
Abstract
Type II odontoid fractures represent the most common cervical spine injury in the elderly. The decision for surgical treatment is still controversial, particularly with regard to the elevated peri-operative risk attributed to frequent comorbidities and poor bone quality. The purpose of this study was to assess both short-term mortality and mid-term clinical and radiological outcome in the elderly. Between January 2007 and December 2015, 35 patients with type II odontoid process fractures who underwent posterior atlanto-axial instrumentation using a modified Goel-Harms technique were retrospectively analyzed and prospectively examined clinically and radiologically. Comorbidities, mortality, and length of intensive care unit (ICU) and hospital stay were determined, as were medical and surgical complications. Quality of life was measured using the EuroQol five dimensions (EQ-5D) and Short Form-36 (SF-36) questionnaires at final follow-up. Average age was 86.5 years. All patients had severe comorbidities pre-operatively. No in-hospital mortality was observed. Average length of hospital stay was 13.8 days and 2.0 days for the ICU. Three patients developed cardiopulmonary complications; one wound infection developed post-operatively. Mean follow-up was 22 months (range, 6–72 months). The quality of life measured by EQ-5D showed a good outcome (0.7 ± 0.1). All SF-36 domains were reduced in comparison to a representative group. Solid bony fusion could be achieved in all patients. Atlanto-axial fusion by using intra-operative spinal navigation is a safe and effective procedure in the elderly, with few complications and preservation of favorable post-operative quality of life. The overall major complication rate was 11%. Surgery in the very old should be considered as first-choice treatment.
Introduction
O
Treatment of odontoid type II fractures poses a great challenge in elderly patients due to multiple clinical comorbidities and an often poor nutritive state, which can influence treatment risk. However, only little is known about long-term clinical and radiological outcome of nonsurgically or surgically treated elderly patients and there is a lack of evidence in the literature as to whether nonsurgical or surgical management constitutes the better treatment strategy. 4,5 On the one hand, conservative treatment may result in nonunion and prolonged fracture instability, which can deteriorate the anatomy of the cervical spine and cause new neurological deficits and complicate secondary surgery. 6 Conservative halo-vest immobilization itself is associated with a heightened mortality due to cardiopulmonary failure or pneumonia, which is reported in up to 42% of cases with an overall complication rate of 66%. 7 –10 On the other hand, surgery involves a high peri-operative risk due to often multiple comorbidities, with a mortality rate of 19.2% and an overall complication rate of 27 %. 11
Little is known about long-term clinical and radiological outcome in elderly patients, either nonsurgically or surgically treated. Whether these patients can return to their previous environment or previous level of independence still remains unclear.
However, different surgical techniques have been developed over the past decades for the treatment of odontoid type II fractures and many factors should be taken into account when elderly patients are involved. The surgical trend is towards posterior C1 lateral mass and C2 pedicle screw placement. The so-called Goel-Harms technique has become the technique most commonly employed at many institutions worldwide. 12,13 Despite its advantages, this technique has its down side as well, especially in the elderly. During the preparation of the C1/C2 lateral mass, troublesome bleeding from the epidural venous plexus can be provoked, leading to hemodynamic instability in the elderly because they have fewer compensation possibilities than younger patients. 8,14 Additionally, the C2 nerve root must be distracted downwards, which can induce occipital neuralgia. 15,16 Surgical techniques for posterior stabilization of odontoid type II fractures in the elderly are technically more challenging, but rapid mobilization is of utmost importance.
High screw failure, nonunion rates in osteoporotic bone, and high risk of peri-operative complications such as dysphagia and pneumonia constitute arguments against the anterior screw fixation in elderly patients, 17,18 which also matches our in-house experience of anterior screw fixation in elderly patients. Therefore, posterior atlanto-axial fusion was principally performed in all elderly patients with odontoid fractures. Here, we present a retrospective study from a prospective database of 35 patients older than 80 who underwent posterior atlanto-axial stabilization using a navigation-assisted, modified Goel-Harms technique at our Level I trauma center where we have gained 8 years of experience using the technique.
Therefore, the aim of this study was to evaluate the peri-operative safety, short- and long-term mortality, and mid-term clinical, functional, and radiological follow-up in elderly patients with type II odontoid process fractures.
Methods
Following local ethics committee approval and patient consent, 35 patients who suffered confirmed, unstable odontoid type II fractures between January 2007 and December 2015 were retrospectively studied based on a prospectively maintained database at one Level I trauma center. Additional inclusion criteria included an age of 80 and older, the absence of neurological deficits, the absence of accompanying injuries, and of primary importance, no previous fracture treatment. The average age at surgery was 86.5 years (range, 80–96 years).
