
Abstract
This review of the literature on traumatic brain injury (TBI) in older adults focuses on incident TBI sustained in older adulthood (“geriatric TBI”) rather than on the separate, but related, topic of older adults with a history of earlier-life TBI. We describe the epidemiology of geriatric TBI, the impact of comorbidities and pre-injury function on TBI risk and outcomes, diagnostic testing, management issues, outcomes, and critical directions for future research. The highest incidence of TBI-related emergency department visits, hospitalizations, and deaths occur in older adults. Higher morbidity and mortality rates among older versus younger individuals with TBI may contribute to an assumption of futility about aggressive management of geriatric TBI. However, many older adults with TBI respond well to aggressive management and rehabilitation, suggesting that chronological age and TBI severity alone are inadequate prognostic markers. Yet there are few geriatric-specific TBI guidelines to assist with complex management decisions, and TBI prognostic models do not perform optimally in this population. Major barriers in management of geriatric TBI include under-representation of older adults in TBI research, lack of systematic measurement of pre-injury health that may be a better predictor of outcome and response to treatment than age and TBI severity alone, and lack of geriatric-specific TBI common data elements (CDEs). This review highlights the urgent need to develop more age-inclusive TBI research protocols, geriatric TBI CDEs, geriatric TBI prognostic models, and evidence-based geriatric TBI consensus management guidelines aimed at improving short- and long-term outcomes for the large and growing geriatric TBI population.
Introduction
T
Unsurprisingly, older adults with TBI experience higher morbidity and mortality, 4,14 –16 and slower recovery trajectories 17 –20 and have, on average, worse functional, cognitive, and psychosocial outcomes months or years post-injury than do younger patients. 5,17,21 –24 Consequently, there is often an assumption of futility surrounding the acute management of these patients. Some centers impose age cutoffs for even offering treatment, such as neurointensive care admission or neurosurgical intervention, for older adults presenting with severe TBI. 25,26 However, a subset of older adults with TBI, including severe TBI, may recover well, suggesting that chronological age and TBI severity alone are inadequate prognostic markers. 27 –29 Multiple medical comorbidities and cognitive impairment frequently precede TBI among older adults and likely complicate recovery. 13 Yet few studies have assessed the role of pre-existing conditions on outcomes post-TBI in this population, and virtually none have included measures of premorbid function. In fact, older adults, particularly those with pre-existing functional impairment or multiple comorbidities, are often excluded from TBI research altogether. 30 Despite the large and growing epidemic of older adults with incident TBI, there are few to no evidence-based geriatric TBI guidelines to inform complex medical decisions for either acute or long-term management.
This scoping review 31 of the literature on all-severity TBI in older adults focuses on incident TBI sustained in older adulthood (“geriatric TBI”) rather than on the separate, but related, topic of older adults with a history of earlier-life TBI. Whereas most past studies define “older adults” as those 60–65 years of age or older, we chose to use the more inclusive age cutoff of 50–55 years or older that is used in several well-known longitudinal studies of aging 32,33 as well as several past studies of geriatric TBI. 18,20,34 –38 We describe the epidemiology of TBI in older adults, the role of comorbidities and baseline function, diagnostic testing, emerging geriatric TBI guidelines and management issues, outcomes, and critical future directions for research.
Methods
We conducted a scoping review following the methodological framework proposed by Arksey and O'Malley 31 to achieve the broad goals of summarizing current scientific knowledge of geriatric TBI and identifying major research gaps. Briefly, a scoping review is similar to a systematic review, incorporating a systematic approach to reference search, and is therefore less susceptible to bias than a traditional rapid, critical, or expert review. 39 However, given the broader nature of the research question, it generally uses more flexible screening and inclusion criteria and does not involve systematic quality assessment.
In consultation with an experienced medical librarian, we conducted literature searches in PubMed, Web of Science, Biosis Previews, Embase, and PsycINFO to explore six related questions about TBI in the elderly. The PubMed search used the following MeSH terms and keywords: ((“brain injuries, traumatic” [MeSH] OR “brain concussion” [MeSH] OR “traumatic brain injury” OR “traumatic brain injuries” OR concussion) AND (“aged, 80 and over” [MeSH] OR elderly or “older adults” or geriatric or elders)) without limiting results by date of publication. Because there are no available MeSH terms to specifically identify adults ages 50 and older, we used a combination of the one available specific MeSH term (“Aged, 80 and over”) and several non-MeSH terms (“elderly,” etc) to identify our target age category. This search returned 9010 citations. We combined this root search with each of six targeted subtopic searches: 1) epidemiology (2435 citations); 2) outcomes (2180 citations); 3) biomarkers (721 citations); 4) neuroimaging (including magnetic resonance imaging [MRI] and positron emission tomography [PET]; 1447 citations); 5) comorbidities (682 citations); and 6) guidelines (176 citations). Subtopic searches were conducted on February 6, 2017, and results were not limited by date of publication. The PubMed search algorithm was then translated to work properly in Web of Science, Biosis Previews, Embase, and PsycINFO by substituting in database-specific controlled vocabulary. These additional database searches yielded the following nonduplicated citations in each subtopic: 1) epidemiology (1446 citations); 2) outcomes (1603 citations); 3) biomarkers (262 citations); 4) neuroimaging (including MRI and PET; 1043 citations); 5) comorbidities (352 citations); and 6) guidelines (327 citations).
English-language titles and abstracts were manually screened by the authors (R.C.G., K.D.O., and M.R.M.) for relevance. Priority was given to references originating from PubMed. The vast majority of citations identified were not relevant to geriatric TBI, and therefore >95% of citations were eliminated at this initial stage. Additional articles were identified from governmental sources, for example, the Centers for Disease Control and Prevention (CDC), from consultation with subject-matter experts, and from cited reference searching in PubMed. This scoping review represents a qualitative summary and synthesis of the most relevant literature identified.
