
Abstract
The present study examined dynamic interhemispheric structural and functional connectivity in mild traumatic brain injury (mTBI) patients with longitudinal observations from early subacute to chronic stages within 1 year of injury. Forty-two mTBI patients and 42 matched healthy controls underwent clinical and neuropsychological evaluations, diffusion tensor imaging, and resting-state functional magnetic resonance imaging. All mTBI patients were initially evaluated within 14 d post-injury (T-1) and at 3 months (T-2) and 6–12 months (T-3) follow-ups. Separate transcallosal fiber tracts in the corpus callosum (CC) with respect to their specific interhemispheric cortical projections were derived with fiber tracking and voxel-mirrored homotopic connectivity analyses. With diffusion tensor imaging-based tractography, five vertical segments of the CC (I–V) were distinguished. Correlation analyses were performed to evaluate relationships between structural and functional imaging measures as well as imaging indices and neuropsychological measures. The loss of integrity in the CC demonstrated saliently persistent and time-dependent regional specificity after mTBI. The impairment spanned multiple segments from CC II at T-1 and CC I, II, VI, and V at T-2 to all subregions at T-3. Moreover, loss of interhemispheric structural connectivity through the CC corresponded well to regions presenting altered interhemispheric functional connectivity. Decreased functional connectivity in the dorsolateral prefrontal cortex thereafter contributed to poor executive function in mTBI patients. The current study provides further evidence that the CC is a sign to interhemispheric highways underpinning the widespread cerebral pathology typifying mTBI syndrome.
Introduction
Even a mild head injury can have long-lasting progressive neurobehavioral consequences, including heightened risk of several psychiatric and neurodegenerative diseases. 1 –4 Traumatic brain injury (TBI) often leads to deterioration of white matter connections, 5 and it is widely accepted that corpus callosum (CC) is particularly susceptible to damage in TBI that affect interhemispheric integrity. In a previous study, diffusion tensor imaging (DTI) results indicated significant microstructural damage in the CC following TBI as reflected by a decrease in fractional anisotropy (FA). 6 Thus, the structural connectivity of the CC may exert salient influence on homotopic functional connectivity across the whole brain. 7 However, somewhat heterogeneous findings across modalities prohibit a converging perspective on system-level pathology, possibly due to limited studies addressing structure and function simultaneously after mild TBI (mTBI). 8 –11
Cognitive deficits, particularly impaired executive function, are pervasive, precede clinical diagnosis, and form the core of TBI-associated cognitive disabilities. 12 –14 In particular, executive function decline has been demonstrated in both early acute and later chronic phases following mTBI. 14,15 As the largest white matter tract in the brain, the CC plays a crucial role in cognitive function, and loss of structural integrity in the CC directly contributes to a decline in cognitive function. 16 –19 Executive function deficits affected by abnormal CC structure have also been reported in neurodegenerative diseases and neurodevelopmental disorders, including Parkinson disease (PD), autism, schizophrenia, and attention deficit disorder. 20 –24 One study reported volume loss in subregions of the CC in PD, with specific neuroanatomic distributions in PD patients with dementia and relationships between regional atrophy and different cognitive domains, such as midposterior callosal atrophy associated with executive function domains. 24 Although loss of structural integrity in the CC is also reported to be correlated with executive function in TBI patients, 12,25 few microstructural or morphologic magnetic resonance imaging (MRI) studies have examined CC abnormalities in different subregions following mTBI. Instead, previous studies have only investigated the midsagittal plane using area measurements, which lacks definitive anatomical landmarks that clearly demarcate anatomically and functionally distinct CC regions. 26
Considering the high functional specificity between CC interhemispheric structure connectivity and cortical projection targets of the topographically organized callosal subregions, 27 understanding the effects of traumatic axonal injury on cognitive function will require simultaneous investigation of the different subsections of structural injury and corresponding functional brain connectivity changes. One study of interhemispheric structural and functional connectivity in patients who suffered trauma from traffic accidents being studied within 2 d of being the accident suggested that CC-mediated aberrant interhemispheric structural connectivity may subserve alterations in interhemispheric functional connectivity. 28 However, that investigation provided limited information about the time-course of the span of structural injury in the CC and lacks fine division of CC regions, which is less relevant for considering both specific interhemispheric functional communications organized by neuroanatomic callosal division and evaluation of long-term neuroprotective therapies. Therefore, the present study conducted both cross-sectional and longitudinal examinations from early subacute to chronic stages of mTBI within 1 year of injury and aimed to: i) investigate microstructural CC integrity in five separate CC subregions defined with an established parcellation scheme by DTI; ii) measure whole brain interhemispheric functional connectivity changes using voxel-mirrored homotopic connectivity (VMHC) and link changes corresponding to different subsections of CC-projecting cortical areas; iii) evaluate relationships between structural and functional imaging measures as well as their possible link to behavioral consequence (particularly core cognitive components, such as executive function) following mTBI.
