
Abstract
Mild traumatic brain injuries (mTBIs) commonly occur in children and adolescents and can result in persistent cognitive symptoms. The neurophysiological changes that underlie persistent post-concussive symptoms (PPCS) have not been characterized. Our objective was to compare working-memory related functional magnetic resonance imaging (fMRI) response in children with persistent symptoms after mTBI at one month post-injury to children with typical recovery and healthy controls. This was a prospective, controlled cohort study of children with mTBI at one month post-injury. PPCS was defined as children with a 10-point increase in their post-concussion symptom inventory score (compared with pre-injury score) at one month post-injury and a two-point increase in at least two symptom categories compared with pre-injury. One hundred and seven participants (60 PPCS, 30 recovered mTBI, and 17 controls) with a mean age of 14.2 years (standard deviation [SD] 2.5) (44% male) were assessed 38 (SD 5.9) days after mTBI. The primary outcome measures were visuospatial n-back working memory task performance and fMRI blood oxygen level dependent (BOLD) signal change. Children with PPCS had decreased activation relative to children with typical recovery in the posterior cingulate and precuneus during the one-back working memory condition, despite similar task performance. Differences in cortical activation in children with PPCS at one month highlight the persistent neurobiological consequences of pediatric mTBI on working memory cortical activation. These findings encourage recommendations to avoid contact sports and provide continued care at school for children with persistent symptoms at one month post-injury.
Introduction
Traumatic brain injuries (TBI) have a substantial global impact. 1 Mild TBIs (mTBI) or concussions account for up to 90% of all TBIs and occur when a direct or indirect force is applied to the head, resulting in brain dysfunction. 2,3 Children and adolescents are at the highest risk of sustaining such injuries. 4 Although most children recover after an mTBI, a substantial proportion continues to experience physical, cognitive, mood, and sleep related symptoms—known as post-concussion syndrome (PCS).
Up to 50% of children will continue to remain symptomatic one month post-injury, experiencing persistent post-concussion symptoms (PPCS), and 13% continue to be symptomatic three months post-injury. 5 This extended period of recovery can significantly affect the social functioning and quality of life of the child and family. 5 –7 Little is known about the neurobiological explanations of PPCS in children and youth, and what leads to the prolongation of post-concussive symptoms for some but not others. 8,9
Of particular concern are the cognitive difficulties that children with PPCS report, especially as they occur during a time of life that is critical for cognitive development. 10 –15 Common complaints after mTBI are concentration difficulties and memory problems. 13,15 Working memory is the ability to hold recent information and transiently manage it for goal-directed behaviors. 16 –18 Neuropsychological tests, however, rarely detect differences in objective performance on working memory tasks in children after mTBI. 17 –20 Functional neuroimaging may help to characterize the pathophysiology underlying subjective complaints.
Functional magnetic resonance imaging (fMRI) studies of working memory in adults with mTBI suggest altered cortical activation patterns. Both hypo- and hyperactivation have been noted with the direction of differences largely dependent on the time point of observation after injury. 13,21 –28 Acutely, hyperactivation of the posterior cingulate was observed in symptomatic patients with mTBI without task performance differences. 21 Subacutely, a few smaller studies observed hyperactivation one month after injury, specifically in the parahippocampal gyrus and posterior cingulate gyrus in the latter study. 13,22,23
In contrast, in a larger study (n = 55), Van der Horn and colleagues 28 observed hypoactivation in the dorsolateral prefrontal cortex (DLPFC) in symptomatic adults with mTBI compared with greater default mode deactivation in individuals who no longer experienced symptoms one month after injury. Lower task related activation in DLPFC has also been associated with symptom severity, and “recovery” of working memory activation differences occurred over time. 26,27
As a whole, this research suggests that neurocognitive performance is maintained after sustaining an mTBI as an adult, but subjective complaints and functional differences still persist up to six months after injury. Note that because of the nature of this condition, few studies have baseline measures of the condition of the participant against which to compare performance.
