
Abstract
The number of systematic reviews on the effects of exercise on aerobic fitness and muscle strength in people with spinal cord injury (SCI) has recently increased. However, the results of some of these reviews are inconclusive or inconsistent. To strengthen recommendations, this overview was undertaken to assimilate evidence about the effectiveness of different types of physical activities, exercises, and therapeutic interventions for improving aerobic fitness and muscle strength in people with SCI. Cochrane Overview of reviews methods were adopted to undertake this overview. An online search was conducted in August 2018 on eight databases based on predefined search criteria. Potential systematic reviews were screened, selected, and assessed on methodological quality by two independent authors, and discussed and resolved with a third author, when necessary. Only systematic reviews published in the English language were included. The protocol was registered on PROSPERO. Overall, 16 systematic reviews were included (aerobic fitness, n = 10; muscle strength, n = 15). For all 16 reviews, the quality of evidence was rated as “critically low.” Despite low evidence, this overview strengthens the existing guidelines for people with SCI, providing specific advice on exercise domains (types, intensities, frequency, and duration) for improving aerobic fitness and muscle strength. The evidence from this overview suggests that ergometry training with/without additional therapeutic interventions (20 min, moderate to vigorous intensity, twice weekly for 6 weeks) may improve aerobic fitness; similarly, resistance training with/without additional therapeutic interventions (three sets of 8–10 repetitions, moderate to vigorous intensity, twice weekly for 6 weeks) may improve muscle strength.
Introduction
Spinal cord injury (SCI) resulting from trauma or disease leads to muscle paralysis (or paresis), loss of sensation, and autonomic dysfunction below the level of injury. Secondary medical complications commonly occur following SCI and frequently include urinary tract infections, spasticity, hypotension, autonomic dysreflexia, and pressure sores. 1 Loss of lower limb function and reliance on wheelchair mobility may lead to various negative sequelae, including lower physical fitness, poor endurance, diminished physical strength, loss of bone mass, and a predisposition toward developing obesity, diabetes, and cardiovascular diseases. 2 –5
For people with SCI to attain an optimum level of functioning in the community and reduce the risk of secondary complication, an active lifestyle with participation in regular leisure-time physical activity and/or structured exercises is advisable. 6 The available literature suggests that increased physical activity and exercise can promote well-being and psychological benefits 7 –9 as well as improve health-related quality of life. 4,10,11 People with SCI who regularly participate in increased physical activity or exercise programs have been shown to have a lower risk of developing chronic diseases when compared with people with SCI who possess a sedentary lifestyle. 12 –14 A recently published guideline has recommended a minimum of 2 days per week of moderate to vigorous intensity of 20 min of aerobic exercise and three sets of 8–10 repetitions of strengthening exercise for every major functioning muscle group to improve cardiorespiratory fitness and muscle strength in people with SCI. 15
The literature investigating the effects of exercise on aerobic fitness and muscle strength in people with SCI has grown in recent years. 15 Health care practitioners rely on updated systematic reviews to inform evidence-based practice. 16 However, basing clinical practice on the results of a single systematic review can engender some risks. Among various systematic reviews, the approaches to quality assessment may vary 17,18,and the aims, outcomes, interventions, and population can overlap, leading to conflicting findings that may confound health care practitioners who wish to implement “best clinical practice.” 19 An overview of systematic reviews is a research design that aims to support clinical decision-making by synthesizing the findings and critically appraising the quality of published systematic reviews that address the effects of two or more interventions for a single condition or health problem. 17 Therefore, the present overview of systematic reviews will determine the effectiveness of different types of physical activities, exercises, and therapeutic interventions for improving aerobic fitness and muscle strength in people with SCI.
Methods
Study design, protocol, and registration
This study adopted the framework and processes for conducting an appraisal of systematic reviews established by the Cochrane Overview of reviews. 17,19 The protocol of this study was registered on PROSPERO in 2017 (registration ID: CRD42017079923).
Search methods for identification of reviews/Search strategy
Eight databases including the Cochrane Library (inception–2018), MEDLINE (1946–2018), EMBASE (1947–2018), AMED (1985–2018), CINAHL (1982–2018), SPORTDiscuss (1975–2018), SCOPUS (1969–2018), and Web of Science (1974–2018) were searched. The language of reviews was restricted to English. Empirical studies have shown no overall differences in retrieved studies when reviews in languages other than English have been included. 20 The most recent search was conducted during August 2018. Search terms included the combination of words, phrases, and Medical Subject Headings (MeSH) as follows: spinal cord injury, quadriplegia, paraplegia, exercise, exercise therapy, resistance training, electrical stimulation therapy, cardiovascular fitness, physical fitness, exercise test, muscle strength, review, and meta-analysis. A full search strategy is provided in Supplementary Appendix S1.
