
Abstract
Pressure ulcers (PUs) are common debilitating complications of traumatic spinal cord injury (SCI) and tend to occur in soft tissues around bony prominences. There is, however, little known about the impact of SCI on skin wound healing because of the lack of suitable animal models for studies in controlled experimental settings. Herein, we describe a reproducible and clinically relevant mouse model of PUs in the context of complete SCI. Adult male mice (BALB/c) were subjected to thoracic (T9–T10) complete SCI. Immediately after, a skin fold on the back of mice was lifted and sandwiched between two magnetic discs held in place for 12 h, thus creating an ischemic area that developed into a PU over the following days. The wounded areas demonstrated tissue edema and epidermis disappearance by day 3 post-magnet removal. PUs spontaneously healed, although slower in SCI mice compared to control non-SCI mice (5 vs. 3 weeks; p < 0.001). A similar delay in healing was observed for full-thickness excisional wounds. Histology data showed that there was a slower migration of epidermal cells over the granulation tissue in the SCI group compared to the control group. The SCI group also showed the smaller thickness of epidermis and dermis, lower blood vessel density, decreased numbers of proliferating cells, and decreased expression of alpha-smooth muscle actin compared to the control group at the time of wound closure. Taken together, these data suggest that SCI significantly slows down the dynamics of skin wound healing in experimental pressure and excisional wounds in mice.
Introduction
P
Metabolic and physiological changes reported in SCI patients, such as compromised blood flow regulation in tissues innervated below the level of SCI, 9 are believed to be major factors impeding the wound healing process. 1 However, there have been no studies in controlled experimental settings to investigate the impact of SCI on the PU healing process because of the lack of suitable animal models. Here, we describe a reproducible and clinically relevant mouse model of PU in the skin. This model can be used to study the dynamics of PU development and healing, as well as to test potential therapeutic approaches to prevent PUs or improve PU healing in the context of SCI.
Methods
Animal studies were conducted in accord with a protocol approved by the Rutgers University Institutional Animal Care and Use Committee. Mice were fed standard diet (PMI Nutrition International, Brentwood, MO) and water ad libitum. Adult Balb/c male mice (9 weeks old; 21–25 g) were purchased (Charles Rivers Laboratory, Wilmington, MA) and, upon receipt, randomly placed into cages (4–5 mice/cage) to acclimate to the laboratory environment for 7 days preceding surgery. Mice were kept on a 12:12 light/dark cycle and group-housed in a controlled-environment animal room.
Spinal cord injury
One the day before surgery, the back of mice was shaved using electric clippers and Nair™ cream from neck to tail. On the next day, mice were randomly picked from cages then were alternately assigned into either SCI or control (non-SCI) groups. Mice assigned to the SCI group received a low-thoracic complete spinal cord transection. 10 Briefly, mice were anesthetized with isoflurane (Henry Schein Animal Health, Dublin, OH), and, using an aseptic technique, a partial laminectomy was performed at vertebral level T9–T10, after which the spinal cord was cut using spring scissors. Spinal cord rostral and caudal ends were lifted to confirm complete transection and a piece of subcutaneous fat was applied over the laminectomy site to provide additional protection to the spinal cord before surgical site closure. Mice received buprenorphine (0.01–0.05 mg/kg, intraperitoneally) post-surgery, were placed in pre-warmed (37°C) cages to maintain body temperature, and housed individually thereafter. Postoperative care of SCI mice included immediate subcutaneous injection of saline (1 mL) for resuscitation, daily meloxicam (1 mg/kg), cefazolin (50 mg/kg for 7 days), and daily bladder evacuation. Mice assigned to the non-SCI group received a sham surgery, where they were handled similarly, but were not subjected to SCI.
Pressure ulcer and excisional wound induction
Wounds were created immediately post-SCI (or sham-SCI) and during the same surgical session while the animal was under general anesthesia. Some animals received PUs, whereas others received excisional wounds Further, some animals received wounds above and some below the SCI site. PUs were created by sandwiching a dorsal skin fold between two magnets ∼2 cm below the SCI site on the back of mice. Before magnet application, 10 μL of (0.125%) bupivacaine solution was injected at equidistant places approximately 0.5–1.0 cm apart, in an ellipse around magnet application site. The skin was gently lifted and two magnets (5 × 12 mm diameter, 2.4 g weight, 3800-G magnetic force) were placed on opposite sides of the skin fold. After 12 h, magnets were removed. Excisional wounds were created on the back of the mouse. A template was used to mark a 1 × 1 cm area of skin, and the area was cut out using scissors while gently lifting the skin up. The wounds were digitally photographed and covered with Tegaderm™ (3M, St. Paul, MN). The wounds were monitored until complete closure. Digital photographs were captured weekly and compared to the initial images using ImageJ (NIH, Bethesda, MD). Wound closure percentage was calculated as (1-remaining wound area/initial wound area) × 100.