Methods and Materials
Participants
Participants from the local emergency department were enrolled between May 2013 and April 2016. Patients who underwent non-contrast head computed tomography due to head trauma formed the initial population of this study. Screening for mTBI was based on the World Health Organization's Collaborating Centre for Neurotrauma Task Force criteria. 29 The inclusion criteria were a Glasgow Coma Score of 13–15; one or more of the following: loss of consciousness <30 min, post-traumatic amnesia <24 h, and/or other transient neurological abnormalities (e.g., focal signs and seizure); no contraindications to MRI; and agreement to communicate by telephone or e-mail for 3 months and 6–12 months after enrollment and to come back to the hospital for follow-ups. Exclusion criteria were a history of neurological disease or psychiatric disorder, previous head injury, history of substance or alcohol abuse, intubation and/or presence of a skull fracture, administration of sedatives on arrival to the emergency department, spinal cord injury, or manifestation of mTBI due to medications or other injuries/problems (e.g., systemic injuries, facial injuries, intubation, psychological trauma, language barrier, coexisting medical conditions, or penetrating craniocerebral injury). Forty-two mTBI patients (23 males) with a mean ± standard deviation (SD) age of 37.4 ± 11.9 years were enrolled. All patients were initially assessed at the subacute phase and returned for their longitudinal visit at 3 months and 6–12 months follow-up. In addition, 42 sex-, age-, and sociocultural-matched healthy controls (HC; 24 males), with a mean ± SD age of 38 ± 9.7 years and no history of neurological or psychiatric disorder, were also recruited and received only one imaging and neuropsychological assessment. Another independent sample of diffusion data from 20 matched HC patients (10 males, mean ± SD age, 37.6 ± 9.8 years) was collected for the purpose of CC segmentation. All subjects gave written, informed consent after all experimental procedures were fully explained, and all research procedures were approved by the local Institutional Review Board in accordance with the Declaration of Helsinki.
Clinical assessment
Clinical assessments were performed within 48 h of MRI for all participants. The clinical protocol included broad neuropsychological and symptom assessments. The presence and duration of retrograde and post-traumatic amnesia were assessed using the Rivermead Post-Traumatic Amnesia Protocol. 30 All subjects underwent cognitive examinations, including Mini Mental State Examination and Clinical Dementia Rating. 31,32 Executive functions, such as set-shifting, inhibitory control, cognitive flexibility, and word generation fluency, were measured by the Trail-Making Test alternating-switch cost index. Self-reported symptomatology was assessed with the post-concussion symptoms scale, State Trait Anxiety Inventory (STAI-Y), Hamilton Depression Rating Scale, and Fatigue Severity Scale (FSS). 33 –37
Image acquisition
The protocol for scanning included a non-contrast CT scan for acute head injury using a 64-row CT scanner (GE, Lightspeed VCT), and 1.5-T Siemens MRI scanner (Erlangen, Germany). Patients were initially surveyed with non-contrast CT at the emergency room by a nonblinded neuroradiologist, and none were deemed to have trauma-related pathology. High-resolution T1-weighted images were obtained for each subject with T1-weighted 3-dimensional magnetization-prepared rapid acquisition gradient-echo sequencing [echo time (TE) = 2.8 ms, repetition time (TR) = 1900 ms, inversion time (TI) = 1000 ms, flip angle = 8°, slice thickness = 1 mm, field-of-view (FOV) = 256 mm × 256 mm, matrix size = 256 × 256], single-shot gradient-recalled echo planar imaging sequencing with 30 slices covering the whole brain (TR = 2000 ms, TE = 40 ms, flip angle = 90°, thickness = 4 mm, FOV = 224 mm × 224 mm, matrix size = 64 × 64), axial T2 turbo spin echo (TR = 4000 ms, TE = 79 ms, thickness = 5.5 mm, slices = 18, flip angle = 150°, FOV = 230 mm × 198 mm, matrix size = 231 × 384), axial T1 (TR = 195 ms, TE = 4.76 ms, flip angle = 70°, thickness = 5.5 mm, slices = 18, FOV = 230 mm × 187 mm, matrix size = 208 × 256), axial fluid-attenuated inversion recovery (TR = 8500 ms, TE = 84 ms, flip angle = 150°, thickness = 5.5 mm, slices = 18, FOV = 230 mm × 194 mm, matrix size = 173 × 256), and axial susceptibility-weighted imaging (TR = 49 ms, TE = 40 ms, flip angel = 15°, thickness = 2 mm, slices = 72, FOV = 230 mm × 230 mm, matrix size = 272 × 320).
DTI were acquired by a single-shot, spin echo-based and diffusion-weighted echo planar imaging sequence (TR = 7300 ms, TE = 99 ms, flip angle = 90°, thickness = 3 mm, FOV = 256 mm × 256 mm, matrix size = 128 × 128, two averages). DTI scans (b = 1000 s/mm2) were acquired with 30 diffusion gradient orientations, with the b = 0 repeated twice. Resting-state functional MRI (rs-fMRI) scans were acquired with 480 temporal volumes over a total of 16 min. All subjects were asked to close their eyes during rs-fMRI scanning. In addition, two certified neuroradiologists with 9 and 7 years' experience independently reviewed MRI scans (conventional T1, T2, and susceptibility-weighted images) to classify the presence of structural contusion and microbleeds for all subjects in random sequence; the reviewers were blind to clinical information and group membership (patient or control). Any disagreement between these two observers was resolved by consensus.