Criteria for inclusion
The predetermined criteria for including the relevant systematic reviews in the current overview is shown in Table 1. The PICO framework (Participants, Interventions, Comparison, and Outcomes) was adopted. 21 All published systematic reviews with the same research questions were included. When a systematic review was updated after earlier publication, the most recent version was included herein.
Selection Criteria
Participants
Eligible systematic reviews included adults over the age of 16 years who were diagnosed as having SCI of traumatic or non-traumatic etiology, at all levels (paraplegia and quadriplegia) and severity of injury (complete and incomplete).
Interventions
Systematic reviews that included primary studies, which evaluated one (or a combination) of physical activity, exercise, and/or physical therapeutic interventions were included in this overview.
Physical activity interventions were defined as bodily movements undertaken for health or enjoyment, but excluding occupational tasks. 22
Exercise was defined as movements of the body evoked by skeletal muscle contractions that resulted in levels of energy expenditure in a structured time and/or venue, but not including occupational tasks. 5
Physical therapeutic interventions referred to all physical interventions or training prescribed by a therapist that may have involved the use of electrical stimulation, repetitive task-training, robotic-assisted training, and/or other therapeutic modalities during structured activities in a clinical setting. 23
Comparisons
Reviews with findings that compared interventions and outcomes from two or more primary studies were included.
Outcomes
Reviews that investigated quantifiable changes in aerobic fitness and/or muscle strength were included.
Aerobic fitness was defined as the capacity of heart and lungs to provide oxygen to the muscles where it could be consumed during physical exertion. A change of aerobic fitness following an intervention could be an increase in peak oxygen uptake (VO2peak), a decrease of submaximal-intensity oxygen consumption at a same or higher work intensity, a decrease of submaximal heart rate at a same or higher work intensity, or other proxies of the performance of the cardiorespiratory system such as augmented work output or higher power output. 24,25
Muscle strength was defined as the ability of a group of muscles (or a single muscle) to produce resistance or movement against an external force during a muscle contraction. One-repetition maximum (1-RM), manual muscle tests, and other proxies of augmented muscle performance, or laboratory tests including magnetic resonance imaging (MRI) scans quantifying changes of muscle circumference/volume or muscle biopsies assessing altered histomorphology of muscle were accepted. 25,26
Design
To be included in this overview, reviews must have been clearly declared as being a systematic review of two or more interventional studies with quantitative findings. The review methodology must have provided information about the comprehensive search from multiple sources, search strategy, selection criteria, assessment of study quality, and the methods for critical appraisal of included studies.
Further, the included reviews must have described the characteristics of the primary studies reports, scores for methodological quality, and/or descriptive statistics that could include but not be limited to effect sizes and 95% confidence intervals from meta-analyses, or similar statistical treatments.
Data collection and analysis
Selection of reviews
Two authors (AE and CQO) independently screened the titles and abstracts of the search output according to the predetermined criteria shown in Table 1. Any disagreement or ambiguity between authors was resolved by consensus after discussion with a third author (GMD). All disagreements were recorded for later evaluation. Ultimately, full texts of potential systematic reviews were evaluated for inclusion. Reference lists and relevant “gray” literature from the Spinal Cord Injury Research Evidence (SCIRE) database were manually searched to identify any further relevant studies.
Data extraction and management
A data extraction form was developed based on the Cochrane Handbook for Systematic Review of Interventions comprising “Characteristics of included studies,” “Number of relevant studies,” and “Summary of findings.” 17 The data were extracted independently by two authors (AE and CQO), and any disagreement was resolved by consensus with the third author (GMD). Numbers of disagreements were recorded. Any unclear or missing information that was identified from the included systematic reviews was noted and resolved by contacting (via e-mail) the corresponding author of the publication for further clarification.
Assessment of methodological quality of included reviews
Quality of included reviews
The methodological quality of the included systematic reviews was assessed using A Measurement Tool to Assess Systematic Reviews, version 2 (AMSTAR 2). 27 AMSTAR 2 was developed to appraise systematic reviews of health care interventions, including the domain of flaws of a study due to the uncertain or poor conduction of the review. It describes any risk of bias as detailed in the Cochrane risk of bias for non-randomized and randomized control trials guidelines. 28 Two authors (AE and CQO) independently rated the quality of the included systematic reviews using AMSTAR 2. Any disagreements were recorded and resolved by consulting the third author (GMD).