The pre-operative diagnosis was made on the basis of thin-layer computed tomography (CT) to determine the bony anatomy, CT angiography to exclude anatomical abnormalities or kinking in the course of the vertebral artery, and magnetic resonance imaging of the cervical spine to assess ligamentous involvement and spinal cord status. To estimate vertebral bone integrity, mean Hounsfield units (HU) were measured in three axial planes of interest in each vertebra for C1-C7 according to Schreiber and colleagues. 19 Yoganandan and colleagues reported vertebral bone density in the cervical spine to be significantly higher than in its lumbar counterpart. 20,21 As vertebral density below 120 HU can be considered osteopenic in the lumbar vertebral bodies, this cut-off point can safely be used to distinguish osteopenic patients from patients with normal bone density. 22 In this study, all 35 patients showed osteopenic bone density.
All patients underwent posterior C1/2 fusion using our modified technique based on CT-guided navigation. At our department, unstable odontoid fractures in the elderly are exclusively treated by posterior atlanto-axial stabilization. Surgery was performed by two surgeons at one institution.
Of 35 patients included in our study, 25 patients were available for mid-term follow-up and five died during follow-up periods. Patients were followed up for an average of 22 months (range, 6–72 months).
A routine clinical and radiological follow-up examination was performed before discharge from hospital, as well as 6 months and yearly after surgery.
Surgical technique and implants used in the study
For the posterior C1/C2 fusion technique, two polyaxial titanium alloy screw systems were used (Mountaineer OCT System, DepuySynthes, and Oasys cervical system, Stryker), with a diameter of 3.5 and 4.0 mm and variable length according to each patient's anatomy.
After inducing general anesthesia and peri-operative single-shot antibiotics, the patient was positioned prone with the head fixed using a radiolucent carbon Mayfield three-point head holder. Cervical alignment was verified under a lateral fluoroscopic view and the final position of the C1/C2 complex was optimized.
A standard midline posterior approach from the occiput to the C4 process with subperiosteal exposure of C1 and C2 was employed. To prevent bleeding from the epidural venous plexus along the C1/C2 facet joints, the C1/C2 complex and dorsal arch of the atlas were exposed laterally, but only up to the medial part of the C1/2 facet joints without visualizing the complete facet joint capsule in order to leave it intact. The C1 arch was exposed without manipulating the C2 nerve roots.
After that, navigation reference markers (MatrixNeuro 4 mm self-drilling screws; Synthes) were attached to the laminae and the spinous process. A minimum of three reference markers were needed to determine the exact geometric characteristics of the vertebral anatomy. For the posterior C1/2 stabilization, four reference markers were inserted in all patients. An intra-operative CT scan (Siemens, CT Emotion, Sliding Gantry, Erlangen, Germany) was performed and the data were transferred to the navigation system (Fig. 1). Screw position, trajectory, length, and diameter were virtually determined after three-dimensional reconstruction of the new, imaged datasets (Fig. 2). A reference clamp was positioned at the lower spinous process under the area of fixation and the reference markers were merged with the CT scan of the cervical spine on the navigation system and defined as reference points. SpineMap 3D (Stryker Navigation System II with SpineMapTM 3D-Navigation, Kalamazoo, MI) navigation software was used. The inserted reference markers were registered to the navigation system by touching the markers using a tracked pointer. A point-to-point navigation was calculated. Correct location and mean deviation were validated by a navigated awl and anatomical landmarks. A calculated navigation accuracy of 0.3-0.8 mm was always given. Virtual drill paths were generated and adjusted to optimize screw placement (Fig. 2).

Intra-operative computer tomography (CT) with the head fixed using a radiolucent carbon Mayfield three-point head holder

Sagittal
Our modified entry point for the C1 lateral mass screws was at the junction of the lamina and superior-posterior part of the C1 lateral mass (Fig. 3) with an appropriate trajectory delineated by our spinal navigation. Due to a more lateral and superior-posterior position of the entry point, excessive epidural bleeding can be prevented and manipulation of the C2 nerve root can be avoided. In case of bleeding, nonsticking bipolar electrocautery (SuperGliss; Freiburg, Germany) was used to eliminate tissue sticking. To protect the vertebral artery, a blunt dissector was used under microscopic view to prepare the posterior C1 arch. Thereafter, our modified C1 entry point, located with the navigated awl, was marked with a 2-mm high-speed drill to prevent instrument slippage. The screw holes were created using a manually navigated 2.4-mm twist drill, which is fitted with a navigation tracker to guide drilling along the pre-selected trajectory up to the pre-determined insertion depth. A pedicle feeler was always used to check the integrity of the screw hole. Self-cutting polyaxial screws were inserted without the head of the screw pressing on the C1 posterior arch to avoid a conflict with the vertebral artery. The C2 screws also were inserted according to Harms’ technique in the pars of C2, lateral to the superior margin of the C2 lamina. 23 In case of narrow C2 pedicles (widths of less than 4 mm), we inserted C2 pars interarticularis screws with an entry point 3 mm superior and 3 mm lateral to the medial aspect of the C2/3 facet joint. This was indicated in four patients. After insertion of all four screws, an intra-operative CT was performed to verify screw placement (Fig. 4). Closure of the site and end of the operation followed. Patients were not required to wear a cervical collar post-operatively.