Locomotion assessment
The Basso Mouse Scale (BMS) was used to monitor the progress of hindlimb functional recovery post-SCI, with scores ranging from 0 (no ankle movement) to 9 (complete functional recovery) points. 10 BMS scores were recorded at day 2 and then weekly post-SCI by two independent examiners who were blind to the experimental conditions. When differences in the BMS score between the right and left hindlimbs were observed, the average of the two scores was used.
Histology and immunohistochemistry
On post-wounding days 3, 5, 7, 10, 21, and 35, mice were sacrificed, wounds excised, and tissues were processed for histology and immunohistochemistry as previously described. 11 –13 Briefly, wound tissues were fixed in 10% formalin for 24 h and then stored in ethanol at 4–8°C. Tissues were then paraffin-embedded and thin sections (5 μm thick) stained with hematoxylin and eosin (H&E) to visualize tissue morphology and measure the thickness of epidermis and dermis using ImageJ (NIH). For immunohistochemistry, tissues were de-paraffinized and rehydrated, followed by antigen retrieval (2100 Antigen Retriever). Sections were then rinsed in pphospphate-buffered saline (PBS) followed by endogenous hydrogen peroxide blocking (3% H2O2 in PBS, 20 min). For blocking nonspecific staining, sections were stained with serum-free protein (20 min, room temperature [RT]; Dako, Glostrup, Denmark), and endogenous biotin blocking using an Avidin/Biotin reagents kit (Vector Laboratories, Burlingame, CA) with washing the sections at each step by Tris-buffered saline with Tween 20 (TBST; 2 × , 5 min each). Then, sections were stained overnight with primary antibody, namely anti-alpha-smooth muscle actin (α-SMA; Rabbit Monoclonal immunoglobulin G [IgG], 1:2000; Epitomics, Inc., Burlingame, CA), CD31 (Rabbit Polyclonal IgG, 1:200; Abcam, Cambridge, MA), and Ki67 proliferation antigen (Rabbit Monoclonal IgG, 1:1000; Lab Vision Corporation, Fremont, CA) followed by secondary antibody (Biotinylated Goat Anti-Rabbit, 1:200; Vector Laboratories). Sections were then washed (TBST, 2 × , 5 min each), stained with working ABC reagent (VECTASTAIN® ABC kits, 30 min at RT; Vector Laboratories), NovaRed Solution (5 min at RT), and counterstained with Mayer's hematoxylin and Scott's bluing reagents, with intermediate washes with dH2O. Sections were then dehydrated and mounted using Cytoseal 60. Sections were also stained with normal rabbit Ig fraction (1:400,000; Dako) overnight at 4°C as a negative control. The % positive area (sum of dermis and epidermis) for Ki67, α-SMA, and CD31 in stained sections was determined by ImageJ (NIH). Thickness of epidermis and dermis was measured at three locations (two edges and one center), and the averaged value was used for each section. Two sections were averaged for each animal. A similar method was used for immunohistochemistry studies.
Statistical analysis
Data are represented as mean ± standard error of the mean (SEM). Statistical analysis consisted of one-way analysis of variance (ANOVA) followed by Fisher's least significant difference (LSD) multiple comparison tests using KaleidaGraph software, or Student's t-test when only two groups were compared. A p value <0.05 was considered statistically significant.
Results
Standardization of skin pressure ulcers in spinal cord injury mice
