markers of outcome, such as neuroimaging, would differ in those with or without sub-acute cognitive testing. Third, it is possible that those who agreed to do the testing were less severely injured and were likely to recover at the same rate regardless of cognitive testing. That is, it is possible that those who declined participating in the testing, which was about 75% with the longer battery and about 50% with the shorter battery, could have been adversely impacted by the testing and could have taken longer to recover. We do believe, however, that the current sample has a similar recovery trajectory to larger samples studied though the same ED. 3,4
Fourth, this sample consisted of those with the mildest TBIs based on severity indicators. It is unknown whether brief computerized testing would alter outcome in those with more substantial injuries (e.g., GCS of 13 or 14) or with positive neuroimaging findings. And fifth, we did not track their duration of rest, their time to return to activity, nor their time to return to academics, and we were not able to control for any treatments these participants may have engaged in during their recovery period. Further research will help to elucidate these limitations.
Despite limited and mixed empirical support, 12 rest remains a cornerstone recommendation for mTBI management in children and adolescents. 6 –11 Rest is prudent and cautious, particularly regarding physical rest from activities or sports that present a risk of another injury. However, this study supports that brief cognitive exertion through cognitive testing in the ED does not alter symptomatic recovery following mTBI in children and adolescents. Considering that computerized testing can characterize acute cognitive concerns 26 and may predict outcome, 27 further research is warranted to determine if this type of tool will help the management of mTBI in the emergency room. Children can participate in cognitive testing sub-acutely as part of early management and potential prognostication from mTBI without contraindication that their recovery will be delayed.
Footnotes
Acknowledgments
The authors thank the following people: Brenda Turley, BA (Hons) for coordinating this study, supervising students, and overseeing data collection; Janie Williamson, RN (manager, Pediatric Emergency Research Team, Alberta Children's Hospital), the Pediatric Emergency Medicine Research Assistant Program (PEMRAP) students, and (alphabetically) Peter Hong (University of Alberta), Basil Kadoura (McGill University), Aneesh Khetani (University of Calgary), Mariam Narous (University of Calgary), and Alex Scurfield (University of Victoria) for assistance with recruitment in the emergency department; Susan Crawford (Alberta Health Services) for database management; Rob Hrapchak (Sol Supply Ltd) for providing the noise-dampening ear muffs; the staff in the Alberta Children's Hospital emergency department; and the patients and families who agreed to participate in this study.
Funding for this study was provided by: the Pediatric Brain Injury Research Program (administered by the Alberta Children's Hospital Research Institute) awarded to Drs. Barlow and Brooks; summer studentships from the Canadian Institutes of Health Research training program (administered by the Alberta Children's Hospital Research Institute; the McCarthy Tetrault Award (administered by the Alberta Children's Hospital Research Institute) awarded to Dr. Brooks; in-kind test credits from the computerized test publisher (CNS Vital Signs); and in-kind support from the neurosciences program at Alberta Children's Hospital (Conny Betuzzi). None of the funding sources were involved in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Author Disclosure Statement
BLB receives royalities from Psychological Assessment Resources, Inc. for two pediatric tests (Child and Adolescent Memory Profile ™, Sherman and Brooks, 2015; Memory Validity Profile ™, Sherman and Brooks, 2016) and book royalties from Oxford University Press (Pediatric Forensic Neuropsychology, Sherman and Brooks, 2012). BLB received in-kind support from the computer test publisher (CNS Vital Signs) in the form of free test credits. BLB, AM, and KMB are principal investigators, co-investigators, and/or collaborators on several grants relating to the study of mild TBI/concussion in youth. None of the authors have a financial interest in any of the measures in this study.