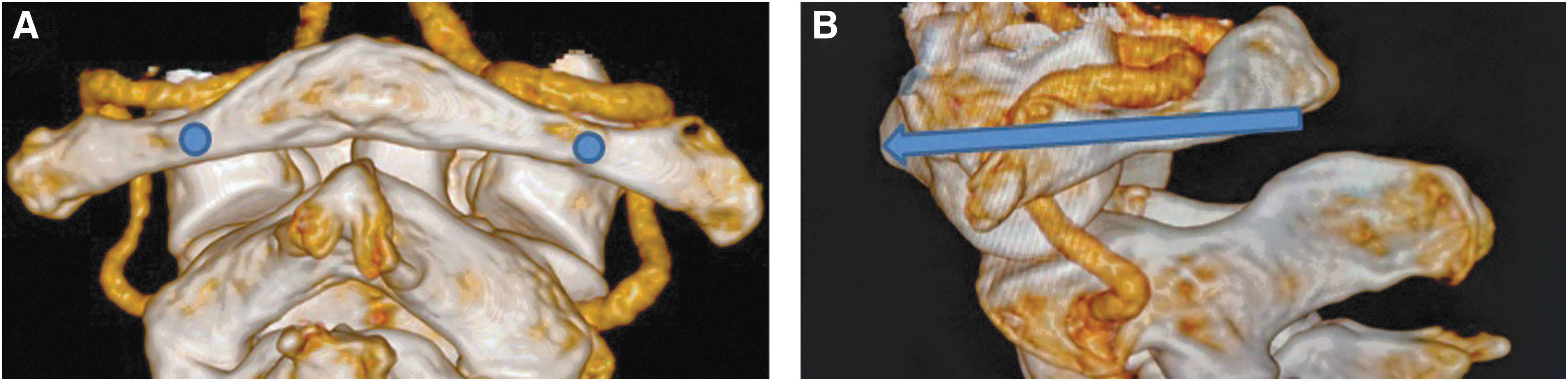
Three dimensional reconstruction of the upper cervical spine showing the course of the vertebral artery. The colored dots show the modified entry points of the C1 lateral mass screws
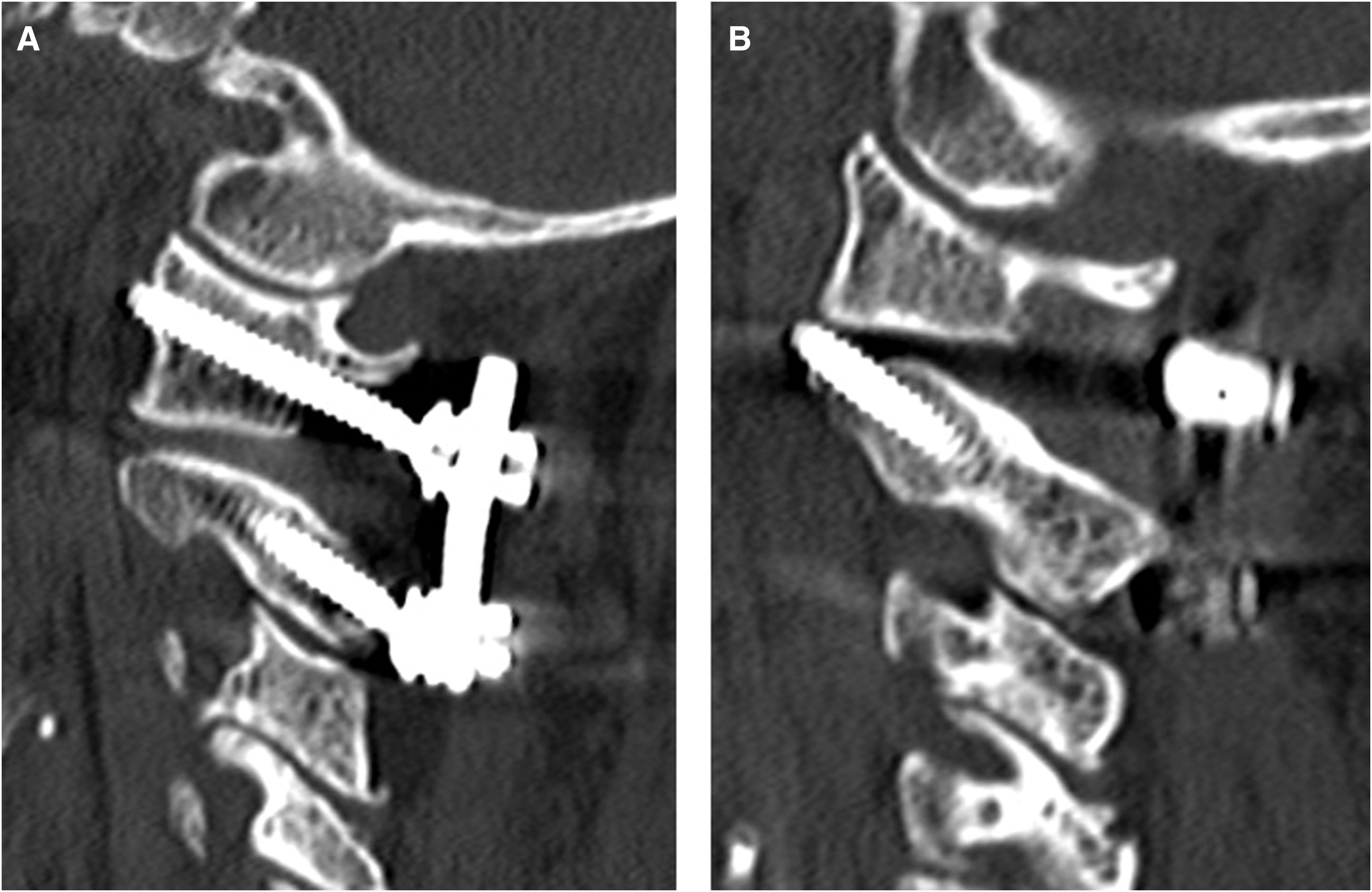
Intra-operative computed tomography control revealed correct screw placement for C1 lateral mass
Clinical outcome parameters
Study documentation was standardized and included validated outcome measures such as the EuroQol five-question broad questionnaire (EQ-5D-3L) 24 to measure quality of life index (0 = dead, 1 = perfect health) and the Short Form-36 Version 2 (SF-36v2), 25 which were determined at the last follow-up. Comorbidities were assessed pre-operatively on the basis of the age-adjusted Charlson Comorbidity Index (AACCI) 26,27 and rated according to the American Society of Anesthesiologists (ASA) score. 28,29 Numerous clinical parameters, such as body mass index (BMI), hospital stay, intensive care unit (ICU) stay, intra-operative blood loss, and necessity of blood transfusion, also were assessed. Intra- and post-operative complications and mortality rate were recorded. After discharge from the hospital, all patients completed a 14-day geriatric rehabilitation with the goal of returning the patient to a pre-injury quality of life. To measure the effect of the rehabilitation, the Barthel Index 30 was used to assess independence in activities of daily life before rehabilitation (14 days post-operatively) and after rehabilitation (30 days post-operatively).
Radiological outcome