Epidemiology
Prevalence and incidence
TBI is extremely common, with a lifetime prevalence of up to 40% among adults. 40 Whereas incidence of TBI peaks three times over the life course—in childhood, adolescence, and older adulthood—the highest incidence of TBI occurs in older adults (Fig. 1). More than 1 in 200 Americans ages 65–74 years and more than 1 in 50 Americans ages ≥75 years experienced a TBI-related ED visit, hospitalization, or death in 2013, with the next highest incidence occurring in children ages 0–4 years (incidence 1,591 in 100,000). 1 In 2013, adults ages ≥75 years accounted for 26.5% of all TBI-related deaths and 31.4% of all TBI-related hospitalizations in the United States. From 2006 to 2008, 800,000 adults ages ≥65 years were evaluated in U.S. EDs for TBI, among whom the average age was 80 years. 41 Incidence of admission to acute inpatient rehabilitation for a primary diagnosis of TBI also increases with age, with the highest incidence occurring among those ages ≥80 years. 5
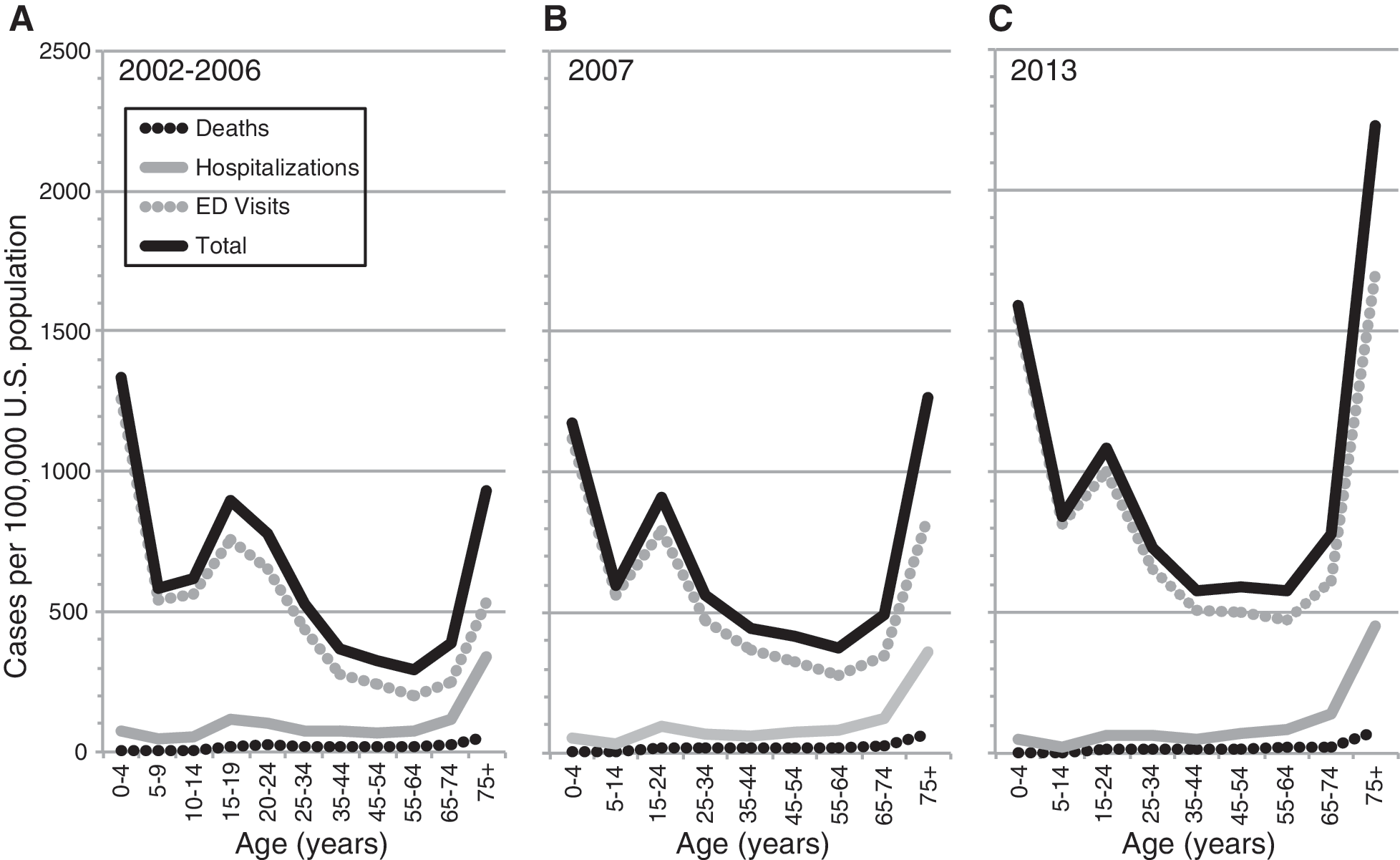
Annual incidence of traumatic brain injury (TBI) emergency department (ED) visits, hospitalizations, and deaths 2002–2013 by age. Annual incidence of TBI-related ED visits, hospitalizations, and deaths per 100,000 U.S. population are shown for the periods 2002–2006 (
Incidence of TBI-related ED visits, hospitalizations, and deaths is increasing among older adults, whereas incidence of TBI-related hospitalizations and deaths is declining among children and adults <55 years of age 42 (Fig. 1). From 2007 to 2013, TBI-related ED visits among those ages ≥75 years doubled and TBI-related hospitalizations increased more than 25%. 1 The rapid rise in TBI-related hospital visits among the oldest segment of the U.S. population exceeded population growth during this time frame. 9 This high and increasing incidence of TBI-related ED visits, hospitalizations, and deaths among older adults has been confirmed in multiple epidemiological studies in individual U.S. states and nation-wide databases 4,43 –45 as well as in higher-income countries around the globe including Spain, 46 the United Kingdom (UK), 47 Scotland, 48 the Netherlands, 49 Austria, 50 Finland, 51 Canada, 52 –54 and Australia. 7 Despite this high incidence, older adults may be less likely to seek medical attention for TBI 55 and are also less likely to be accurately diagnosed even when medical attention is sought. 56 These findings suggest that TBI incidence among older adults likely exceeds published reports.