Cortical activation during working memory remains largely unexplored in the mTBI pediatric population. Working memory fMRI studies in the acute phase after pediatric mTBI have mixed findings regarding abnormal activation in the working memory circuitry, with studies finding prefrontal and parietal hyperactivation that correlates either positively or negatively with symptom severity, depending on the study. 29 –31 The nature and location of activation differences have not been thoroughly elucidated in the subacute recovery phases. 32,33 Studies in the subacute PCS phase have observed cerebellar hyperactivation, but also widespread hypoactivation including the DLPFC, other parts of the prefrontal cortex, and motor areas. 32,33
Finally, smaller studies have examined cortical activation in the chronic phase with uncertain findings, some indicating hyperactivation and others observing no differences that persist 20 months after injury. 34,35 The mixed findings may be explained by small sample sizes and variable reporting periods without longitudinal designs. 5,32
The objective of the work presented here is to investigate differences in fMRI blood oxygen level dependent (BOLD) response during a visuospatial working memory task in children experiencing PPCS one month after injury, compared with typically recovering children and controls with no history of mTBI. Given that previous research has shown differences localized to the DLPFC, a subset of analyses focused specifically on this region. 26 –28,32,33
Methods
Participants
Three groups were recruited for this study: (1) children with an mTBI and persistent PCS at one month post-injury; (2) children with an mTBI who were asymptomatic (PCS symptoms back to pre-injury levels) at one month post-injury; and (3) healthy control participants without a history of mTBI. Children aged eight to 18 years inclusive were recruited from the emergency department at the Alberta Children's Hospital if they presented with an mTBI within 14 days of their injury, as defined using the American Academy of Neurology criteria: a biomechanically induced alteration in brain function with one or more symptom(s) after injury. 36
Children were excluded if they had loss of consciousness greater than 30 min or a Glasgow Coma Scale (GCS) score of less than 13, a mTBI within the previous three months, or failure to recover from a previous mTBI, significant past medical or psychiatric history (attention deficit hyperactivity disorder [ADHD]/attention deficit disorder [ADD] diagnoses were not excluded), use of neuroactive drugs that could affect fMRI, an inability to complete questionnaires or evaluations, and had a contraindication to MRI.
The Post-Concussion Symptom Inventory for Youth (PCSI) was used to assess symptoms. 37 The questionnaire assesses symptoms in four domains: somatic, cognitive, emotional, and sleep and has been shown to be a reliable measure of PCS with good internal reliability. 5,6 Clinically significant symptomology was defined as an increase of 10 points compared with retrospective pre-injury PCSI report collected at the same time (symptomatic group). 38 The asymptomatic group consisted of participants whose total PCSI score had returned to pre-injury level or less and who reported no differences compared with their pre-injury status. Controls were recruited through family and friends of mTBI participants. Controls were excluded if they had a history of mTBI, MRI contraindication, or inability to complete the study questionnaires.
Study design
This was a prospective, controlled cohort study. This study received ethical approval by the University of Calgary Health Ethics Research Board (13-0372). Children were also scanned again at two months post-injury, the results of which are not presented in this article.
Procedure
Participants were scheduled for a visit approximately one month post-injury. Consent and assent were obtained from the parent and child, respectively. A health assessment with a trained medical professional was performed that included the collection of demographic and injury details and details of past medical and family history. Socioeconomic status was determined by average family income. Outcome measures were collected and, subsequently, participants completed preparation for MRI, including safety screening, practice in a mock scanner for younger children, and training on the n-back task with a graduate student or research assistant, followed by an MRI. Symptom validity testing was employed to separate participants with either insufficient effort or exaggerated impairment using the Test of Memory Malingering (TOMM). 39,40
Neurocognitive assessment
Subjective cognitive difficulties were examined using the PCSI cognitive domain questions “feeling slowed down,” “mentally foggy,” “difficulty concentrating,” and “difficulty remembering.” A score of one or more was considered a positive complaint.
A computerized neurocognitive assessment, CNS-Vital Signs, was used to objectively measure cognition on the day of MRI. 41 This assessment consisted of seven tests: Verbal Memory, Visual Memory, Finger Tapping, Symbol Digit coding, Stroop test, Shifting Attention test, and the Continuous Performance test (age adjusted with a mean of 100 and SD of 15). It has high test-retest reliability in this population (Pearson r = 0.63–0.82) and demonstrates concurrent validity with traditional neurocognitive testing measures. 41 –44 The composite neurocognition index (NCI) is the average of five domain scores: Composite Memory, Psychomotor Speed, Reaction Time, Complex Attention, and Cognitive Flexibility and was used as a global score of neurocognition.
Statistical analyses
Descriptive and cognitive performance statistics were performed using IBM SPSS Statistics 19 (IBM Corp. Released 2010. IBM SPSS Statistics for Windows, Version 19.0 Armonk, NY: IBM Corp.). The Shapiro-Wilk test was used to test normality of data. 45 Normally distributed data are presented with means and standard deviation (SD). Means for the three independent groups were compared with analysis of variance (ANOVA) and presented with post hoc pairwise Bonferroni or Tukey tests. Means for two independent samples were compared with an independent samples t test, and two dependent samples were compared with a paired samples t test.
Non-parametric data are presented with median and interquartile ranges (IQR). Three independent groups were compared with a Kruskal-Wallis test, and post hoc pairwise comparisons were made with a Dunn test. Two independent samples were compared with Mann-Whitney U test, and two dependent samples were compared with a Wilcoxon Signed-Rank Test.
fMRI
A visuospatial n-back working memory task using letter stimuli was designed in Eprime 2.0 (Psychology Software Tools Inc., PSTNET) for this study and is similar to that employed by Hockey and associates 46 and Dettwiler and coworkers. 47 On each trial, uppercase letters were presented in one of four circles in the top, bottom, left, or right positions.
The task included three levels of working memory load, n = 0, 1, 2. The 0-back condition required a response if the presented stimulus matched a pre-defined exemplar, acting as a control condition to account for visual and motor processing requirements of the task. The 1-back task required a response when two successive stimuli were identical, and the 2-back task required a response when identical stimuli were separated by one non-identical image.
