
Abstract
Acute subdural hematoma (ASDH) caused by bridging vein (BV) rupture is a frequent and lethal brain injury, especially in the elderly. Brain atrophy has been hypothesized to be a primary pathogenesis associated with the increased risk of ASDH in the elderly. Although decades of biomechanical endeavors have been made to elucidate the potential mechanisms, a thorough explanation for this hypothesis appears lacking. Therefore, a recently improved finite element head model, in which the brain–skull interface was modeled using a fluid-structure interaction (FSI) approach with special treatment of the cerebrospinal fluid as arbitrary Lagrangian–Eulerian fluid formulation, is used to partially address this understanding gap. Models with various degrees of atrophied brains and thereby different subarachnoid thicknesses are generated and subsequently exposed to experimentally determined loadings known to cause ASDH or not. The results show significant increases in the cortical relative motion and BV strain in the atrophied brain, which consequently exacerbates the ASDH risk in the elderly. Results of this study are suggested to be considered when developing age-adapted protecting strategies for the elderly in the future.
Introduction
Acute subdural hematoma (ASDH) induced by bridging vein (BV) rupture has been considered to be a catastrophic brain injury, 1,2 especially in the elderly. Epidemiological studies have shown a much higher incidence rate of BV-sourced ASDH in the elderly than in younger adults, along with elevated morbidity and mortality, and poorer treatment outcomes. 3 –9 Clinical studies suggest brain atrophy as a primary etiology contributing to the increased ASDH risk in elderly trauma patients. 9,10 However, this hypothesis remains to be verified and associated mechanisms are yet to be better uncovered.
As numerical surrogates, finite element (FE) head models have been used to quantify the biomechanical influence of brain atrophy on ASDH. However, consistent findings have not been reached to date. In a study by Zou and colleagues, 11 FE simulations were performed to investigate the effect of brain size on brain-skull relative motion, showing that, when decreasing the brain volume and thereby increasing the thickness of the cerebrospinal fluid (CSF) in the subdural space, the maximum brain-skull relative motion was reduced. Two subsequent studies by Yanaoka and Dokko 12,13 shrank the geometric features of the Global Human Body Models Consortium (GHBMC) brain model developed by Mao and coworkers 14 to represent those of the elderly. Elongation of BVs was chosen as the predictor for ASDH in both studies, showing that decreased brain volume resulted in larger maximum elongation of BVs in occipital and temporal impacts. Later, Antona-Makoshi and associates 15 developed two FE rat models, representing the young adult rat and its older counterpart. Both models were subjected to injurious levels of rotational accelerations. The results suggested that reduced brain volume produced higher relative motion damage measurement (RMDM), an ASDH risk indicator proposed by Takhounts and colleagues. 16
Previous numerical studies suggest that a precise brain–skull interface modelling approach in the FE head model is essential for accurate ASDH prediction. 17 –19 Among the aforementioned FE models, the brain–skull interaction modeling approaches vary from representing the CSF as an incompressible material with low shear modulus 15 to more complex contact algorithms including sliding-only contact 11 and tied contact. 12,13 Of all these approaches, the fluid properties of the CSF and the potential of impacted-induced CSF flow within the subarachnoid space are ignored, because CSF is consistently modeled as Lagrangian solid elements in which the mesh exactly follows the material deformation. Moreover, given that the fluid material may endure considerable deformation, it is more appropriate to model the CSF as fluid elements, in which the mesh either is fixed in the space or moves according to a pre-defined directive, to better represent its fluid behavior without causing severe element distortion and resultant numerical instability. 11,18,20 –24 To date, there are a few two dimensional (2D) FE models 25 –28 and simplified spherical three dimensional (3D) models 29 that implement fluid elements for the CSF. Recently, Zhou and colleagues 30 improved the brain–skull interface in a 3D head model using a fluid-structure interaction (FSI) approach with special treatment of the CSF as arbitrary Lagrangian–Eulerian (ALE) multi-material fluid elements. This FSI approach contributed to an improved validation performance with respect to brain-skull relative motion and an enhanced ASDH predictability.
The aim of the present investigation is to advance the understanding of the ASDH mechanism associated with brain atrophy in the elderly. To account for the fluid behaviour of the CSF and its mechanical interaction with the brain and skull, the model developed by Zhou and colleagues 30 is used. Models with different brain sizes and various subarachnoid thicknesses are generated and subsequently subjected to experimentally measured loadings known to cause ASDH or not. By studying the relative motion between the brain cortex and the skull, and BV strains in models with varying severities of atrophy, the biomechanical mechanisms of the predisposition of the elderly to ASDH will be better addressed.
Methods
FE head model
The FE head model employed here was originally developed by Kleiven 23 and recently improved by Zhou and colleagues. 30 The head model includes the scalp, skull, brain, CSF, superior sagittal sinus (SSS), transverse sinus, ventricles, and meninges; a simplified neck with extension of the spinal cord; and 11 pairs of parasagittal BVs (Fig. 1). Details regarding the geometry discretization and mechanical properties of each anatomical structure have been reported earlier. 23,30 In particular, the 11 pairs of parasagittal BVs are constructed by connecting one node on the cerebral surface in the vertical region to a node on the SSS (Fig. 1b). The length of each BV and the resultant angles between the SSS and the BV elements are: frontopolar, 16.5 mm and 87 degrees; anterior frontal, 15.8 mm and 103 degrees; middle frontal, 9.7 mm and 69 degrees; posterior frontal, 13.7 mm and 64 degrees; pre-central, 18.2 mm and 46 degrees; vein of Trolard, 18.4 mm and 47 degrees; central, 14.9 mm and 61 degrees; post-central, 15.0 mm and 59 degrees; anterior parietal, 8.8 mm and 44 degrees; posterior parietal, 19.9 mm and 66 degrees; and occipital, 17.8 mm and 74 degrees. It is important to note that the angles are measured from the SSS to the BV elements for BVs on the left hemisphere and vice versa for BVs on the right hemisphere, although consistently along a counterclockwise direction. Based on the experiments by Lee and Haut, 31 a uniform tensile stiffness of 1.9 N per unit strain is adopted to model BVs' resistance.