Mechanisms and demographics
The majority of TBIs sustained by older adults are attributed to low-level or same-level falls from standing height or less, 7,57 even among those requiring surgical treatment of traumatic intracranial hemorrhage (Fig. 2). 58 Mechanisms of TBI are biologically important because fall-related TBIs more commonly result in mass lesions, such as subdural hemorrhage, while the motor vehicle accident–related TBIs experienced by teens and younger adults more commonly result in diffuse axonal injury. 59 Physically active older adults may be at elevated risk for specific sport-related mechanisms. For example, adults ages 55–64 years have the highest incidence of skiing-related TBI. 60 Bicycle-related injuries, including TBI, in older adults most commonly occur while mounting or dismounting the bicycle. 61 Compared to younger individuals with TBI, older adults are less likely to engage in alcohol or drug abuse. 5 Finally, the majority of the oldest old patients with TBI are female and white (Fig. 3), 9,41,51,56 mirroring U.S. nation-wide demographics of aging. 62 Although few population-based or multi-center studies have compared the distribution of TBI severity (e.g., mild, moderate, or severe) across age categories, at least one U.S. nationally representative study reported a similar distribution of TBI severity as defined by the Glasgow Coma Scale (GCS) and Abbreviated Injury Scale (AIS) across the age spectrum. 9
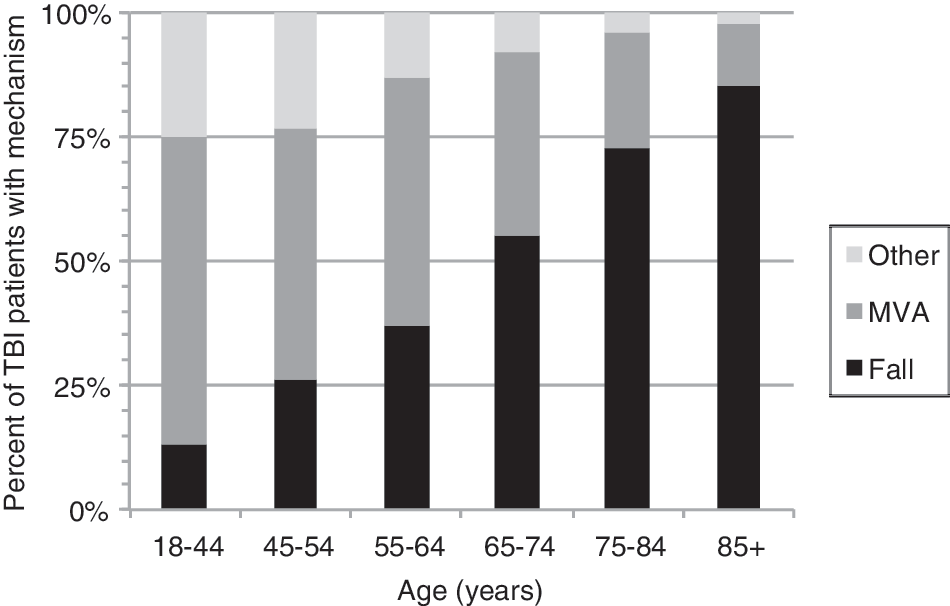
Major mechanisms of traumatic brain injury (TBI) by age (2007–2010). Falls are shown in black; motor vehicle accidents (MVA), in dark gray; and other mechanisms, in light gray. Mechanism of TBI among older adults is predominantly falls whereas mechanism among younger individuals is predominantly MVA. 9
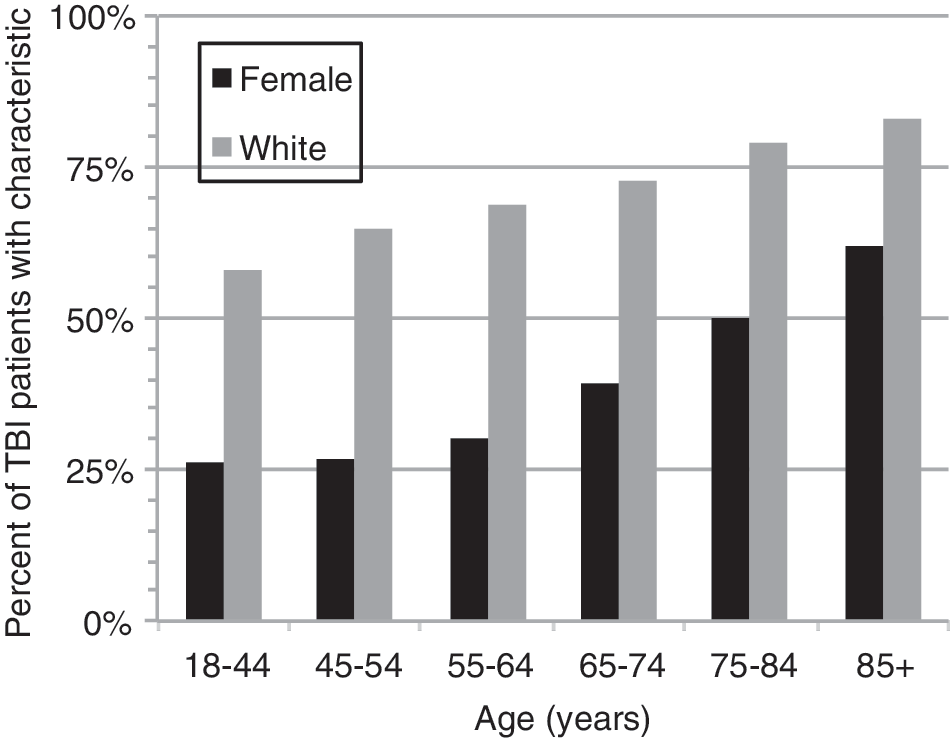
Sex and race of adults with traumatic brain injury (TBI) by age (2007–2010). The demographics of TBI shift toward increasing prevalence of white race (dark gray bars) and female sex (black bars) with increasing age such that by age 85 years+ the majority of patients with TBI are female. 9
Healthcare cost and utilization
Compared to younger patients with TBI, those ages ≥65 years who seek emergent care are nearly 3 times more likely to receive a head computed tomography (CT) or MRI in the ED setting and 4 times more likely to be admitted to the intensive care unit (ICU), step-down, or surgical unit. 41 In the inpatient rehabilitation setting, an improvement of one point on either the Functional Independence Measure (FIM) or the Disability Rating Scale was associated with double the healthcare expenditures in older versus younger adults. 18 In a large, nation-wide sample of older adults treated in hospitals for TBI, 63 the average annual treatment cost per person ranged from $73,000 to $78,000. 64 In this study, older-old patients had significantly lower rates of outpatient injury-related clinic visits and significantly higher rates of rehospitalizations, home healthcare visits, and weekly hours of unpaid care from friends and family compared to younger-old patients, suggesting possible age-related disparities in coordinated care after hospital discharge. 64
The Role of Pre-Existing Comorbid Conditions and Baseline Function
Pre-existing conditions are extremely common among older adults with TBI. In a nation-wide study of older adults admitted to UK hospitals for TBI, 11% had pre-existing dementia, 22% had pre-existing hypertension, and 99% had at least one pre-existing medical condition. 47 Those with one pre-existing condition often had additional co-occurring conditions, such as diabetes, cardiovascular disease, pulmonary disease, or renal disease. 65,66 Pre-injury cardiovascular conditions and endocrine disorders are particularly common in the oldest age categories of adults with moderate-severe TBI, with the presence of these conditions occurring up to 5 times more frequently among those >75 years of age compared to those ages 50–54 years. 65
Pre-existing conditions, including past history of TBI, are risk factors for sustaining a TBI. Among adults ≥65 years, baseline cerebrovascular disease, depression, and impaired activities of daily living are associated with late-life incident TBI risk. 13 Earlier-life TBI accounts for an estimated 20% of population-attributable risk of late-life TBI. 15 Several additional studies demonstrate higher past-year medical costs among older adults who sustain a TBI (relative to matched uninjured controls) 67 and greater numbers of systemic disease hospital admissions in the years preceding injury compared to those with non-brain injury. 68 This is not surprising, given that falls are the most common cause of TBI in older adults, 1 and older adults who are pre-disposed to falls are more likely to have chronic medical conditions, 8 history of past TBI, 69 medication side effects, visual impairment, cognitive impairment, and balance or gait impairment. 8,70 –72
Pre-existing conditions, including past history of TBI, are associated with worse outcomes post-TBI. In two large, prospective studies, past history of TBI was associated with worse emotional, psychosocial, and behavioral outcomes, including substance use problems, even though those with past TBI had overall less-severe index injuries. 73,74 Greater disease comorbidity at the time of TBI is associated with reduced functional independence at rehabilitation admission, 75 at discharge, 75 and 2–4 years post-injury 76 as well as with increased 1-year mortality. 77 Individuals >55 years of age with TBI who died within 5 years of discharge after inpatient rehabilitation had more comorbid medical conditions and gait instability noted in the hospital records compared to matched survivors. 78 Trauma centers are seeing a greater proportion of elderly patients with more comorbid diseases as the U.S. population ages 79 ; these trends, along with improvement in trauma care, have resulted in a shift in the causes of death after traumatic injury, such that fewer people are dying of injury-related complications whereas more people are dying of complications of pre-existing medical conditions. 80 It is therefore not surprising that self-rated poor health in the year preceding TBI may be more predictive of outcome after mild TBI than injury characteristics in older adults. 81