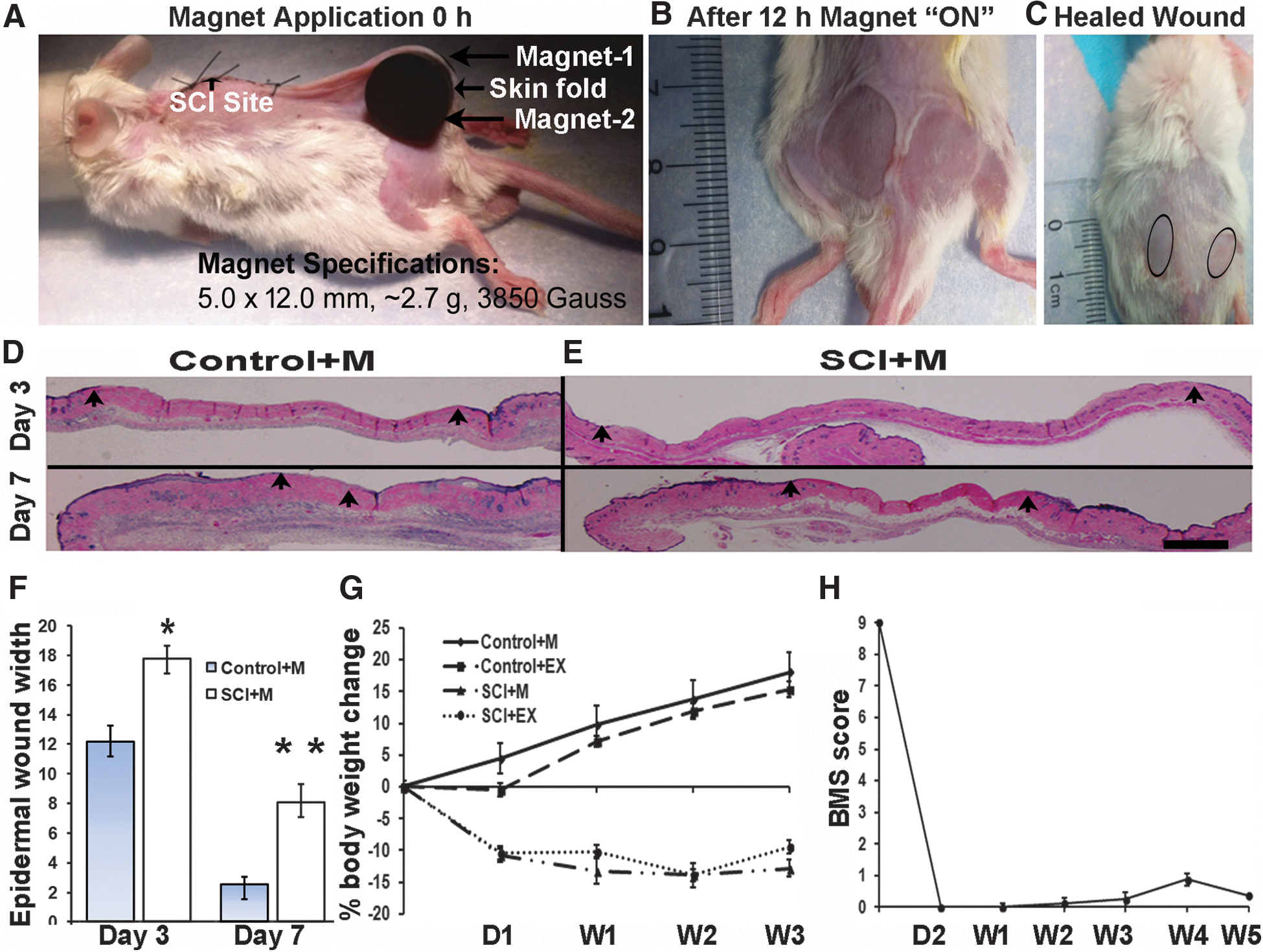
All mice with or without SCI tolerated the magnets very well, which remained in their original position for the full 12 h. Food and water consumption remained normal throughout the experimental period as noted with and without injury. Visual assessment of the wound sites was conducted at days 3, 5, 7, and 10, then weekly up to 35 days post-magnet-induced injury. The wounds were graded per the criteria specified in Table 1. The initial wounding response was similar in mice with or without SCI (Fig. 1A–C). All the mice developed two circular wounds separated by a bridge of normal tissue (Fig. 1B).
Experimental procedure for creating pressure wounds in SCI animals. (
Mean ± SD.
SCI, spinal cord injury; PU, pressure ulcer; SD, standard deviation.
A subset of mice was sacrificed at early time points (days 3 and 7 post-injury) to assess the difference in early PU development between control and SCI groups. Histological analysis showed the disappearance of epidermis at day 3 and reappearance at day 7 in control non-SCI mice (Fig. 1D). A similar pattern was observed in SCI mice (Fig. 1E), albeit with a significantly slower migration of epidermal cells at both time points (p < 0.05 and p < 0.01, respectively; Fig. 1F).
At the systemic level, body weight of mice with or without SCI was recorded on post-skin injury day 1 and weekly thereafter. SCI mice exhibited lower body weight compared to control non-SCI mice at all time points (ANOVA, p < 0.001; Fig. 1G), which is consistent with literature data. 14 To confirm that complete SCI was achieved in the SCI group, mice were assessed for their locomotor recovery post-SCI (Fig. 1H). The BMS score on day 2 post-SCI was 0.058 ± 0.058 (median 0-no movements, n = 17) and did not reach BMS score 1 (slight ankle movement) by week 5 (0.35 ± 0.12, median-0, n = 17). These scores are consistent with complete transection injury and absence of recovery during the experimental time frame.
Pressure ulcer development and healing below the spinal cord injury site
All mice developed two circular PUs separated by a narrow bridge of normal tissue after 12 h of magnet application. PU size reached its highest value around day 10 irrespective of the group of mice. In the control non-SCI group (Fig. 2A, top panel), PUs healed completely (re-epithelialization) by day 21, versus day 35 in the SCI group (Fig. 2A, bottom panel). Time to wound closure was significantly increased (ANOVA, p < 0.0001) in the SCI group (Fig. 2B). Percent closure was significantly lower from 7 days onward in the SCI group. Interestingly, the wound appearance was also different in the SCI group, whereby the color of the tissue in the wound area remained pale throughout the process in the SCI mice, whereas non-SCI mice exhibited a deep red color until the wound was completely closed. Scar area of healed SCI mouse wounds was significantly larger (p < 0.001) compared to control non-SCI mice, suggesting a decreased contribution of wound contraction in the skin wound healing process in the SCI group (Fig. 2C–E). Histology data show significantly thinner (p < 0.01) epidermis and dermis in SCI mice as compared to control non-SCI mice at their wound closure time (days 35 and day 21, respectively; Fig. 2F–H).
