
Abstract
Traumatic brain injury (TBI) carries a risk of developing post-traumatic epilepsy (PTE). Currently, animal models that replicate clinical PTE (delayed spontaneous and recurrent seizures) are limited, which hinders pre-clinical research. In this study, we used two rat models of penetrating ballistic-like brain injury (PBBI) and closed-head injury (CHI) to induce spontaneous seizures and also measure changes in seizure susceptibility. In the PBBI model, two trajectories (frontal and lateral) and two injury severities for each trajectory, were evaluated. In the CHI model, a single projectile impact to the dorsal/lateral region of the head was tested. Continuous video-electroencephalographic (EEG) recordings were collected for 10 days at 1 or 6 month(s) post-injury. After EEG recording, all rats were given a sub-convulsant dose of pentylenetetrazole (PTZ) to challenge the seizure susceptibility. The video-EEG recording did not detect PTE following the PBBI. Only one CHI rat demonstrated persistent and recurrent non-convulsive seizures detected at 6 months post-injury. However, after PTZ challenge, 50–100% of the animals across different TBI groups experienced seizures. Seizure susceptibility increased over time from 1 to 6 months post-injury across the majority of TBI groups. Injury severity effects were not apparent within the PBBI model, but were evident between PBBI and CHI models. These results demonstrated the difficulties in detecting delayed spontaneous post-traumatic seizures even in a high-risk model of penetrating brain injury. The PTZ-induced increase in seizure susceptibility indicated the existence of vulnerable risk of epileptogenesis following TBI, which may be considered as an alternative research tool for pre-clinical studies of PTE.
Introduction
Advanced medical technology has greatly improved the prognosis of patients who sustain severe traumatic brain injury (TBI), but at the same time has set these patients onto a long journey of rehabilitation. Although motor, cognitive, and psychological impairments are the most common sequela of severe brain trauma, TBI patients also inherit an increased risk of developing post-traumatic seizures. Early seizures occurring during the 1st week of the injury are considered a direct consequence of acute neurological turmoil of TBI and are often referred to as “provoked” seizures. However, in a subpopulation of TBI patients, seizures do not emerge until weeks or even years after the emergent state of TBI recedes. These late seizures, once they have occurred, carry a high risk of recurrence over a long period of time. 1,2 Because of their delayed and chronic nature, these delayed seizures are often referred to as “unprovoked” seizures and constitute the diagnosis of post-traumatic epilepsy (PTE). The early post-traumatic seizures are often prophylactically managed with standard antiseizure drugs. However, the “timely” treatment of PTE is very difficult because of the unpredictability of its onset and its sporadic manifestation. Therefore, animal research is urgently needed to advance our knowledge of the epileptogenesis of PTE and targeted treatment strategies.
Pre-clinical studies of PTE have been attempted in a few well-established rodent models of TBI 3 ; for example, lateral fluid percussion brain injury, 4 controlled cortical impact brain injury, 5,6 and weight-drop closed-head brain injury. 4 Despite of the maturity of these models in contributions to the understanding of molecular, cellular, and functional aspects of human TBI, their applications in modeling clinical PTE have encountered serious challenges because of logistical difficulties caused by the prolonged and random latent period of seizure occurrence. Video-electroencephalographic (EEG) recordings have often been employed either intermittently over a period of time 7 –9 or continuously for a defined duration, 10 and have indeed detected spontaneous non-convulsive seizures in 3–18% of the animals following controlled cortical impact brain injury 5,8 and in 3–50% following lateral fluid percussion brain injury 5,10 over a long period of time. To mitigate logistical difficulties, a measure of seizure susceptibility has been used as an alternative PTE model, in which delayed post-traumatic seizures are elicited by a convulsant agent; for example, pentylenetetrazole (PTZ), at a sub-convulsant dose that is normally benign for naïve animals. Following the PTZ challenge, an increased seizure susceptibility (lowered seizure threshold) may indicate an increased risk of PTE and may serve as a surrogate measure of PTE. 11 –14 This kind of seizure susceptibility test can significantly reduce the logistical burden of detecting spontaneously occurring seizures after TBI.