Directly after the operation as well as at defined follow-up examinations, standard X-rays were performed in antero-posterior and lateral view to evaluate screw position and fusion rate. Post-operative, solid fusion was defined as the presence of a trabecular bony bridging assessed by an independent radiologist.
Endpoints
The 6-month mortality and clinical and radiological outcome were considered to be the primary endpoints. Mid-term clinical and radiological follow-up, as well as functional outcome, quality of life, and long-term mortality, were considered to be secondary endpoints of the study. Whenever necessary, cause and time of death were recorded. The assessment of long-term mortality, especially for patients who could not be reached, was based on secondary contact with the patient's family. Patients who were not able to visit our outpatient clinic were contacted by phone to determine whether there were any permanent complications related to surgery.
Statistical analysis
Data were carefully checked for consistency, outliers, and normality. Descriptive analysis was calculated for the entire cohort for each variable.
The Wilcoxon test for two related samples was used to determine a statistical difference across time in the same group. A p value of less than 5% was used to indicate a statistically significant difference. All analyses were done using SPSS 22 (SPSS, Munich, Germany). All data were statistically evaluated by an external independent statistician.
Results
Patient characteristics
A total of 35 patients met the inclusion criteria and were included in this study. The median follow-up was 22 months (range, 6–72 months).
The population comprises 17 men (49 %) and 18 women (51 %) with a median age of 86.5 years (range, 80–96 years) at the time of surgery (Table 1). Mean BMI was 25, representing normal weight status.
SD, standard deviation.
