
Abstract
Thermal diffusion flowmetry (TDF) is an appealing candidate for monitoring of cerebral blood flow (CBF) in neurocritical-care patients as it provides absolute measurements with a high temporal resolution, potentially allowing for bedside intervention that could mitigate secondary injury. We performed a systematic review of TDF-regional(r)CBF measurements and their association with (1) patient functional outcome, (2) other neurophysiological parameters, and (3) imaging-based tissue outcomes. We searched MEDLINE, EMBASE, SCOPUS, BIOSIS, GlobalHealth, and the Cochrane Databases from inception to October 2018 and relevant conference proceedings published over the last 5 years. Nine articles that explored the relationship between TDF-rCBF, mortality, and Glasgow Outcome Scale (GOS) or GOS-Extended (GOS-E) at various intervals were included. Despite being based on an overall weak body of evidence, our analysis suggests a link between sustained low or high CBF and poor functional outcome. Twenty-five studies reporting associations with neurophysiological parameters were included. The available data also point to an association between low or high TDF-rCBF and intracranial hypertension. TDF-rCBF appears to correlate well with regional brain tissue oxygenation measurements. We found no studies reporting on imaging-based tissue outcome in relation to TDF. In conclusion, despite being based on a relatively weak body of evidence, the available literature suggests a link between consistently abnormal TDF-rCBF values, intracranial hypertension, and poor functional outcome. TDF-rCBF also appears to correlate well with regional measurements of brain tissue oxygenation. Currently, such monitoring should be considered experimental, requiring much further evaluation prior to widespread adoption.
Introduction
Thermal diffusion flowmetry (TDF) allows for real-time continuous measurement of absolute cerebral blood flow (CBF). There is growing interest in employing this monitoring technique in patients with severe acute neurological insults such as traumatic brain injury (TBI) as it theoretically facilitates early bedside detection of ischemic brain tissue at risk for secondary injury. 1 –4 In contrast, the traditional positron emission tomography (PET) and computed tomography (CT)-based radiographic methods for CBF measurement only allow for snapshot assessments and may not be suitable for unstable patients who are not able to tolerate transport for image acquisition, 5 and it is uncertain if invasive brain tissue oxygen (PbtO2) monitors measure a surrogate of true CBF versus extracellular oxygen diffusion capacity.
Commercially available TDF probes (Bowman Perfusion Monitor and Saber) work by calculating the power required to maintain a temperature difference between a proximal and a distal thermistor, which is directly proportional to cerebral tissue perfusion. The probes can either be placed on a cortical surface of interest (Saber) or directly in the brain parenchyma (Bowman Perfusion Monitor). Despite long-standing use of TDF in experimental models and recent interest in incorporating it into a multi-modal monitoring regimen, there is currently no consensus on thresholds for intervention based on TDF-CBF measurements, or a comprehensive understanding of how to employ such a device for standard monitoring of the critically ill TBI patient. The consensus summary by the International Multidisciplinary Consensus Conference on Multimodality Monitoring provides little additional guidance, merely stating that a “TDF probe may be used to identify patients with focal ischemic risk within the vascular territory of the probe,” a “weak” recommendation based on “very low quality evidence.” 6 However, a comprehensive breakdown and review of the literature was not provided, particularly the association between TDF-measured CBF and patient-oriented outcomes such as global functional outcome, other physiological measures, and imaging-based tissue outcomes.
The purpose of this scoping systematic review was to synthesize the available evidence on TDF in adult TBI in a robust and comprehensive manner to understand the association between this monitored variable and: global patient outcome, other measured aspects of cerebral physiology, and documented imaging-based tissue fate. Our review was designed to address the following three key questions: Is there an association between TDF-based CBF measurements and functional patient outcomes? Is there an association between TDF-based CBF measurements and commonly monitored neurophysiological parameters? Is there an association between CBF parameters measured by thermal diffusion and imaging-based tissue outcomes?