The task had three experimental blocks of each cognitive load, for a total of nine blocks. Each block presented 20 images containing four correct responses and 16 incorrect responses. The task began with a 20 sec introduction, and each block began with a 10 sec slide informing the participant of the upcoming block, followed by a 15 sec fixation slide. Then, the stimulus was presented for 0.5 sec with an interstimulus interval (ISI) period of 1.5 sec. Stimuli were pseudo-randomized in each block.
Participants completed a practice task outside the scanner, where they completed one block of each cognitive load and required 75% accuracy to proceed. All participants completed practice training within two attempts.
Performance on the n-back working memory task was measured by reaction time and A-Prime (A'), calculated as a non-parametric measure using true positives and false positives. 48 Participants who scored below 0.6 on any task condition were excluded from the analysis because they may not have understood the working memory task. 48
MRI acquisition parameters
The fMRI BOLD signal during the n-back working memory task allowed for the measure of cortical activity in response to the task. The MRI data were acquired at the Alberta Children's Hospital (University of Calgary) 3.0 T GE Healthcare Discovery MR 750w Magnetic Resonance scanner using a 32-channel head coil. The fMRI images were obtained in the oblique axial plane using a Gradient Echo EPI pulse sequence with the following scanning parameters: repetition time (TR) = 2000 msec, echo time (TE) = 30 msec, flip angle = 90, number of dummy acquisitions = 5, field of view (FOV) = 23 cm, slice thickness = 3.6 mm, number of slices = 317, matrix = 64 × 64, scan time = 10:44 min, interleaved acquisition.
Two anatomical acquisitions were also acquired for registration: T1-weighted and T2-weighted images. The T2-weighted anatomical images were obtained with a T2 FRFSE-XL (fast relaxation fast spin echo) sequence with the following parameters: TR = 6216 msec, TE = 80 msec, echo train length = 26, flip angle = 111, FOV = 23 cm, slice thickness = 3.6 mm, scan time = 0:44 min, interleaved acquisition. The T1-weighted anatomical images were obtained with a FSPGR (fast spoiled gradient echo) BRAVO sequence with the following parameters: TR = 8.2 msec, TE = 3.2 msec, flip angle = 10, FOV = 24 × 24 cm, matrix = 300 × 300, number of slices = 230, slice thickness = 0.8 mm, scan time = 5:32 min.
fMRI processing pipeline
All MR pre-processing and analysis were completed using FSL FMRIB Software Library v5.0 (Oxford, UK)—specifically, the FEAT toolbox. 49 Motion correction, slice timing correction, BET brain extraction, spatial smoothing of FWHM 6.0 mm, and highpass temporal filtering with 200 sec period cutoff were applied. The fMRI images were registered to the brain extracted T2-weighted image and then to the brain extracted T1-weighted image. Images were standardized to the MNI152 2 mm brain template, using non-linear transformation, 12 d.o.f and 10 mm warp resolution. 50 FSL Motion Outliers was used to identify volumes exceeding a framewise displacement threshold of 0.5 mm.
If >25% of volumes during the task blocks were flagged for excessive displacement, the participant was excluded from analysis. Participants with an absolute displacement >4.0 mm were excluded. For retained participants, flagged volumes were censored during first-level general linear model (GLM) analysis. After exclusions for incomplete scans, inadequate performance on task (A' score <0.6), failing the TOMM, and excessive motion, participant files were prepared for first level analysis using FSL FEAT.
The first level analysis was run using univariate GLM, and three different explanatory variables (EVs) modeled the n-back task conditions, with block onsets convolved with a double-gamma hemodynamic response function with a 38.5 sec duration. 51 The following contrasts were run: 1-back >0-back; 2-back >0-back; and 2-back >1-back. Contrast images from first-level models were entered into group-level analyses. Activation maps were generated within each group to ensure that the task engaged expected regions of the working memory network. Group level comparisons were performed using a second level GLM, using FSL FEAT (FLAME). 52
Regressors for age, sex, handedness, and task performance were de-meaned for the entire sample and included in the model because these factors have been shown to influence working memory related activation. 53 –55 Contrasts were set up within this ANOVA model to assess differences between each of the symptomatic mTBI, asymptomatic mTBI, and healthy control groups.
Statistical inferences were drawn using a peak Z threshold of 2.3 (p < 0.01) cluster corrected for multiple comparisons at a p value of 0.05. Based on previous literature showing differences in the DLPFC, a region of interest (ROI) analysis was used to investigate differences in this region specifically, using a probabilistic middle frontal gyrus (MFG) mask taken from the Harvard-Oxford atlas (supplied as part of FSL and thresholded at 25% probability). 26,27,32,33 This mask was used to explore differences between the groups within the DLPFC, using the aforementioned statistical design and thresholds.