Both clinical 15 –17 and animal 5,6,10,18 studies have shown that injury severity of TBI is correlated with the increased risk of PTE. Following a mild TBI, 1.5–5% of patients developed delayed post-traumatic seizures and epilepsy. 19,20 This number rises to 13–20% of patients with moderate to severe non-penetrating TBI, 1,19,21 and is further escalated up to 35–53% of patients by penetrating TBI, especially among veterans of World War II and the Vietnam War. 17,22 Although closed-head brain injuries are generally milder and carry a lower risk of developing PTE, the actual number of PTE victims resulting from mild TBI can be significant, because the vast majority of TBI patients have mild TBI. According to a 2015 Centers for Disease Control (CDC) report to Congress, ∼2,200,000 TBI patients sustained mild brain injury (treated and released from emergency department) in 2010 alone. To date, success in modeling human PTE in animal models of penetrating brain injury or closed-head (without craniotomy) brain injury is very limited. 3,9 In this regard, our laboratory is uniquely equipped with two well-characterized rat TBI models: a military relevant penetrating ballistic-like brain injury (PBBI) model, 23 and a severe closed-head injury (CHI) model. 24 Importantly, the PBBI model has been successfully used in studies of antiseizure drug therapy against early (< 7 days) post-traumatic non-convulsive seizures. 25,26 In this study, we took the advantage of having both penetrating and closed-head brain injury models in-house, and investigated delayed post-traumatic seizures in an attempt to establish potential novel etiology-based animal models of PTE that may be used for pre-clinical studies of PTE.
Methods
Adult male Sprague–Dawley rats (275–350 g, Charles River Labs, Raleigh, VA) were used in this study. The rats were housed individually in a well-ventilated vivarium under a normal 12 h light/dark cycle (lights on 0600–1800). Food and water were provided ad libitum. All surgical procedures were performed with the animals under 2% isoflurane anesthesia with their body temperature maintained at 37.0°C using a heating blanket (Harvard Apparatus, Holliston, MA).
TBI models
PBBI
The rat PBBI model was implemented by an apparatus consisting of a computer-controlled pressure pulse generator operated by a cylinder impact system filled with water (Mitre Corp, McLean, VA). A specially designed PBBI probe was made of a 20 g stainless steel tube with lines of perforations along one end (∼ 10 mm) sealed by a piece of airtight silastic tubing. The other end of the probe was attached to the PBBI device. Two injury trajectories (frontal and lateral), two injury severity levels (10% and 12.5% of the brain volume) for each trajectory, and two survival durations (1 month and 6 months post-injury) for each injury condition were tested in separate cohorts of animals, yielding a total of eight experimental groups: 2 trajectories × 2 severities × 2 time points (n = 8–15/group). These PBBI groups are abbreviated as the following: F10% PBBI-1 (n = 9), F10% PBBI-6 (n = 9), F12.5% PBBI-1 (n = 8), F12.5% PBBI-6 (n = 15), L10% PBBI-1 (n = 8), L10% PBBI-6 (n = 10), L12.5% PBBI-1 (n = 9), and L12.5% PBBI-6 (n = 12).
Frontal PBBI
The general procedures of frontal PBBI have been described extensively in our previous publications. 23,27 Briefly, during the surgery, the rat was secured on a stereotaxic device equipped with a custom-made probe holder. The PBBI probe was secured on the holder at an angle of 50 degrees from the vertical axis and 25 degrees from the midline (counterclockwise), aiming at the right frontal pole of the rat brain for entry. After a midline incision and craniotomy (anteroposterior [AP]: +4.5 mm and mediolateral [ML]: +2.0 mm to bregma; diameter = 4 mm), the probe was advanced through a cranial window into the right frontal cortex to a depth of 12 mm from the surface of the brain. Once it was in place, the pressure pulse generator was activated by a computer to rapidly inflate/deflate (∼37 ms) the silastic tubing on the probe to an elliptical-shaped water balloon. This rapid inflation/deflation of the water balloon mimics the generation of a ballistic shock wave, creating a temporary cavity in the brain. The balloon size was calibrated to be either 10% or 12.5% of the rat brain volume. Once the balloon was deflated, the probe was retracted, the cranial opening was sealed with sterile bone wax, and the skin incision was suture-closed.
Lateral PBBI
For the lateral PBBI trajectory, similar procedures as those described were followed except that the rat left temporal surface of the skull was exposed by an incision of the left temporalis and an opening of the cranial window was made (AP: +1 mm to bregma, −4 mm below the lateral temporal skull ridge; diameter = 4 mm). The PBBI probe was inserted horizontally through the cranial window into the brain to a depth of 12 mm.
Injury severity level
The injury severity of PBBI was determined by the size of the inflated balloon calibrated to produce brain damages, which were measured in volumes proportional to the total brain volume. In this study, two injury severity levels were tested for each trajectory. The 10% PBBI was produced by the balloon size with a diameter of 6.3 mm, and the 12.5% PBBI was produced by the balloon size with a diameter of 7.1 mm.
