
Abstract
People who suffer a traumatic spinal cord injury (SCI) are at increased risk for developing dermatological complications. These conditions increase cost of care, incidence of rehospitalization, and the risk for developing other infections. The consequences of dermatological complications after SCI are likely exacerbated further by post-injury deficits in neural-immune signaling. Indeed, a functional immune system is essential for optimal host defense and tissue repair. Here, we tested the hypothesis that SCI at high spinal levels, which causes systemic immune suppression, would suppress cutaneous inflammation below the level of injury. C57BL/6 mice received an SCI (T3 spinal level) or sham injury; then one day later complete Freund's adjuvant (CFA) was injected subcutaneously below the injury level. Inflammation was quantified by injecting mice with V-Sense, a perfluorocarbon (PFC) tracer that selectively labels macrophages, followed by in vivo imaging. The total radiant efficiency, which is proportional to the number of macrophages, was measured over a 4-day period at the site of CFA injection. Fluorescent in vivo imaging revealed that throughout the analysis period, the macrophage reaction in SCI mice was reduced ∼50% compared with sham-injured mice. Radiant efficiency data were confirmed using magnetic resonance imaging (MRI), and together the data indicate that SCI significantly impairs subcutaneous inflammation. Future studies should determine whether enhancing local inflammation or boosting systemic immune function can improve the rate or efficiency of cutaneous wound healing in individuals with SCI. Doing so also could limit wound infections or secondary complications of impaired healing after SCI.
Introduction
T
Dermatological complications likely develop more frequently after SCI for many reasons. For example, after injury, as blood is redistributed to vital organs such as the heart and brain, the skin becomes more vulnerable to tissue hypoxia. 16 Cutaneous hypoxia promotes microbial activity and antagonizes endogenous wound healing cascades, perhaps explaining why wound healing is impaired in SCI patients compared with able-bodied individuals. 4 Effective wound healing also requires a functional immune system. 16 –20 After SCI, denervation of skin below the level of injury could impair neurogenic inflammation, 21 where neuropeptides released from nerve terminals regulate blood flow, vascular permeability, and local inflammation. 22,23 SCI also causes spinal cord injury-induced immune depression syndrome (SCI-IDS), 24,25 a systems-wide deficit in immune surveillance. SCI-IDS is characterized by persistent splenic atrophy, 26,27 leukopenia, 25 reduced anti-microbial activity in myeloid cells, 28 impaired humoral immunity, 26,27,29 depressed hematopoiesis, 30 and impaired lytic activity in T and NK cells. 31 These immunological deficiencies impair anti-viral and anti-bacterial immunity, thereby increasing the incidence and severity of systemic infections, notably pneumonia. 32,33 Whether SCI-IDS predisposes individuals to skin infections or exacerbates impaired wound healing is not known.
A goal of this study was to test the hypothesis that SCI impairs leukocyte recruitment, macrophages in particular, to sites of cutaneous inflammation. Indeed, macrophages are essential for cutaneous wound healing. 34 –36 Also, in SCI patients, particularly those with pressure sores that do not heal, expression of cell adhesion molecules (CAMs) needed to recruit leukocytes to sites of inflammation is reduced. 31,37,38 Rather than monitor inflammation using traditional histological or biochemical techniques, which are labor-intensive and require static measurements from multiple animals over time, 39 we tested a novel in vivo imaging technique that incorporates perflourocarbon (PFC) contrast agents. 40 –43 PFC emulsions are preferentially taken up by macrophages 42 and the 19F signal is proportional to macrophage density at the site of inflammation. 39,40 Moreover, the 19F signal can be quantified using either fluorescent imaging (e.g., in vivo imaging system [IVIS]) or magnetic resonance imaging (MRI). 44 –47 In this article, using both MRI and fluorescent imaging, we show that subcutaneous inflammation is significantly impaired after SCI. These data reveal a potential mechanism underlying delayed wound healing and increased risk for dermatological complications after SCI.