Results
One hundred and twenty-three participants met the study criteria. Sixteen participants were excluded either because of excessive motion during the MRI (n = 12), significant abnormality on neuroimaging (brainstem glioma; n = 1), and/or failure to pass the TOMM symptom validity test (n = 3) (Fig. 1). One hundred and seven participants (60 symptomatic, 30 asymptomatic mTBI, and 17 healthy control) were included in analyses presented here (Table 1). Groups were similar in age (sample mean 14.2 years, SD 2.5, F(2,104) = 0.017, p = 0.983), sex (sample proportion 44% male, χ2(2) = 1.506, p = 0.471), handedness (sample proportion 90% right, χ2(2) = 0.665, p = 0.717), and socioeconomic status (Kruskal-Wallis H test, χ2 (2) = 1.224, p = 0.542).
Table 1. Pre-Injury Characteristics
Pre-injury characteristics were similar between groups.
Pre-injury post-concussion symptoms were higher in children with persistent post-concussive symptoms (symptomatic) compared with children who had recovered (asymptomatic) and controls.
SD, standard deviation; ADHD, attention deficit hyperactivity disorder; PCSI, Post-Concussion Symptom Inventory for Youth; IQR, interquartile range.
Indicates p < 0.05
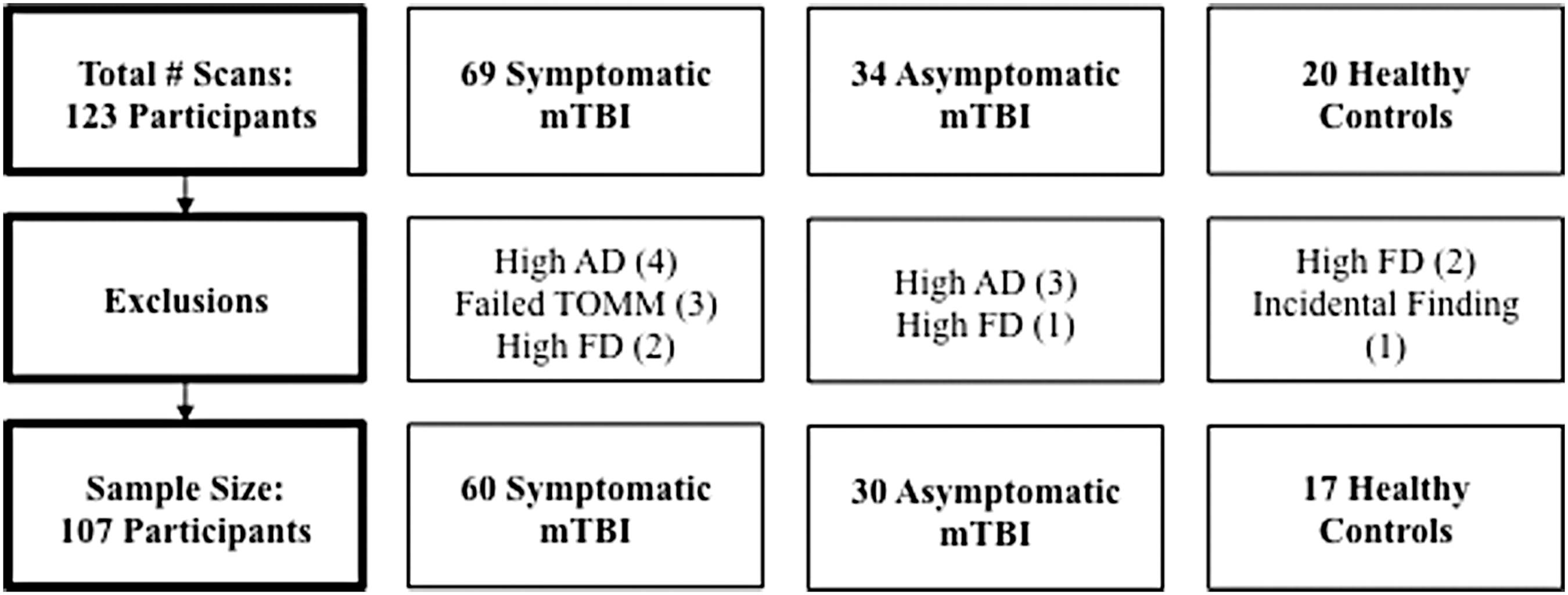
Study consort diagram. There were 123 participants who met study inclusion and exclusion criteria. After excluding for excessive FD (framewise displacement), excessive AD (absolute displacement), failing the TOMM (test of memory malingering), and incidental findings, 107 participants comprised the sample. Group sizes are shown. TBI, traumatic brain injury.
The number of previous concussions (U = 751.5, p = 0.131) were similar between groups. Reported pre-injury PCSI symptoms differed, however, and were more common in the symptomatic mTBI group (median 5; IQR 7.75) than the asymptomatic mTBI group (median 2.5; IQR 7.75), (K-W χ2 (2) = 27.665, p < 0.001) (post hoc Dunn test stat = -5.235, p < 0.001).
Injury characteristics
Sport-related concussion/mTBI accounted for the largest proportion of mTBIs (75.6%) and was similar across groups (χ2 (4) = 6.070, p = 0.194) (Table 2). Of mTBI participants, 12.5% reported a loss of consciousness at the time of injury; that did not differ between groups (χ2 (2) = 1.508, p = 0.470).