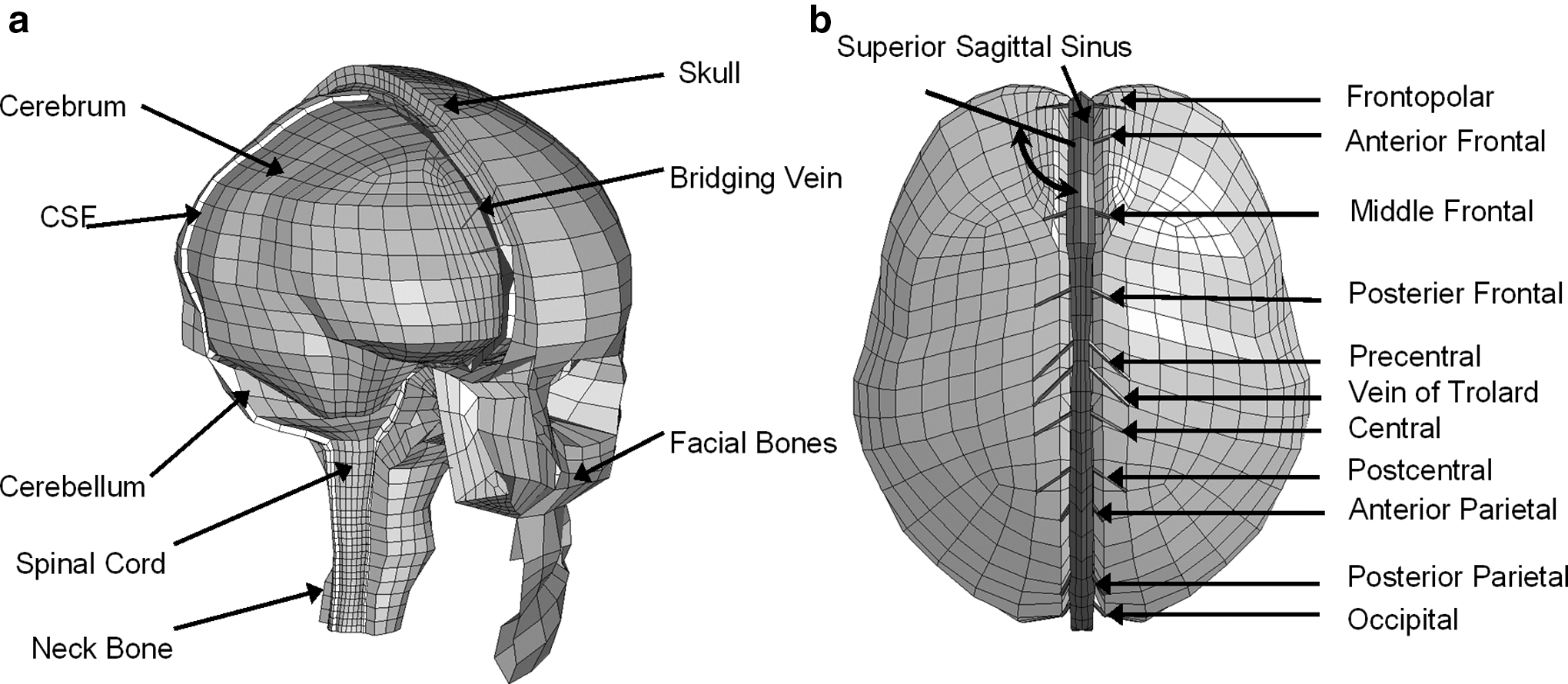
Finite element (FE) model of the human head.
Brain–skull interface modeling
A FSI approach is used to simulate the brain–skull interface. Based on the anatomical findings that the subdural space may not exist in physiological conditions, 32 it is assumed that no relative motion occurs between the dura mater and arachnoid mater. Therefore, as detailed by Zhou and colleagues, 30 the CSF elements in the subarachnoid space are updated as ALE multi-material fluid formulation. It is expected, except for flowing within the subarachnoid space, that the CSF may also flow to the region that is initially occupied by the brain cortex because of brain deformation and the brain-skull relative motion secondary to exterior loading. To account for that, void meshes are generated at the peripheral region (Fig. 2). The void meshes overlap with the brain cortex meshes and are not filled by the fluid material at the initial configuration.
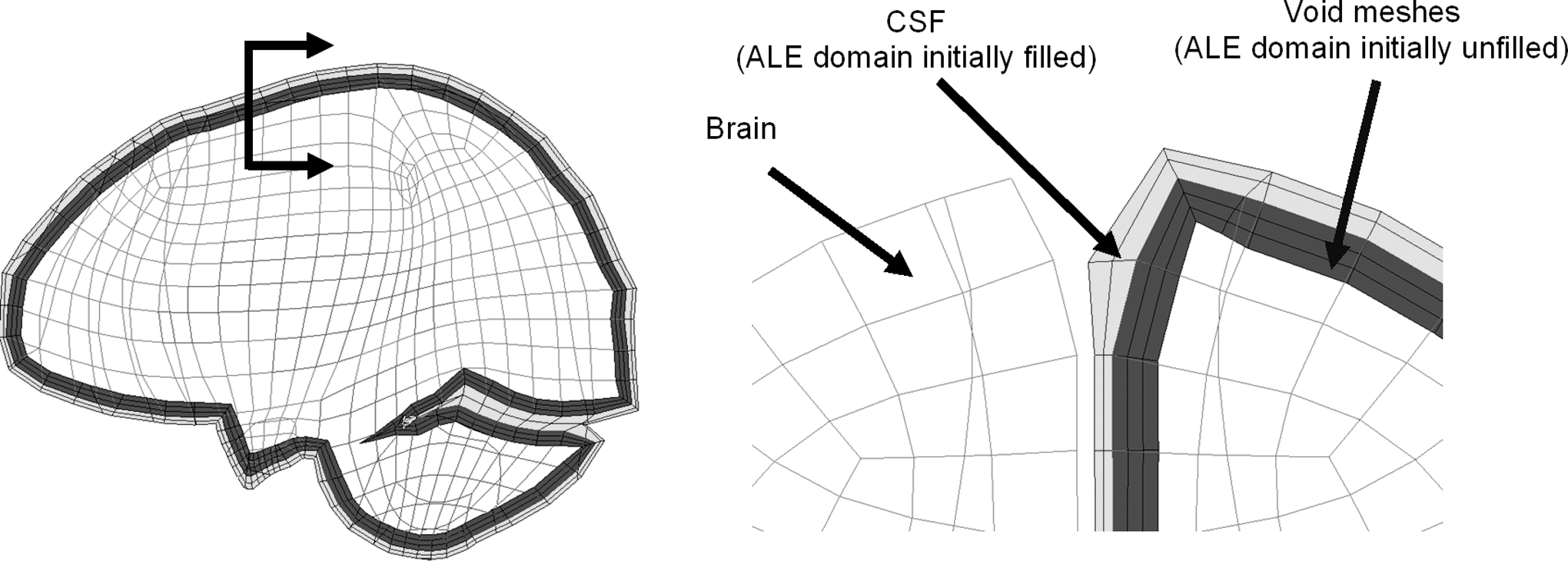
Sagittal section of the head model (left) together with a magnified coronal section (right) showing the initial cerebrospinal fluid (CSF)-filled volume (arbitrary Lagrangian–Eulerian [ALE] elements), initially unfilled volume (ALE elements), and brain (Lagrangian elements). The ALE elements surrounding the brain on the left side are masked for a better illustration in the right of the figure.
The ALE multi-material formulation advances the solution in time by dividing the operation into two steps, wherein the material is initially deformed in a Lagrangian step, followed by an advection step with a remapping of the element variables. In the Lagrangian step, the CSF deformation is determined by the equation of state (EOS) for the dilational responses and the constitutive equations for the deviatoric responses with associated formulations and material constants listed in Table 1. In the advection step, the element state variables are remapped back to the reference domain with potential mass flux flowing within the mesh. Here, a second-order van Leer scheme is selected, given its superiority in terms of numerical stability and advection accuracy.