Methods
Animals
Adult C57BL/6 female mice (13–14 weeks old; 17–21 g) were purchased from The Jackson Laboratory (Bar Harbor, ME), then were randomly placed into cages (4–5 mice/cage) to acclimate to the laboratory environment. Animals were kept on a 12:12 light/dark cycle and group-housed in a barrier facility. At the time of surgery, mice were randomly picked from cages, then were alternately assigned into either injury or sham-injury groups. All procedures were performed according to The Ohio State University's Institutional Laboratory Animal Care and Use Committee. Mice received a high-thoracic complete spinal transection injury. Briefly, mice were anesthetized with an intraperitoneal injection of ketamine (120 mg/kg) and xylazine (10 mg/kg), then were given prophylactic antibiotics (5 mg/kg, s.c.; Gentocin®). Hair was removed using an electric shaver at the level of injury and at the site of CFA to minimize interference during fluorescence imaging. Using aseptic technique, a partial laminectomy was performed at vertebral level T3–T4, after which the spinal cord was cut using spring scissors. Suction was used to confirm complete separation of the rostral/caudal ends of the transected spinal cord. After surgery, muscle and skin were sutured and mice were injected with saline (2 mL, s.c.). Bladders were voided twice daily throughout the duration of the experiment and animals received daily injections of saline and antibiotic (5 mg/kg, s.c.; Gentocin). Animals were housed on cage warmers at 32°C throughout the study to maintain body temperature.
Induction of localized skin inflammation
To induce localized skin inflammation, emulsions of complete Freund's adjuvant (CFA; BD Difco, Lawrence, KS) containing 0.5 mg/mL Mycobacterium tuberculosis were prepared in a 1:1 mixture with sterile phosphate-buffered saline (PBS), then were injected (s.c.) on each flank (100 μL total/mouse). Injections were made into anesthetized mice at 1-day post-spinal cord injury (dpi). Anesthesia was induced in a Plexiglas® anesthesia box using isofluorane (4%), then mice were maintained at 1.5% isofluorane until injections were completed. After CFA administration, mice were handled for 30 sec, then returned to their home cages.
Contrast agent for inflammatory reaction
V-Sense VS-1000H DM NIR (Celsense, Inc., Pittsburgh, PA), a dual probe for MRI (19F) and fluorescence imaging (excitation max 750 nm, emission max 780 nm), was used to label macrophages in situ. A single tail-vein injection of V-Sense (170 μL) was made into SCI and control mice 18 h after CFA injection.
IVIS fluorescent imaging
Mice were anesthetized and imaged five times during this study starting at 3 h post-V-Sense injection (or 21 h post-adjuvant injection). Imaging was performed using an IVIS LUMINA II system (Caliper Life Sciences, Hopkinton, MA) with 745 nm excitation and ICG emission filters to detect the fluorescently tagged V-Sense tracer. Images were collected for a 7.5 × 7.5 cm field of view, f/2 lens aperture, and medium pixel binning. A sequence of exposure times was selected for each animal, although the 2 sec exposure time was selected for analysis across all animals and time-points for normalization and to avoid overexposure. Mice were anesthetized in a clear Plexiglas anesthesia box (2.5% isoflurane), and then placed on non-fluorescent black paper on the imaging platform of an IVIS station. The imaging chamber was continuously infused with 1.5% of isoflurane and the platform was heated at 37°C during the course of imaging. Animals were imaged at 21, 24, 48, 72, and 96 h post-adjuvant injection. This time interval was chosen based on published data showing that monocytes infiltrate cutaneous wounds within 24 h with peak accumulation of wound macrophages evident at 3 days. 34,48
Data were analyzed with the Living Image® software (v.4.3.1, Caliper Life Sciences). The adaptive fluorescence background correction was selected and the image threshold was manually chosen so that only the adjuvant injection site was highlighted. All selected images were mapped to the same color scale, and then regions of interest (ROIs) were selected using the contour ROI tool. Total radiant efficiency (photons/sec)/(μW/cm2) was determined by the Living Image software for the selected ROIs, with radiant efficiency defined as the ratio of emitted light (photons/sec/cm2/steradians) to excited light (μW/cm2). This measure uses calibrated units to compensate for non-uniform excitation light patterns. For this analysis, it was impossible to remain blind to group designation because SCI animals were obviously paralyzed. However, analysis of fluorescent signal in each animal was unbiased because ROIs were determined using a single color scale and generated automatically by Living Image software.