Methods
A scoping systematic review of the literature was conducted using the methodology described in the Cochrane Handbook for Systematic Reviewers. 7 Data items were reported in accordance with the preferred reporting system for systematic reviews and meta-analyses (PRISMA). 8 The search questions and search strategy were developed by consensus between the primary author and the senior author (FM and FAZ).
Search questions
The primary and secondary research questions for this review were:
Primary
Is there an association between CBF parameters measured by thermal diffusion and functional patient outcome in TBI patients in need of neurocritical care?
Secondary
(A) Is there an association between CBF parameters measured by thermal diffusion and other commonly measured neurophysiological parameters in TBI patients in need of neurocritical care? (B) Is there an association between CBF parameters measured by thermal diffusion and imaging-based tissue outcomes?
Functional outcome
For our primary research question, functional outcome measures of interest included any description of morbidity, mortality, functional outcome scale score (e.g., Glasgow Outcome Scale [GOS], or GOS-Extended [GOS-E]) or cognitive function assessments. Complications associated with TD monitoring were also recorded as a secondary outcome measure when available.
Neurophysiological outcome and imaging-based outcome
For our secondary research questions, measures of interest included any monitoring correlates of cerebral physiology such as intracranial pressure and compliance, autoregulation indices, brain tissue oxygenation, microdialysis analytes, entropy, and non-TD measures of cerebral CBF. Tissue outcome of interest was radiological evidence of ischemia, infarction, or atrophy of brain parenchyma during the acute hospital stay or at long-term follow-up, utilizing CT, computed tomographic angiography (CTA), computed tomographic perfusion (CTP), xenon CT (Xe-CT), magnetic resonance imaging (MRI), MR angiography (MRA), MR perfusion (MRP), MR spectroscopy (MRS), and PET.
Inclusion and exclusion criteria
Inclusion criteria were all studies enrolling adult (18 years or older) moderate and severe TBI (GCS score 3–12) patients in which TDF was used and any of the primary or secondary outcomes of interest were reported. Studies that enrolled pediatric or mild TBI patients exclusively, non-English studies, and case reports or studies that used non-TD-based CBF probes were excluded.
Search strategy
MEDLINE, EMBASE, SCOPUS, BIOSIS, GlobalHealth, and the Cochrane Databases were searched from inception to October 2018 using the strategy detailed in Supplementary Appendix A. Relevant meeting proceedings for the last 5 years were also screened to identify unpublished work on TDF use in the TBI population. A list of society meetings searched can be found in Supplementary Appendix B. Lastly, all the review articles discussing TDF use in TBI that we identified through our database search were set aside and their reference lists were searched for additional primary research articles meeting our inclusion criteria.
Study selection
Two of the authors (FM, FAZ) reviewed all of the articles returned by our search strategy in a two-step process. A first filter was conducted based on manuscript titles and abstracts to identify articles potentially meeting our inclusion criteria. A second filter was then performed on the identified articles by reviewing their full text to confirm that they met the inclusion criteria and that the primary or secondary outcome measures of interest were reported. Any discrepancies between the two reviewers were discussed and resolved by involving a third reviewer if required.
Data collection
Data of interest pertaining to demographics, study characteristics, and outcome measures were extracted from the final list of relevant articles and abstracts and compiled in an electronic database. Specific data fields included article location, study type, sample size, mean age, functional and physiological outcome measures, and complications.
Bias assessment
For all the final articles and abstracts to be included in our review, risk of bias was assessed using the RTI item bank. 9 Based on scores for each of the 29 bank items, studies were classified as either high risk (H), low risk (L), or unclear risk (U) for each of the bias type sub-domains. This assessment can be found in Supplementary Appendix C.
Statistical analyses
The heterogeneity in outcome reporting and lack of robust quantitative data for most of the studies included in this review did not allow for a meta-analysis.