Quality of evidence in included reviews
The included systematic reviews were summarized based on the agreement or conflicting results between individual findings. Additionally, to determine the quality of the evidence, the methodological quality of the primary studies scored by the included reviews were extracted and summarized.
Data synthesis
The extracted data from included systematic reviews were collected and presented using a narrative approach. Reporting of results were presented as follow: author(s) and year of publication, the research questions of the reviews regarding their PICO statement, the aims of the reviews, and the findings and conclusions about aerobic fitness and muscle strength outcomes.
Results
A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart of the search strategy is presented in Figure 1. The initial database search revealed 656 potentially relevant titles. After duplicate articles were removed, 535 titles and abstracts were screened. A total of 39 full texts were assessed. Then, a further 23 articles were excluded (Supplementary Appendix S2). The remaining 16 systematic reviews 7,29 –43 met the inclusion criteria and were included in this overview of systematic reviews with 94.9% agreement among the independent authors. No additional systematic reviews was retrieved from the search of reference lists of a selected article or from the gray literature.
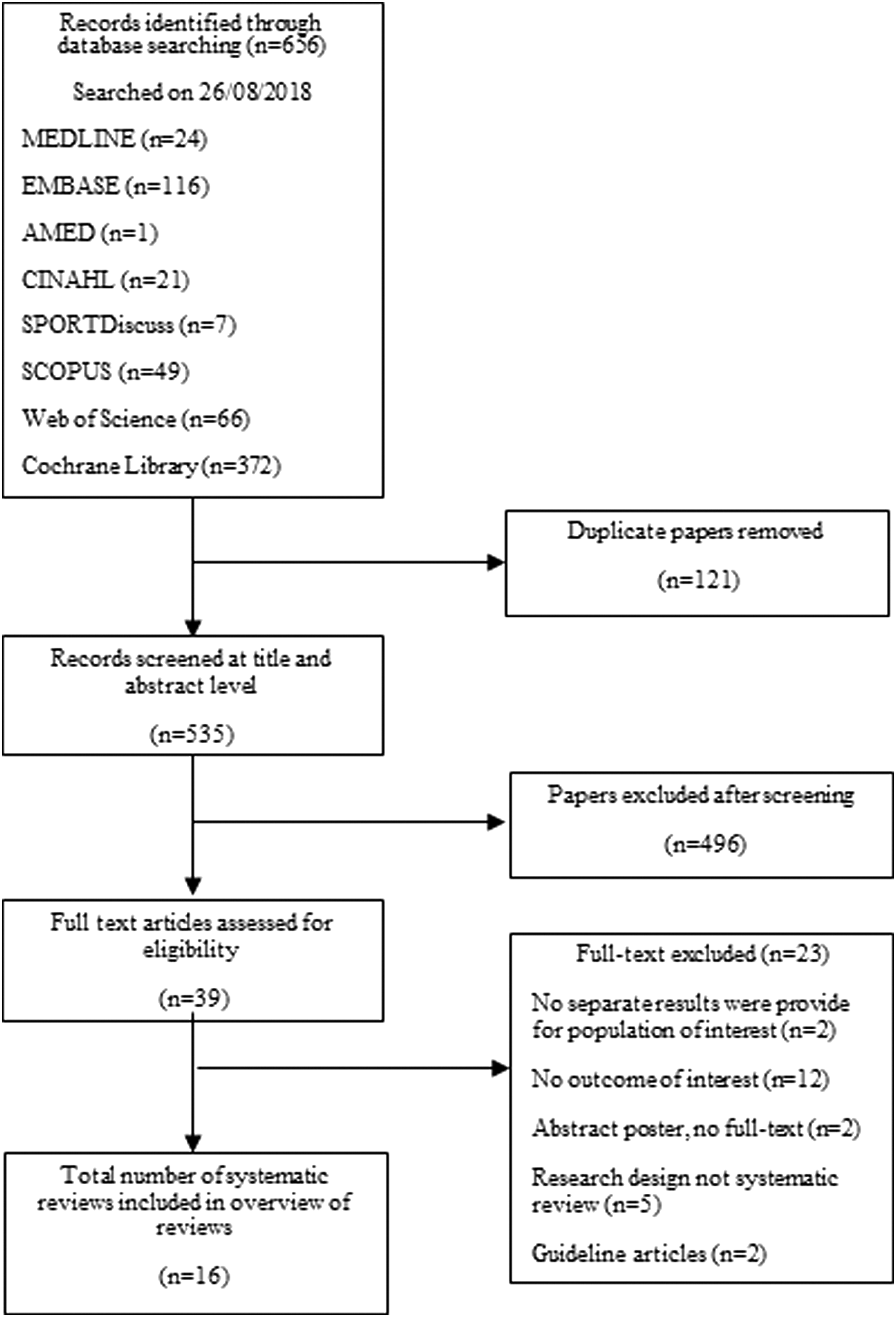
Flowchart of studies through the review.