Magnetic resonance imaging
Imaging was performed at 48 and 96 h after CFA injection using a Bruker BioSpin 94/30 magnet (Bruker BioSpin Co., Billerica, MA) equipped with a 72 mm diameter volume coil tunable to both 1H and 19F nuclei. Animals were anesthetized using isofluorane (3% in air for induction, followed by 0.75–1.5% in a mixture of 95% oxygen and 5% CO2). Respiration and body temperature were monitored using SA Instruments products (Stony Brook, NY). 19F scans were acquired using rapid acquisition with relaxation enhancement (RARE) sequence: repetition time [TR]/echo time [TE] = 1956/8 msec, RARE factor = 8, 40*40 mm field of view [FOV], 64 × 64 matrix, 2 mm slice thickness, 100 averages, scan time = 26 min, 5 sec. 1H anatomical scans were acquired over the same geometry (RARE sequence, TR/TE = 1200/7.5 msec, RARE factor = 4, 40*40 mm, 2 mm slice thickness, 256*256 matrix, 2 averages). Data were analyzed using the Voxel Tracker software (Celsense, Inc.) from manually defined ROIs.
Tissue processing and ex vivo analysis
At 5 dpi, animals were anesthetized and then transcardially perfused with 0.1M PBS followed by ice-cold 4% paraformaldehyde in PBS. Spinal cords, spleens, and lungs were post-fixed for 2 h at 4°C, transferred to 0.2M PBS at 4°C overnight, then cryopreserved in 30% sucrose/PBS at 4°C until tissues sank. For ex vivo analysis, tissues were placed intact on slides and imaged in the IVIS system. Images were collected for a 7.5 × 7.5 cm field of view, f/2 lens aperture, small pixel binning. A sequence of exposure times was selected for each animal, although a 20 sec exposure time was selected for analysis across all animals and time-points for normalization. Adaptive fluorescence background correction was selected, and all selected images were mapped to the same color scale. For spinal cords, an ROI was created with the software free draw tool and this same ROI was applied to all analyzed images. Total radiant efficiency (photons/sec)/(μW/cm2) was determined by the Living Image software for the defined ROI area.
Statistical analysis
All results are expressed as group mean ± standard error of the mean (SEM). Presented data are pooled from samples obtained in two independent experiments. For experiment 1, group sizes were n = 4/group. For experiment 2, group sizes were n = 4 (laminectomy [Lam]) and n = 5 (SCI). For experiment 1, one animal in the Lam group was excluded from all image analyses because of abnormally low V-Sense signal. For experiment 2, one animal in each group died during imaging at the 48 h time-point, likely due to anesthesia complications; however, all preceding data acquired from these animals were used in the final analysis. For logistical reasons (e.g., access to MRI or IVIS), not all mice were imaged at all time-points in experiment 1. This created unbalanced group sizes at each of the time-points and required that we pool data from individual experiments. We then analyzed using a mixed effect model, incorporating repeated measures across time for each mouse. The model included group (SCI or Lam) and time post-adjuvant as two fixed factors and mouse as a random factor, allowing the baseline of each mouse to serve as its own control. 49 In this model, the interaction term, group × time, enabled us to compare the difference between two groups at each time-point. Holm's method was used to adjust the multiplicity to control the family-wise error rate at 0.05. 50
Data analyses were conducted using SAS 9.4 software (SAS, Inc., Cary, NC). Otherwise, group means were compared by two-sample t tests with significance set at p < 0.05 using GraphPad Prism v.5 (GraphPad Software Inc., San Diego, CA). All bar and category graphs were created in GraphPad. All images were generated in Adobe Photoshop CS5 v.12 (Adobe Systems Inc., San Jose, CA).
Results
Fluorescent in vivo imaging reveals attenuated subcutaneous inflammation after SCI
Skin inflammation was quantified as a function of time post-CFA injection in both SCI and sham-injured mice. Serial imaging was performed using an IVIS LUMINA II system (Fig. 1). Images taken from mice representing the group mean reveal a markedly reduced fluorescent signal in SCI mice relative to sham-injured mice at all times after CFA injection (Fig. 2A). Quantification of total radiant efficiency at the injection site reveals an ∼50% signal reduction in SCI animals (Fig. 2B,C). This difference is significant at each time-point, except 96 h (Fig. 2B), and also for the average of each animal across all time-points (Fig. 2C).