The age-adjusted Charlson Comorbidity Index score was calculated for each patient to classify comorbidity and grouped as having either no comorbidity (AACCI = 0), moderate comorbidity (AACCI = 1–5), or severe comorbidity (AACCI >6). All patients included in our study presented with at least three comorbidities with a mean AACCI value of 7.1 for the entire cohort, indicating severe comorbidity (Table 1). Comorbidities are summarized in Table 2.
Pre-operative narcotic-relevant ASA scoring revealed 26 patients with an ASA 3 score and nine patients with an ASA 4 score. Both ASA 3 and ASA 4 scores are associated with a heightened risk of peri-operative complications (Table 1).
No intra-operative complications developed in this patient series; in particular, no cortical screw breaches or vertebral artery injuries were seen. Excessive bleeding from the venous plexus did not occur during any operation. Blood transfusion during surgery was necessary in one patient due to a coagulation disorder, which was diagnosed post-operatively for the first time. The average intra-operative blood loss was 450 mL for all patients. No patient developed any new neurological deficits post-operatively. The average length of hospital stay was 13.8 days and 2 days for ICU. Except for one patient, all could be mobilized on day one after surgery.
Mortality
Five patients died during the follow-up period. One patient died 41 months after surgery as a result of plasmacytoma; another patient died 56 months after surgery of coronary heart disease. Two patients died 11 and 24 months after surgery, respectively, as a result of pneumonia. The fifth patient died 20 months after surgery as a result of a malignant middle cerebral artery infarction. All of the deceased patients had at least seven comorbidities and cause of death was not related to surgical treatment in any of these patients. Therefore, these study results indicate that short-term mortality rate is negligible when applying an optimal anesthesiological management and the described surgical technique. The overall mortality rate due to other comorbidities was 14%. Median time to death was 30 months (range, 11–56 months).
Clinical and functional characteristics
To evaluate the effect of geriatric rehabilitation, we evaluated the Barthel index (0-100 points) before discharge 2 weeks post-operatively and after rehabilitation 30 days post-operatively. At discharge from the hospital, the mean Barthel index was 46 points (severe dependence) and improved significantly to 70 points after rehabilitation (moderate dependence; p < 0.05), which clarified the importance of rehabilitation in the elderly. All patients stated that they were independent before trauma.