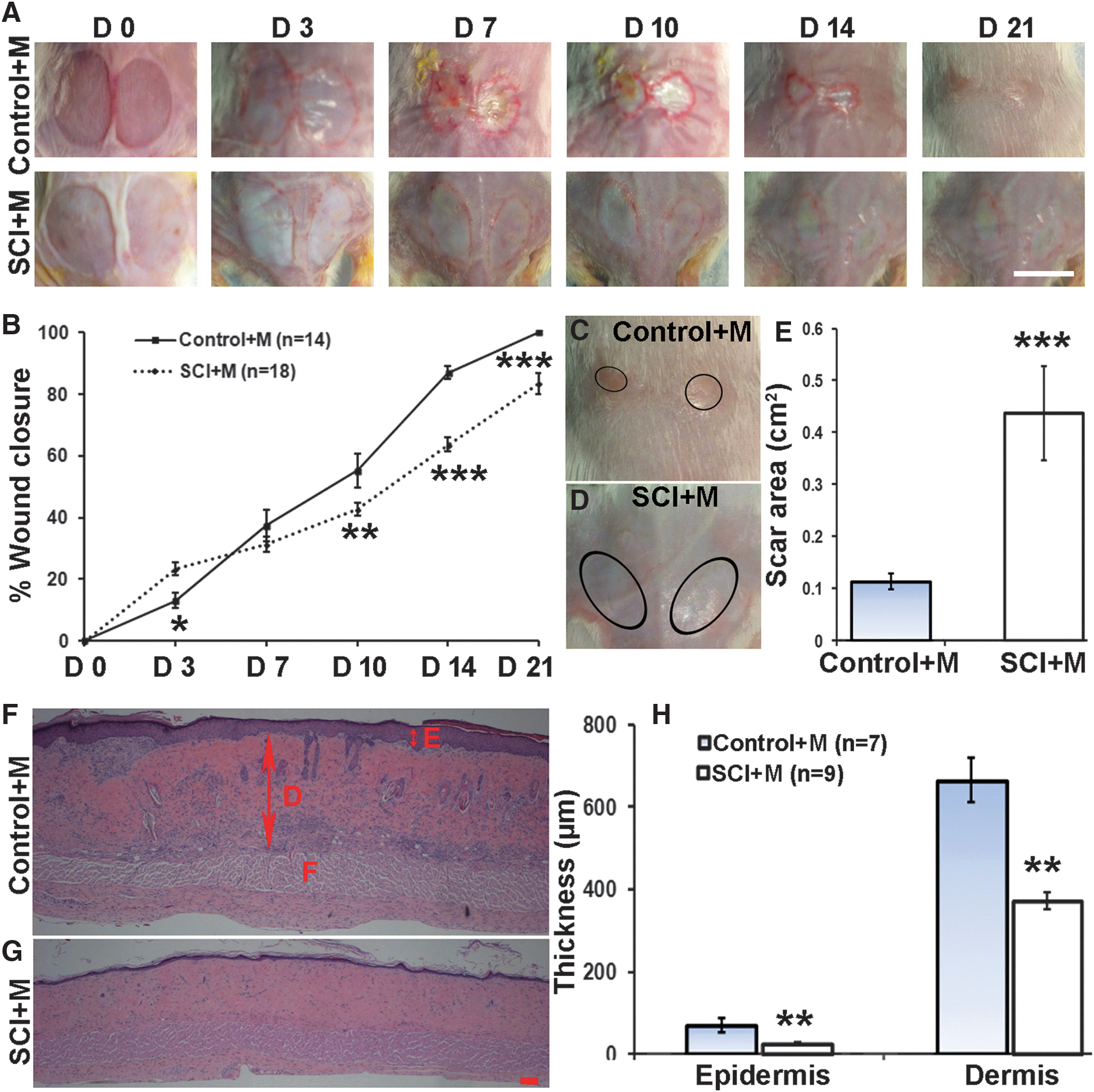
Impact of SCI on magnet-induced PU development and healing. (
To further assess the impact of SCI on the wound healing dynamics, we also analyzed the wound tissue sections for the density of proliferating cells (Ki67+ cells), blood vessels (CD31+ cells), and α-SMA. The % area of tissue expressing Ki67 was significantly lower (p = 0.011) in SCI versus non-SCI control mice (Fig. 3A–C). Similarly, the % area of CD31+ cells (Fig. 3D–F, p = 0.023) and α-SMA fibers (Fig. 3G–I, p = 0.002) was significantly decreased in wounds of SCI mice as compared to control non-SCI mice.