Material Constants for the CSF
P is the pressure, C is the intercept of vs-vp
curves with vs
being the velocity of a shockwave travelling through the intermediary material and vp
being the velocity of the shocked material; S
1
, S
2, and
Because the dura mater tightly adheres to the skull inner surface, a tied contact is imposed between the dura mater and the skull. For the interface between the CSF and pia mater, a penalty-based contact is defined, which permits sliding motion in the tangential direction as well as transfering tension and compression loads in the radial direction. Because skull fracture is outside of the scope of the current study, the CSF can only flow within the compartment enveloped by the dura mater. Thus, a no-slip condition is defined between the CSF outer surface and the dura mater, the same as the approach adopted by Batterbee and colleagues. 28
Brain atrophy modeling
In order to model brain atrophy during aging, three models with different brain sizes and CSF thicknesses in the subarachnoid spaces were created by scaling the brain independently while keeping the skull size constant (Fig. 3), the same as the approach used by Yanaoka and Dokko. 12 Based on the relationship between CSF thickness and atrophy severity, 33 the model with a 1.6 mm CSF layer approximately represents a young adult, whereas the ones with 2.6 mm and 3.6 mm CSF layers represent a mildly atrophied brain, and a severely atrophied brain, respectively. Of the three models, the brain masses are 1.457, 1.402, and 1.358 kg for the young adult, mild atrophy, and severe atrophy, respectively, which approximate the average brain weights from the autopsy report 34 of the cohort 20 years old (YO), 60 YO, and 75 YO, respectively.
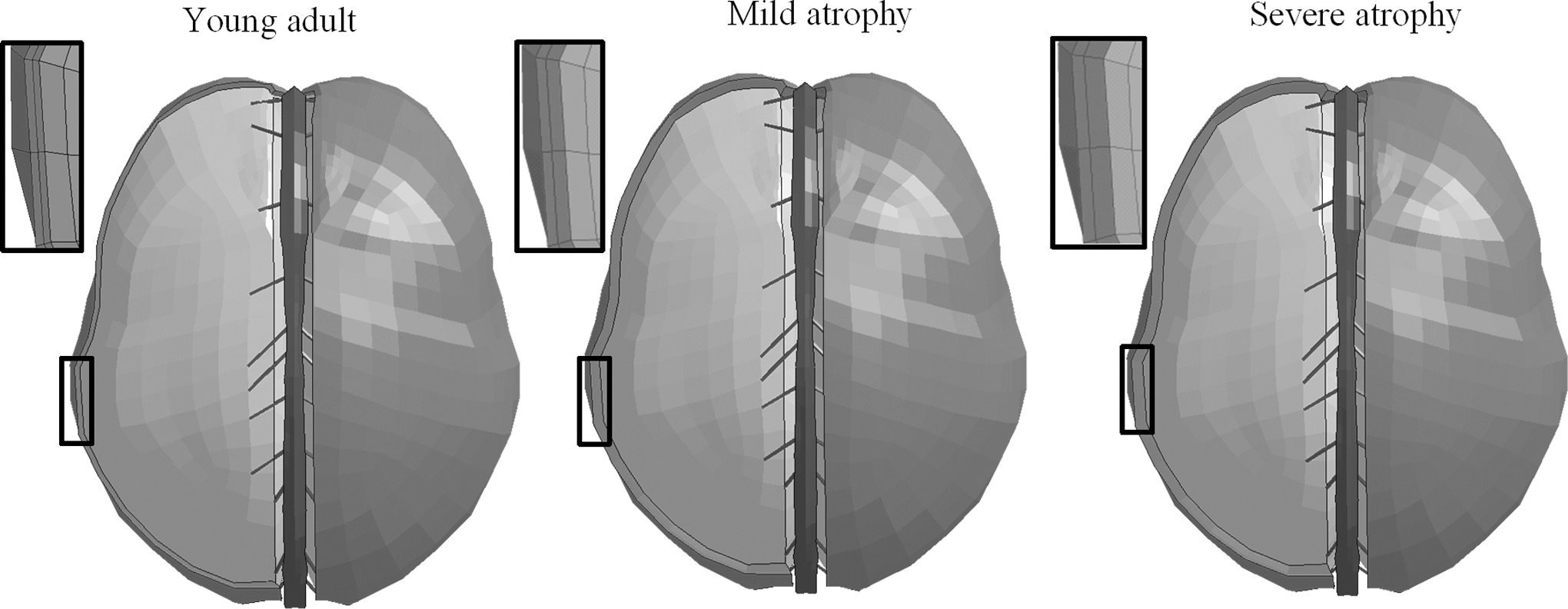
Models with different cerebrospinal fluid (CSF) thicknesses to represent young adult (left), head with mild brain atrophy (middle), and head with severe brain atrophy (right). To better illustrate the increased CSF thickness during aging, part of the CSF is masked, and a magnification of the region is indicated by the black rectangle provided for each model.
Loading conditions
Because the age-related increase in BV-sourced ASDH occurrence in motor vehicle crashes is most prominent in the frontal crashes with anterior-posterior head motion, 35 BV responses secondary to rotational loading in the sagittal plane are of particular interest. A study by Depreitere and associates 36 experimentally determined the human tolerance level for BV-induced ASDH in the sagittal plane by delivering occipital impacts to the cadavers. Six representative impacts are simulated by the models with kinematic peaks and injury conditions listed in Table 2. 36, 37 The experimental kinematics are applied to the nodes located at the center of gravity of the head and constrained to the rigidly modelled skull. Out of the six selected experiments, the only one resulting in BV rupture, secondary to a loading with peaks of 450 g for the translational acceleration and 26.2 krad/sec 2 for the rotational acceleration, is exemplified in Figure 4.