Table 2. Injury Characteristics of the Symptomatic and Asymptomatic Groups
Injury characteristics of these groups were similar.
MVC, motor-vehicle collision; SD, standard deviation; PCSI, Post-Concussion Symptom Inventory for Youth; IQR, interquartile range.
Indicates p < 0.05.
Post-concussive symptoms
The PCS symptoms in mTBI groups were assessed at similar times post-injury (t(88) = -1.051, p = 0.939). Symptomatic children reported a median PCSI of 39.5 (IQR 37.75), and asymptomatic children reported a median PCSI of 3 (IQR 5.75).
Cognition
Subjective cognitive difficulties are shown in Table 3. There were no significant group differences in complaints of feeling slowed down (χ2 (2) = 2.842, p = 0.241) or feeling mentally foggy (χ2 (2) = 1.770, p = 0.413). Groups differed, however, in pre-injury complaints for difficulty concentrating (χ2 (2) = 13.229, p = 0.001) and difficulty remembering (χ2 (2) = 19.262, p < 0.001). Post-injury, a significantly higher proportion of symptomatic children complained of feeling slowed down (χ2 (1) = 43.107, p < 0.001), mentally foggy (χ2 (1) = 32.105, p < 0.001), difficulty concentrating (χ2 (1) = 33.192, p < 0.001), and difficulty remembering (χ2 (1) = 42.108, p < 0.001) compared with asymptomatic participants.
Percentage of Each Group that Reported Subjective Cognitive Complaints Pre- and Post-Injury
Neurocognitive performance scores on the CNS Vital Signs are shown in Table 4. There were significant differences between the three groups on the NCI score (F(2,103) = 3.648, p = 0.029), Visual Memory (F(2,103) = 3.429, p = 0.036), and Complex Attention (F(2,103) = 3.822, p = 0.025) subscores. None of these differences survived correction for multiple comparisons. Post hoc analyses demonstrated lower NCI and complex attention scores in the symptomatic group compared with asymptomatic (post hoc Bonferroni, p = 0.045 and p = 0.030, respectively).
Performance on Computerized Cognitive Tests
Tests, using CNS Vital Signs, were well within the normal range for all groups. Visual memory, complex attention, and the overall neurocognitive index, however, were lower in the children with persistent post-concussive symptoms (symptomatic) compared with children without post-concussive syndrome symptoms (asymptomatic) and healthy controls.
*p < 0.05. Post hoc corrected for multiple comparisons.
Working memory task performance during the fMRI was similar between groups at all levels of difficulty. In addition, reaction times for true positives or false positives during these tasks were similar. Median (IQR) A' scores on the 1-back for the groups were: symptomatic mTBI 0.98 (0.05); asymptomatic mTBI 0.98 (0.04); controls 0.97 (0.08); χ2 (2) = 3.897, p = 0.143, η2 = 0.018, d = 0.273. The A' scores on the 2-back for the groups were as follows: symptomatic mTBI 0.88 (0.12); asymptomatic mTBI 0.89 (0.09); controls 0.91 (0.08); χ2 (2) = 3.453, p = 0.178, η2 = 0.04, d = 0.408.
Working memory task BOLD response
All three groups demonstrated extensive activation of the working memory network that included regions in the prefrontal cortex, inferior frontal gyrus, parietal cortex, anterior cingulated, and occipital cortex (Fig. 2, warm), and deactivation in regions of the default mode network including the precuneus and medial prefrontal cortex (Fig. 2, cool).