Results
Search strategy results
A PRISMA flow diagram outlining our search strategy results at each step can be found in Figure 1. A total of 1711 articles were identified through our database search. Of those, 141 duplicates were removed. Five additional relevant articles were found through a reference list check of review articles, and one abstract was identified from the gray literature search. The first filter through titles and abstracts applying our inclusion and exclusion criteria yielded 48 eligible articles. Our subsequent full text review provided 25 final articles that met our criteria for the functional and/or physiological outcome measures. We identified no studies that reported imaging-based tissue outcome in relation to TDF measurements.
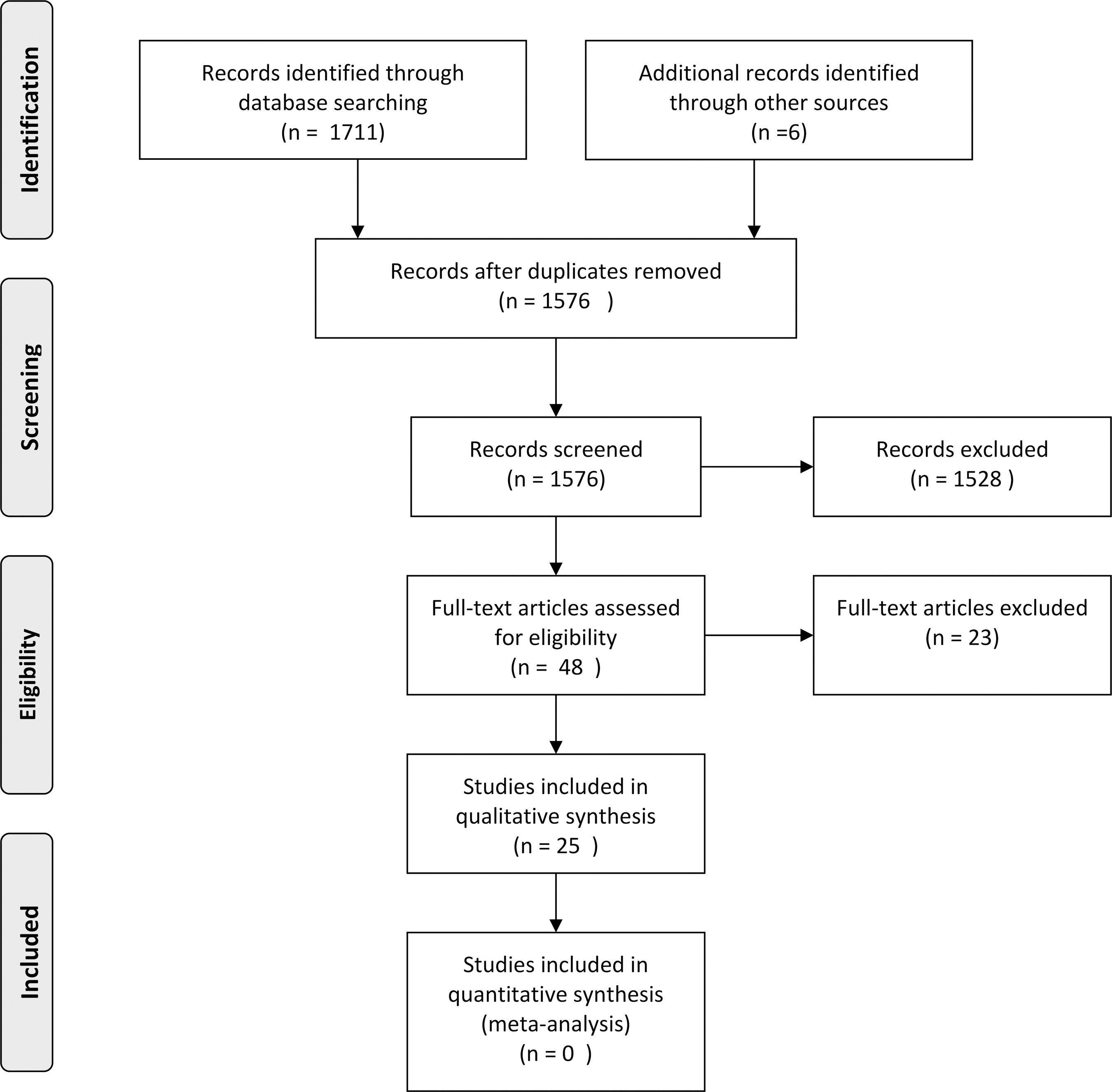
PRISMA flow diagram.