The critical importance of pre-morbid functional status in predicting long-term morbidity and mortality in older adults has been established in studies of older hospitalized adults and older adults with hip fracture. 82 –85 Several studies of geriatric trauma (not TBI-specific) have demonstrated that incorporating comorbidities, polypharmacy, baseline function, or measures of frailty into prediction models of outcome post-trauma substantially improve their prognostic value. 86,87 In an illustrative case report, Crossley and colleagues elegantly described an 80-year-old woman with normal pre-injury function—defined as complete independence in self-care, financial and household management, and an active and healthy lifestyle—who made an excellent recovery after a severe TBI. 88 Very few studies of outcomes after geriatric TBI, however, have systematically measured pre-TBI functional status 21,64,89 –91 and even fewer have assessed the prognostic role of pre-TBI functional status on outcomes. 92,93
Initial Clinical Assessment and Diagnostic Studies
Clinical assessment
The GCS, although the most widely used clinical assessment to determine TBI severity at the time of initial presentation, may lack the nuance required to accurately assign TBI severity in older adults. Older adults with pre-existing dementia may have an abnormal GCS at baseline, 94 others may have comorbid medical conditions or medication side effects that may complicate accurate diagnosis, 95 and in others the burden/evolution of TBI may not be adequately captured by the initial GCS. 96,97 As an example, age-related atrophy may provide space for an intracranial hemorrhage to expand substantially before leading to clinically apparent signs or symptoms that would be detected by the GCS. Thus, there is an urgent need for objective biomarkers to aid in the diagnosis, management decisions, and recovery monitoring of older adults with TBI, particularly those with pre-existing medical or neurological conditions.
Neuroimaging
Head CT is an important diagnostic tool in the acute evaluation, management, and outcome prediction for patients across the age spectrum. CT evidence of neurotrauma both increases with age and is associated with worse outcomes. 36,98,99 The types of neurotrauma observed on head CT differ by age: Prevalence of extradural hematoma declines with age whereas prevalence of midline shift and subdural hematoma increases. 100 Among adults ages ≥65 years admitted to hospitals with any severity of TBI, up to 45% may have subdural hematoma apparent on head CT. 47 Among adults ages ≥65 years presenting to the ED with mild TBI (GCS 13–15), 11–21% may have evidence of intracranial trauma (compared with 5% in younger adults). 101 –104 Even those with normal GCS (GCS = 15) are at high risk: 17% of adults >60 years of age with a normal GCS had a positive head CT in one large Canadian study, 102 and 57% of adults >60 years of age who were found to have an intracranial hemorrhage on head CT had presented with a normal GCS in a large Swedish study. 101 This dramatically higher prevalence of CT evidence of neurotrauma among older versus younger patients is hypothesized to result from several factors: age-related changes in vasculature and white matter rendering vessels more vulnerable to rupture and white matter tracts more susceptible to shear injury, weakened musculature in the neck and trunk; such that even ground-level falls are not well braced by the body, pre-existing conditions, and medications such as antithrombotics. 10,11,13
Structural MRI has been shown to improve prognostic modeling post-TBI by identifying evidence of neurotrauma that may be missed on head CT. 105 Only a few studies have investigated the impact of age on MRI findings in TBI. One prospective study of 98 patients across the spectrum of age and TBI severity that performed MRIs, on average, 2.3 years post-TBI identified an association between older age and both larger lesion volumes and smaller gray matter volumes. 106 Emerging neuroimaging technologies for TBI include advanced structural MRI sequences such as diffusion tensor imaging or 7-Tesla MRI, functional MRI, 107 and a number of PET ligands that bind (with varying specificity) to amyloid-beta, tau, and markers of inflammation. 108,109 Using these emerging technologies in older adults deserves further study. Evidence of tau or amyloid deposition on PET in older adults with TBI, however, will need to be interpreted carefully given evidence from multi-site nonselected autopsy studies that have demonstrated that high-grade amyloid and tau neuropathology increase approximately 10–15% per decade beginning in the sixth decade of life, rising from 1% to 2% among those ages 61–65 years to nearly 40% among those ages 91–95 years. 110
Emerging proteomic and blood biomarkers