DTI data analysis
DTI data for study and independent samples were preprocessed using FMRIB's Diffusion Toolbox in the FMRIB Software Library (FSL). Preprocessing steps for DTI data, including skull stripping with the brain extraction tool was applied to the b0 image in each subject. Then, eddy current correction was used to correct for distortions and subject motions on DTI sequences by aligning diffusion-weighted images to the b0 image. Diffusion tensor fitting was used to estimate the diffusion tensor and calculate scalar DTI statistics. Then, diffusion tensor maps were nonlinearly registered to the standard target using affine alignments and were smoothed using a 6-mm full width at half maximum Gaussian kernel. 38
Quality control for DTI data
Because head motion induces bias in DTI scalar measurements, 39,40 quality assurances were conducted on head motions for all subjects. Subjects were excluded from further analysis if they were identified as motion outliers (3 SD greater than their cohorts). The rotation and translation parameters from each DTI acquisition were obtained using FSL’ s linear imaging registration tool (FLIRT) of each brain volume to the averaged b0 volume. 41
Parcellation of the CC and DTI metrics
Tractography was performed to conduct geometric partitioning schemes to subdivide the CC by using DTI data from an independent sample of 20 HC obtained from the same site with the same scanning protocol. 42,43 DTI-based fiber tracking involved 3-dimensional masks in the CC and cerebral cortex. The CC mask was defined in the Montreal Neurological Institute (MNI) space based on the Jülich probabilistic histological atlas included in FSL. In the cortex, five masks were adopted in each hemisphere, including the bilateral prefrontal areas, Brodmann area 6 [which is composed of the premotor cortex (PMC) and supplementary motor area (SMA)], primary motor areas, primary sensory areas, and parietal-temporal-occipital lobes (Fig 1). 44 Each fiber tracking was projected from these five specific cortical areas based on cortical segmentation. 42, 43 This analysis accommodated crossing fibers in each voxel, and the tracking was from all voxels in the CC to the five cortical regions in both hemispheres. 45 As a result, a probabilistic map from the CC to each of the five pairs of cortical masks was generated (Fig 2). Then, different CC voxels in each participant were classified into five classes according to the cortical region they mostly connected to (“winner-take-all”). 38, 46 The classification at an individual level was then fused as a merge result and transformed from the MNI space into the individual diffusion space for subsequent DTI analysis. 47
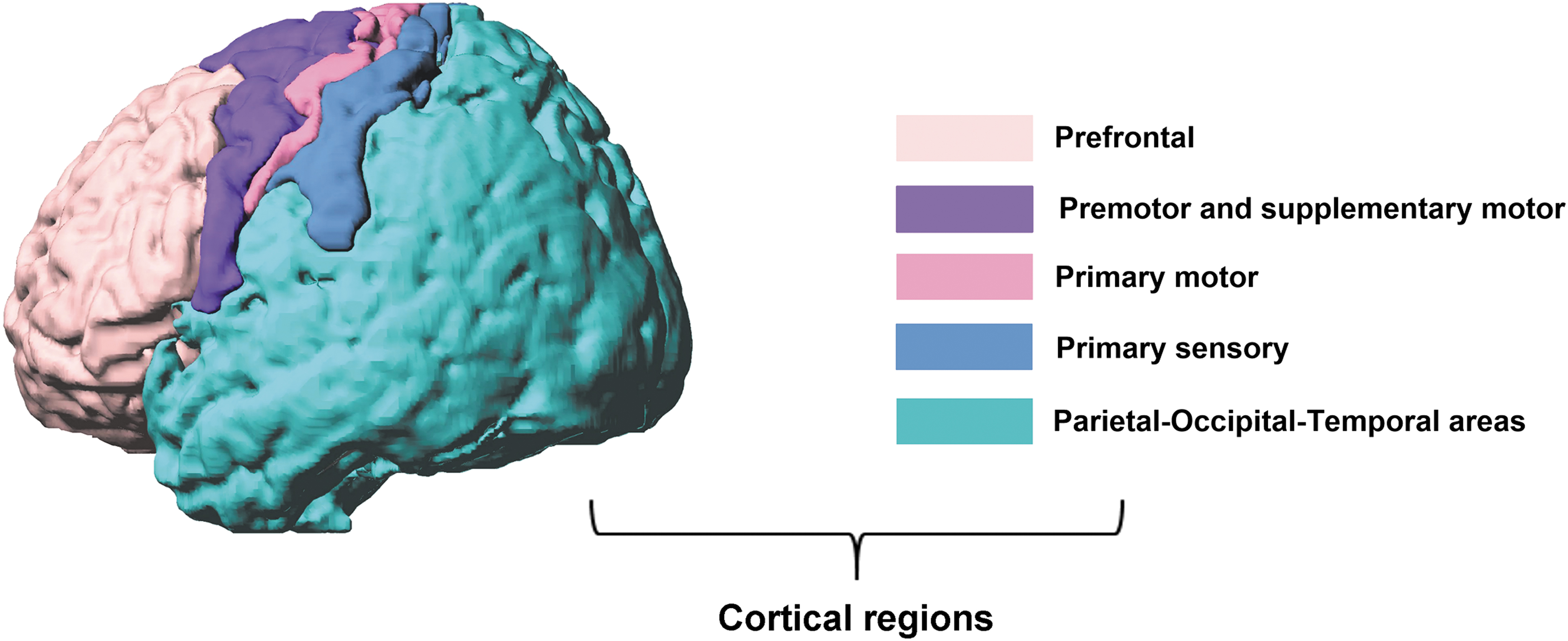
Cortical projection based corpus callosum (CC) segmentation. Five cortical regions used for fiber bundle tractography in the CC segmentation. Color image is available online.