Expression of Ki67, CD31, and α-SMA in PUs of control non-SCI and SCI mice. Wound tissues were harvested after wound closure, namely on days 21 (Control+M) and 35 (SCI+M) post-PU induction. Images are that of representative 5-μm-thick sections (5 μm) stained with anti-Ki67, anti-CD31, or anti-α-SMA and visualized with a 40 × objective. Representative images of non-SCI control (
Excisional wound development and healing below the spinal cord injury site
Because full-thickness excisional wounds (1 × 1 cm) are more commonly used to evaluate experimental skin wound therapies in the field, we also performed a comparison between SCI and non-SCI mice in the healing of such wounds. Excisional wounds were created (D0) similarly and monitored for their healing pattern in control non-SCI (Fig. 4A, top panel) and SCI groups (Fig. 4A, bottom panel). Excisional wounds healed at the same rates as the PUs, with wound closure observed at day 21 in the non-SCI control group, and at day 35 in the SCI group, a statistically significant difference (ANOVA, p < 0.0001; Fig. 4B). Wound healing dynamics were clearly slower from 7 days onward in the SCI group. As was the case for PUs, wounds in SCI animals remained white in color and contracted less (p < 0.05), whereas those in control non-SCI exhibited a red color with more active contraction (Fig. 4C–E). Wound cross-sections also revealed a thinner dermis (p < 0.02) and epidermis (p > 0.05) in the SCI group (Fig. 4F–H). Furthermore, significant decreases were observed in the SCI group for Ki67 levels (p < 0.01; Fig. 5A–C), CD31 levels (p < 0.05; Fig. 5D–F), and α-SMA expression (p < 0.05; Fig. 5G–I). Thus, the effect of SCI on the wound healing response of excisional wounds was very similar to that of pressure wounds.