Study description and demographics
Of the 25 articles included in this review, 17 are formal publications 10 –27 and 8 are meeting abstracts. 18,28 –33 Of these articles, 23 have a prospective 10,11,13 –33 and 2 have a retrospective observational design. 12,34 In total, 18 studies included only severe TBI (defined as admission Glasgow Coma Scale [GCS] score 3–8) patients, 11 –13,15–18,28 –30,33 3 studies also included patients with moderate TBI (GCS score 9–13), 14,21,27 and 2 studies included TBI patients of unspecified severity. 31,34 Of the studies enrolling severe TBI patients only, 3 studies focused on patients undergoing a neurosurgical procedure. 10,16,34 Lastly, 2 studies also enrolled patients with a non-TBI acute neurological insult such as a spontaneous intracerebral hemorrhage 23 or subarachnoid hemorrhage. 26 The number of subjects enrolled ranged from 3 to 56, but one abstract did not specify the total sample size. 32 Across all studies, there were a total of 443 patients with TBI who underwent CBF monitoring by a thermal diffusion technique. The mean age ranged from 21 to 52 years, but 11 studies did not report any information related to patient age. Details of concurrent neurocritical care interventions were not described in most article. Tables 1 through 3 detail the study populations and design for each included article.
Study Characteristics and Patient Demographics
BIS, bispectral index; CBF, cerebral blood flow; CBFx, cerebral blood flow index; CBFx-CPPopt, cerebral-blood-flow-index-based optimal cerebral perfusion pressure; CO, cerebral oximetry; CO2, carbon dioxide; COx-CPPopt, cerebral-oximetry-based optimal cerebral perfusion pressure; CPP, cerebral perfusion pressure; CPPopt, optimal cerebral perfusion pressure; CSD, cortical spreading depression; ETCO2, end-tidal carbon dioxide; GCS, Glasgow Coma Scale; ICH, intracerebral hemorrhage; ICP, intracranial pressure; MAP, mean arterial pressure; ORx-CPP, brain-tissue-oxygen-based optimal cerebral perfusion pressure; PbtO2, brain tissue oxygen tension; PRx, pressure reactivity index; rCBF, regional cerebral blood flow; SAH, subarachnoid hemorrhage; sXE-CT, stable xenon-enhanced computed tomography; sXE-CT CBF, cerebral blood flow measured by sXE-CT; TBI, traumatic brain injury; TD, thermal diffusion; TD-CBF, cerebral blood flow measured by thermal diffusion; TD-rCBF, regional cerebral blood flow measured by thermal diffusion.
Thermal diffusion flowmetry technique
The type of thermal diffusion device used was parenchymal in 16 studies 11 –13,16–20,23,24,26,30 –34 and cortical for the remaining 9 studies. 10,14,15,21,22,25,27 –29 CBF measurements are reported in terms of mL/100 g/min. The measurement period varies between studies and patients, but was usually initiated within hours of admission to an intensive care unit and lasted for up to 10 days after admission. Placement was achieved via a bedside cranial access kit burr hole, via a small dedicated craniotomy, or at time of craniotomy or craniectomy for a TBI-related indication. Most studies targeted relatively normal appearing cortex or white matter in the frontal region, but a few studies specifically targeted perilesional parenchyma to monitor tissue at high risk for secondary injury. 13,16,25 In 2 studies, the authors specifically targeted the least-injured hemisphere, 19,20 but the rationale is not discussed. Most studies described confirming probe placement by routine post-insertion CT scan of the head. Although the commercially available TDF probes are said to monitor blood flow “continuously,” they necessitate frequent recalibration periods (every 30 min to 2 h, a calibration that usually takes 2–5 min) during which recordings are interrupted and this must be kept in mind when interpreting the data. Currently available methods also suffer from lapses in conduction in high pulsatility environments or when the intracranial temperature exceeds 39.5°C, further interrupting the continuity of measurements. Ranges of CBF considered normal also varied between studies, but generally hovered around a lower threshold of 20–40 mL/100 g/min and upper threshold of 70–100 mL/100 g/min depending on whether the technique was cortical- or parenchymal-based. Methods used to increase CBF included expanding plasma volume, inotropic support, and osmotic agents. Interventions used to lower CBF included hyperventilation and barbiturate coma.