Description of included reviews
The characteristics of the 16 included systematic reviews are summarized in Table 2. The findings on aerobic fitness and muscle strength are summarized in Tables 3 and 4, respectively.
Characteristics of Systematic Reviews
This information was not adequately described in the Methods section; therefore it was extracted from the Results section.
ARAT, Action Research Arm Test; D&B, Downs and Black Checklist; ES, electrical stimulation; FES, functional electrical stimulation; GRASSP, Graded Redefined Assessment of Strength, Sensibility and Prehension; LEMS, lower extremity motor scores; N, number of studies included in the systematic review; NMES, neuromuscular electrical stimulation; n/a, not applicable; nAF, number of studies with participants with SCI and aerobic fitness outcomes; nMS, number of studies with participants with SCI and muscle strength outcomes; nSCI, number of studies with participants with SCI included in the systematic review; MMT, manual muscle test; PEDro, Physiotherapy Evidence Database; PO, power output; PPO, peak power output; QoL, quality of life; RAGT, robot-assisted gait training; RCT, randomized controlled trials; SCI, spinal cord injury; VO2max, maximum oxygen consumption; WISCI, Walking Index for Spinal Cord Injury.
Summary of Findings on Aerobic Fitness
+, reported conclusive positive result; ?, reported inconclusive result; BWSTT, body-weight support treadmill training; CI, confidence interval; D&B: Downs and Black Checklist; FER, forced expiratory ratio; FES, functional electrical stimulation; FEV1, forced expiratory volume in 1 sec; FVC, forced vital capacity; HR, heart rate; HRpeak; peak heart rate, PEDro, Physiotherapy Evidence Database; Rest HR, resting heart rate; RCT, random controlled trial; SCI, spinal cord injury; VO2max, maximal oxygen consumption; VO2peak, peak oxygen uptake.
Summary of Findings on Muscle Strength
+, reported conclusive positive result; ?, reported inconclusive result; 1 RM, one-repetition maximum; ASIA motor score, American Spinal Injury Association-International Standards for Neurological Classification of Spinal Cord Injury; BWSTT, body-weight support treadmill training; CI, confidence interval; D&B, Downs and Black Checklist; ES, electrical stimulation; FES, functional electrical stimulation; NMS, neuromuscular stimulation; Nm, Newton-metro; MMT, manual muscle test; PEDro, Physiotherapy Evidence Database; RCT, randomized controlled trial; SCI, spinal cord injury.
Fifteen out of 16 reviews clearly stated that their aim was to investigate treatment effectiveness of an intervention in an SCI population. Three reviews only included cohorts with cervical SCI, 34,36,37 and one review included people with different neurological conditions (including spinal bifida, stroke, cerebral palsy, peripheral nerve lesion, and multiple sclerosis). 31
The interventions varied among reviews, with six reviews including specific interventions or modalities such as combined aerobic and strength training, 29 robotic-assisted body-weight support training, 30,43 transcutaneous neuromuscular electrical stimulation, 31,42 and aquatic exercise. 35 Ten reviews did not specify the type of exercise interventions investigated in their method section, but such information was extracted from the result section of the articles.
Aerobic fitness was investigated in 10 reviews. 7,29 –40 These systematic reviews included a number of primary studies, ranging from 1 to 95. Muscle strength was investigated in 15 reviews. 7,29 –39,41 –43 These systematic reviews included a number of primary studies, ranging from 2 to 75. These studies have sample sizes between 12 and 1600 subjects with SCI across all included primary studies.
Meta-analysis was performed in five reviews 30 –33,43 for muscle strength training (Table 3). Out of these five reviews, three reviews 30,33,43 performed meta-analysis on effects of interventions on an SCI population. One review included a mixed population (i.e., SCI, stroke, spina bifida, cerebral palsy, etc.), but only provided summary results of the therapeutic interventions without meta-analysis on muscle strength outcomes in people with SCI and was therefore included. 31 One other review included an SCI population with an outcome of interest but had not performed meta-analysis for that outcome. 32 Only one review 33 performed meta-analysis on effects of interventions on aerobic fitness training on an SCI population (Table 4).