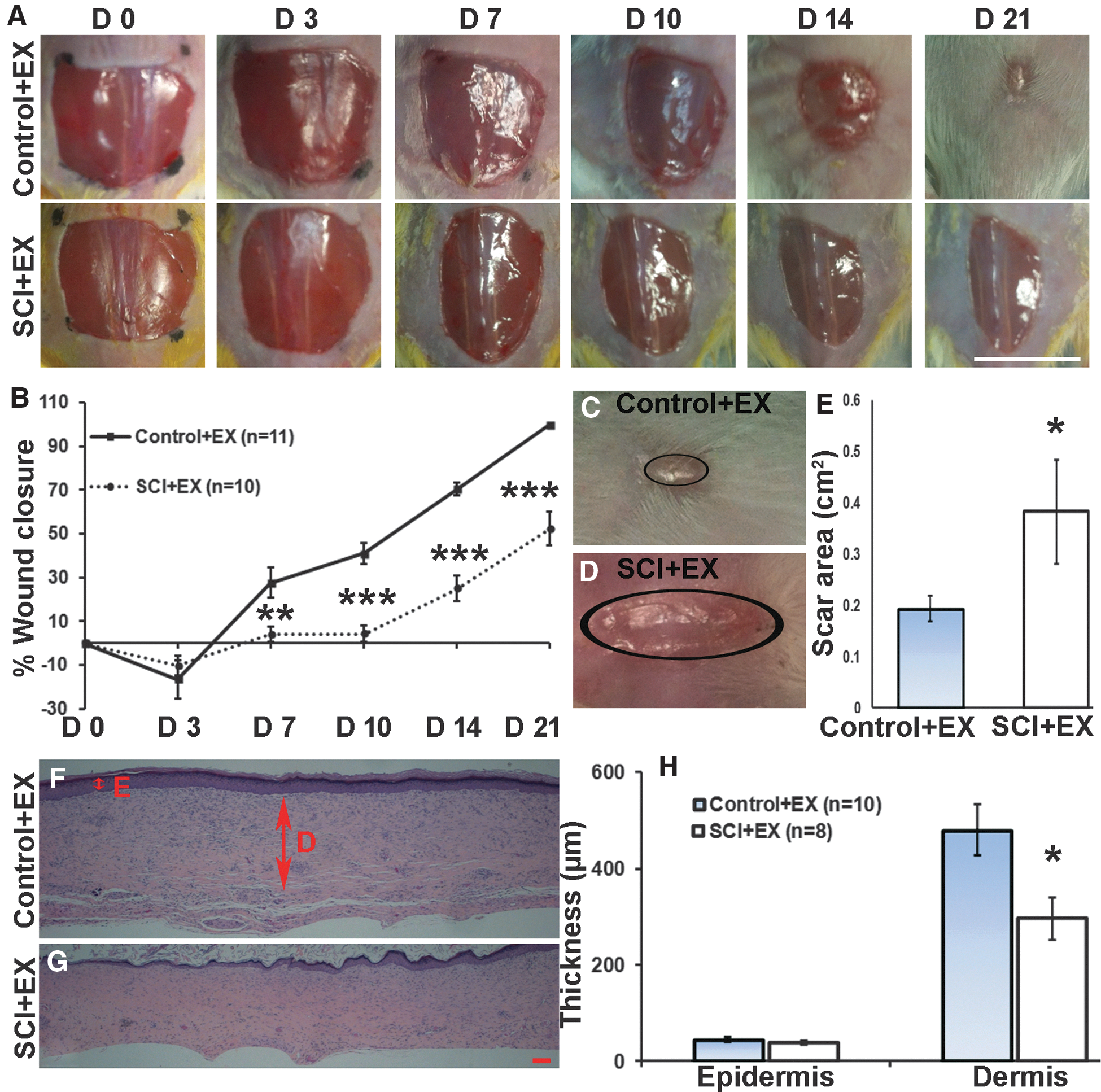
Impact of SCI on excisional wound (EX) healing. (
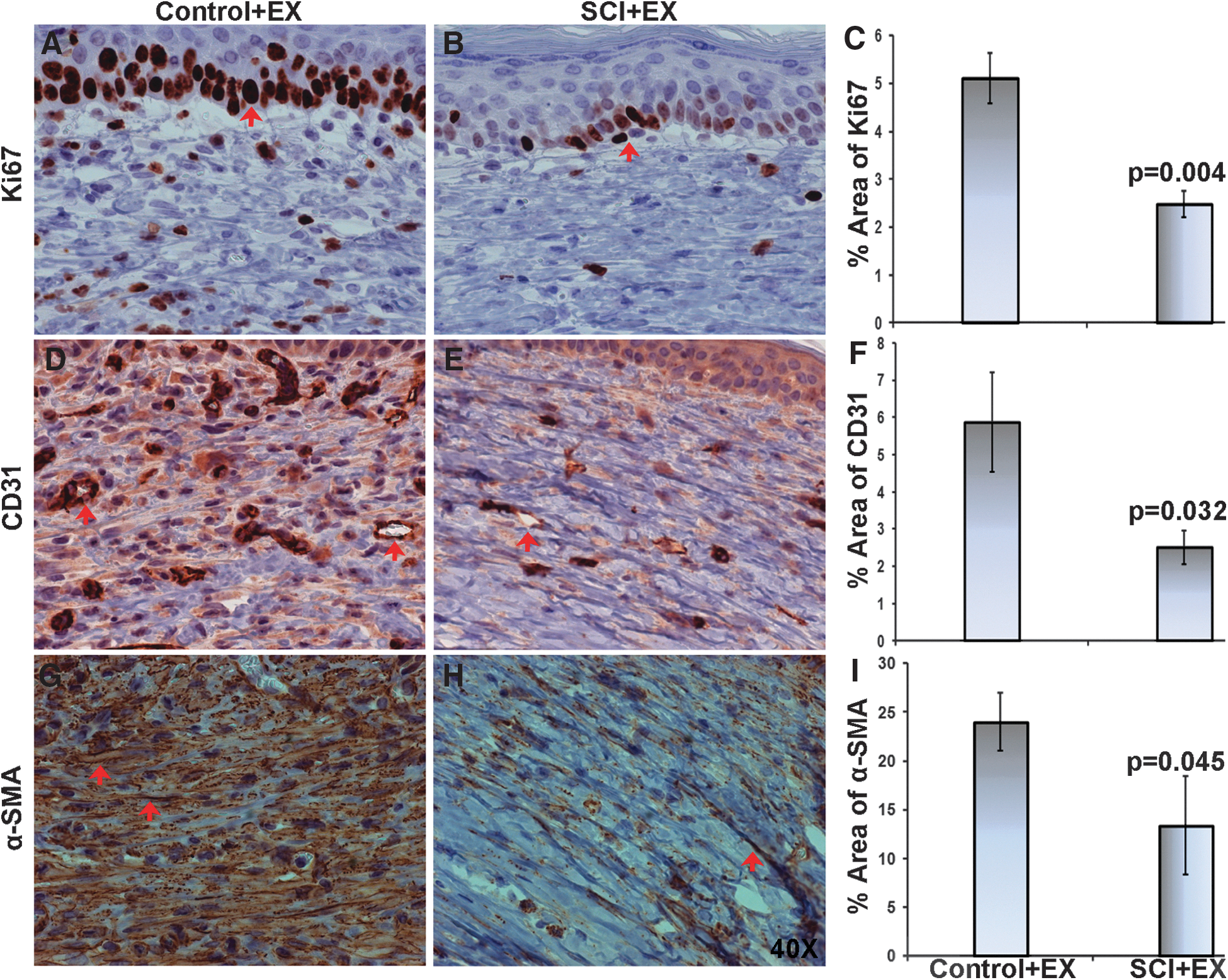
Expression of Ki67, CD31, and α-SMA in excisional skin wounds of control non-SCI and SCI mice. Wound tissues were harvested on days 21 (Control+M) and 35 (SCI+M) post-wounding by excision. Images are that of representative 5-μm-thick sections stained with anti-Ki67, anti-CD31, or anti-α-SMA and visualized with a 40 × objective. Representative images of non-SCI control (
Pressure ulcer and excisional wound development and healing above the spinal cord injury site
To determine whether the wound healing impairment by SCI is attributed to local loss of connection with the central nervous system, or rather a systemic effect of SCI, we determined whether SCI would similarly impact pressure and excisional wounds created above the site of injury. Therefore, mice were subjected to SCI using similar methods, and then received pressure wounds or excisional wounds above the SCI site. These wounds spontaneously healed by day 21, showing no difference between the SCI and control non-SCI groups (Fig. 6A–D). The evaluation of the percent wound closure as a function of time was also comparable between non-SCI and SCI mice. For excisional wounds, there was a trend toward smaller scar in the SCI group, although the effect was not statistically significant (p = 0.145; Fig. 6E). For pressure wounds, there was no difference in scar area between SCI and non-SCI mice (p = 0.588 for pressure wounds). Post-healing wound histology suggests thinner epidermis and dermis in the SCI groups for both pressure and excisional wounds, although the effect was not statistically significant (p = 0.39, p = 0.37 and p = 0.177, p = 0.208, respectively; Fig. 6F,G).