Sham controls
Two age-matched sham PBBI rats received surgery procedures under isoflurane anesthesia to expose the frontal brain surface through a cranial window without the insertion of the PBBI probe. They were allowed to survive 1 or 6 month(s) after surgical procedures and named Sham PBBI-1 and Sham PBBI-6.
Severe closed-head brain injury
The CHI was produced by a projectile impact to the dorsal/lateral surface of the rat skull without craniotomy. 24 The apparatus of the CHI consisted of an elevated platform and a computer-controlled electropneumatic pressure release system, which is equipped with a projectile-launching device located directly beneath a small oval opening on the platform. A stainless steel ball projectile (3.5 g and 10.0 mm diameter) was launched upward through a tightly fit silicone tube at a distance 5 cm beneath the platform. To induce a severe CHI, the rat was deeply anesthetized with 4% isoflurane vapor for 4 min in an anesthesia chamber and then quickly placed on the elevated platform in a supine position with the head situated over the small oval opening on the platform such that it was in the direct vertical path of the projectile. Once the rat was put in position, the projectile was launched by the computer through the release of compressed air, aiming at the dorsal-lateral frontal quadrant of the rat head. Immediately after the impact, the rat was returned to its home cage and its righting reflex latency was recorded. Subsequently, the animals were re-anesthetized with isoflurane for the examination of gross pathology of the impacted skull. For this purpose, a skin incision was made longitudinally on the rat head. The presences of skull fracture and subcutaneous and/or subdural hemorrhage were recorded for each rat. Then the skin incision was closed with sterile silk suture. The CHI rats were allowed to survive 1 month (CHI 1-mon, n = 13) or 6 months (CHI 6-mon, n = 20) after the injury. Each CHI group was paired with an age-matched sham control group, which received isoflurane anesthesia of equal duration without being subjected to the projectile impact and survived 1 month (Sham CHI-1) or 6 months (Sham CHI-6) after the sham procedures.