Functional outcome studies
Functional outcome was most commonly reported using the GOS or GOS-E at 3 months, 6 months, or at an unspecified interval. 11,15,16,19,22,24,25,27,30 That said, 2 studies only report mortality at an unspecified interval 10,14 and 15 studies do not report any functional outcome measure in relation to CBF parameters. 11,13,15,17 –21,23,26,28,33,34 Table 2 summarizes the studies on TDF and association with global patient outcome.
TDF-rCBF and Patient Functional Outcomes
ACA, anterior cerebral artery; CBF, cerebral blood flow; CO2, carbon dioxide; CPP, cerebral perfusion pressure; CPPopt, optimal cerebral perfusion pressure; CSF, cerebrospinal fluid; DC, decompressive craniectomy; GOS, Glasgow Outcome Scale; GOS-E, extended Glasgow Outcome Scale; MCA, middle cerebral artery; PaCO2, arterial partial pressure of carbon dioxide; PRx, pressure reactivity index; rCBF, regional cerebral blood flow; TDF, thermal diffusion flowmetry.
An association between a sustained reduction in CBF below 20 mL/100 g/min and increased mortality was seen across a number of studies. 14,22,29,30 Conversely, hyperemia—defined as CBF greater than 80–100 mL/100 g/min—was generally associated with a poor outcome. 14,27,29 For patients with regional (r)CBF values predominantly falling within the normal range, 3 studies saw higher average CBF in the favorable outcome group (46.8 vs. 32.2 mL/100 g/min 16 ; 55 vs. 48 mL/100 g/min 22,27 ). One study reported significantly lower CBF in patients with a good outcome compared with poor outcome (17 vs. 29 mL/100 g/min), 31 but the authors do not describe the functional outcome evaluation that was used. One study did not observe a difference between the proportion of patients with normal CBF in those who survived after a decompressive craniectomy for refractory intracranial hypertension and those who had a fatal outcome. 10 In one patient, a consistent reduction in rCBF correlated with severe ipsilateral anterior cerebral artery (ACA) and middle cerebral artery (MCA) vasospasm leading to a hemispheric infarct and a vegetative outcome. 14
Neurophysiological outcome studies
Various measured neurophysiological variables were correlated with continuously measured CBF via TDF, including: intracranial pressure (ICP), cerebral perfusion pressure (CPP), PbtO2, and cerebrovascular reactivity. Table 3 details the studies assessing the association between TDF-based CBF and neurophysiological measures.