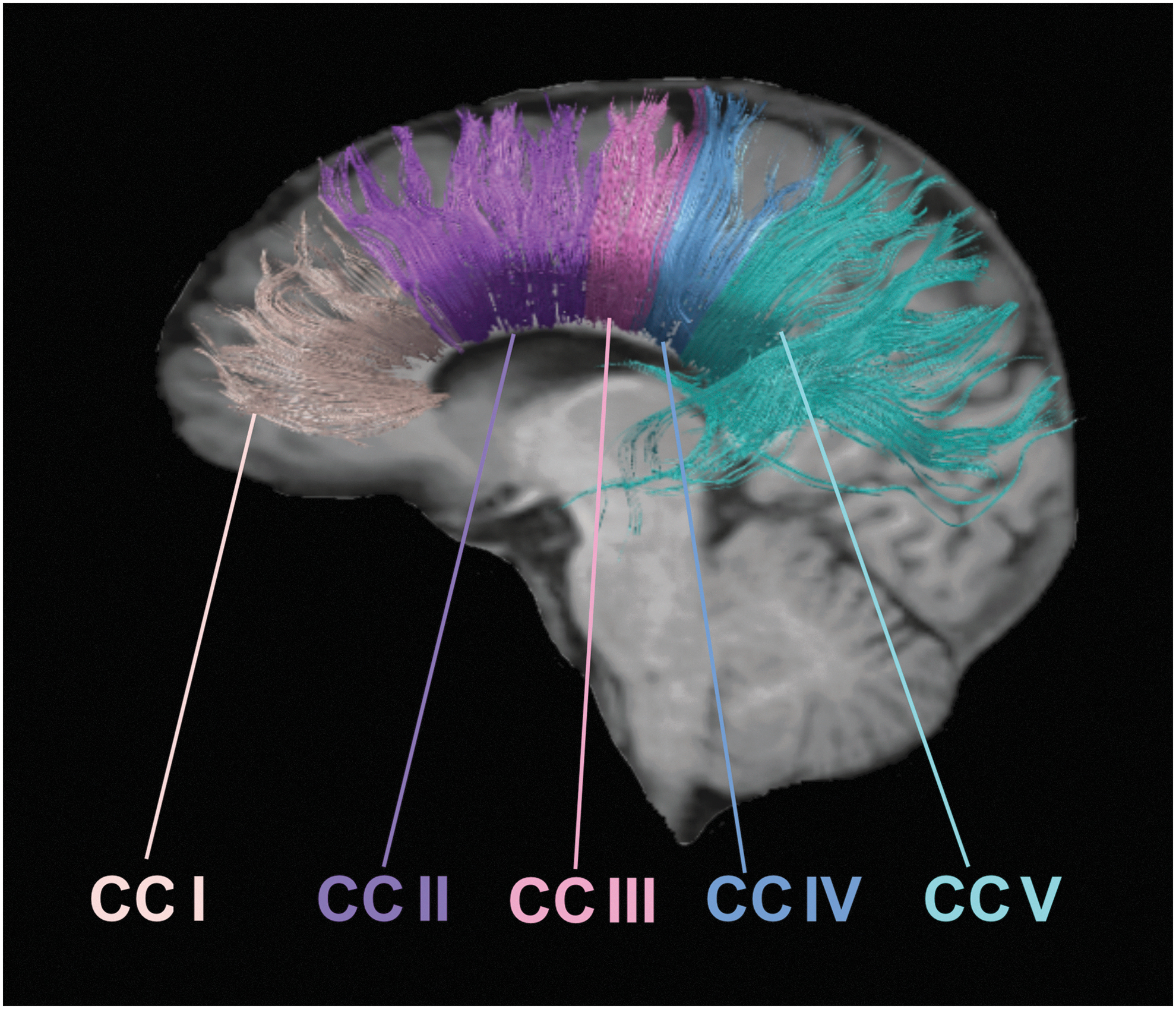
Cortical division corresponding transcallosal fiber bundle projection map of single subject's anatomical reference images. Sagittal views of all transcallosal fiber bundles projected into the pre-frontal cortex (corpus callosum, CC I), pre-motor cortex and supplementary motor area (CC II), primary motor area (CC III), primary sensory area (CC IV), and parietal-temporal-occipital cortical cortex (CC V). Color image is available online.
Preprocessing rs-fMRI Data
All rs-fMRI data were preprocessed using FSL 5.0.2.1. Functional data were analyzed using FMRIB's expert analysis tool (FEAT) version 6. The first five volumes were discarded to eliminate T1 relaxation effects. The preprocessing steps included motion correction using motion correction FLIRT, 41 brain extraction using the brain extraction tool 48 aligned with high-resolution anatomical volumes initially using linear registration FLIRT and then optimized using boundary-based registration, 49 spatial normalization (MNI space) with manual inspection to verify successful transformation, normalization of images with resection at a resolution of 2 mm × 2 mm × 2 mm, smoothing using Gaussian filters of 6-mm full width at half maximum, and spurious variances (head motion, ventricular and white matter signal, and derivatives of each of these signals) were removed using linear regression and band-pass filtering (0.01–0.08 Hz). Data from participants whose head motion exceeded 1.5 mm were removed from subsequent analyses as recent studies have indicated that micro head motion can significantly influence measures derived from fMRI. 50,51 Voxel-specific head motion, including voxel-specific frame-wise displacement and voxel-specific total displacement values for each subject using the Data Processing Assistant for Resting-State fMRI toolbox in SPM8, was also computed.
Interhemispheric correlation analysis
Resting State Functional MR Imaging toolkit was used to carry out VMHC analysis. 52 To account for geometric differences between hemispheres, the spatial normalization was refined from individual anatomical to MNI152 template space using the group-specific symmetrical template. In detail, all registered structural images were averaged to create a mean normalized T1 image which was then averaged with its left-right mirror image to generate a group-specific symmetrical template using FSLUTILS. Nonlinear registration to this symmetrical template was performed for each participant, and the resultant transformation was applied to each participant's preprocessed functional data.