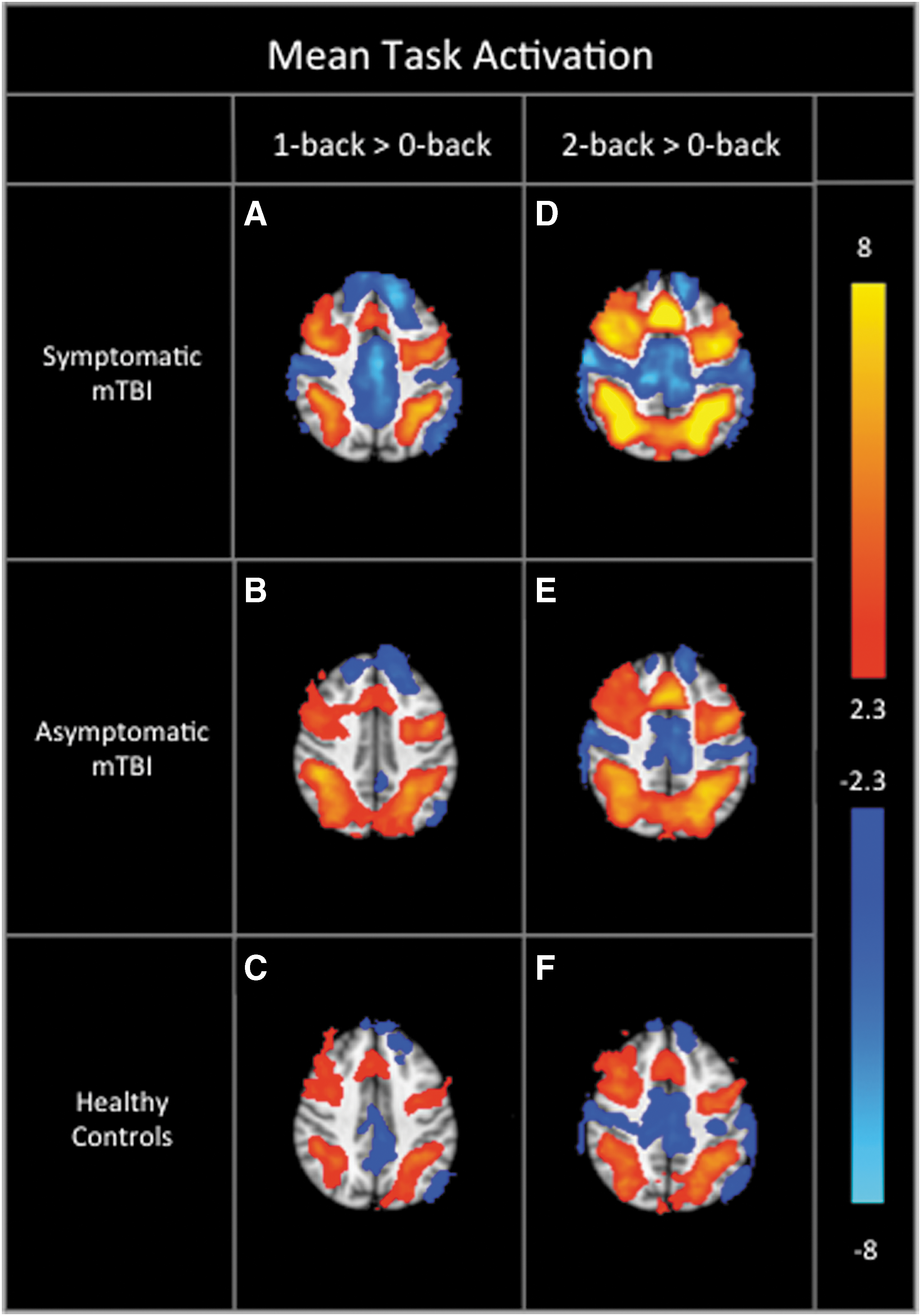
Mean task related working memory network activation for each group. Included were regions in the prefrontal cortex, inferior frontal gyrus, parietal cortex, anterior cingulate, and occipital cortex. Working memory network activation (warm) is observed for each group. The red-yellow indicates positive activation and the (cool) blue-yellow indicates negative activation. The 1-back >0-back contrast is displayed for each group in
No significant differences were found between the mTBI groups and healthy controls. We found, however, decreased activation in the symptomatic group compared with the asymptomatic group on the 1-back >0-back contrast (Fig. 3A)—specifically, in the precuneus cortex, posterior cingulate, juxtapositional lobule, and anterior cingulate gyrus ([20 -50 46], 1294 voxels, p = 0.024, ZMax = 3.72). Inspection of Figure 2 suggests that this difference may be driven by relatively higher deactivation in the default mode network in the symptomatic mTBI group.
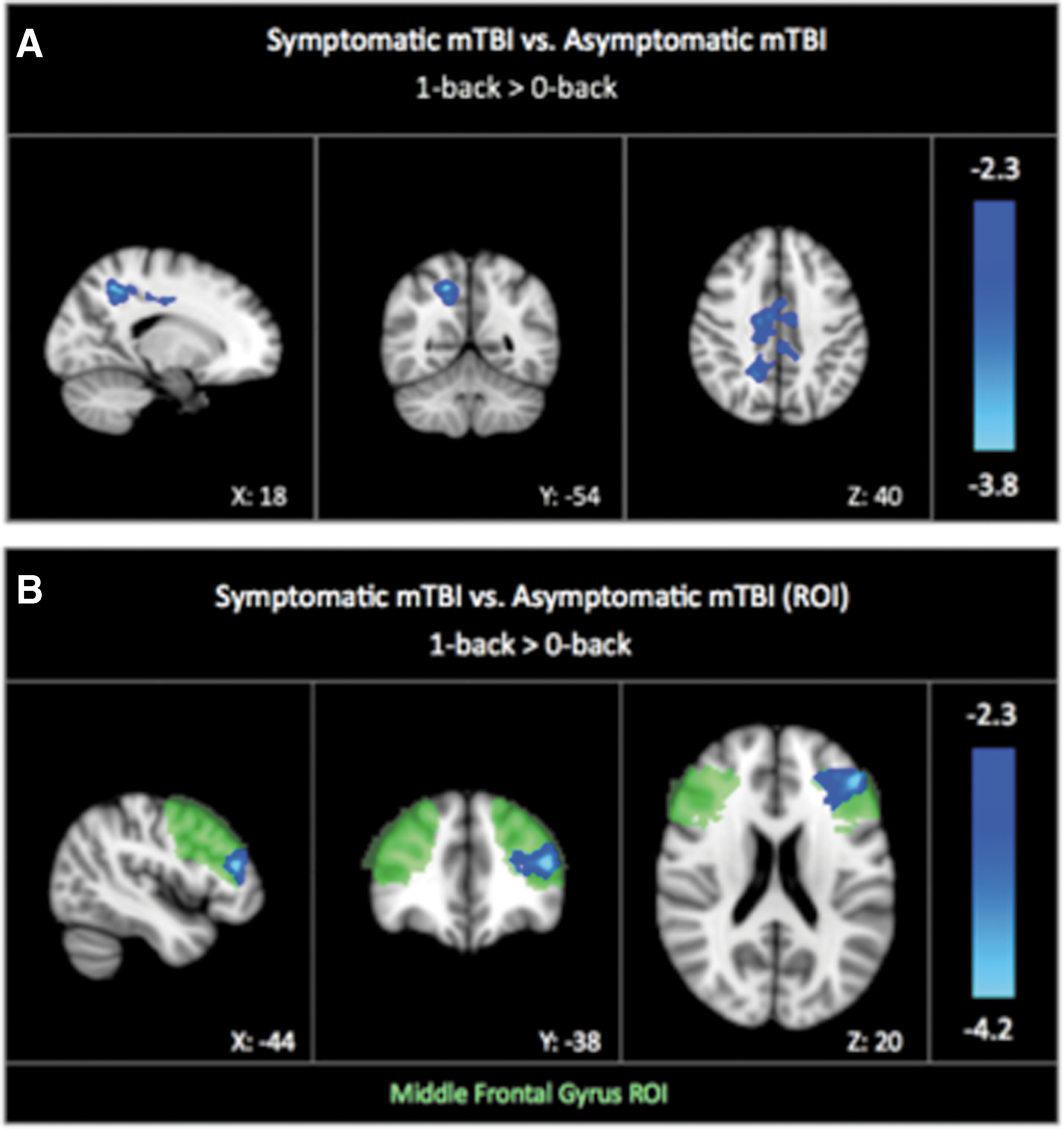
The symptomatic mild traumatic brain injury (mTBI) group had decreased activation compared with the asymptomatic mTBI group. Decreased activation was noted in the precuneus cortex, posterior cingulate, juxtapositional lobule, and anterior cingulate gyrus on the whole brain analysis (
Within the DLPFC ROI, we also found that a region of the left Broca area BA 44/45 ([-44 38 18], 608 voxels, p = 0.0283, ZMax = 4.13, Fig. 3 B) showed decreased activation in the symptomatic group compared with the asymptomatic group for the 1-back >0-back contrast. No group differences were observed for the 2-back >0-back contrast in the whole-brain or ROI analyses.
Discussion
There has been little research exploring working memory network activation in children with persistent post-concussion symptoms. 29 –35 Mixed findings may have resulted from differences in working memory task design, populations studied (e.g., sports concussions, single or repetitive, mTBI populations, adult versus children, etc.), varying age groups, an exclusive focus on sport mTBI and the time post-injury, where individuals in dissimilar stages of recovery may be grouped together. 56 Most previous works examined children at relatively disparate time points and have a small sample size. We report the largest study to date examining working memory cortical activation using fMRI in children with PPCS.
Working memory-related cortical activation was decreased in children who had not yet recovered at one month post-injury, despite performing similarly on the task as their recovered counterparts. This finding is in keeping with Keightley and colleagues 33 who reported similar regions of cortical hypoactivation in children at 41 days post-concussion. Their study employed a task similar to ours—a language-based working memory task with a visuospatial component.