Association between TDF-rCBF and Other Neurophysiological Measures
AVDO2, arterio-venous difference in oxygen; BIS, bispectral index; CBF, cerebral blood flow; CBFx, cerebral blood flow index; CBFx-CPPopt, cerebral-blood-flow-index-based optimal cerebral perfusion pressure; CI, cerebral compliance; CO, cerebral oximetry; CO2, carbon dioxide; COx-CPPopt, cerebral-oximetry-based optimal cerebral perfusion pressure; CPP, cerebral perfusion pressure; CPPopt, optimal cerebral perfusion pressure; CSD, cortical spreading depression; CVR, cerebrovascular resistance; DC, decompressive craneictomy; ECoG, electrocorticography; ETCO2, end-tidal carbon dioxide; ICP, intracranial pressure; MAP, mean arterial pressure; ORxs, short oxygen reactivity index; ORxs-CPP, short-oxygen-reactivity-index-based optimal cerebral perfusion pressure; PaCO2, arterial partial pressure of carbon dioxide; PAx, pulse amplitude index; PbtO2, brain tissue oxygen tension; PRx, pressure reactivity index; PRx-CPPopt, pressure-reactivity-index-based optimal cerebral perfusion pressure; PVI, pressure-volume index; rCBF, regional cerebral blood flow; SjVO2, jugular venous oxygen saturation; sXE-CT, stable xenon-enhanced computed tomography; sXE-CT CBF, cerebral blood flow measured by sXE-CT method; sXE-CT rCBF, regional cerebral blood flow measured by sXE-CT method; TD, thermal diffusion; TD-CBF, cerebral blood flow measured by thermal diffusion; v-a(CO2), venous-arterial difference in carbon dioxide.
TDF-CBF association with ICP
A number of studies found an association between high ICPs and either significantly reduced CBF or hyperemia. 14,22,24,29 Five studies describe a relationship between high ICPs and hyperemic CBF patterns. 11,14,22,27,29 In those patients, hyperemia tended to precede the development of increased ICP by a few hours. 12,14 One study reported a positive correlation between CBF and ICP (r = 0.370, p < 0.01) even within the normal range. 30 A negative association between CBF and ICP was seen in 3 studies. 13,14,22 One study reported a negative association across the entire range of CBF values, whereas in the other 3 studies the inverse correlation was seen at CBF values below the ischemic threshold. 14,22,27 In one study, improvement of ICP after hypertonic saline (HTS) bolus was preceded by a mean increase in CBF. 13
One study reported a positive correlation between delta-focal-ICP and delta fCBF within individual patients, but no clear correlation between the two parameters when looking at the overall study population. 34
TDF-CBF association CPP
One study describes optimal CBF patterns when CPP was in the 75–80 mm Hg range and CBF was consistently below the ischemic threshold when CPP was less than 50 mm Hg. 24 Another study saw no significant fluctuation in CBF with changes in CPP in less severely injured patients, although more severely injured patients demonstrated changes in CBF that correlated closely with instantaneous changes in perfusion pressure, suggesting disturbances in autoregulatory mechanisms. 18
TDF-CBF association with PbtO2
Of the studies that explored the relationship between CBF and PbtO2, most found a positive correlation between the two variables. 17,19,23 A reduction in CBF induced by hyperventilation in one study was associated with a concomitant reduction in regional PbtO2. 23 Multi-variate analysis in another study showed a strong association between brain tissue oxygen tension and the product of CBF and arteriojugular venous difference of oxygen (AVDO2; p < 0.001). 19 No studies reported a negative association between CBF and PbtO2. A poor overall correlation between CBF and PbtO2 is reported by Garcia-Perez and colleagues, 30 but their study lacked statistical power with only 5 subjects.
TDF-CBF association with cerebrovascular reactivity
In one study looking at a CBF-based vascular reactivity index (CBFx), the percentage of time when vascular reactivity was preserved and CBF exceeded the ischemic threshold was maximized in the 75–80 mm Hg CPP range for the overall patient population, with individual optimal CPP (CPPopt) ranging from 60 to 100 mm Hg. 24 As described above, Krasberg and associates 18 observed a close relationship between changes in CBF and instantaneous changes in CPP only in the most severely injured members of their cohort, presumably because of a failure of autoregulation. Lastly, vascular reactivity as measured by pressure reactivity index (PRx) and CBFx showed a slight improvement on average after a hypertonic saline bolus and this was associated with a mean increase in CBF. 13
TDF-CBF association with other CBF measures
Changes in regional CBF measured by TDF correlated with changes in global CBF determined via the Kety-Schmidt technique in one study (regression slope = 0.636). 15 One study comparing CBF values obtained via TDF and stable Xe-rCBF (sXe-rCBF) found a good correlation between the two techniques (r = 0.89, p < 0.0001), 26 whereas a similar study found no significant correlation between TDF measurements and sXe-CT CBF data from 2-cm and 3- to 5-mm regions of interests adjacent to the TD probe. 21
Complications of TDF
Eleven studies totalling 214 patients commented on complications observed during TDF monitoring. 14 –16,19,21,22,24,26 –29 Of those, 7 reported no probe-related complications. 14 –16,19,24,26 –28 The overall complication rate—excluding studies that failed to disclose adverse events—was 3.7% (8/214), most of which were of infectious nature. Four patients developed a cerebrospinal fluid (CSF) leak around the probe 21,29 ; which led to meningitis in one case 21 ; one patient developed an intracerebral abscess requiring surgical management 21 ; and three patients developed a superficial soft-tissue infection at the scalp exit site. 22 There were no clinically significant intracranial hemorrhages related to probe insertion.