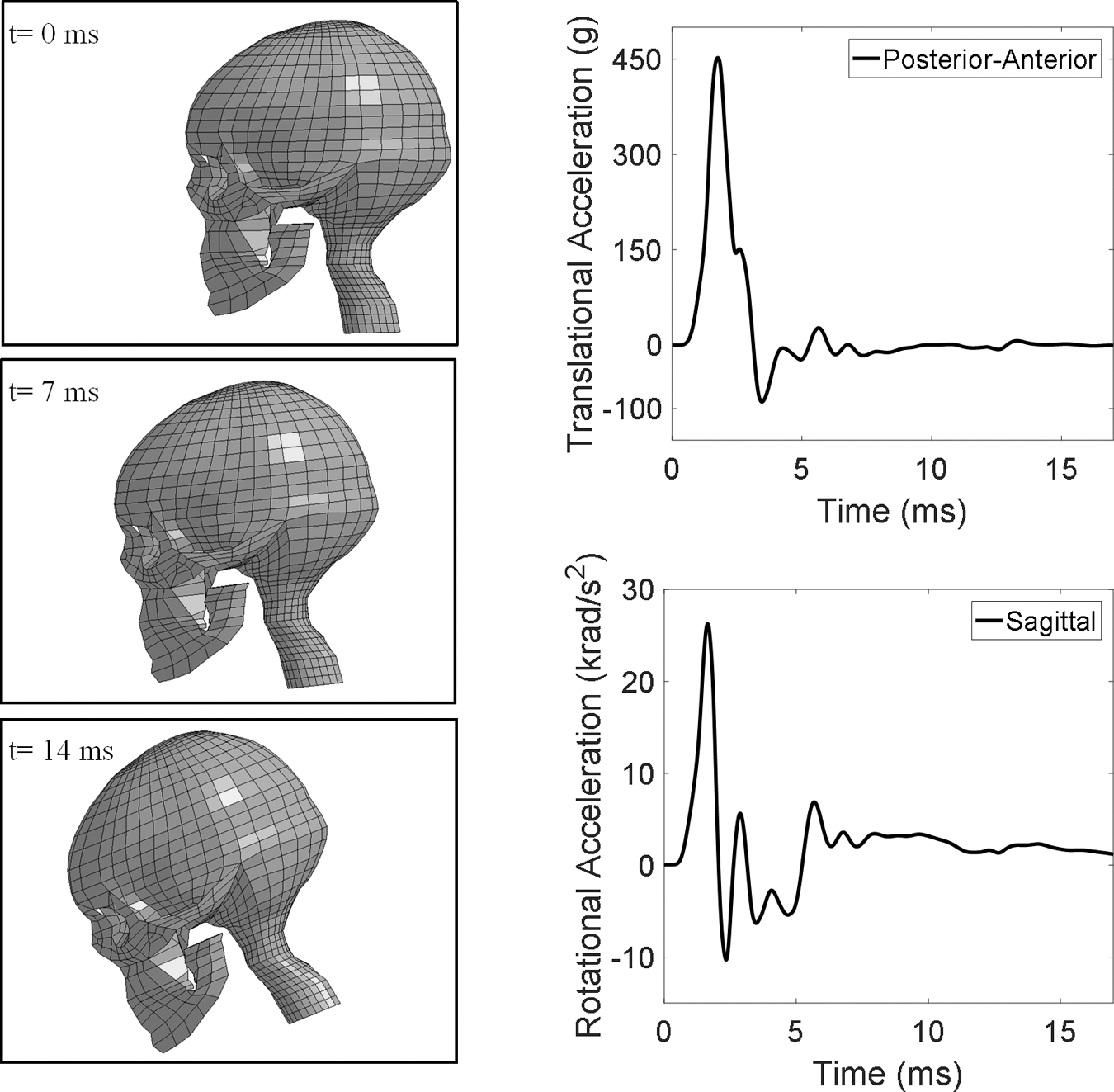
Head model loading condition for case 21-2_2 with detected BV rupture.
Experimental Kinematics and Bridging Vein Rupture Conditions of Six Representative Cases
A selectively reduced integration and hourglass control are used for the brain in all simulations. The hourglass energies are consistently controlled to be <10% of the peak internal energy for each part in the model.
Results
Cortical relative motion (i.e., relative motion between the cerebral surface and the skull) and maximum BV strain are used to evaluate ASDH risk. Such a strategy is previously used by Kleiven 18 and Zhou and colleagues. 30
For case 21-2_2 with detected BV rupture, the maximum cortical relative motions over the entire cortical surface are noted at the posterior frontal and precentral regions for all the three models (Fig. 5a). The maximum cortical relative motion shows an increase with atrophy severity (Fig. 5b). The maximum values are 7.6, 8.4, and 9.2 mm for the young adult, mild atrophy, and severe atrophy, respectively. The maximum BV strains are collected from the BV at anterior parietal regions for all the simulations. As shown in Figure 5c, the maximum BV strain is 0.31 for the young adult, whereas for its mild and severe atrophied counterparts, the maximum BV strains are 0.41, and 0.46, respectively. Of the two models representing mild and severe atrophy, the maximum BV strains fall within the ultimate BV strain range (0.5 ± 0.16) reported by Lee and Haut. 31 The relatively larger BV strain peaks in the older models indicates the ASDH risk increases with atrophy severity.
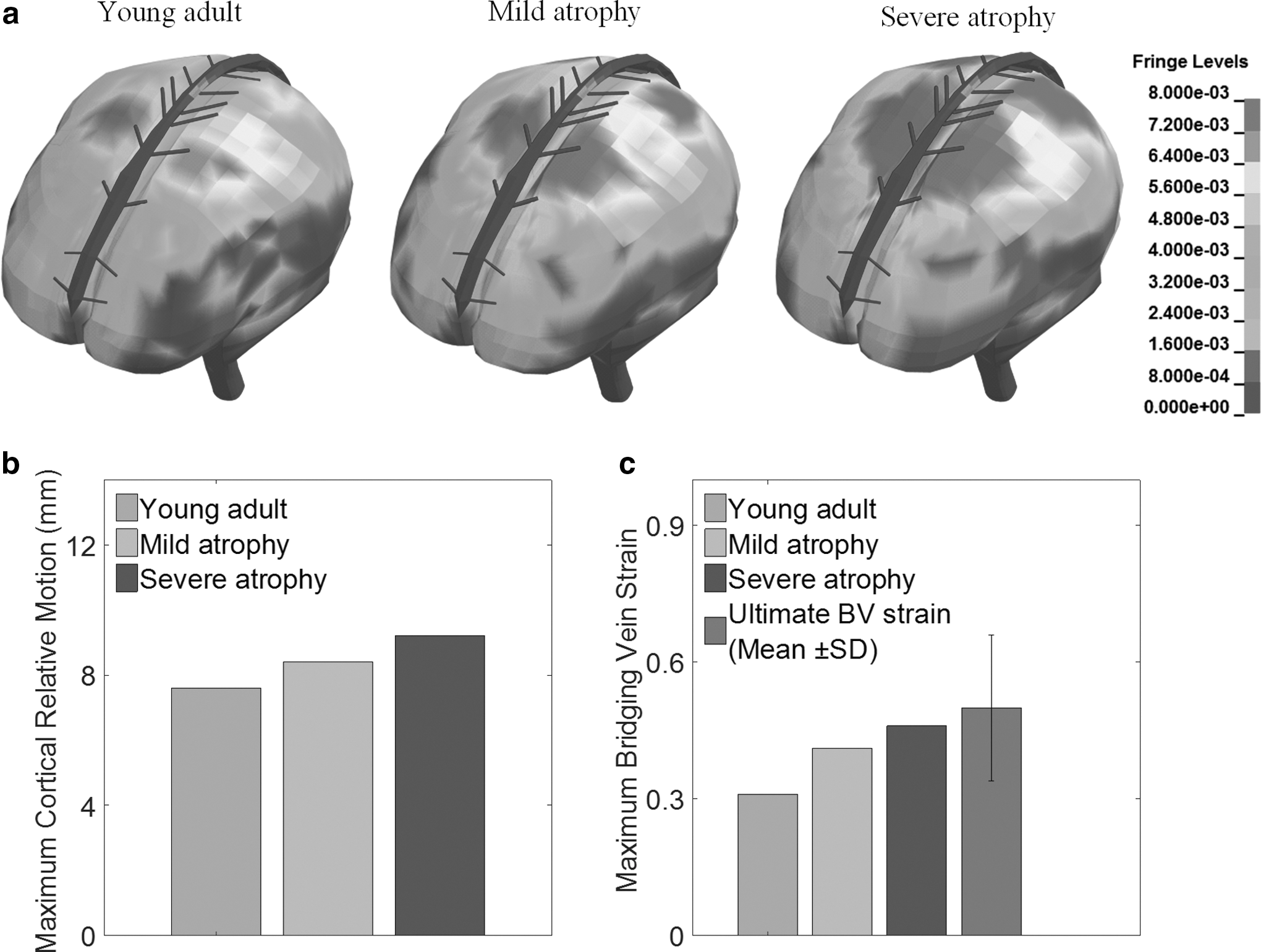
Result of cortical relative motions and BV strains for the young adult, mild atrophy, and severe atrophy for case 21-2_2 with detected bridging vein (BV) rupture.