Experimental time line. MRI
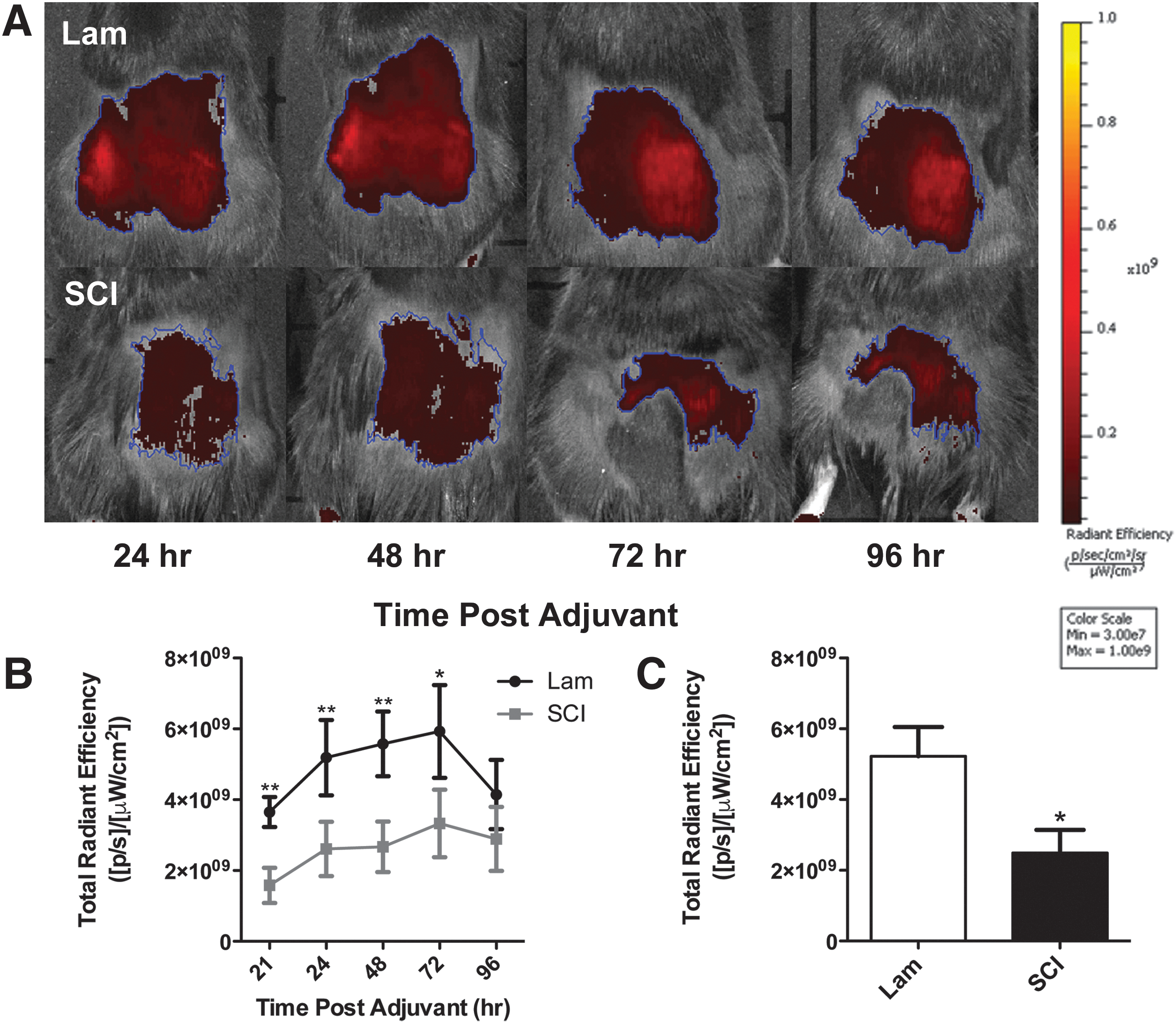
SCI suppresses subcutaneous inflammation.