The analysis of the EQ-5D-3L index at final follow-up showed a median index score of 0.7 (SD 0.1). The maximum EQ-5D index score of 1.0, which is equal to perfect health, could not be achieved. In consideration of age and comorbidities, a median EQ-5D-3L index of 0.7 is more than satisfactory. In a comparison of the 5 sub-items of the EQ-5D questionnaire (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) at final follow-up to a representative sample of a noninstitutionalized population in Germany in the dimension of pain/discomfort and mobility (28% and 17 % of a representative German sample, 31 our data suggested similar results to the German population (30 % and 20 % in our study). None of the patients complained about anxiety/depression. With regard to the remaining sub-items, usual activities and self-care, we registered higher patient percentages than in the general German population (35% and 25% vs. 10% and 3%).
To assess functional outcome, the SF-36 questionnaire was used at the last follow-up and compared with a representative sample of a German population ages 80 years and older consisting of 13 males and 50 females. 32 In summary, none of the items were superior in our study group, but were very acceptable (Fig. 5; Table 3).
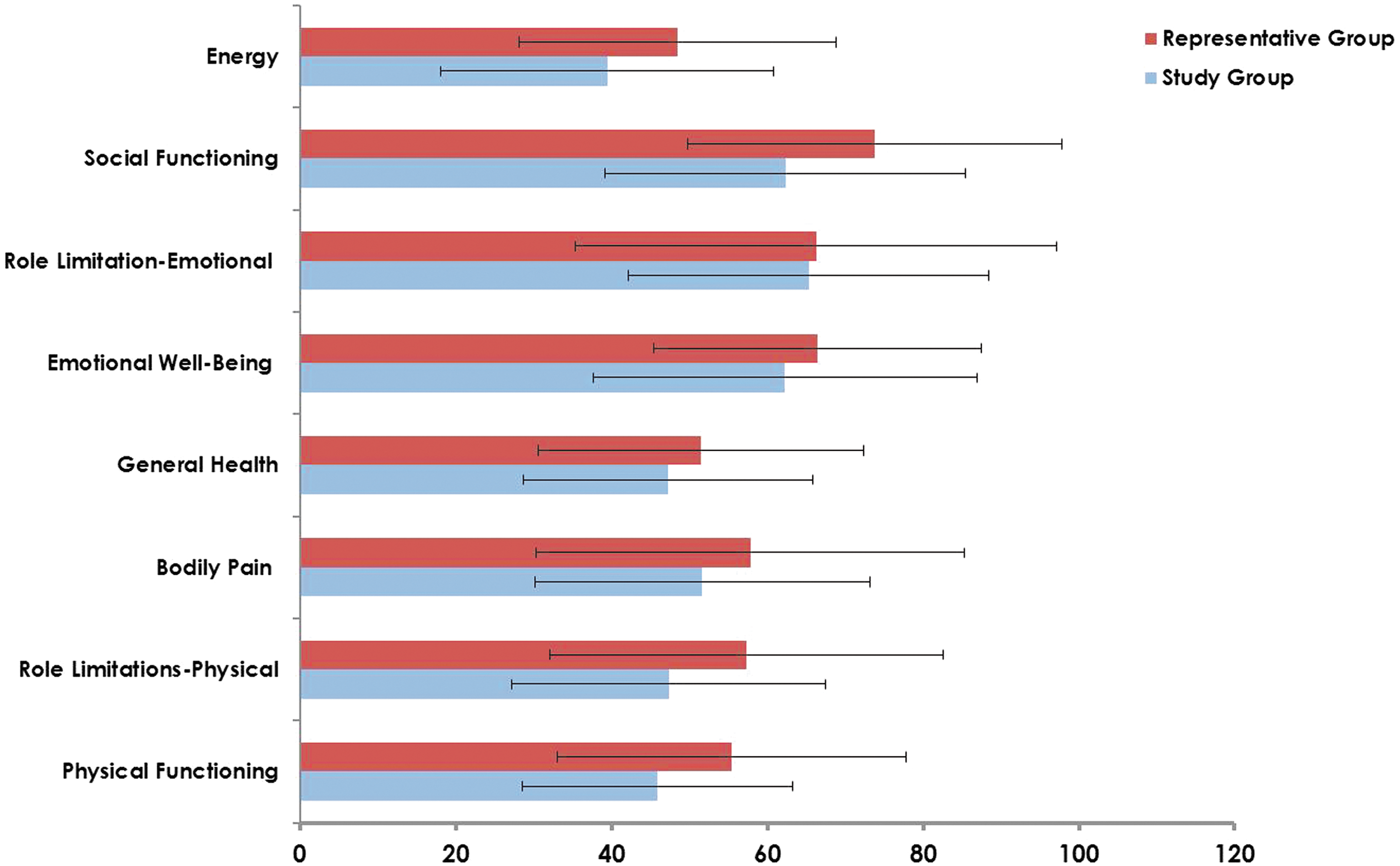
Bar charts demonstrating Short Form-36 Version 2 for the study group in comparison to a representative group. Mean value and standard deviation are given.
Numbers are given as mean values and standard deviation.
SF-36v2, Short Form-36 Version 2.
Radiographic results
Within two days after surgery, a standard x-ray in antero-posterior and lateral view showed correct screw placement. Proper alignment of the atlanto-axial spine was restored in all cases without alteration at the post-operative follow-up 6 months after surgery. No signs of screw loosening or migration were diagnosed. Fusion could be achieved in all patients by clearly visible continuous bony trabeculation and bone bridges connecting the atlas and axis at the last follow-up.
Complications
Four major complications occurred. One patient required surgical revision for wound infection during the early post-operative phase and was treated with antibiotics. Three patients developed transient cardiopulmonary complications (two pneumonia, one heart attack) after surgery. Therefore, the overall major complication rate was 11%.
Minor complications, which occurred in 29 % of cases, could be treated successfully using medication (Table 4). No patient suffered permanent complications.
Two patients had more than one complication. All patients recovered uneventfully.