A few other studies in this field present contrasting findings however, observing hyperactivation in various cortical areas either in children or young adults. 29,30, 32,34 These previous research studies, although limited, have varied considerably not only in when subjects were examined post-injury, but also in the type of task perfomed. 29,30,33,57 Most studies performed in the acute/subacute post-injury period have observed areas of hyperactivation, 29,30 except one that reported hypoactivation in posterior middle and superior temporal gyri. 31 Although these aforementioned studies used a visual n-back task, one added an inhibitory task component, and the observed region of hyperactivation differed between dorsal attention regions, other prefrontal and parietal regions, and cerebellar areas. 32
Cortical activation may also correlate with symptom severity. Lovel and associates 29 and Pardini and coworkers 30 found increased activation in prefrontal regions to correlate with a prolonged recovery period or increased symptom severity. 30 Although we did not perform this correlation, our findings contradict this. Herein, decreased cortical activation was found in children who remained symptomatic at one month, compared with those who recovered. This effect, however, was not observed in the more demanding n 2-back task, and our findings are unlikely to be explained by differences in working memory performance. Although there were slight differences in neurocognition between the groups (using computerized cognitive evaluation), scores were well within the normal range. Further, n-back task performance was similar between groups, as has been observed by others. 16,24,26 –28,58
In addition to decreased DLPFC activation in our ROI analysis, we noted decreased activation of the precuneus and posterior cingulate gyri. The latter are pivotal hubs facilitating default mode network (DMN) interactions. 59,60 The DMN is downregulated during goal-directed activities. 60 –62 Our findings demonstrate that children who remain symptomatic at one month post-injury have greater DMN inhibition and less DLPFC activation in comparison with children who recover quickly. 62,63
Although this effect has not been observed in children with PPCS previously, Van der Horn and associates 28 observed a similar yet contrasting effect in adults with PPCS. One month post-injury, they observed greater DMN deactivation in recovered adults compared with adults with PPCS, while also noting a lack of difference between their injured and control groups. Despite our findings disagreeing in the directionality of differences, together these studies implicate the DMN in cognitive issues underlying PPCS, requiring additional research.