Attenuated subcutaneous inflammation after SCI confirmed with in vivo MRI
Whole-body 1H/19F MRI analyses at 48 and 96 h after CFA injection show a significant reduction in inflammation in SCI mice at both time-points (Fig. 3). Sites of skin inflammation are easily distinguishable and in Figure 3A are denoted by white arrows on the dorsal surface of each animal. Reduced inflammation after SCI is obvious from images captured from animals representing the mean 19F MRI signal for each group. Quantification of injection-site total spin number using the Voxel Tracker software reveals that this SCI-dependent reduction is significant at both imaging times (Fig. 3B). Similar to the data obtained with IVIS imaging, the 19F MRI signal was reduced ∼50% in SCI animals relative to sham; however, only MRI revealed a significant difference between groups at 96 h. This discrepancy might be explained by the improved ability to detect labeled macrophages throughout the thickness of inflamed skin with three-dimensional (3D) MRI, whereas IVIS is limited to detection in two dimensions.
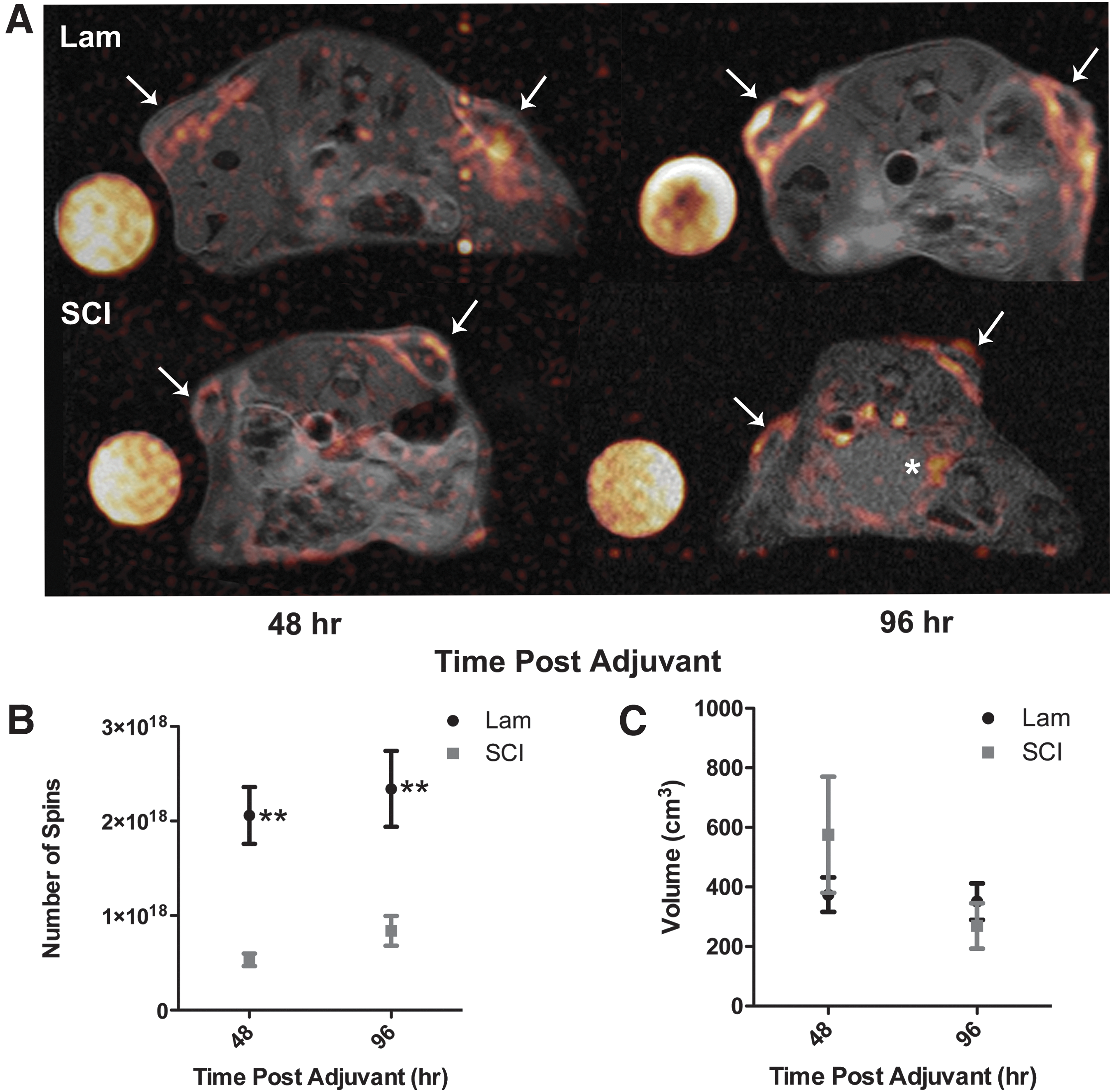
In vivo serial 1H/19F MRI analysis reveals attenuated subcutaneous inflammation after SCI.