Discussion
Cervical spine fractures are the most common spine fractures and have been shown to be significantly associated with increased morbidity and mortality in elderly patients. 33 Odontoid type II fractures are the most common isolated spinal fractures and are often a result of low-impact trauma. 34 The majority of these fractures are challenging to treat. 35 Despite previously published data for the treatment of odontoid type II fractures in the elderly, the optimal management for patients 80 years and above is still controversial and the quality of evidence ranged from very low to low with a lack of prospective studies. 36 The decision for early surgery is still under debate among spine surgeons, often in the same hospital. One reason for this may be that odontoid type II fractures in the elderly are partially correlated with high mortality regardless of the treatment option. This is especially due to lower physiological reserve, poor rehabilitation potential, and many comorbidities that affect the surgical outcome negatively. 37
However, when the decision for conservative treatment is made, an external immobilization is necessary. Several studies have shown a high mortality in the elderly with odontoid type II fractures who were either treated with a rigid collar or halo-vest immobilization. Due to the fact that patients were kept immobilized, mortality was mainly attributed to an increased risk of cardiopulmonary complications, such as pneumonia, pulmonary embolism, and cardiac arrest. 7,38 Early mortality has been described in 25% to 40% of cases. 14,39,40 Additionally, nonunion rates have been described to be as high as 35% to 85% after nonsurgical treatment. 41 Even with halo-vest immobilization, the nonfusion rate remains high due to inadequate reduction or insufficient stabilization and fracture displacement. 42 –44
Unstable odontoid fractures can be managed in two ways. The anterior screw fixation can be performed easily during a short operation and with minimal blood loss. This saves neck motion, with good results in young patients. 45 –47 Nevertheless, this technique has been linked to a high screw failure and nonunion rate in osteoporotic bone. 45 The second treatment option is posterior C1/C2 fixation, which is preferred by most surgeons in elderly patients and can be performed either as transarticular stabilization (Magerl) or by using polyaxial screws and rod fixation (Goel-Harms technique). 23,48 The Harms technique offers many advantages over other techniques, such as individual C1 lateral mass screw placement and C2 pedicle screws, which minimize the risk of vertebral artery injury in comparison to Magerls’ technique. However, one of the major drawbacks of the Harms technique is preparation and visualization of the lateral aspect of the C1 lateral masses located at the lateral border of the C1/C2 articulation. To determine the correct C1 entry point, the C1/C2 joint has to be exposed laterally and prepared fully to the depth, which can lead to excessive epidural bleeding from the venous plexus and therefore deteriorates the surgeon's view and complicates safe screw placement with extension of operation time. Especially in the elderly, a high blood loss is poorly tolerated and associated with an extended ICU stay and higher mortality. 11,49
Therefore, the outcomes of the operative intervention in odontoid type II fracture in the elderly is highly dependent on the technique used. In this study, we used a modified Goel-Harms technique under CT-guided navigation with the C1 entry point at the junction of the C1 posterior arch and superior-posterior part of the C1 lateral mass to prevent bleeding from the epidural venous plexus.
All patients older than 80 years admitted to our hospital with an unstable odontoid type II fracture were exclusively operated by posterior atlanto-axial stabilization. A high screw failure and nonunion rate in our department prompted us change our surgical strategy.
Comparison with the literature
One of the few prospective studies, and a level Il study regarding elderly patients with odontoid type II fractures, was published by Vaccaro and colleagues. 50 Here, 159 geriatric patients with odontoid type II fractures of which 101 had been surgically treated were enrolled. Surgery included one anterior and two posterior fusion techniques, demonstrating a 1-year mortality of 18% in the surgical group, which was lower than in the nonsurgical group (28%). Complications occurred in 30% versus 36% in the nonsurgical group and treatment-related deaths in 2% of cases during a follow-up period of one year. The authors concluded that surgical treatment produced a significant benefit with regard to clinical and radiological outcomes in comparison to nonsurgical treatment, but pointed to the issue that elderly patients with odontoid fractures will not regain their pre-injury level of function 50 ; in contrast to that, Platzer and colleagues 51 did not report any decline in the functional results of elderly patients who received surgery in the form of either anterior screw or posterior screw and rod fixation. To identify factors associated with success or failure in managing odontoid fractures in elderly patients, Fehlings and colleagues (2013) 52 published a further multi-center prospective study in the same year as Vaccaro and colleagues 50 based on the same patient cohort. In that study, failure was defined as death by any cause, decline in Neck Disability Index by more than 9.5 points, and occurrence of a major treatment-related complication. Of the 159 geriatric patients with odontoid type II fractures, 44 (27.7%) were categorized as treatment success, 86 (54.1%) as treatment failure, and 29 (18.2%) as withdrawn or lost to follow-up. The authors pointed out that older age, male sex, and initial nonsurgical treatment were associated with treatment failure. Based on these results, the authors suggested that initial conservative treatment was associated with a 2.92-fold higher risk of failure, compared with patients who had early surgery. The authors described several limitations of their study. Although the results were adjusted by confounding variables, there still might have been bias in the selection of patients by the surgeons. Further, the follow-up period of one year was deemed short. Another limitation might be that a minimum of six different surgical techniques were used in that study. The optimal surgical strategy, therefore, still remains unclear.
Based on a systematic literature review, Schroeder and colleagues 53 concluded that short- and long-term mortality was lower in patients who underwent surgical treatment, regardless of the type of surgery, than in nonsurgically treated patients and did not identify any increased risk of complications in patients who underwent surgery. This is consistent with results of Vaccaro and colleagues. 50
In a survey to assess complications of operative and nonoperative treatment for odontoid type II fractures in octogenarians, Smith and colleagues 54 carried out a retrospective study based on 72 patients, of whom 32 had been treated surgically (10 anterior, 22 posterior) and 40 nonsurgically. According to that study, the acute in-hospital mortality was 12.5% for the surgical group and 15% for the nonsurgical group. Here, at least one major complication developed in 62% of patients in the surgical group and 42% of patients in the nonsurgical group. 54
Aim and results of the study
To the best of our knowledge, this study represents, despite the small sample size, one of the largest studies in a more homogeneous patient group to investigate mid-term follow-up with clinical, functional, and radiological outcome in patients older than 80 years, that also addresses quality of life and long-term mortality. One of our primary goals was to investigate patient safety in terms of complication and reoperation rate.