Recent advances in biochemical assays of serum and cerebrospinal fluid (CSF) have identified a number of promising candidate blood-based and proteomic biomarkers of apoptosis and neuronal injury (neuron-specific enolase, tau, and amyloid-beta 1–42), glial injury (glial fibrillary acidic protein [GFAP], S100B, and excitatory amino acids), demyelination (myelin basic protein), proinflammatory cytokines (interleukins-1, −6, and −8), and gene expression of microRNAs (miR-16, miR-26a). 111 Very few studies have evaluated the impact of aging on the kinetics or clinical performance of serum or CSF-based biomarkers of TBI. 112 –117 For example, although serum S100b showed initial promise in identifying low-risk patients who do not require head CT, 118 this biomarker may have reduced specificity among adults ages ≥65 years. 113 Additional emerging evidence suggests that there may be differences in CSF levels of excitatory amino acids and cytokines in older versus younger patients with TBI that may be independent of TBI severity. 114 Of note, circulating cytokine levels are affected by a range of comorbidities that are common among older adults, including hypertension, diabetes, dementia, Parkinson's disease, and osteoporosis. 119,120 Studies of TBI biomarkers in rodent models have identified compelling differences between aged and younger animals on TBI-associated proteomic signatures, 115 peri-TBI levels and temporal sequences of mRNA expression of microglial (CD11b and ionized calcium binding adaptor molecule 1), and astrocytic (GFAP and S100b) activation markers, 116 and peripheral monocyte recruitment post-TBI. 117
Management
Guidelines
Older adults with TBI are more likely to experience an interfacility transfer to a level 1 or 2 trauma center compared to younger adults, suggesting higher rates of either inappropriate initial triage or delayed deterioration necessitating transfer. 121 The GCS is widely used to assign TBI severity, but is poorly predictive of morbidity and mortality in older adults who frequently have better initial GCS scores than younger individuals with the same injury severity. 122 For this reason, researchers in Ohio have been working to develop and validate geriatric trauma-field triage criteria to optimally identify older adults with TBI who require emergent transfer to a trauma center, for example, a GCS cutoff of ≤14 (vs. ≤13 for younger individuals). 123 –125
Most, but not all, 126 existing rules and validation studies support the routine use of head CT for all patients >60 102 or >65 years of age 103,104,127,128 presenting with mild TBI even after rapid return to baseline. The American College of Emergency Physicians recommends considering head CT in all patients ages ≥65 years who present with TBI, even mild injury without loss of consciousness (LOC), and recommends obtaining a head CT in all patients >60 years of age with TBI and LOC. 129 The Canadian CT Head Rule identifies ages ≥65 years as a high-risk factor for intracranial trauma needing neurosurgical intervention among patients presenting with TBI and a GCS of 13–15, regardless of LOC. 103 A large Austrian study later confirmed age >65 years as a high-risk factor for CT evidence of neurotrauma, but also identified novel high-risk comorbidities, including history of dementia or ischemic stroke. 128 Further development and validation of geriatric TBI neuroimaging guidelines are therefore critically important.
Efforts are underway to predict which geriatric TBI patients may be managed safely on a standard medical or surgical ward rather than an ICU. 130,131 One Swedish trauma center developed a protocol for geriatric neurosurgical decision making based on pre-injury functional status and predicted 1-year survival. 29 While this center reported favorable outcomes in 41% of patients >65 years of age who underwent craniotomy for acute subdural hemorrhage, further research is needed to determine whether this approach may be overly conservative. 29 According to the Eastern Association for the Surgery of Trauma, clinicians are encouraged to limit further aggressive treatment for older adults with severe TBI who do not improve within 72 h of admission. However, at least one retrospective observational study found that although lack of improvement by 72 h was significantly associated with increased in-hospital mortality, it was not associated with functional status at discharge or 12-month survival among those who survived to discharge. 27
There remain, however, few to no evidence-based national or international consensus guidelines to inform acute inpatient management or long-term outpatient follow-up of older adults with TBI. This is, in large part, attributed to the paucity of dedicated Class I prospective clinical trials of treatments for older adults with TBI. In the absence of evidence-based guidelines, some centers have proposed strict age cutoffs for offering aggressive treatment such as neurointensive care admission or neurosurgical intervention for older adults with severe TBI, 25,26,132 whereas others have a policy to admit all older adults with any TBI to the neurointensive care unit for serial neurological assessments and head CTs—a practice that may prove overly conservative. 133
Neurocritical care and neurosurgical management issues
Acute care and prognosis of older adults with moderate-to-severe TBI are particularly challenging as demonstrated by dramatic variability in practice and outcomes across centers (Supplementary Table; see online supplementary material at
Whether ICP monitoring improves outcomes in this population remains controversial, with some studies supporting its use 134 and one study finding no evidence of meaningful benefit. 135 The surprisingly low prevalence of ICP monitoring in the negative study, however, suggests that there may have been unmeasured confounding variables. A single-center study of continuous bedside neuromonitoring data found that although older patients have lower ICP and higher cerebral perfusion pressure compared to younger patients, factors typically associated with better outcomes, 137 they also had worse vascular pressure reactivity and autoregulation compared to younger patients, factors that may contribute to worse outcomes. 137 Together, these findings suggest that although ICP monitoring likely improves outcomes in some older adults, given the tendency for older adults to have lower ICPs on average than younger adults, it is possible that older adults may benefit from the development of geriatric-specific clinical criteria to determine whether ICP monitor placement is appropriate.