To confirm that signal differences between groups were not caused by differences in the total volume of CFA injected (and retained) in each animal, the total volume of adjuvant signal was calculated for each animal from a 3D reconstruction of transverse sections through the thickness of the skin on the flank. CFA volume was constant between groups at either time-point (Fig. 3C); therefore, signal differences are due to differences in macrophage recruitment and not variable CFA delivery.
In vivo and ex vivo analysis of V-Sense signal reveals systemic and organ-specific inflammation after SCI
Although our experiment was not designed to quantify inflammation in other organs, V-Sense signal was detected in other organs using both MRI and IVIS imaging. For example, in a subset of SCI mice but never in sham-injured mice, inflammation was observed in/around the bladder (Fig. 3A, asterisk), although no gross signs of bladder infection were noted during daily bladder expression.
Ex vivo analysis of lung and spinal cord also showed obvious signs of inflammation. Similar to the bladder, lung inflammation was variable and although there was a trend for higher fluorescent signal in the lungs of SCI mice, small group sizes and high inter-animal variability precluded detection of significant inter-group differences (data not shown). Clearance of PFC emulsions from the body occurs through the reticuloendothelial system and weakly through the lungs, so this may also contribute to inter-animal variability. 51 Conversely, the intense focal intraspinal inflammation caused by SCI was easily detected by ex vivo IVIS imaging (Fig. 4). These data highlight the utility of these imaging modalities for screening for systemic and organ-specific inflammation. They also confirm that the reduced subcutaneous V-Sense signal in SCI mice relative to sham mice is a result of impaired cell recruitment and cellular inflammation and is not the result of impaired tracer uptake by macrophages or poor circulation in SCI mice.
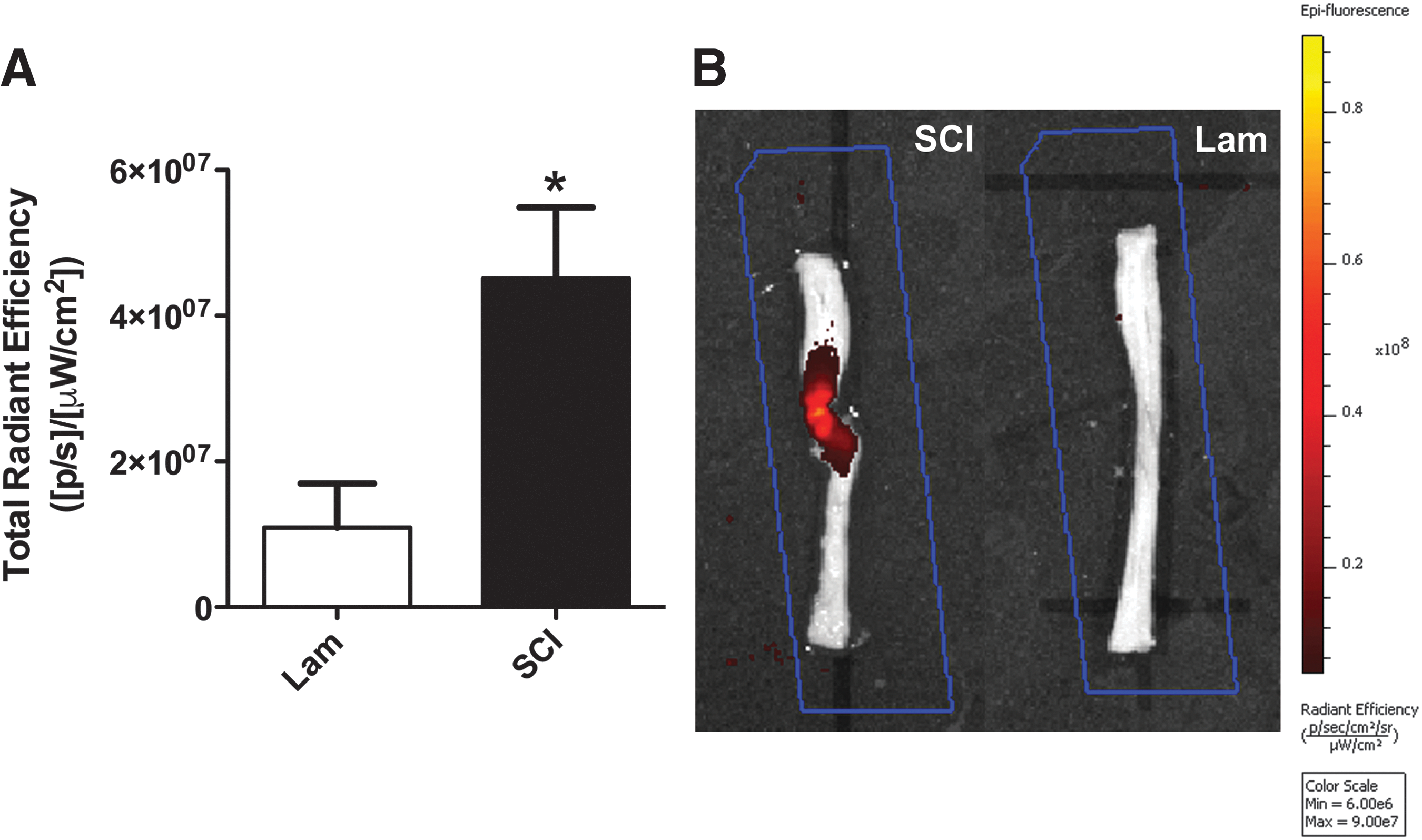
Ex vivo analysis (IVIS) of fluorescent signal in injured and sham/control spinal cords at 5 dpi reveals higher inflammation in injured cords.
Discussion
To date, few studies have evaluated the effects of experimental SCI on cutaneous immunity. 21,52 Novel data in the current report show definitive time-dependent changes in macrophage recruitment to the inflamed skin below the level of SCI. Specifically, serial in vivo imaging techniques show that macrophage recruitment to sites of cutaneous inflammation is suppressed by ∼50% as early as 2 days after SCI, with persistent deficits evident until at least 5 dpi (Fig. 3). Macrophages are potent anti-microbial effector cells and are essential for cutaneous wound healing. 34 –36 As such, these data could help to explain why after SCI there is a higher incidence of wound infection with slower or inefficient wound healing.