Of the 35 included patients, 25 were available for mid-term follow-up, whereas five died over time. The five patients who were not available for final follow-up live in nursing homes and the lack of follow-up was related to the patient's difficulty to present to the clinic for clinical and radiological check-up. Most elderly patients rely on relatives’ support to present to the clinic, a fact that often complicates follow-up examinations.
All patients passed for the same post-treatment management visiting a rehabilitation center for 2 weeks specialized on elderly patients. Our clinical and radiological data revealed satisfactory results throughout the entire post-operative course. Neurological deficits did not occur post-operatively. Neurovascular complications, especially severe bleeding from the epidural venous plexus or injury of the vertebral artery, could be avoided in all patients. With the use of intra-operative CT-guided navigation, all screws were placed correctly and without difficulties by employing the described modified technique. Implant failures such as migration or loosening, which can often occur in osteoporotic bone, did not occur. The purpose of this study was not to demonstrate superiority of one technique over another, but rather to highlight alternative options for screw insertion in odontoid type II fractures made possible by the use of CT-guided point-to-point navigation, which has proven to be a highly reliable and helpful tool for safe screw placement at our department.
The overall survival was high in our study. We observed a 1-year mortality of 3 %, a 2-year mortality of 9 %, and a 5-year mortality of 14%, and therefore ranged below the mortality reported in most published studies. 3,36,50,53,55
Controversy
Summarizing the literature, including both large multi-center prospective studies and our results, there is a clear trend towards early surgical treatment in elderly patients with odontoid type II fractures. The best surgical strategy is not well addressed in the literature, but most authors prefer a posterior C1/C2 stabilization. 13,36,50,52 However, a consensus does exist that anterior screw fixation in elderly patients is associated with higher morbidity rates than posterior fusion procedures as a result of implant-related complications. 17,56 Nonsurgical treatment strategies, such as halo-vest or rigid cervical orthosis, correlate with significantly higher morbidity and mortality rates in elderly patients. 7,9,10,57 Further, patient compliance is poor. 38 Poor compliance can lead to high rates of nonunion, but the presence of osseous union should not be considered an outcome measurement tool for successful treatment. Radiological findings do not correlate with clinical and functional outcomes in odontoid fractures. 58 However, the relatively lower mortality and morbidity rate and a satisfying clinical and functional outcome in geriatric patients in whom posterior atlanto-axial fusion was performed, has prompted many spine surgeons worldwide to opt for early surgery.
Limitations of the study
Due to our good experience with favorable outcomes of primary surgical treatment in elderly patients, conservative treatment at our institution is rare. Therefore, no control-matched cohort group of conservatively treated patients was available. Although possibly unfavorable, SF-36v2 questionnaire results were compared with the general noninstitutionalized population older than 80 to address functional recovery from surgery.
Another limitation of this study is the follow-up period, with a mean follow-up of 22 months. However, this examination period is longer than in most published studies investigating the surgical treatment of odontoid fractures in the elderly. Routine follow-up CT images could not be obtained to precisely verify bone fusion or the ratio of fibrous fusion due to concerns of the ethics committee that this did not necessarily represent the standard of care. Large prospective randomized controlled studies are needed to underline our findings and to determine the optimal management of odontoid type II fractures in patients ages 80 years and older.
Conclusions
As the average life expectancy increases in the general population, spinal surgeons will be frequently confronted with odontoid fractures in the elderly. The results of this study show that our modified C1/2 posterior stabilization technique can be performed safely using intra-operative spinal navigation, with good clinical, functional, and radiological results and few complications in multi-morbid patients ages 80 years and older, demonstrating further that surgical treatment of odontoid type II fractures in octogenarians and nonagenarians does not negatively impact survival. In light of the results of this study and previous studies concerning nonsurgical treatment options, we believe that the mortality and complication rate of patients with odontoid type II fractures can be substantially reduced by deciding for surgical treatment. We hope that this study can contribute to building a consensus about the best treatment strategy to enable patients with odontoid type II fractures to return to their previous environment or previous level of independence.
Footnotes
Acknowledgments
The authors of this study would like to thank Sherryl Sundell for language editing and proofreading the manuscript.
Author Disclosure Statement
The study was undertaken as part of the department's internal quality reviewing process and therefore financed by the clinic's internal resources. Data collection and analysis for the current study were fully independent of any type of external financial support. No external funding was received by any of the authors or the institution.
No competing financial interests exist.