The included reviews used different tools to assess methodological quality: the Physiotherapy Evidence Database (PEDro) scale 44 (n = 9[7,29,31 –33,39,40,42,43]), a Downs and Black Checklist 45 (n = 5[7,35,36,39,40]), van Tulder's Quality Assessment Scale 46 (n = 2[37,38]), the Jovell and Navarro-Rubio classification of study designs 47 (n = 1[34]), and the Cochrane risk of bias assessment tool 48 (n = 1 30 ). Moreover, three reviews 7,39,40 adopted additional level-based ratings or confidence rating systems to categorize the level of evidence. Two reviews 7,39 applied SCIRE 49 (see Supplementary Appendix S3). One review 40 used Sackett's levels of evidence 50 to categorize the overall quality of its included studies. Finally, three reviews 33,39,41 used the Grading of Recommendations Assessment, Development, and Evaluation (GRADE), 51 as proposed by the Cochrane Review Group. 17
Methodological quality of included reviews
Quality of included reviews
Details of AMSTAR 2 assessment of methodological quality are presented in Table 5. The two primary authors (AE and CQO) agreed with more than 90% of the AMSTAR 2 ratings across the 16 systematic reviews. Based on AMSTAR 2, the quality of all included reviews was considered “critically low,” because all contained more than one critical flaw (see Table 5 on AMSTAR 2 criteria with “a”) with several non-critical flaws (see Table 5 on AMSTAR 2 criteria without “*”).
AMSTAR 2 Assessment of Methodological Quality of Systematic Reviews
Multiple non-critical weaknesses may reduce confidence within the review, leading to appropriately lower overall appraisal down from moderate to low confidence.
AMSTAR 2 critical domains.
N, no; n/a, not applicable; NM, no meta-analysis performed regarding the participants and/or outcomes of interest; NRSI, non-randomized studies of interventions; P, partially yes; RCT, randomized control trial; RoB, risk of bias; Y, yes.
The most common critical flaw in the included systematic reviews was the absence of information about publication bias (either graphical representation or statistics) and the likelihood and magnitude of its impact on quality of evidence (Item 15). Almost all included reviews had at least two reviewers independently agree on study selection and achieved consensus on inclusion (Item 5). 7,29 –37,39,42,43 In addition, most studies used an appropriate tool to assess the quality of included studies and risk of bias (Item 9, which is rated separately from publication bias), 7,29 –33,35 –43 as well as provided a discussion of the impact of risk of bias on the results (Item 13). 30 –43 Half of the included reviews failed to provide an adequate and clear description of participants and intervention in the Methods section but the information was extracted from the Results section of the review (Item 1). 7,29,34,35,37,38,40,41 Similarly, nearly half of the reviews failed to provide comprehensive information of their PICO components in their Methods section (Item 8) 7,31,34,37,38,40 or potential sources of conflict of interest (Item 16). 30 –32,34,35,37,42 Five reviews provided a list of excluded studies along with the justification for the exclusion (Item 7) 30,31,34,38,41 and discussed sources of heterogeneity (Item 14). 32,33,36 –38 Five reviews 34,36,38,40,41 did not report either how a consensus was reached between authors or the agreement rate when performing the data extraction (Item 6). Only a few reviews successfully explained their study designs of interest (Item 3), 32,38,41 or provided a comprehensive literature search strategy (Item 4). 29,43 Out of the reviews 30,33,43 that performed meta-analyses, one 43 reported the possible causes of heterogeneity (Item 11) or analyzed the possible impact of risk of bias on summary estimates of effect (Item 12). Only two reviews 42,43 reported having partial a protocol statement or written protocol before conducting the review (Item 2), and one review 41 reported the source of funding for the included primary studies (Item 10).
Authors of included reviews were contacted when data were unavailable for the included review. Three authors 30,35,42 replied with the requested information, five authors 7,29,31,38,39 reported being unable to provide data or no longer having access to the files, six authors 32,33,36,40,41,43 did not reply, and two corresponding authors 34,37 were not able to be contacted.
It was decided not to conduct meta-analyses on either of the two outcomes in this overview due to a lack of additional information being available and to avoid any duplication. In one meta-analysis, 33 the information about the outcome for aerobic fitness was not provided and the corresponding author was contacted to obtain additional information and clarification about whether the outcome for aerobic fitness was VO2peak. In addition, the same author also indicated that a meta-analysis of the effect of exercise training on muscle strength outcomes in people with SCI has been undertaken and is currently under review.