Previous publications from our lab and others show that SCI causes SCI-IDS, a system-wide deficit in immune cell survival and function. 24,25 Indeed, significant splenocyte apoptosis occurs as early as 3 dpi 26,27 and the spleen is a primary source from which monocytes (macrophage precursors) are mobilized after SCI. 53 As such, reduced cutaneous inflammation and impaired wound healing could represent a new and previously undefined clinical manifestation or by-product of SCI-IDS. Because wound infections and pressure sores negatively affect neurological outcome and increase patient morbidity and mortality, 8,10,12,15 treatments that improve inflammatory cell recruitment to the compromised skin could greatly improve quality of life after SCI. Many therapeutics currently used in the context of wound healing and skin infections, such as Medihoney®, silver-impregnated dressings, and anti-fungal creams, are designed to supplement the host immune system; however, these interventions are used inconsistently and the data reporting their efficacy are inconclusive. 2,54 –56 It may be possible to increase the skin's immune response directly using drugs designed to reverse or block SCI-induced suppression of systemic immunity, such as glucocorticoid receptor and beta-2-adrenergic receptor antagonists. 27,57 However, simply boosting cellularity may not be enough because other factors including reduced cutaneous blood flow, impaired neurogenic inflammation, and reduced expression of cell adhesion molecules also likely contribute to deficits in cutaneous immunity and impaired wound healing. 16,21,37,38,58
Another goal of this article was to use whole-body imaging technology to generate quantitative unbiased measures of inflammation. We used a PFC emulsion to selectively label macrophages; then using two different in vivo imaging platforms, IVIS and MRI, we quantified the magnitude of cutaneous inflammation as a function of time after immune challenge in vivo. The magnitude of intraspinal inflammation (ex vivo) also was quantified. Both measures were achieved in a matter of hours, as compared with the days or weeks that are required for routine histological analyses. In addition to being more efficient than histological methods, IVIS/MRI imaging of inflammation also reduces user bias and requires fewer animals. MRI is particularly valued for its high spatial resolution within biological tissues. 40 However, in the field of in vivo 19F imaging, the reduced operating cost and scan times associated with whole-body fluorescent imaging (IVIS) offers unique advantages. For example, MRI scans require ∼1.5 h per mouse; similar IVIS measurements take ∼20 min for a complete cohort of mice. The similarities in data obtained from these two imaging modalities indicate that only IVIS fluorescent imaging is needed for in vivo analysis of inflammation, although important differences in sensitivity still exist between the two modalities with MRI capable of higher 3D resolution. This may explain discrepancies between the IVIS and MRI data at the 96 h time-point (see Figs. 2 and 3).