The time-course of each voxel was correlated with the time-course of the homologous voxel in the other hemisphere (as determined by the x coordinates in MNI space). Considering the influence of head motion, mean voxel-specific frame-wise displacement was used as a covariate for group comparisons of interhemispheric connectivity. 50 To avoid the VMHC accounted for by applying spatial-smoothing, all further analyses were restricted to the lateral aspects of the brain by including only gray matter voxels that were at least 6 mm away from the midline. Correlation coefficients of each participant's voxels were converted to z values using Fisher's transformation to improve normality.
Statistical analysis
The Shapiro-Wilk W-test was used to test for normality distribution of all continuous variables. The independent two-sample t-test and the Mann-Whitney test were used to compare group differences based on data normality. Chi-square analyses were applied to assess categorical variables. Effect sizes (Cohen's d) were computed to demonstrate the magnitude of observed differences. FA values for each of the five CC subsections were compared between the mTBI cohort and HC in both initial and follow-up phases, with age, sex, education level, post-injury days, and presence of microbleeds as covariates using a general linearity model and Bonferroni correction for multiple comparisons, yielding an adjusted P-level of P < 0.01 (P < 0.01 [0.05 ÷ 5] for each of the five CC subsections). Group comparisons of VMHC were conducted using a voxel-wise two-sample t-test, controlling for age, sex, education level, post-injury days, and presence of microbleeds as covariates. A Monte Carlo simulation was used to estimate the cluster size for the correction of multiple comparisons. A corrected significance level of P = 0.05 was achieved with cluster correction. To test the correlations between the structural and functional imaging measures presented with between-group difference, Pearson's correlation analyses were performed with a threshold cluster level of P < 0.05 (Gaussian Random Field-corrected). Spearman correlation was also conducted and restricted to clinical assessment and regional VMHC showing a significant time effect as a function of recovery with Bonferroni correction for multiple comparisons.
Results
Demographic and clinical assessments
Demographics and behavioral statistics for the entire cohort of mTBI patients and HC participants are summarized in Table 1. Patients were initially assessed in the subacute phase post-injury (T-1: 6.9 ± 5.2 d; range, 2–13 d). All patients returned for their longitudinal follow-up visit at 3 months (T-2: 93 ± 27.3 d; range, 51–129 d) and 6–12 months (T-3: 278 ± 86.2 d; range, 167–395 d). There was no correlation between any clinical assessment and number of days from injury to initial or follow-up scan (Spearman correlation, r = - 0.326 - 0.358, P > 0.1), even the relative broad SDs in post-injury timing (details in Supplementary Table S1). None of patients had visible contusion lesions using conventional neuroimaging techniques, and 3/42 (7%) patients exhibited cerebral microbleeds on susceptibility-weighted imaging.
Demographic and Neuropsychological Data for Subacute mTBI and HC Participants
mTBI, mild traumatic brain injury; HC, healthy controls; SD, standard deviation; PSS, Post-concussive Symptoms Scale; IPS, information processing speed by Trail-Making Test A; EF, executive function by Trail-Making Test B-A; MMSE, Mini Mental State Examination; CDR, Clinical Dementia Rating; HDRS, Hamilton Depression Rating Scale; STAI-Y, State Trait Anxiety Inventory; FSS, Fatigue Severity Scale.
The following analysis was used in the presence of microbleeds as covariates. Those caused by injury included motor vehicle accidents (20 patients, 47.7%), assaults (14 patients, 33.3%), struck by an object (3 patients, 7.1%), and falls (5 patients, 11.9%). Nineteen (45.2%) patients experienced loss of conscious. There were no differences between patients with mTBI and HC in major demographic variables (P > 0.05). For the initial assessment, patients with mTBI presented significantly higher post-concussive symptoms scale, Clinical Dementia Rating, Hamilton Depression Rating Scale, STAI-Y, and FSS scores compared with HC (P < 0.001). mTBI patients presented worse performance on neurocognitive tests (information processing speed using Trail-Making Test A, P < 0.001; executive functions using Trail-Making Test B-A, P < 0.001) and demonstrated no significant differences on Mini Mental State Examination (P = 0.87) and STAI-Y (P = 0.27) scores compared with HC.
Longitudinal comparisons
Longitudinal analyses were conducted to examine changes in self-reported symptomatology as a function of recovery. The main effect of time was significant only in the STAI-Y (F 2, 121 = 11.39, P < 0.001). The main effect of time also showed a nonsignificant trend in executive function (F2, 123 = 6.28, P = 0.051). Other measures presented no significant time effect (all P > 0.05). STAI-Y scores were significantly improved only at T-3 relative to T-1 (P < 0.001, Cohen's d = 1.09) but not T-2 (P = 0.19, Cohen's d = 0.06) following multiple comparison correction. STAI-Y scores recovered to normal levels at T-3 in mTBI patients (P = 0.148, t1, 80 = 1.67, Cohen's d = 0.35). Other measures (including information processing speed using Trail-Making Test A, executive functions using Trail-Making Test B-A, post-concussive symptoms scale, Hamilton Depression Rating Scale, and FSS) were significantly higher in mTBI patients than HC at 14 d post-injury (T-1: all P < 0.001), 3 months (T-2: all P < 0.01), and 6–12 months (T-3: all P < 0.01). In addition, the comparisons of neuropsychological and self-rating scores between mTBI patients and HC at both follow-up times (3 and 6–12 months) are summarized in Supplementary Table S2.