Risk of bias
Risk of bias in individual studies was assessed via the RTI item bank. Overall, all studies were deemed at high risk for bias given their observational nature, relatively small size, and lack of reporting regarding concurrent interventions. A table summarizing individual risks of bias for different bias domains derived from the RTI questionnaire can be found in Supplementary Appendix C. Meeting abstracts in particular were considered to have very high risk of bias for most of these domains.
Discussion
This scoping systematic review of cerebral TDF summarized all the major available studies documenting the relationship between TDF-rCBF measurements, patient functional outcome (11 studies), and neurophysiological parameters (25 studies). Although the relatively small scale and heterogeneity of the included studies make it difficult to draw robust conclusions, a few consistent findings emerged through our synthesis of the evidence. With respect to TDF-rCBF and functional outcome, a sustained reduction in rCBF and hyperemia were both consistently associated with a poor outcome. Similarly, very low initial rCBF was predictive of catastrophic neurological outcome or progression to brain death. On the other hand, the relationship between TDF-rCBF and functional outcome remains unclear for patients who tended to stay within the normal perfusion range. Importantly, more than half of the studies included did not comment on the link between rCBF and functional outcome. Of those who did, intervals for outcome measurement and type of outcome scale used were very inconsistent between studies, highlighting the need for more concerted research efforts to elucidate the predictive value of this technique. As for relationships between TDF-rCBF and other neurophysiological parameters, very low or very high rCBF dependably correlated with intracranial hypertension. A positive correlation between changes in rCBF and PbtO2 was also observed across a number of studies. This is in line with findings from an Xe-CT CBF study showing a significant correlation between regional blood flow and brain tissue oxygenation. 35 Unfortunately, there are too few studies reporting on associations with other neurophysiological variables such as autoregulation indices, cerebral microdialysis analytes, and global CBF measures to draw meaningful conclusions in these domains. The technique does appear to be well tolerated with an overall complication rate of 3.7%, which is comparable to other invasive neuromonitoring techniques. 36,37
An important factor identified from the available literature is that TDF-based continuous CBF monitoring has really only been employed in the experimental setting and has yet to receive widespread adoption. Prior issues with the technique have been identified, including the need for repeated zeroing of the device when in situ. 38 Further, the invasive nature of both parenchymal and subdural probes may dissuade clinicians from placement in patients already requiring multiple invasive monitoring devices. In general, this scoping review confirms that much more prospective work is needed to determine the exact role—if any—that TDF devices should play in the multi-modal monitoring of critically ill patients.
First steps for future work should focus on better characterizing the association between continuously measured CBF from TDF methods, continuous brain tissue oxygenation, and validated measures of cerebrovascular reactivity. Such analysis should focus on high-frequency time-series relationships to determine the degree of correlation between these three variables under high temporal resolution windows. In addition, such relationships should be interrogated through dynamic physiological challenges (through CO2, mean arterial pressure [MAP], or ICP manipulation). These type of analyses would help determine if any complementary information is added by directly monitoring CBF, as it is currently unclear how much explained variance in prediction models is added when introducing additional CBF measures on top of CPP, which is the surrogate used by most centers today.