There is substantial between-study heterogeneity in outcomes after craniotomy or craniectomy in geriatric TBI. 132,138 The method of surgical intervention may impact outcome as demonstrated by a retrospective cohort study that utilized propensity scores to mitigate confounding by indication; patients who were treated with decompressive craniectomy had worse 6-month Glasgow Outcome Scale (GOS) outcomes compared to those treated with craniotomy. 136
The contribution of antithrombotic therapies to poor outcomes in older adults with TBI is contested. Some studies have identified increased mortality and worse outcomes for all classes of antithrombotic agents. 139,140 Others report that anticoagulant agents such as warfarin (but not antiplatelet agents) are associated with increased mortality 141 (particularly if warfarin is at a therapeutic level 142 ) and need for neurosurgical intervention. 143 Still others have found that early aggressive treatment can mitigate any negative impact of antithrombotics on mortality or outcomes. 144,145 Thus, although antithrombotic therapies may not be associated with worse post-TBI outcomes in a setting in which patients receive rapid and aggressive treatment for hemorrhagic complications and in analyses that adjust for initial TBI severity, it is clear that anticoagulant therapy is associated with worse initial TBI severity, such as acute subdural hemorrhage after relatively minor trauma. 141,142,145,146 This conclusion is further supported by a study of 80 patients (all ages) with acute subdural hemorrhage reporting that initial hematoma volume and GCS are better predictors of hematoma expansion and outcome than age or antithrombotic therapy if patients are rapidly given appropriate agents to reverse coagulopathy. 147 The decision to restart anticoagulants such as warfarin after a TBI in older adults at high risk of thrombotic events or ischemic stroke is complex. One large, retrospective study of over 10,000 Medicare beneficiaries hospitalized for TBI who had been taking warfarin during the month preceding admission reported that restarting warfarin after discharge was associated with a 51% increased risk of all hemorrhagic events and only a 23% reduction in all thrombotic events over the subsequent year. However, when stroke risk was assessed in isolation, there was a net benefit of a 17% reduction in risk of combined hemorrhagic or ischemic stroke. 148
Outcomes
The controversial role of age
It is well established that, on average, older adults with TBI have higher mortality,
4,14
–16
slower rates of functional and cognitive recovery,
17
–20
and worse functional outcomes post-TBI compared to their younger counterparts.
5,17,21
–24
In one of the largest studies to date to investigate the association between age and 6-month functional outcome score on the GOS among 8719 patients with moderate-to-severe TBI contained in the IMPACT database, there was a strikingly linear relationship observed between age and outcome.
149
Thus, some have argued that there is unlikely to be a specific age beyond which outcomes precipitously worsen.
150
Other studies, however, have reported an “inflection point” in the fourth or fifth decade of life at which trauma mortality appears to increase steeply.
151,152
Regardless of the presence or absence of an inflection point, it is clear that a substantial number of older adults with TBI may recover well (Table 1, Table 2, and Supplementary Table; see online supplementary material at
This table summarizes outcomes data for identified studies that report group-level mortality or functional outcomes after geriatric TBI. Whereas primary outcomes reported in each study may differ from those reported in this table, data displayed here were chosen to optimize direct comparison across studies.
ED, emergency department; FIM, functional independence measure; GCS, Glasgow Coma Scale; GOS, Glasgow Outcome Scale; GOSE, Glasgow Outcome Scale-Extended; Pro, prospective; Retro, retrospective; TBI, traumatic brain injury.
This table summarizes outcomes data for identified studies that report group-level mortality or functional outcomes after geriatric TBI. Whereas primary outcomes reported in each study may differ from those reported in this table, data displayed here were chosen to optimize direct comparison across studies.
DRS, disability rating scale; IVH, intraventricular hemorrhage; ICU, intensive care unit; PTA, post-traumatic amnesia; SD, standard deviation; TBI, traumatic brain injury. Other abbreviations per Table 1.
The role of provider attitudes as well as patient and family preferences must also be considered when interpreting outcomes in older adults with TBI, who may be more likely to have care electively withdrawn. 155 The issue of provider attitudes was highlighted in a large UK study of patients with TBI and cerebral contusions, reporting that increasing age was associated with longer delays in obtaining an initial head CT, lower likelihood of being transferred to a neurotrauma center, and lower likelihood of review by a senior (vs. junior) physician. 156 Similar findings suggestive of agism in TBI management decisions were reported in one Scottish study, 157 but a multi-center, prospective U.S. study did not identify any evidence of age-related neurosurgical intervention bias. 91
Outcome assessment
In the United States, the GOS and the Glasgow Outcome Scale-Extended (GOSE) are the most widely used and widely cited functional outcome measures in TBI clinical research 158 and are included in the National Institute for Neurological Disorders and Stroke TBI Common Data Elements (CDEs). 159 Neither the GOS nor the GOSE were developed or validated in older adults and may not adequately quantify TBI-related functional impairment in a geriatric population, particularly in those with pre-existing functional impairment. For example, a multi-center, prospective study of older adults with severe TBI found that although these patients experienced significant improvement in physical function over 1 year according to the Health Related Quality of Life Measure, this functional improvement was not detected by the GOSE. 160 Additionally, many in the field rely upon the 1998 GOS and GOSE administration and scoring guide by Wilson and colleagues. 161 Yet, even in this comprehensive guide, scoring of patients with pre-injury disability is described as “problematic.” 161 Thus, a patient with severe baseline disability who fully recovers to their severely disabled baseline status may be scored as a GOSE 3 (severe disability) by one study and a GOSE 8 (good recovery) by another study. Additionally, the GOS and GOSE do not systematically distinguish between effects of brain versus body trauma or between cognitively versus physically mediated function. 161
We report nearly 40 studies that assessed functional outcome after all-severity or moderate-severe TBI in older adults (Table 2 and Supplementary Table; see online supplementary material at
There is increasing recognition that the use of the GOS, GOSE, or FIM as the primary endpoint for TBI clinical trials does not adequately capture the complex, multi-dimensional, and evolving nature of TBI, thus historically limiting the success of these trials. 162 To address these limitations, efforts are underway to develop improved TBI endpoints. 163,164 As part of this effort, it will be critically important to either evaluate the performance of existing multi-modal measures in geriatric TBI populations (as was done in this Taiwanese study, 165 these Canadian studies, 166,167 this meta-anlaysis, 168 and this review/opinion piece 169 ) or develop novel multi-modal geriatric-specific TBI endpoints to optimize success of future TBI clinical trials in older adults.