To further check the influence of brain atrophy on the motion pattern of the superior brain surface, cortical relative motion peaks of four specific sites (Fig. 6a) for case 21-2_2 are plotted in Figure 6b. It can be noted that, for all the four sites, the cortical relative motion peaks increase with atrophy severity.
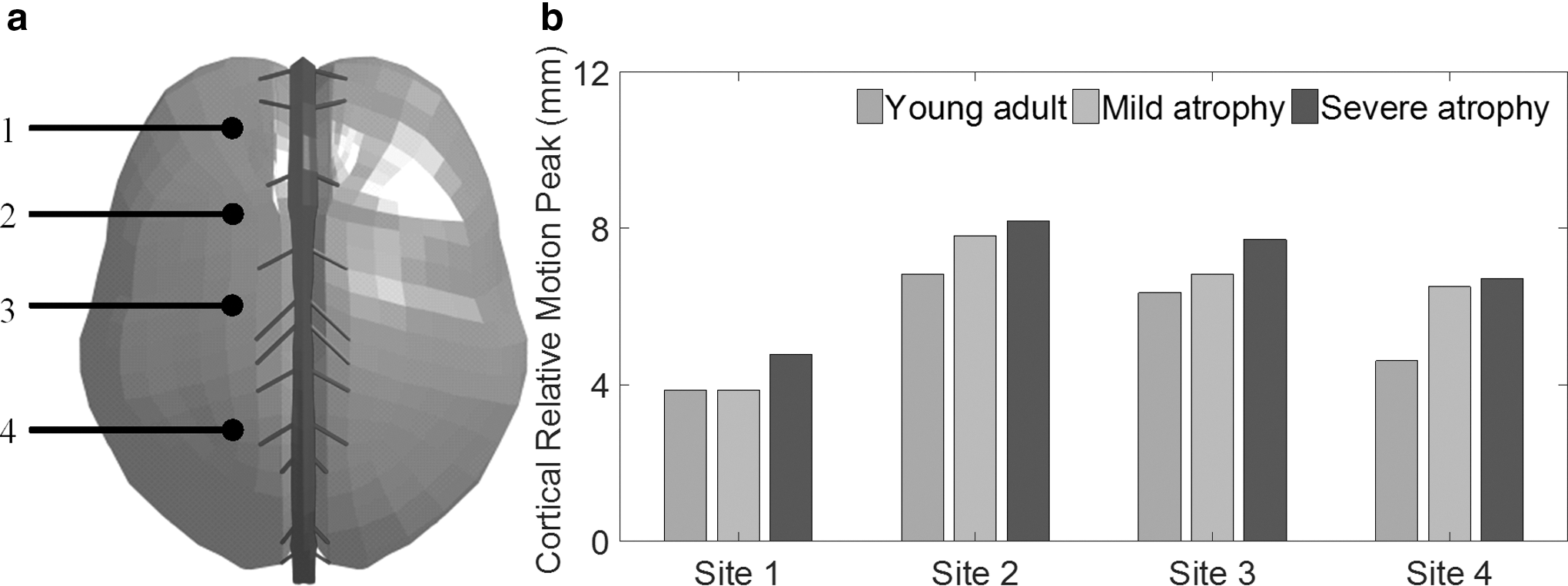
Cortical relative motion peaks of four cortical sites for young adult, mild atrophy, and severe atrophy for case 21-2_2 with detected bridging vein (BV) rupture.
For the five cases without detected BV rupture, maximum cortical relative motion and maximum BV strain over the whole cortical surface are plotted in Figure 7. Consistently, the peak values increase with the atrophy severity. It can also be noted that the predicted BV strain peaks for all the five cases fall below the ultimate BV strain range (0.5 ± 0.16), 31 agreeing with the experimental observation.
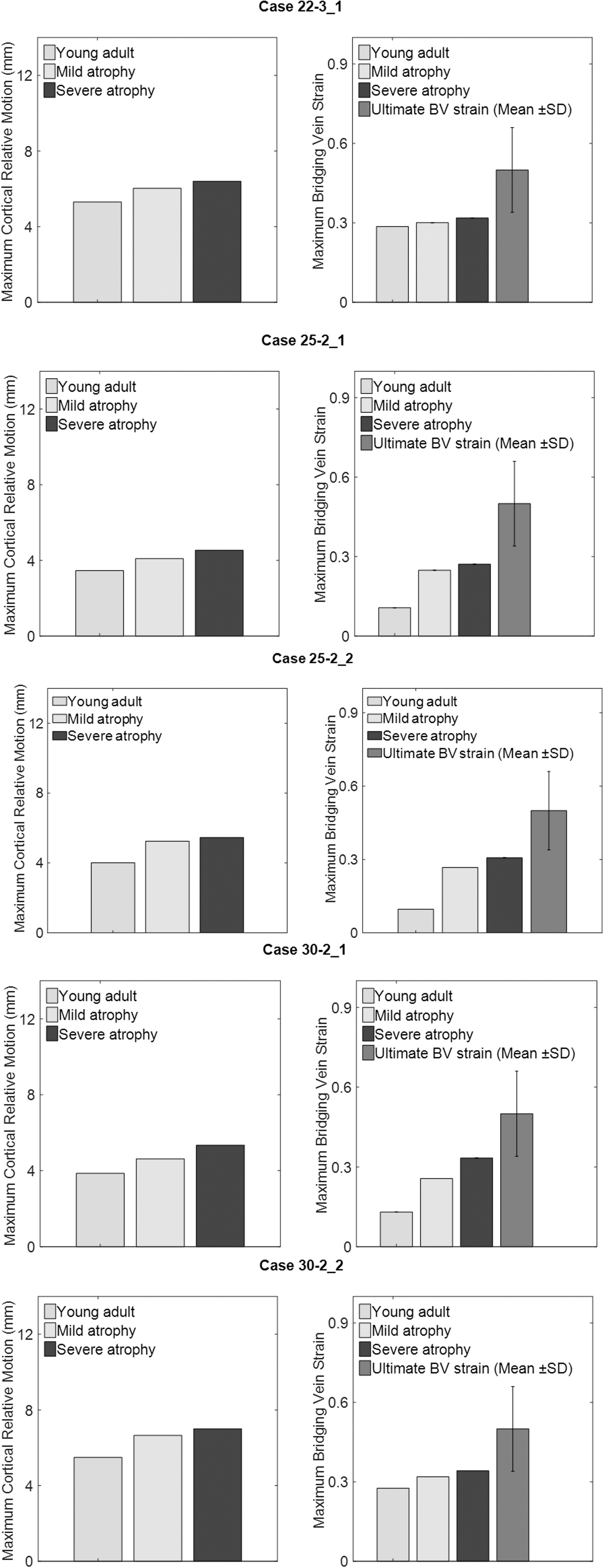
Results of maximum cortical relative motions and maximum bridging vein (BV) strains for the young adult, mild atrophy, and severe atrophy, secondary to five experimental loadings known not to cause BV rupture. Maximum BV strains are plotted together with the BV ultimate strain from Lee and Haut. 31 SD, standard deviation.