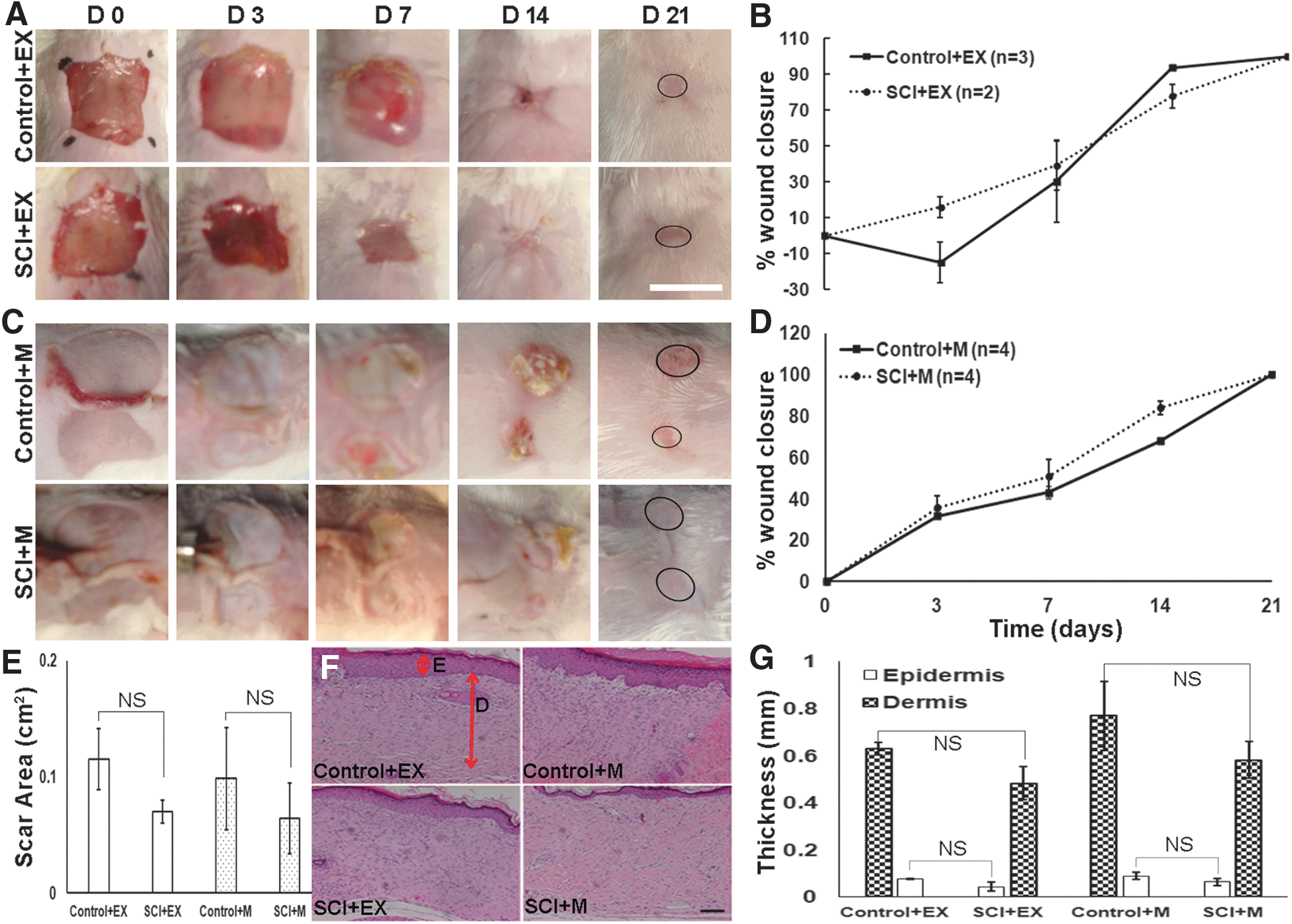
Impact of SCI on development and healing of excisional wounds and PUs above the SCI site. (
Discussion
In this study, we report on a novel experimental model of PUs to evaluate the impact of SCI on wound healing. PUs were induced by a 12-h application of two 12-mm-diameter disc magnets on a dorsal skin fold. Such wounds healed with dynamics that were very similar to that observed in commonly used 1 × 1 cm full-thickness excisional wounds. Post-SCI, skin wounds below the level of SCI healed much slower, taking 35 instead of 21 days. Skin wounds exhibited decreased wound contraction, which resulted in a larger scar with thinner epidermis and dermis. Markers that are associated with the wound healing process, such as Ki67, CD31, and α-SMA, were expressed at lower levels in wounds of SCI animals. Taken together, these results show that SCI slows down skin wound healing in mice. Importantly, these observations were specifically observed in skin wounds below the innervation level of the SCI, because wounds made above the SCI level were largely unaffected in their wound healing pattern as compared to the control non-SCI group.