Fiber tract integrity in the CC
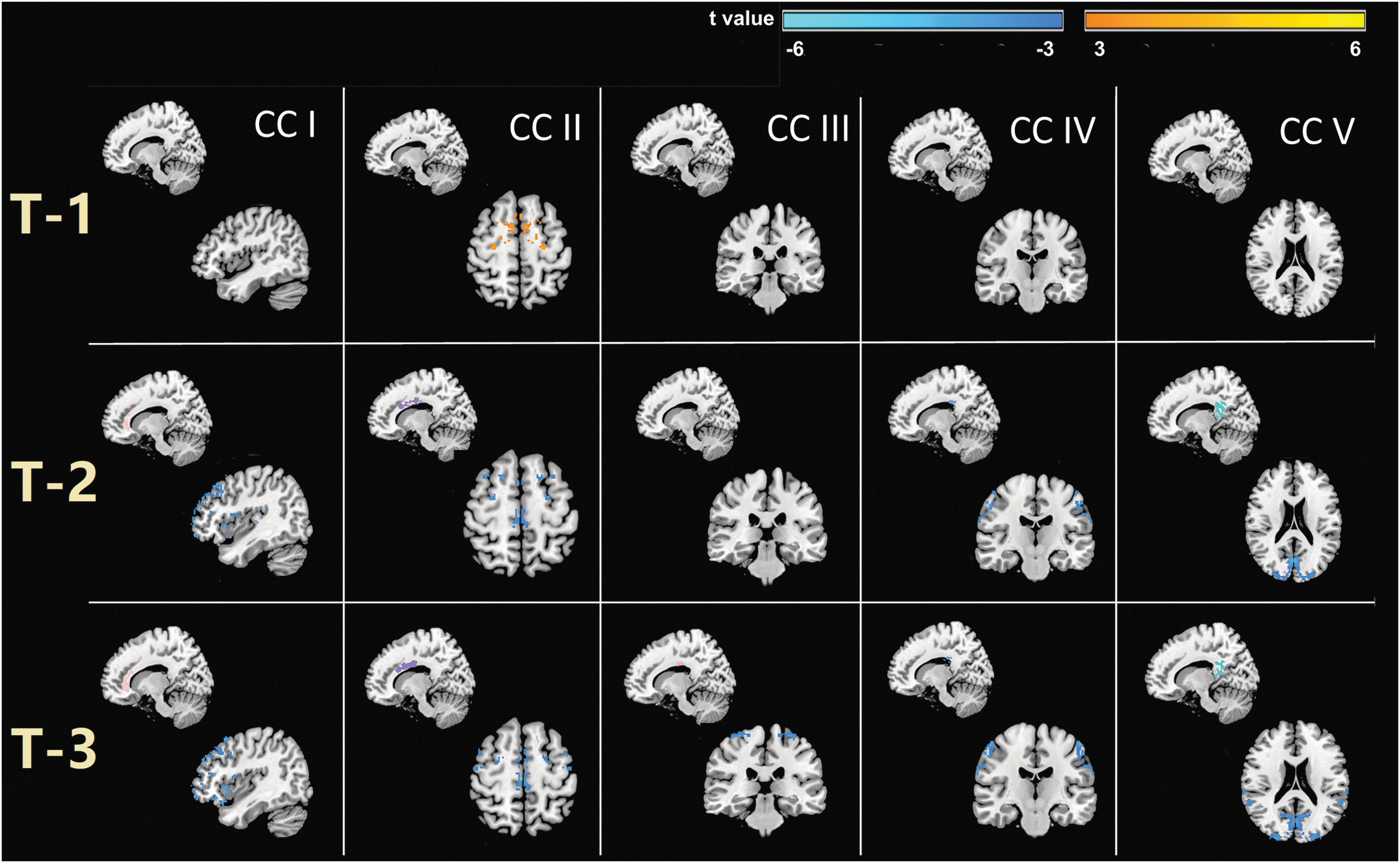
For CC subsection integrity, FA reductions were only significant in CC II at T-1, and this region showed sustained decreases after 3 months. Decreased FA of the CC also emerged in the wider subregions, including CC I, IV, and V at T-2. For T-3, loss of integrity and sustained injury in the CC extended to all five subregions with even more salient reductions (Fig 3). To further test whether microstructural changes were partly associated with neuropsychological differences, between-group differences were also compared in the FA metric of each of the five CC subsections in both initial and follow-up phases with STAI-Y, FSS, Trail-Making Test A, and Clinical Dementia Rating (these tests showing significant between-group differences) as covariates using a general linearity model (summarized in Supplementary Table S3). The results showed that neuropsychological changes can only influence between-group FA differences, especially in CC II during T-1 (P = 0.05) and CC IV during T-2 (P = 0.047) and T-3 (P = 0.049). Most of the results that were kept remained after regression (shown in Supplementary Table S3).

Group comparisons of impairments in the corpus callosum (CC) subregions between subjects with mild traumatic brain injury (mTBI) and healthy controls (HC) in different stages using a general linearity model and Bonferroni correction for multiple comparisons, yielding an adjusted level of p < 0.01. Spatial correspondences between findings of impairment in both the subacute and follow-up phases of CC subregions (first row) and statistical maps group comparison of diffusion metrics (fractional anisotropy [FA]) reductions (second row). Impairment was noted in CC II (T-1); CC I, CCII, CC IV, and CC V (T-2); and all five subregions (T-3), respectively. Color image is available online.