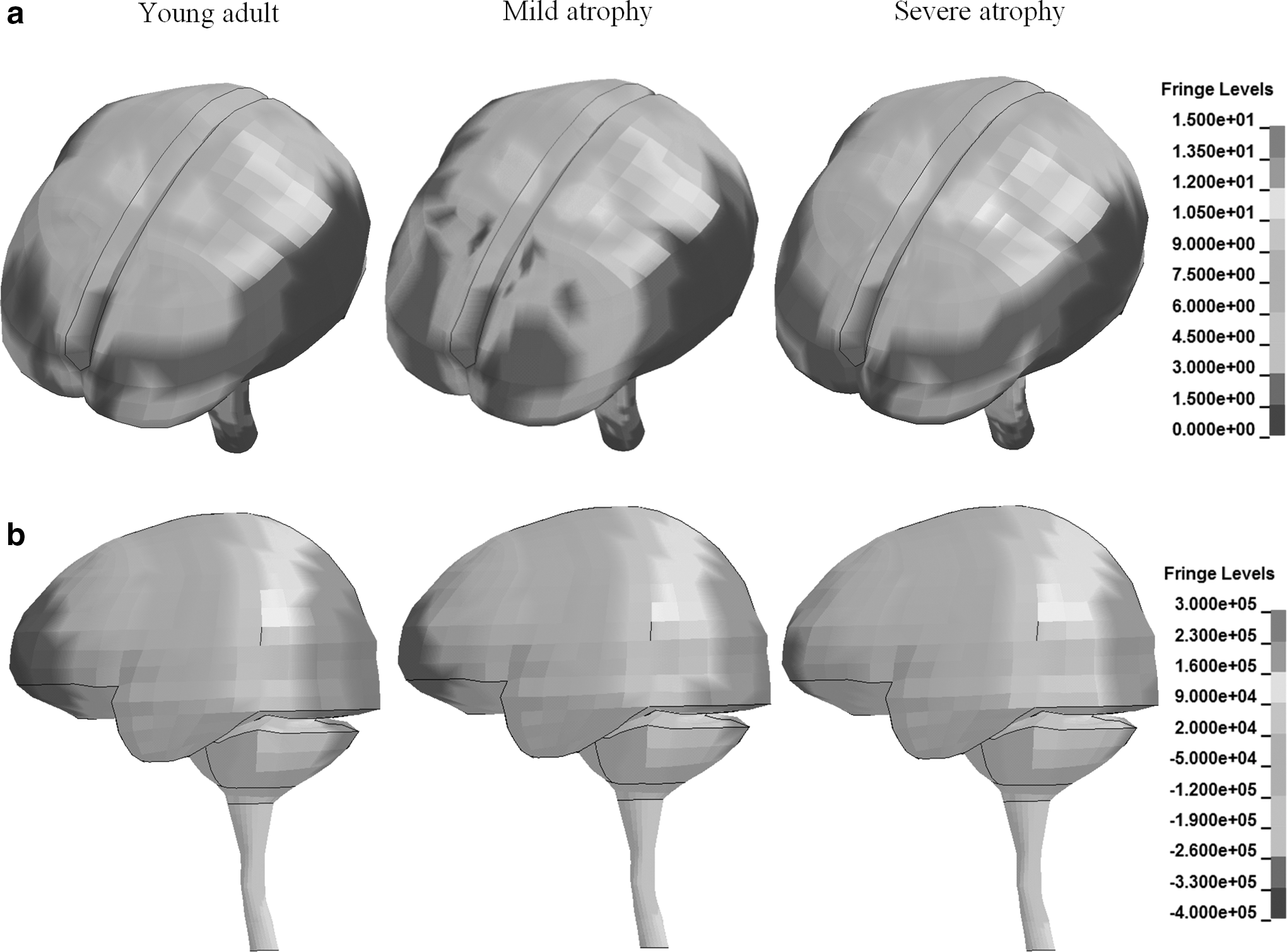
For case 21-2_2 with detected BV rupture, the first principal Green–Lagrangian strain contour in the brain for both transverse and sagittal cross-sections at 17 ms shows similar distribution among the three models (Fig. 8a). No considerable discrepancy is found in peaking values within different subregions of the brain (Fig. 8b). A similar finding that brain atrophy introduces inconsiderable variations to the strain peaks is also noted for the remaining five cases without detected BV rupture (Fig. 9).
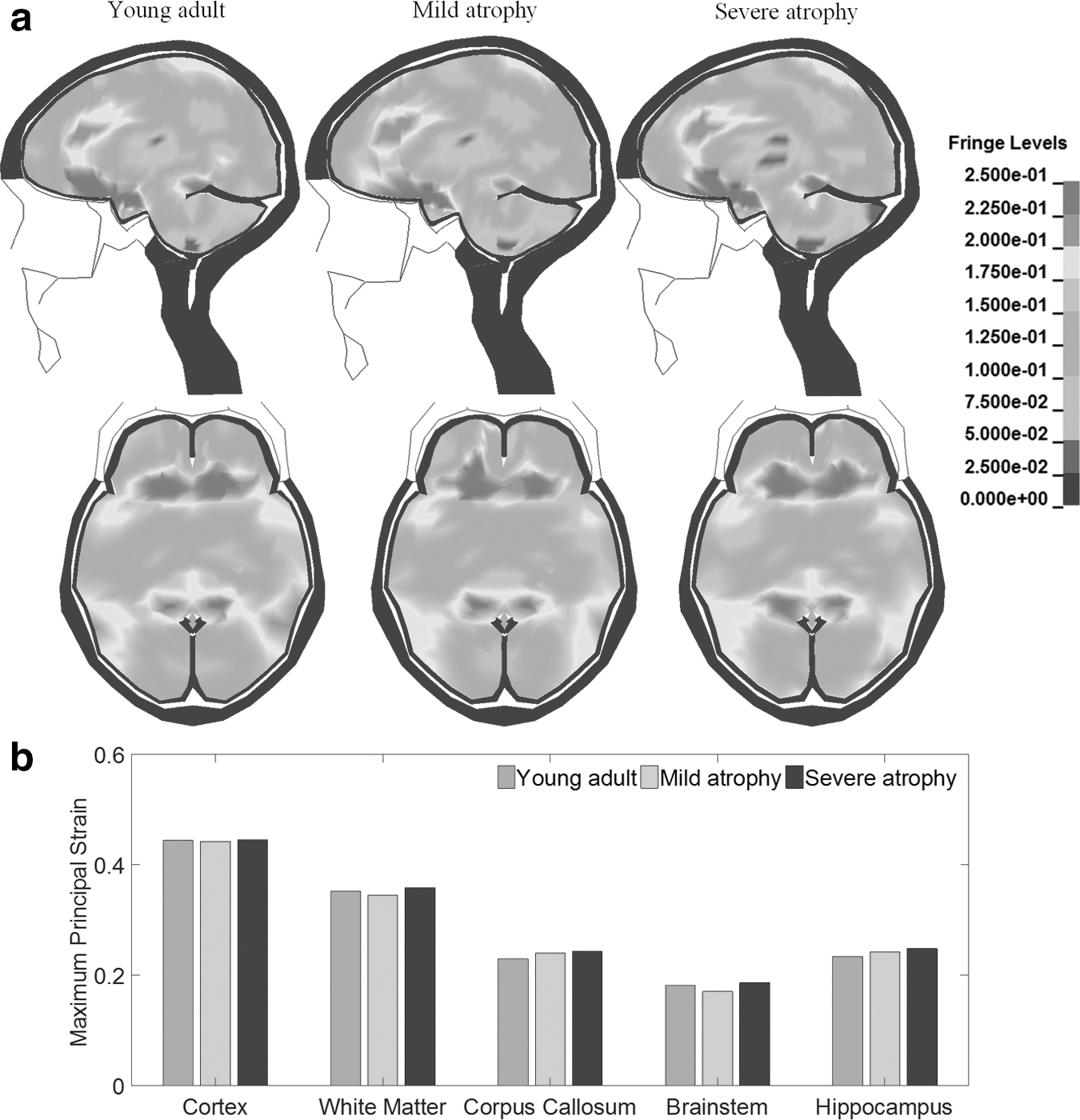
Result of first principal Green–Lagrangian strain in the brain for the young adult, mild atrophy, and severe atrophy cases for case 21-2_2 with detected bridging vein (BV) rupture.