Although there have been several reports in the literature describing models of PUs with varying severity and in different animal species, 3 very few involve simultaneous SCI. 15 –17 Hyodo and colleagues developed a swine monoplegic model by surgical resection of the unilateral lumbar nerve roots. 15 A pressure applicator was percutaneously implanted into the greater trochanter of the monoplegic pig to create grade intravenous PUs, which were characterized by gross morphology descriptions during the healing process. Yu and colleagues used magnetic-induced compression in the left thigh of rats subjected to complete spinal cord transection (T11–L1) to test the effect of electric stimulation on wound healing; however, animals exhibited relatively low survival rate (17%). 16 Ahmed and colleagues described methods to produce PUs of varying severity 7 days after partial SCI (thoracic hemisection) in rats using C-clamps applied for 8 h at varying pressures on the thighs of the paralyzed hindlimbs. 17 Blood flow and blood count changes were monitored for up to 5 days post-injury. In these studies, there was no comparison in the healing behavior of the PUs between normal and denervated skin. 15 –17 This is the first report that provides a direct comparison of the healing dynamics of skin wounds between SCI and normal animals.
The compressive force between two magnets, which is expected to substantially exceed capillary and venous perfusion pressures in the skin, has been well documented to be an appropriate degree of compression to induce lesions in larger animals. 18 Previously, repeated cycles of magnet application have been used to create PUs of varying severity 11 ; however, we found in our mouse model that a single cycle was sufficient to create a PU that had injury extending deep into the dermis. The method resulted in a PU that was highly reproducible and of a size that healed with similar dynamics as commonly used 1 × 1 cm full-thickness excisional wounds. PUs generated by magnet application seemed to fall within stages I and II according to the staging system of Stadler and colleagues 11 ; although the panniculus carnosus is destroyed, the underlying skeletal muscle is not involved in the procedure, which provides a reasonable wound bed for testing various therapeutic strategies. Further, the methodology does not require a complex device and does not impair the animal's ability to freely roam. The site of PU generation does not interfere with the skin incision used to access the site of SCI. This model allows side-by-side evaluation of the effect of SCI on wound induction and healing.
PU causation in humans is a multi-factorial process associated with several extrinsic factors (pressure, shear, duration of loading, temperature, moisture, and hygiene) 19 and intrinsic factors (general physical conditions, morphology of bone and tissues, and muscle tissue mechanical properties). 20 –24 In this study, we could eliminate most of these variables, although SCI had profound systemic effects, on body weight gain, which was completely stunted post-SCI. Nevertheless, the inhibitory effect of SCI on skin wound healing was only observed when the skin injury was below the level of the SCI. Thus, systemic effects of SCI seem to have little impact on wound healing, and the mechanism is likely to involve local effects attributed to the loss of innervation to the wound area. A common underlying cause often cited involves blood flow changes within the affected tissues attributed to SCI. 25 Hyperemic response and reactive hyperemic response are decreased in SCI based on laser Doppler flow measurements. 26 Along the same lines, it has been suggested that compromised blood flow in dermal arterioles results in skin lesions, a further indicator of altered blood flow in SCI individuals. 27 Consistent with such observations are our histological data, showing decreased blood vessel density in wounds of SCI animals, even after the wound healed, which is consistent with decreased blood flow 9,28 in patients and experimental models with SCI. 17
Even with the best hospital care and education, SCI patients are substantially challenged and PUs impart significant cost to the U.S. healthcare system. The potential exists for the animal model described herein to study therapies for both patients who are at risk and those affected by PUs. Such therapies may focus on ways to strengthen the skin and decrease ischemic injury by a free radical scavenging system or methods to increase blood flow in the pressure ulcer susceptible areas. 17 These modalities will be relevant to SCI patients as well as others at risk for pressure ulcers development (like elderly, malnourished patients, diabetic patients, or chronically deconditioned patients).
Conclusions
We have created a simple, reproducible, and clinically relevant mouse model of PU formation in the experimental setting of SCI. PUs, as well as experimental excisional wounds, exhibit a significant and similar delay in wound closure in SCI animals. This delay is observed specifically when the wounds occur below the innervation level of the SCI and is associated with decreased activity of various cellular processes required for wound closure and repair.
Footnotes
Acknowledgments
This work was partially supported by the New Jersey Commission on Spinal Cord Research (CSCR15IRG010), the U.S. Department of Defense (SC160029), and the Yale Department of Surgery Ohse Research Grant Program. We thank Sean O’ Leary from the Keck Center for Collaborative Neuroscience and Yuying Tan from the Department of Biomedical Engineering for technical assistance.
Author Disclosure Statement
No competing financial interests exist.