Detecting spontaneous post-traumatic non-convulsive seizures
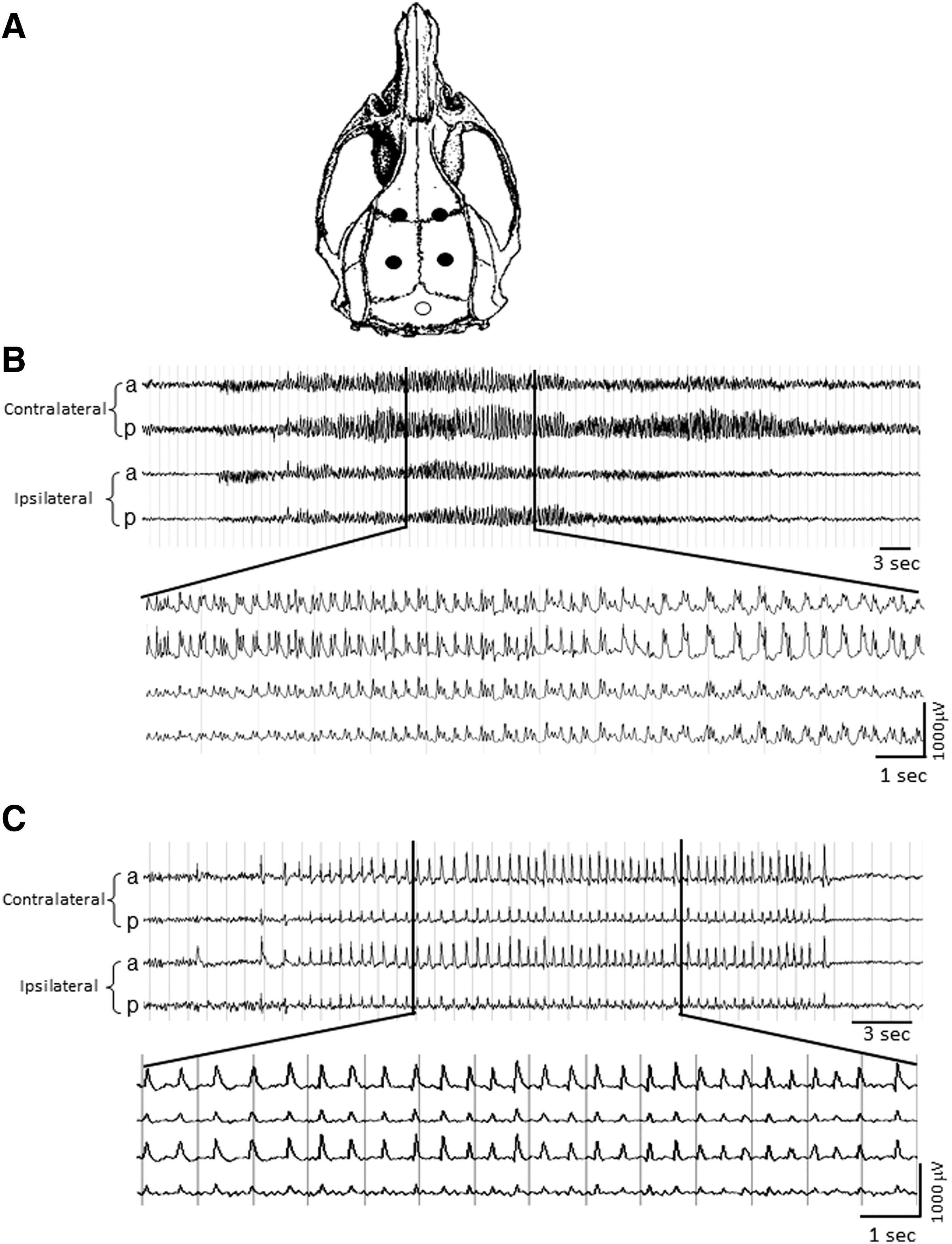
A diagram of the experimental design is provided in Figure 1. Following PBBI or CHI brain injuries, rats were visually observed in their home cages periodically during the day and regularly twice per week (60 min per session) for detection of convulsive behavioral seizures. In anticipation of seizures that may be non-convulsive in nature, all PBBI rats (n = 80) and CHI 6-mon rats (n = 20) received continuous video-EEG monitoring for 10 days at the end of each experimental time point. The CHI 1-mon rats were excluded from EEG monitoring because of the unhealed skull fractures. For rats receiving EEG monitoring, four EEG electrodes were symmetrically implanted over the bilateral frontal and parietal regions of the brain (AP: +1 and −4 mm; ML: ±3.5 mm to bregma) when rats were under 2% isoflurane anesthesia. These electrodes were individually connected to a reference electrode to create a four channel mono-referential EEG recording montage 23 (Fig. 2A). The EEG recordings were collected with synchronized video recordings (Stellate Harmonie software, Natus Medical Inc., San Carlos, CA) immediately after electrode implantation and continued for 10 days. The EEG signals were reviewed off-line to identify spontaneous non-convulsive seizures.
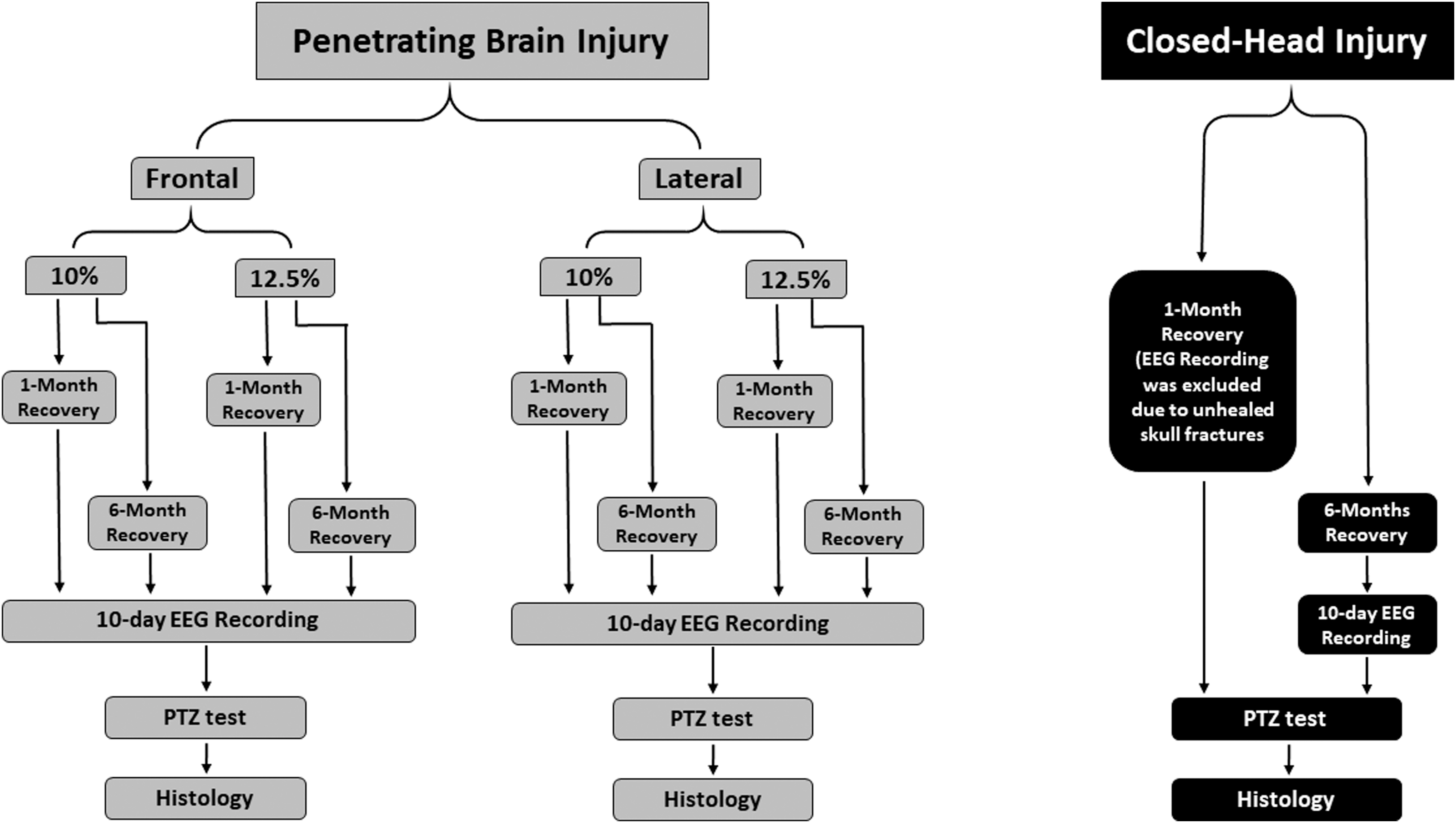
A flow chart of the experimental design.
Evaluating increased seizure susceptibility
PTZ is a selective inhibitor of the chloride channel, which is coupled to the γ-aminobutyric acid (GABA)A receptor 28,29 and therefore serves as a GABAA receptor antagonist. 11 It has been widely used as a chemo-convulsant in rodent seizure research. 30 –32 A high dose of PTZ; for example, ≥50 mg/kg, consistently causes seizure activities, progressing from myoclonic jerks to generalized tonic-clonic seizures in naïve rats, 28,33,34 whereas a lower dose of PTZ; for example, 30 mg/kg, causes seizures in only a small portion of naïve rats. 34,35 In order to evaluate increased seizure susceptibility potentiated by a brain trauma, a sub-convulsant dose of PTZ at a range of 25–35 mg/kg has been commonly used to measure higher seizure incidence compared with sham controls. 11 –14,35 –38