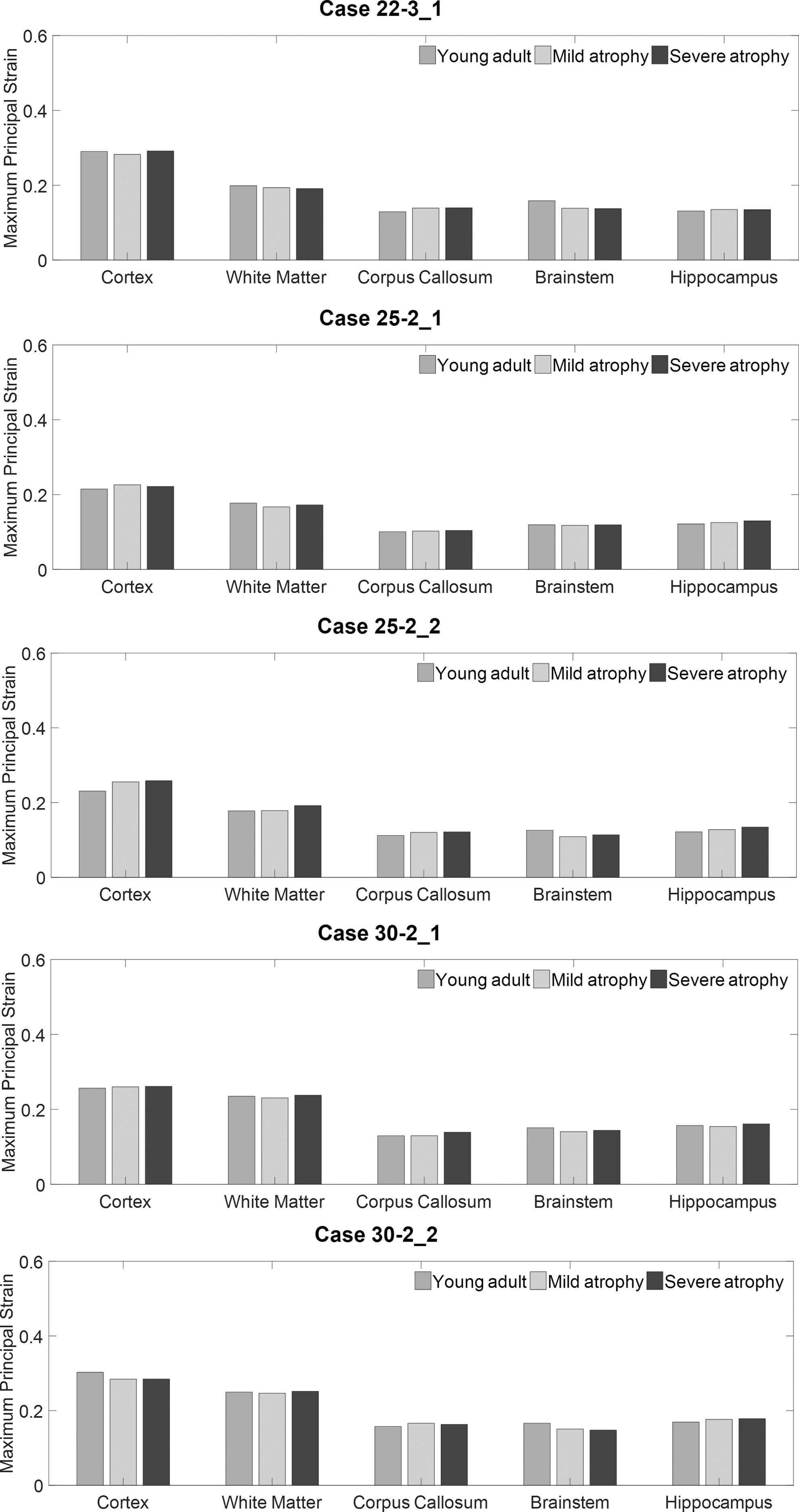
Maximum first principal Green–Lagrangian strain of gray matter, white matter, corpus callosum, brainstem, and hippocampus for the young adult, mild atrophy, and severe atrophy secondary to five experimental loadings known not to cause bridging vein (BV) rupture.
Discussion
The present study verifies the clinical hypothesis that brain atrophy aggravates ASDH risk in the elderly. Based on the results of the numerical simulations, it is revealed that brain atrophy in the elderly leads to increased cortical relative motion and more severe BV stretching, consequently contributing to relatively higher ASDH risk in the elderly.
Given its superiority in terms of ASDH prediction, 30 the FSI approach is adopted to simulate the brain–skull interface with special treatment of the CSF as ALE fluid elements. Thus, the dilatational behavior of the CSF is exclusively determined by the EOS, whereas the deviatoric response is solely governed by the constitutive modelling. As a result, the resistance in the tangential direction at the brain–skull interface, arresting the brain-skull relative motion, consists of two parts; that is, the shear stress in the CSF and the frictional force in proportion to the pressure at the brain cortex. As exemplified by the results of case 21-2_2, the shear stresses endured by the CSF are consistently minute (< 15 Pa) (Fig. 10a). In contrast, the pressure magnitude at the brain surface exhibits notable decreases in the atrophied brain, which is identified by smaller regions enduring large pressure in the atrophied cases (Fig. 10b). Thus, it indicates that the dose of the frictional force associated with the pressure at the brain cortex would be proportionally reduced as the brain atrophies. This finding provides a possible explanation for the elevated cortical relative motion and more severe BV strain observed in the atrophied brain.