Regional variations of interhemispheric functional connectivity in VMHC
The results demonstrated initially increased VMHC mainly in the PMC/SMA of mTBI patients compared with HC. By contrast, reverse changes (reductions) of VMHC were found in the prefrontal, PMC/SMA, primary sensory, and parietal-temporal-occipital cortical areas at 3 months post-injury. At 6–12 months, decreased VMHC were found in the prefrontal, PMC/SMA, primary motor, primary sensory, and parietal-temporal-occipital cortical areas. Except for cortical regions, prominently decreased VMHC further extended into more widely subcortical areas, such as the parahippocampal gyrus/amygdala, caudate, and thalamus (Fig 4 and Supplementary Table S4).
Spatial correspondence between diffusion metrics (fractional anisotropy [FA]) reduction and inter-hemispheric functional connectivity voxel mirrored homotopic connectivity (VMHC) changes. The color bar indicates statistical maps of VMHC significant contrast t values of subjects with mild traumatic brain injury (mTBI) and healthy controls (HC). Significance level of p < 0.05 with a cluster size > 160 mm3 for the correction of multiple comparisons. Correspondence subregions of the corpus callosum (CC) FA reduction are shown in different columns (from subacute to follow-up phases). Coronal and axial images, left is left. T-1, sub-acute phase; T-2, 3 month phase; T-3, 6–12 month phase. Color image is available online.
Correlation analysis and clinical potential findings
There were no correlations between regional VMHC and FA values of separate subsections in the CC (all for P > 0.09). There was a relationship between the decreased VMHC in the dorsolateral prefrontal cortex (DLPFC) and poor performance on executive function only in the chronic stage at 6–12 months post-injury after Bonferroni correction for multiple comparisons (r = 0.67, P < 0.005). To further test whether decreased functional connectivity in the DLPFC contributed to poor executive function in mTBI patients, all time points were combined and executive function for mTBI patients was dichotomized into impaired or normal levels depending on whether the Trail-Making Test B-A score was greater than the norms adjusted by both age and education level. 53 mTBI patients with poor executive function showed a significant decrease in VMHC in the DLPFC (Z = 0.216 ± 0.12) compared to mTBI patients with normal executive function (Z = 0.432 ± 0.254, t 2, 124 = -6.31, P < 0.001) and HC (Z = 0.44 ± 0.13, t 2, 99 = 6.82, P < 0.001) after Bonferroni correction for multiple comparisons (shown in Supplementary Fig. S1).
Discussion
Abnormalities in the CC are of particular interest in mTBI given the central role of this large white matter fiber bundle in interhemispheric functional connectivity and coordination of cognitive function. The present study found that loss of integrity in different sections of the CC demonstrated salient persistence and time-dependent regional specificity within 1 year post-injury. The impairment spanned multiple segments from the initial CC II within 14 d post-injury, CC I, II, VI, and V at 3 months, and to all subregions from 6–12 months. Moreover, impaired interhemispheric structural connectivity through the CC corresponded well to regions with altered interhemispheric functional connectivity. Decreased interhemispheric functional connectivity in the DLPFC thereafter contributed to the poor executive function outcome in patients with mTBI. The CC-facilitated interhemispheric spread and multiple bihemispheric regions connected through the five different CC regions interfered with recovery from mTBI, which is in line with previous studies suggesting the concept of mTBI as a widespread cerebral network disorder.
Herein, CC II was found to present the earliest injury, with decreased FA. This area is generally located in the anterior part of the midbody of the CC, which is inconsistent with previous studies showing damage in the genu and splenium of the CC during subacute mTBI. 54 –58 Contrary to the current results, previous studies have shown prominent increases FA in the genu of the CC at subacute phases (within 21 d post-injury). 55, 56 Such heterogenous results may be due to differences in relatively modest sample sizes (e.g., others: 8 < n < 35; current study: n = 42), major differences in time from injury to initial imaging (others: 1–60 d post-injury; current: 6.9 ± 5.2 d post-injury), 54 –58 diverse characteristics of injury (others: sport-related concussion) 54,55 , not controlling for abnormal imaging findings 54, 57, 58 (current: limited to an emergency department cohort carefully screened for pre-injury medical, psychiatric, and neurological problems and completely excluded patients with legal disputes), and DTI analysis techniques (others: CC measurement area based on midsagittal view and division into three subsections; 55, 57, 58 current: divided CC into five subregions). The current findings also show the injury area expanded from the anterior midbody of the CC (CC II) in T-1 into both anterior (CC I and II) and posterior regions (CC IV and V) at T-2 and continued to the whole CC by T-3. In addition, the present results showed the structural integrity of CC II became impaired very early on and presented sustained injury up to 1 year after mTBI. The neuropsychological changes observed herein were also found to influence between-group FA differences, especially in CC II during T-1 and CC IV during T-2 and T-3. This result may indicate that the loss of structural integrity in the CC may be partly explained by individual neuropsychological profiles.
In addition, clinical symptoms continued to emerge for months subsequent to injury, persisting beyond 1 year, with some neuropsychological assessments failing to show any trend toward improvement. This result indicated recovery from mTBI was a nonlinear process and that the time-course to full recovery for some patients might be protracted, unlike other reports showing recovery of cognitive symptoms within 3 months. 59,60 It is possible that full recovery may not ever be achieved in a subpopulation of patients. In current neuroimaging findings, impairments were found to span multiple segments from the initial CC II in the subacute phase to all five subregions after 6–12 months, with greater extent and ongoing salient FA reductions over time. Previous studies have also found a reduction in FA that spreads to whole regions of the CC 6–14 months post-injury, 61 with continuing reduction beyond 1 year following mTBI. 62 Given the central role of the CC in coordination of cognitive function, a recent study investigated atrophy of the CC in PD and its relationship to cognitive impairment. They found that most cognitively impaired participants (PD patients with dementia) can be distinguished from cognitively-intact participants with PD by volume loss across multiple callosal segments. 24 Therefore, the extended range of CC injury after mTBI may be a risk factor for neurodegenerative diseases, such as PD and Alzheimer disease.