From here, if such analysis confirms added information from CBF monitoring, larger multi-center work should be conducted to assess the added value of such monitoring in terms of both coarse global outcome prediction and more detailed neuropsychiatric/functional outcome measures at various time-points post-injury, including longer-term assessments up to and beyond 12 months. Such outcome analysis should also include acute and long-term high-resolution MRI to assess the association between changes in TDF-based CBF and lesion progression as well as long-term cortical atrophy and connectivity via diffusion tractography. Surrogate markers of tissue outcome, such as protein markers of brain tissue fate, could also be used to see if the extent of affected tissue is associated with abnormal rCBF as measured with TDF. 39 It is through such an integrated approach that we should be able to begin to understand the role of such monitoring in adult TBI care.
Limitations
This review suffers from a number of limitations that primarily arise from heterogeneity in outcome reporting and high risk of bias in the included studies. All of the studies are relatively small, of observational nature, and often had a primary focus that was not well aligned to our primary and secondary research questions. A quantitative synthesis of the evidence via a meta-analysis was also not possible given the lack of common outcome measures.
Further, the majority of studies do not adequately report on possible confounding effects from concurrent interventions or on the influence of medical and surgical therapies on CBF measurements. Without this information, we could not comment on the impact of CBF-directed therapy on outcome. Of the 9 articles that reported functional outcome measures, only 2 superficially discuss the relationship between CBF response to intervention and patient outcome. Lee and colleagues 27 describe how 4 patients with high ICP and ischemia who responded well to osmotherapy were noted to have a good outcome. They also reported that for patients with an initial CBF lower than 20mL/100 g/min, intravascular volume expansion did not improve CBF and these patients universally had a poor outcome. However, the small number of patients and lack of information with respect to what was considered a positive “response” in terms of CBF values makes it difficult to draw meaningful conclusions.
In a pilot study investigating the value of CPPopt-guided therapy, Dias and colleagues 12 reported that patients with larger discrepancy between real CPP and CPPopt were more likely to have an adverse outcome. However, these conclusions are drawn from a PRx-derived CPPopt. Although they describe a reasonably good agreement between PRx-CPPopt and optimal CPP calculated by other cerebrovascular reactivity indices including CBFx-CPPopt, they do not discuss the impact of their interventions on CBF values and the direct relationship between CBFx-CPPopt and GOS.
Another critical limitation is the variability in probe placement between studies, which confounds comparisons of rCBF measurements. rCBF values are likely greatly influenced by positioning of the probe tip in healthy versus lesional or perilesional tissue. Whereas most studies targeted non-lesioned cerebral tissue, 3 studies targeted perilesional parenchyma, which has been shown to have aberrant flow patterns on Xe-CT studies. 40 There was also an uneven distribution of studies using cortical versus parenchymal-based technique, further limiting cross-study comparisons of absolute rCBF values. Establishing reliable thresholds of abnormal rCBF requiring intervention will benefit from a more systematic framework for probe placement commensurate with the clinical scenario.
Conclusion
Despite being based on a relatively weak body of evidence, the available literature suggests a link between consistently abnormal TDF-rCBF values, intracranial hypertension, and poor functional outcome. TDF-rCBF also appears to correlate well with regional measurements of brain tissue oxygenation. Currently, such monitoring should be considered experimental, requiring much further evaluation prior to widespread adoption.
Footnotes
Acknowledgments
FAZ has received salary support for dedicated research time, during which this project was completed. Such salary support came from: the Cambridge Commonwealth Trust Scholarship and the University of Manitoba Clinician Investigator Program. FAZ's research program is supported through the University of Manitoba Thorlakson Chair in Surgical Research Establishment Fund. EPT received post-doctoral grants from the Swedish Society for Medical Research. FM has received salary support for dedicated research time from the Canada Cambridge Scholarship sponsored by the Cambridge Commonwealth Trust.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Appendices A–C
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.