Mortality
When considering mortality after geriatric TBI, it is important to distinguish between short-term mortality (during initial hospitalization or rehabilitation) and longer-term mortality (over months or years after TBI). Short-term mortality post-TBI is high among older adults, particularly those with severe TBI (Supplementary Table; see online supplementary material at
Post-traumatic neurological disorders: Epilepsy, stroke, and neurodegenerative disease
Compared to younger individuals, older adults are at increased risk for post-traumatic epilepsy 177,178 and are more likely to present with delayed rather than early seizures post-TBI. 179 Pre-existing conditions such as Alzheimer's dementia (AD) further increase the risk of epilepsy in older adults. 180 The choice of drug for both short-term post-traumatic seizure prophylaxis and long-term post-traumatic epilepsy treatment deserves further study in older adults. First-generation antiepileptic agents such as phenytoin may be suboptimal in older adults because of nonlinear pharmacokinetics, propensity for drug-drug interactions, and cognitive side effects, whereas certain newer agents such as lamotrigine or levetiracetam may be preferable. 181,182
TBI may be an independent risk factor for both ischemic and hemorrhagic stroke. 183,184 Emerging evidence suggests that initiation of treatment with a selective serotonin reuptake inhibitor (SSRI) among older adults hospitalized for TBI was associated with increased risk of hemorrhagic, but not ischemic, stroke. 185 This finding was further supported by a recent population-based study that identified an association between SSRI initiation and spontaneous hemorrhagic stroke among patients taking oral anticoagulants. 186 Further research is needed to determine the mechanism of post-TBI stroke and SSRI-associated hemorrhage in order to inform safe management of post-TBI depression (which is common and undertreated in older adults 187 ) as well as optimal post-TBI stroke prevention strategies.
Although TBI is now a well-established risk factor for dementia and Parkinson's disease, 188 –191 few past studies have assessed risk of dementia or PD specifically after geriatric TBI (e.g., TBI sustained in the fifth decade or beyond). 34,35,192 –194 One small, prospective study of falls and risk of dementia among individuals ages ≥70 years concluded that fall-related TBI was associated with earlier onset of dementia and that presence of an apolipoprotein E epsilon 4 allele acted synergistically with fall-related TBI to further increase risk of earlier onset of dementia. 192 An important methodological concern in epidemiological studies assessing risk of a neurodegenerative disease after geriatric TBI is the possibility of reverse-causation—that the patient fell and sustained a TBI because of early symptoms of a neurodegenerative disease rather than the reverse. This concern was highlighted by a population-based Danish study reporting that the association between TBI and PD was almost entirely attributed to fall-related TBIs sustained within the 3 months preceding initial PD diagnosis. 194 To mitigate this potential for reverse causation, two large studies using California-wide data from the Healthcare Cost and Utilization Project compared risk of dementia and PD in adults ages ≥55 years at least 1 year after sustaining a TBI versus fracture. In these studies, incident geriatric TBI was associated with a 44% increased risk of PD and a 26% increased risk for dementia over the subsequent 5–7 years. Even mild TBI was associated with a 24% increased risk for PD for those ages ≥55 years and a 21–25% increased risk for dementia among those ages ≥65 years (but not for those ages 55–64). 34,35
Repeated TBI in older adults may be associated with greater risk for neurodegenerative outcomes than single TBI. 34 Repeated concussive and subconcussive injuries have been associated with chronic traumatic encephalopathy (CTE), a unique degenerative tauopathy, primarily described among contact-sport athletes, blast-exposed military personnel, and victims of domestic violence. 195 –197 Whether CTE may result from repeated fall-related TBIs or repeated fall-related subconcussive injuries in older adults is unknown. However, a case series of 139 cases of autopsy-proven multiple system atrophy (MSA)—a rare degenerative movement disorder that causes dysautonomia, parkinsonism, and cerebellar ataxia—identified CTE pathology in 8 cases (6%). Of these 8 cases, only 4 had a history of contact sports generating the hypothesis that repeated falls attributed to MSA may have precipitated the CTE pathology. 198 An analysis of over 1700 brains from the Mayo Clinic brain bank, however, did not identify any cases of CTE in patients exposed to a single fall-related TBI. 199
Other chronic psychosocial and cognitive impairments
Several studies have assessed psychosocial sequelae after geriatric TBI. 24,200 –203 Based on a systematic review of post-TBI depression, prevalence of depression is 1.8–8.9% in older community-dwelling adults, 25% in skilled nursing facilities, and 21–37% among older adults with TBI. 201 TBI in older adults has been associated with 11% increased risk of new-onset depression and 50% increased risk of new-onset PTSD. 204 Risk of depression among older adults hospitalized for TBI may be highest immediately after discharge and then decline over the subsequent 12 months. 202 Whereas this reduction in incident depression with increasing time post-injury may be explained by declining rates of post-TBI longitudinal follow-up and resultant ascertainment bias, at least one study has found that depressive symptoms decline over time post-injury only among older, and not younger, adults. 203 Similarly, a small study of 26 older adults with mild TBI found that, compared to younger patients, older adults reported less psychosocial impairment, psychological distress, and physical symptoms 1 month after their TBI, but these findings were largely mediated by employment status. 24 This finding suggests either that older adults are less prone to some of the psychosocial sequelae of mild TBI or that the outcome assessments capturing psychosocial sequelae of TBI are less sensitive among retirees. Together, these findings suggest that careful screening for mood symptoms among older adults with TBI is important at any time post-injury, but particularly within the first few months to years post-injury when risk and symptom burden may be highest.