We propose that after mTBI, coordination of task positive and task negative network processes are disrupted. Similar DMN disruptions have been observed after adult mTBI in studies using resting-state fMRI and magnetic encephalography (MEG). 18,64 –68 Another mTBI study has shown that this anticorrelated network interaction can be disrupted and be associated with memory complaints, described as the Default Mode Interference Hypothesis. 69 Alterations in DMN hub connectivity, especially the cingulate cortex, have been linked to neurocognitive outcome and symptomology. 65,67,68 Our pediatric study furthers this line of inquiry through presenting new evidence of DMN cortical activation differences in conjunction with cognitive symptomology after mTBI.
While strengths of this study included a large well-characterized cohort assessed at a similar time post-injury, this study also had several limitations—the heterogeneity in injury factors including mechanism, as well as interindividual variability including pre-injury risk factors for development of persistent symptoms that cannot be controlled for. 3,70 To mitigate this and preserve similarities in pre-injury characteristics and social environment, we recruited healthy controls from friends and family of injured children.
We excluded individuals with histories of serious illnesses or neurological conditions. Although this limits the generalizability of the study, children with pre-existing ADHD or specific learning difficulties were included to represent a better “real world” sample, given the prevalence of ADHD in the general population. Although ADHD has been associated with working memory deficits in children, the proportion of children with this diagnosis was not significantly different between our mTBI groups and unlikely to affect our results. 71
The heterogeneity of the working memory tasks used in the literature makes it difficult to compare results across studies. Discrete working memory tasks tend to hypoactivation patterns in mTBI populations, whereas hyperactivation often is seen when using continuous tasks. 57 We used a continuous n-back working memory task given its test-retest reliability. 46 Although practice effect could be a factor in our results, we tried to control for this by using task performance as a covariate in our analysis.
Despite being one of the largest studies of its kind, a smaller control group limited the power of this study. The lack of differences in comparison with our control group may be better elucidated using a orthopedic injury control group with similar pre-morbid characteristics and injury-related characteristics. 72,73
Finally, the symptom score change defined for PPCS in this study was chosen for its clinical significance and reliable change in determining symptom persistence. 6,74 Although some groups have adopted a similar definition for their PPCS studies, a consensus definition in the field will only be reached with further research. 75,76
Future research is needed to determine whether children with mTBI show changes in cortical activation over time, as they recover. Given the lack of pre-injury data, any significant changes would add validity to these deficits being associated with the mTBI and clinical symptoms. Further, examination of cerebellar activations (not possible in our study) would be useful given its significant contribution to working memory performance. 31
Conclusions
Overall, children with mTBI had similar working memory cortical activation and neurocognition to healthy controls. There were significant differences, however, between children with mTBI with different recovery patterns. Compared with children who had clinically recovered from mTBI, children with PPCS exhibited greater inhibition of DMN hubs (precuneus and posterior cingulate gyri) and hypoactivation in the task positive network hub (DLPFC) during a working memory task. These effects were observed in the absence of performance differences. Although more research is needed, these findings provisionally encourage the continuation of support at school for children with PPCS and the avoidance of repeat injury.
Footnotes
Acknowledgments
The authors would like to thank the following individuals for their contribution to the project. Brenda Turley, Tina Samuel, Zahra Ofoghi, for project management and assistance with data collection; Dr. Keith Yeates, Dr. Ashley Harris, and Dr. Catherine Lebel for their input to the graduate project; Dr. Frank MacMaster, Angela Villacicencio-Requis, Natalia Jaworska, and Lisa Marie Langevin, for guiding the design and implementation of the working memory task; Sophie Hu for assisting with the pre-processing of the MRI data.
This study was funded by the Canadian Institutes of Health Research (grant number: 293375) and the Faculty of Medicine, University of Calgary Project number 10005062. AK: Canadian Institute of Health Research, the International and Industrial Imaging Training (I3T) Program at the University of Calgary, and the Natural Sciences and Engineering Research Council (NSERC) for graduate studentship support. CR: Postdoctoral fellowships awarded by Alberta Innovates, NSERC I3T, and University of Calgary Eyes High.
Author Disclosure Statement
No competing financial interests exist.