The current prediction of increased cortical relative motion secondary to brain atrophy agrees with previous analytical and cadaveric experimental studies. Both Papasian and Frim 38 and Morison 39 represented the brain/skull system as analytical models with two spheres representing the brain and skull. The distance between spheres reflects the width of the subarachnoid space. The analytical models estimated increased relative motions between the spheres as the interspheric distance widened. Krauland and associates 40 reported that the brain-skull relative motion increased with brain atrophy severity by imposing the superior halves of cadaveric heads to rotational loading in the horizontal plane. General consistencies with abovedescribed studies further increase the credence of the current computational results.
Past FE studies attempted to elucidate ASDH mechanisms using other brain-skull interaction modeling approaches that did not representing fluid behavior for the CSF, and were limited to either the general cohort or a specific-aged cohort. When approximating the brain–skull interface as a layer of linear elastic solid elements with low shear modulus or tied contact, cortical relative motions usually <1 mm were predicted, engendering negligible strain values in the BVs. 18,19,22 The minute BV strains seem to disapprove of their applicabilities to investigate cortical relative motion-induced injuries, such as ASDH. Sliding-only contact permits sliding motion along the tangential direction and is capable of predicting larger peripheral relative motion. However, as reported by Zou and colleagues, 11 the sliding-only contact estimated a significant decrease in cortical relative motion correlated with the brain shrinkage, which went against the clinical observations. Such a decrease indicates a potential fallibility to use sliding-only contact as a brain–skull interface modeling approach while investigating the age-dependence of ASDH risk. As an alternative to the FSI approach used in the current study, Couper and Albermani 41 adopted Reynolds lubrication theory to represent the FSI scenario between the brain and skull in a series of 2D FE models with varying CSF thicknesses. This study reported similar results to those of the current work, in which larger skull-brain relative motion was observed as the volume of subarachnoid CSF increased. Such consistent findings between these FSI studies appear to underscore the importance of modelling the CSF as a fluid element and its mechanical interaction with the brain and skull, especially while investigating the ASDH risk in different age groups.
Because of the limited topological information, only 11 pairs of the largest parasagittal veins are incorporated into the models. However, the small BVs may be potential bleeding source responsible for the development of ASDH. In order to partially cover this deficiency, cortical relative motion is complementarily checked to assist the ASDH risk assessment, instead of exclusively checking the maximum strain in the BVs. Because the properties of the BVs are quite compliant, ignorance of the small BVs would not markedly affect brain movement relative to the skull as a whole. 18 Therefore, the current BV modeling and ASDH risk assessment strategy is thought to be sufficient for the current study. Comparatively, Yanaoka and Dokko 12,13 used BV elongation predicted by models with varying subarachnoid spaces to assess the ASDH risk. Because of the omission of the initial BV lengths before and after the brain shrinkage, solely checking the BV elongation cannot guarantee the resultant BV strain. Therefore, the reliability of the ASDH risk assessment in these two studies could be questioned.
For the case with detected BV rupture, the site with maximum BV strain is predicted at the anterior parietal regions, in agreement with the experimental observation that BV ruptures occurred in the rolandic or post-rolandic region. 36 However, the maximum cortical relative motions are estimated at posterior frontal and precentral regions, anterior to the maximum BV site. The different locations between the maximum cortical relative motion site and maximum BV strain site are noted in all the cases. This incongruity could be explained by the anatomical variations among the BVs. Compared with its counterparts at the posterior frontal and precentral regions, BV at the anterior parietal region is shorter, with its orientation more closely aligned with the loading direction. Further, clinical studies by Hirakawa and coworkers 42 and Rosenbluth and colleagues 43 commonly reported that the hematoma was susceptible to occurring at the frontal and parietal regions, approximating the computationally predicted sites with maximum cortical relative motion. Such approximations between simulated results and clinical observation further underscore the superiority of collectively checking cortical relative motion and BV strain to evaluate ASDH risk.
The first principal Green–Lagrangian strain has been used as an indicator for diffuse axonal injury (DAI). 23 The results of current work showed that the first principal Green–Lagrangian strain is relatively insensitive to brain atrophy, which is in accordance with the epidemiological findings that the incidence rates of DAI do not exhibit any age dependency. 4 However, an animal study by Antona-Makoshi and associates 15 reported that age had an effect on the amount and distribution of DAI by comparing pathological observations of two elderly rats after an injurious loading. This discrepancy might be explained by the fact that the rats involved in their animal experiments were in a narrow age range from young to adult, instead of covering the whole life span. Moreover, extrapolation of the results derived from animal experiments to human subjects needs to be further justified. 44 For the case with detected BV rupture, the maximum value of the first principal Green–Lagrangian strain was consistently observed at the inferior regions of the cerebral region, probably associated with the constrained effect by the basilar skull. 45 Similar strain pattern is noted in the study by Holbourn, 46 in which deformation of the gel-simulated brain in a physical model was measured secondary to occipital impact.
In this study, the subdural space is assumed to be non-existent, which further implies that no relative motion would occur between the dura mater and the arachnoid mater. It is worth clarifying that the potential pre-strains in the BVs secondary to brain atrophy are not considered in the current study. To the best of our knowledge, such pre-strains have neither been confirmed with certainty nor quantitatively measured. Although minimal variations in the initial lengths of the BVs indeed exist among the models as a result of enlarged subarachnoid space, the BV strains predicted by one model are calculated as the proportions of BV length variations with respect to its initial lengths measured from the same model. The mechanical role of the delicate structures in the subarachnoid space is not considered. Although the material properties of the pia-arachnoid complex of bovines have been tested in in-plane tension, 47 normal traction, and shear, 48 it remains hard to use this mechanical information in a convincing way without the details of the geometric information of the subarachnoid structure. Concerning the high occurrence of ASDH caused by occipital impact, only posterior-anterior rotation is simulated in the current study. Investigations regarding other impact directions need to be performed in the future. Moreover, the current study exclusively investigates the influence of brain atrophy on ASDH risk. Although brain atrophy is a well-observed variation occurring to the brain while aging, it is possible that there may be other potential age-related factors, such as age influence on BV material properties, which is poorly understood so far, 49 contributing to the increased ASDH risk in the elderly as well. Future studies can be performed to uncover other predisposing factors.
Conclusion
This article investigates the mechanisms of age-associated ASDH by essentially accounting for the fluid behaviour of the CSF and its mechanical interaction with the brain and skull. By comparing the cortical relative motion and maximum strain in the BVs predicted by FE models with different brain sizes and various subarachnoid spaces, it is revealed that brain atrophy leads to increased cortical relative motion and elevated BV strain. These concurrent increases better explain increased ASDH risk in the elderly.
Footnotes
Acknowledgments
This research has received funding from the European Union's Horizon 2020 research and innovation program under Marie-Curie grant agreement No. 642662. The help of Markos Kapeliotis from KU Leuven in providing the experimental data is gratefully acknowledged.
Author Disclosure Statement
No competing financial interests exist.