Quality of evidence in included reviews
Each review reported that the primary studies included were mostly rated as having poor-to-moderate quality (see Tables 2 –4 for details).
Effect of interventions
Table 3 and Table 4 summarize the finding across included reviews in this overview.
Exercise training for aerobic fitness
Four reviews 7,33,39,40 reported conclusive findings regarding the positive effects of exercise interventions to improve aerobic fitness. The interventions that significantly improved aerobic fitness in adults with chronic SCI were: arm ergometry training alone (arm cranking), combined arm ergometry with leg functional electrical stimulation (FES), combined arm ergometry with resistance training, arm-hand cycling training, resistance training alone, and wheelchair ergometry/propulsion training. Only two reviews 7,39 reported on the effects of aerobic fitness interventions for people with acute SCI.
The following interventions for improving aerobic fitness were deemed inconclusive: body-weight supported treadmill training (BWSTT), 39,40 robotic-assisted BWSTT, 30 and aquatic therapy. 35
Exercise training for muscle strength
Seven reviews 7,30,34,36,37,39,43 reported conclusive findings regarding the efficacy of exercise interventions on muscle strength increases for people with chronic SCI. The interventions that significantly improved muscle strength were: resistance training alone or in combinationwith the additional training (e.g., arm ergometry, FES, or BWSTT), robot-assisted BWSTT and arm training (e.g., kayak and rowing ergometry). Four reviews 7,30,39,43 reported low confidence on the effect of interventions on muscle strength in people with acute SCI.
Eight reviews 29,31 –33,35,38,41,42 were inconclusive or were affected by the poor quality of included primary studies, insufficient data, or variations of test methodologies and target muscle groups of interest.
Discussion
This overview of systematic reviews achieved its aim of identifying points of agreement among the existing systematic reviews' results from 16 systematic reviews that summarized the effectiveness of physical interventions on aerobic fitness and muscle strength for people with SCI. Exercise is essential for lifelong health maintenance after SCI. Since the introduction of new technologies,such as FES and robotic-assisted devices, the scope of SCI rehabilitation has shifted solely from exercising the remaining muscle groups under voluntary control to a more comprehensive whole-body approach using novel therapeutic equipment and new modalities of exercise. 52 However, most physical activity, exercise, or rehabilitation interventions for SCI have relied on poor-to-moderate quality randomized controlled trials or non-controlled research with a high risk of bias.
Summary of outcomes of interest
This overview included 16 reviews; 10 reporting results for aerobic fitness outcomes and 15 for muscle strength outcomes involving a range of interventions. However, not all reviews were conclusive.
Aerobic fitness
From the 10 included reviews, 4 presented conclusive findings that upper-limb aerobic training (using arm ergometry or similar activities) with or without additional therapeutic modalities (e.g., FES or resistance training), improved aerobic fitness. 7,33,39,40
Muscle strength
From the 15 included reviews, 7 presented conclusive findings for muscle strength improvement by conventional training with or without an additional therapeutic modality (such as FES or arm ergometry training). In particular, 3 studies concluded that FES combined with strength training to the major functioning muscles of the upper limbs significantly improved muscle strength. 7,39,53
According to a current physical activity guideline 15 and other systematic reviews 7,33,39,40 for people with SCI, the recommended exercise duration to achieve improvements of aerobic fitness is a minimum of 20 min of moderate- to vigorous-intensity exercise per session, for two (or more) sessions per week, over a minimum of 6 weeks to achieve significant outcomes. Similarly, guidelines for muscle strengthening in people with SCI 15,54 recommend that use of weights and resistance exercises be performed at least twice a week under the supervision of a health care professional, 55,56 and with a resting period of 1 to 2 min between sets. 54 Apart from conventional weight training, this overview also suggested that voluntary arm-ergometry training at moderate to vigorous effort over 30 min 3 times per week may improve upper-body muscle strength in people with SCI. A significant limitation of the published guidelines and systematic reviews is often lack of sufficient detail or clear recommendation about the specific types of interventions and/or related parameters (e.g., duration, frequency, and intensity). This overview integrates evidence for improving aerobic fitness and muscle strength in people with SCI, as well as strengthens our knowledge about specific exercise types and their related parameters. Table 6 provides a summary of direct effects and indirect benefits of aerobic and muscle strengthening on respective outcomes.