Interhemispheric communication is an important organizational principle of the human brain and reflects individual differences in brain development. Such abnormalities are of interest given the role of the CC in coordinating interhemispheric functional connectivity and the highly topographic organization of its projections. One recent study examined both interhemispheric structural and functional connectivity in patients with amyotrophic lateral sclerosis and indicated that impaired interhemispheric neural communications mediated by the CC may subserve alteration of interhemispheric functional connectivity. 38 DTI tractography maps in the present study demonstrate the link between injuries in CC II with increased VMHC in the PMC/SMA exclusively in the subacute phase. Structural damage within caused by the CC may induce preferential functional connectivity changes in PMC/SMA area. Another study also found increased regional homogeneity of the SMA during the subacute phase after sports-related concussion compared with healthy athletes. 63 The current findings provide the first evidence of hyperconnectivity in the interhemispheric functional connectivity constructed by VMHC analysis within 14 d after mTBI when neurophysiology undergoes rapid changes. One recent study indicated that acute stress shifts the brain into a state that fosters rapid defense mechanisms seen as increased interconnectivity within a network, including inferiotemporal and temporoparietal regions. 64 Evidence from experimental TBI studies also show that the hyperconnectivity only maintained at 7 d but did not persist at 4 weeks post-injury. 65 It is suggested that such “pruning” might be an initial physiologic response indicative of reorganization whereby synaptic strengthening occurs via co-activated inputs leading to enhanced widespread connectivity. Current findings also suggest such hyperconnectivity is a transient event since the patterns did not persist into more chronic periods at 3 and 6–12 months post-injury. After 3 months, aberrant VMHC reduction was found in much wider brain regions, including the prefrontal, PMC/SMA, primary sensory, and parietal-temporal-occipital cortical areas. Expansion of structural damage in mTBI may affect the connectivity of its corresponding functional projection area and thus affect cognitive function.
These homotopic functional connectivity reductions continued and extended into all projection cortical areas after 6 months. Specifically, the DLPFC showed a greater decrease in VMHC that was significantly related to poorer performance in executive functions but only in the more chronic stage 6–12 months post-injury. This finding was also supported by other studies which found functional connectivity damage in the prefrontal, PMC/SMA, and parietal-temporal-occipital cortical areas after an average of 7 or 28 months post-injury. 66,67 The present results also showed VMHC reductions in the primary motor areas after 6–12 months. Patients with mTBI typically show impairments in memory, information processing speed, and attention, so attenuated VMHC in the motor-related cortex may further indicate multisystem damage 6 months post-injury and beyond. 68,69 One study demonstrated compelling evidence that early diagnosis of motor-related dysfunction in PD may decrease the burden of TBI. 70
Although the current findings of interhemispheric functional and structural connectivity were mostly convergent, a divergence was noted. Specifically, decreased functional connectivity of subcortical regions existed in the chronic phase 6–12 months post-injury and was mainly located in the parahippocampus/amygdala, caudate, and thalamus. Instead of directly impacting structural pathways through the CC, these functional alterations may be mediated by indirect structural connections (i.e., via fiber tract links with cortical-subcortical pathways). 71 For example, the thalamus is centrally located in the brain and has abundant ascending and descending white matter projections into multiple cortical regions. In the current findings, post-concussion syndromes persisted for up to 1 year. Yeh et al. reported an association between damaged thalamocortical projections and worse post-concussive symptomology in Veterans. 72 It was inferred that the loss of ability to integrate information from multiple sensory modalities and inhibition of extraneous sensory input due to abnormal interhemispheric functional communication in the thalamus may therefore result in persistent complaints following mTBI. In addition, the present study also found no significant correlations between regional VMHC and FA changes of separate subregions in the CC (all P > 0.09). These results may be due to the fact that rs-fMRI and diffusion metrics were at different spatial resolutions, with rs-fMRI being voxel-wise and diffusion metrics being region of interest-wise. The current findings further support to the notion that structural connectivity provides the material backbone for communication between brain regions and place constraints on functional interactions across brain networks. 73 –75
Some limitations should be noted in the current research. First, the human brain is not completely symmetrical. The present analysis of VMHC assumes and is based on a symmetrical standard template. Therefore, the results were not sensitive to potential asymmetric differences. Second, though impaired interhemispheric structural connectivity through the CC corresponded well with regions presenting altered interhemispheric functional connectivity, there were no significant correlations between interhemispheric functional (VMHC) and structural connectivity (FA in CC subsections). This discrepancy may be due to the fact that fMRI (voxel-wise) and DTI data (region of interest-based) analyses were at different spatial resolutions.
Conclusions
By accurately dividing the CC, the present study found that loss of structural integrity persisted up to 1 year following mTBI. Moerover, the scope of CC damage presented saliently time-dependent regional specificity. In particular, CC II may serve as a stable pattern for indicating long-term damage in very early-stage mTBI. Impaired interhemispheric structural connectivity through the different sections of the CC corresponded well with regions presenting altered interhemispheric functional connectivity, suggesting CC injury might be a risk factor for cognitive decline and neurodegenerative disease that interfere with recovery.
Footnotes
Acknowledgments
This research was supported by the National Natural Science Foundation of China (Grant nos. 81571752, 81771914, and 81571640), National Key Research and Development Plan of China (No. 2016YFC0100300), and Fundamental Research Funds for the Central Universities (No. Xjj 2018229).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.