Cognitive symptoms and impairment after TBI in older adults are common. 205 Just as in younger patients, prevalence and severity of cognitive sequelae in older adults tends to increase with increasing TBI severity. 206 Older adults with TBI, however, experience slower recovery of cognitive function during rehabilitation 18 and over the year after TBI compared to younger patients. 19 Most studies of cross-sectional cognitive outcomes after TBI have reported that older patients have worse cognitive outcomes compared to younger patients. 207 The few studies that have adjusted for expected age-related decline in cognitive function, however, have reported that older adults may have equivalent or even better cognitive outcomes compared to younger individuals with TBI. 207 This compelling finding highlights the importance, as in the evaluation of post-TBI mortality described above, of accounting for expected age-related changes that are unrelated to the injury when comparing outcomes across age categories. Other important modifiers of cognitive outcome in older adults with TBI include pre-injury factors, such as pre-existing comorbidities that may be independently associated with worse cognitive function, as well as the deleterious cognitive impact of trauma and hospitalization more generally, versus the specific impact of TBI. For example, one small study of mild TBI in older adults reported that although 3-month cognitive outcomes were worse among those with mild TBI compared to community-based controls, outcomes were equivalent to orthopedic controls, 208 suggesting that cognitive impairment after mild TBI in older adults may be partially attributed to overall trauma or predisposition to injury. 208
Prognostic models
As the global incidence of geriatric TBI continues to rise, the need for geriatric TBI prognostic models has become increasingly urgent. Recently two prognostic models have incorporated age as well as clinical and CT indicators of TBI severity and have subsequently each been studied in large, population-based samples of older adults with TBI. The CRASH-CT prognostic model is a predictor of 14-day mortality and 6-month unfavorable outcome on the GOS and includes only variables of age, GCS, pupil reactivity, extracranial injury, and evidence of trauma on head CT. 209 The model does not take into account baseline comorbidities or pre-injury function. The model showed adequate discrimination and calibration in older adults with all-severity TBI (ages 65–84 years) in a U.S. study, 210 but performed very poorly with dramatic overprediction of mortality (observed 50%; predicted 81%) and unfavorable outcome (observed 72%; predicted 95%) in older adults with severe TBI (ages 65–92 years) in a Norwegian study. 211 The IMPACT prognostic model predicts 6-month mortality and unfavorable outcome on the GOS. 212,213 The IMPACT model includes age, GCS, pupillary reactivity, hypoxia, hypotension, CT evidence of trauma, and blood glucose and hemoglobin levels, but, again, does not include baseline comorbidities (other than those captured by baseline glucose and hemoglobin) or pre-injury function. It showed adequate discrimination, but poor calibration, among older adults (ages 65–84 years) with evidence of substantial underprediction of mortality. 214 The poor performance of these models in older adults with TBI is not surprising given that the development cohort for both the CRASH-CT and IMPACT models consisted of pooled trials and observational cohort studies that largely excluded older adults with pre-existing comorbidities. Further studies are now needed to determine whether incorporating comorbidities, polypharmacy, baseline function, or measures of frailty into these models will improve their prognostic value, as has already been demonstrated for geriatric trauma outcome prediction models. 86,87
Rehabilitation
There is substantial evidence that intensive inpatient rehabilitation greatly benefits older adults with TBI, 215 with the majority showing functional gains and achieving discharge to home. 38,205 Although functional gains are often slower in older versus younger individuals, necessitating longer lengths of stay, at least one study from the TBI Model Systems database found that overall net functional gains did not significantly differ between older versus younger patients after accounting for TBI severity. 20 It is therefore concerning that a multi-center study of nearly 1500 patients admitted to nine inpatient rehabilitation hospitals reported that adults ages ≥65 years received less intensive rehabilitation services (reflected both in shorter length of stay and also fewer hours of therapy per day) than younger patients and regained less functional ability both during and after inpatient rehabilitation. 216 Race and ethnicity—or associated social factors—may play a role in discharge destination, with discharge to home being more likely among older black and Hispanic adults compared to older white adults. 217 There is an emerging literature on best neurorehabilitation practices for older adults with acquired brain injury including stroke and TBI. A key goal of rehabilitation in this population is the removal of “excess disability,” for example, depression, insomnia, pain, and social instability, that may complicate recovery. 215
Future Directions for Research
Although research on geriatric TBI has expanded in recent years, older adults are severely under-represented in TBI research 218 and important knowledge gaps remain. This under-representation may be attributed to overly restrictive inclusion/exclusion criteria as well as patient factors. 219 –221 Although the study of “pure” TBI may be preferable in some observational studies or clinical trials, strict exclusion criteria based on past medical history systematically excludes older adults 222 and unrepresentative study samples have and will result in a biased and incomplete understanding of TBI outcomes for older adults. 223,224 Further, lack of systematic measurement of pre-injury health and functional status may confound attempts to develop prognostic models in geriatric TBI. Yet, few past studies have measured pre-TBI functional status. 21,90 Rather than treating comorbidities and poor baseline function as detractors from TBI-focused clinical research, heterogeneity of samples could be harnessed to improve power as described by the IMPACT investigators. 221
Concurrent with the need to increase representation of older adults in TBI research, there is an urgent need to develop geriatric TBI CDEs to encourage a systematic approach to measuring pre-injury comorbidities, preinjury functional status, and geriatric-specific imaging and proteomic biomarkers, and improved prognostic models. This information is necessary to develop evidence-based geriatric TBI treatments and consensus management guidelines, including targeted fall prevention strategies. 225 Current TBI CDEs, such as the GCS or GOSE, may need to be modified (as has already been done for pediatric TBI 226 –228 ); existing validated measures may be borrowed from other disciplines such as geriatric medicine, trauma surgery, or neurology; and some measures may need to be developed and validated de novo.
Last, TBI is now a well-established risk factor for neurodegenerative diseases of aging, including AD and PD, but mechanisms are poorly understood. Geriatric TBI presents an opportunity to understand the biological basis for the association between TBI and neurodegenerative disease in a patient population already at elevated risk for aging-related neurodegeneration. Prospective human studies of post-TBI neurodegeneration are challenging given the often decades-long delay between TBI exposure and neurodegenerative disease onset. By studying geriatric TBI, this delay is substantially shorter and may allow for novel insights into links between TBI and neurodegeneration that will directly inform targeted treatment and prevention of post-TBI neurodegenerative diseases among survivors of TBI across the age spectrum.
Conclusions
The world's population is aging and growing. The number of older adults presenting to EDs and being admitted to neuro-ICUs for management of TBI is expected to continue to increase in the coming years. There is an urgent need to develop better geriatric-specific prognostic models 210,214,229 and evidence-based geriatric TBI treatments and management guidelines to identify patients who would benefit most from aggressive versus conservative management and to optimally tailor treatment, rehabilitation, and prevention strategies. The first steps will involve designing more inclusive studies of older adults with TBI that incorporate core geriatric research principles, such as avoiding age cutoffs (masquerading as exclusion criteria for comorbidities) and incorporating measurements of pre-injury function, comorbidities, and frailty, which may prove more predictive of outcome after geriatric TBI than numerical age and trauma severity alone. The next critical steps will be development of geriatric-specific TBI CDEs, including geriatric functional assessments, tailored neuroimaging protocols, and validated biomarkers. Only then will we be able to improve diagnosis, clinical care, recovery monitoring, clinical trial endpoints, and eventually short- and long-term outcomes in the large and growing geriatric TBI population.
Footnotes
Acknowledgments
The authors extend their sincere gratitude to Evans Whitaker, MD, MLIS, an outstanding UCSF medical librarian and former physician who provided critical citation search support for this review. They also extend their sincere gratitude to Amy Markowitz, JD, an exceptional science editor who provided critical editorial support for this review. This work was supported by the National Institute for Neurological Disorders and Stroke (Beeson K23NS095755; to R.C.G.) and the American Federation for Aging Research (to R.C.G.).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.