Direct Effects and Indirect Benefits of Aerobic and Muscle Strengthening on Respective Outcomes
1 RM, one-repetition maximum; BWSTT, body-weight support treadmill training; FES, functional electrical stimulation; VO2peak, peak oxygen uptake.
Agreements and disagreements with other studies or reviews
To date, the authors are not aware of any other overviews summarizing systematic reviews focussed on the effects of interventions on aerobic fitness and muscle strength in SCI. However, our findings concur with some previous systematic reviews, 39 exercise guidelines, 57,58 and multi-national consensus statements 15 on exercise for people with SCI.
One guideline 15 and one position statement 57 recommended different minimal volumes of aerobic exercise: The guideline 15 recommended a minimal dosage of moderate- to vigorous-intensity exercise for 20 min, twice weekly, whereas the position statement from Exercise and Sport Sciences Australia 57 suggested moderate intensity exercise more than 150 min per week or vigorous-intensity exercise more than 60 min per week. Both reviews recommended muscle strength exercise for 2 days (or more) per week. 15,57 Our findings from the current overview supported that a minimum of twice weekly, 20-min aerobic exercise at a moderate to vigorous intensity will improve aerobic fitness in people with SCI.
In regard to exercise modalities, the current overview proposes that the specific modes of exercises that significantly engender improvements in aerobic fitness are consistently upper-body exercises, such as arm ergometry training alone, combined arm ergometry with leg muscle FES, combined arm ergometry with resistance training, arm-hand cycling training, resistance training alone (>30 min per bout), and wheelchair ergometry/propulsion training. If people with SCI can tolerate high-intensity exercise, vigorous aerobic training can be prescribed because this evokes superior benefits in cardiovascular fitness and is likely more time-efficient. 58 In addition to the current exercise recommendations, this overview found that people with SCI could also expect upper-body muscle strength gains from resistance training alone (50–80% 1-RM, three sets of 8–10 repetitions, 2 times per week), specialized ergometry modalities (e.g., kayak and rowing ergometry), or a combination of arm ergometry and FES leg exercise (moderate to vigorous intensity, 30 min per session, 3 times per week).
A critical difference between this overview of extant systematic reviews and the currently proposed physical activity guidelines is that there was little or no evidence supporting positive outcomes after interventions performed in the home setting, likely due to a paucity of research into home-based exercise. An unwarranted assumption that findings from laboratory-based research or structured exercise in a gymnasium might axiomatically translate into the community and home environments possibly overestimates participants' exercise adherence or their knowledge of the optimal progression of exercise intensity and volume.
Quality of the evidence
The AMSTAR 2 is an updated critical appraisal instrument for systematic reviews that do not generate an overall score. It is possible that this descriptive appraisal may disguise critical weaknesses leading to a reduction of confidence in the results of a systematic review. 27 In this overview, all of the included systematic reviews were rated as having “critically low” confidence under AMSTAR 2. This was because two or more critical domains were identified as absent in each review.
The first absent critical domain (Item 2) was the lack of protocols prior to the reviews. Most of the included reviews did not mention the existence of registered protocols before conducting their systematic reviews. Only one review 43 disclosed a registered protocol. Predefined protocols reduce possible researcher bias. Without a protocol, authors may select individual studies or analyze the information based on personal expectations. 59
The second critical domain (Item 4) absent in almost all reviews was the failure to provide comprehensive details of the literature search. Only two reviews 29,43 provided these details; however, they did so partially. It is recommended that a clear, rigorous unbiased search strategy, keywords, and MeSH be visible to the reader or available upon request to avoid language and selection bias. 59 Another critical domain that reviews failed to provide was the justification for the excluded studies (Item 7). A list of excluded studies along with the reasons for exclusion must be provided to ensure that authors did not selectively recruit only primary studies with positive finding, leading to selective outcome reporting bias. 60 Also, a critical domain relating to statistical meta-analyses (Item 11) could not always be satisfied due to wide variations in the type of interventions and the methods of assessing outcomes of interests. Therefore, reasons for not performing meta-analysis should be clearly stated.