Limitations
A limitation of the present study is that the analyses were restricted to the acute post-injury phase (<5 dpi). This is relevant to the peri-operative period after SCI, and data in this report could explain why post-operative wound infections are three times more common in people with acute SCI than in patients undergoing elective spinal surgery. 5 However, the risk of pressure sore development increases as a function of time and most dermatological complications first develop ∼80 dpi. 2 –6 Immunological dysfunction is a chronic and possibly permanent consequence of SCI 27 –29,59 ; however, whether cutaneous inflammation is suppressed indefinitely and is causally linked to impaired healing has not been thoroughly studied. One report found that concentrations of inflammatory factors in chronic pressure ulcers in SCI patients were reduced when compared with concentrations measured in similar chronic lesions in non-injured subjects. 60 Thus, future studies should examine cutaneous inflammation at increasingly longer intervals post-SCI.
To elicit focal and reproducible zones of cutaneous inflammation after SCI, we injected CFA beneath the skin. Subcutaneous CFA elicits inflammation with leukocyte recruitment occurring over a time-course that is identical to that caused by skin infection or tissue injury. 34,61 CFA-induced inflammation also triggers many downstream cellular processes associated with the tissue formation stage of wound healing, including fibroblast proliferation and angiogenesis. 62 However, CFA-induced lesions are unlikely to mimic all aspects of chronic ischemic pressure sores or other infectious skin complications (e.g., fungal infections) that plague SCI patients. As such, future studies should incorporate other models of cutaneous injury and also consider the effects that the neurological level of injury or injury severity have on cutaneous inflammation and wound healing. Here, our analyses were limited to a single model of high-level (T3) SCI, but in humans the types of dermatological complications vary with the level of injury and the risk of developing dermatological complications (e.g., pressure sores) increases with more severe injuries. 1 –3,63
Conclusion
Data in this article reveal a significant reduction in subcutaneous macrophage infiltration after SCI, which may underlie a number of skin complications that become prevalent in SCI patient populations. Two separate in vivo imaging techniques, IVIS and MRI, confirm that this immune suppression persists throughout the first week post-injury. These non-biased imaging tools allow serial quantification of organ-specific inflammation and provide an alternative to time-consuming histological techniques, especially when magnitude of inflammation is the key outcome variable. Future studies are needed to reveal mechanisms responsible for impaired macrophage recruitment to skin after SCI. This will reveal whether new therapeutics may be developed to overcome these deficits in order to improve wound healing and limit infection associated with dermatological complications after SCI.
Footnotes
Acknowledgments
All images in this article were taken using the facilities in the Small Animal Imaging Core of the Dorothy M. Davis Heart & Lung Research Institute, The Ohio State University. We are grateful to Zhen Guan for his technical services, and to Randall Carpenter for his assistance with tissue collection. This study was supported by NIH R01NS047175 and R01NS083942 (PGP), the Ray W. Poppleton Endowment (PGP), NINDS Core Grant P30NS045758, and the HHMI Med-into Grad Scholars Fellowship (JMM).
Author Disclosure Statement
No competing financial interests exist.