In three reviews 30,33,43 in which a meta-analysis was conducted, a non-critical domain relating to statistical significance of clinical heterogeneity (Item 14) was rarely described, but instead, some reviews used the descriptive discussion to point out any treatment effects. Any type of heterogeneity in meta-analysis can lead to significant statistical diversity, inaccurate summary effects, and therefore, misleading decision-making. 61 The conclusions of the individual systematic reviews need to be interpreted with caution, as these studies may contain false-positive findings (Type 1 error). Also, another non-critical domain was that systematic reviews failed to discuss the source of funding of the primary studies (Item 10), with only one 41 review providing this information. This domain must be reported to minimize research bias by individual or institutional interests that could lead to systematic deviation of research results or inferences from the truth. 62
The quality of the included primary studies in the systematic reviews was moderate to low (level 3 and 4 studies) across 90% of the included reviews. Significant methodological flaws were repeatedly identified in the primary studies concerning physical activity or exercise interventions affecting health status in the population with SCI. Such methodological flaws included baseline differences of the participant with SCI within and between groups, small sample sizes, lack of blinding, lack of reports of dropout rate, and non-intention to treat analyses. Future experimental research for SCI should carefully plan and report finding with details of every aspect of a possible flaw in the study. 63 –66
Overall completeness and limitation of evidence
Due to incomplete reports of the included reviews and the diverse heterogeneity among primary studies, the following issues could affect the “robustness” of the findings in the current overview of systematic reviews.
The available data from primary studies included in the systematic reviews had a wide range of information on participants' baseline health status and a significant variety of outcome measures for aerobic fitness and muscle strength. This heterogeneity may be due to the nature of the SCI literature, wherein participants' recruitment criteria are often highly variable. 49 Insufficient homogenous data in terms of participants, interventions, and types of outcome assessments may explain the reduced number of reviews that conducted a meta-analysis. 17 Moreover, this overview found that most SCI literature was unable to detect differences in the level of physical activity prior to the intervention. Any changes in aerobic fitness or muscle strength after participating in physical activity or exercise programs may not be purely from the interventions. Other activities undertaken by participants were rarely reported and may have affected the results, constituting a source of bias.
Only 10% of the primary studies and five reviews 30,35,37 –39 reported adverse events. The occurrence of some symptoms such as muscle soreness, light headache, or nausea may occur during or after aerobic fitness and muscle strength training. The incidence of adverse events of exercise conducted under the supervision of a health care professional was low, and those that occurred were not serious. 67 Reporting adverse events is fundamental to detecting participants' safety issues. How adverse events are monitored, handled, and analyzed must be clearly stated; however, these were rarely addressed by the authors in their reviews.
Combined interventions (e.g., arm ergometry or resistance training with FES) seemed to deliver the best improvements of aerobic fitness and muscle strength and these relied on close supervision by a therapist/trainer. Specialist resources are required when using combined interventions to monitor the individual, adjust therapeutic equipment, correct exercise techniques, and deliver a progression of the exercise dose and intensity, which may limit its application outside research or clinical settings. 58 Other exercise modalities such as arm ergometry alone or resistance training alone (with conventional weight-training equipment) may be widely available in community gyms or in a home-based setting.
Because high-quality studies on community-based or home-based programs are rare, the evidence in this overview is primarily based on laboratory or clinical interventions. Obvious and challenging questions remain regarding the applicability and acceptability of these interventions outside those highly structured and monitored settings. Further, the accessibility of these physical interventions to a population with SCI living in the community and the transferability of knowledge about exercise prescription from clinical/research practice into community-based and home-based environments remains unclear. Clearly, more research in the community or home-based setting is essential.
Conclusion
Implications for practice
This overview concluded that exercise and muscle strengthening interventions with and without therapuetic modalities (including FES and robotic-assistive training) for people with SCI may promote improved aerobic fitness and muscle strength in clinical practice. However, this suggestion is based on moderate-to-low quality evidence in the primary studies and a “critically low” confidence level in the included systematic reviews (using the AMSTAR 2 tool). A summary of potential intervention types and relevant parameters (e.g., duration, frequency, and intensity) for use in clinical practice is provided in Table 6.
Implications for research
Future systematic reviews need to design, conduct, and report their review based on the guidance provided by the Cochrane Collaboration's handbook and the PRISMA checklist.
Authors also need to use the AMSTAR 2 tool for assessing the quality of the review to minimize potential risk of bias.
Future research should investigate the potential for combining and optimizing different interventions for more effective aerobic fitness and muscle strength outcomes.
It is important to standardize the outcome measures and report between-group differences for all outcomes at all time-points. This will aid interpretation of results, future meta-analyses, and inform recommendations.
In addition, future research could consider the use of an activity tracker or self-reported physical activity to identify compliance and other factors that may influence the outcomes of the exercise interventions.
Footnotes
Acknowledgments
The authors declare that there was no difference between the protocol registered at PROSPERO 2018 (CRD42017079923) and the presented overview of systematic reviews.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Appendix S1
Supplementary Appendix S2
Supplementary Appendix S3
Supplementary References
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.