In this study, all rats received an intraperitoneal (i.p) injection of 30 mg/kg PTZ at the end of the EEG recording session. This dose was selected based on the literature references mentioned as well as on our own pilot observations that 30 mg/kg PTZ was more consistent than 25 mg/kg PTZ as a sub-convulsant dose in causing seizures in a small percentage of naïve rats. The rats were monitored individually in EEG recording chambers along with video monitoring for 10 min after PTZ injection. (In a previous pilot study, no seizures were observed beyond 10 min after PTZ injection.) Any seizure activities from mild jerks to tonic-clonic seizures were annotated on the video recordings and reviewed later for accurate latency. The severity level of seizure activities was scored using the following scale: 0 = no overt seizure activities, 1 = five or fewer myoclonic jerks, 2 = more than five myoclonic jerks without convulsive behavior, 3 = mild and non-tonic/clonus seizures (freezing, rearing/falling, and rolling), 4 = myotonic/clonus generalized seizures, 5 = tonic/clonus generalized seizures evolving into “pop-corn” convulsion, and 6 = death following severe convulsion. This scale system was developed based on our own observations, which significantly deviated from Racine's scale, but closely matched the scales developed by others specifically for PTZ-induced seizures in rats. 39,40
Histopathology
At the termination of each experiment, TBI rats were deeply anesthetized and transcardially perfused with 0.1 M phosphate buffer followed by 4% paraformaldehyde. Coronal brain sections (40 μm in thickness at 960 μm intervals) were stained with hematoxylin and eosin and digitally imaged. The lesion volume of each brain was calculated by integrating the lesion areas of sequential brain sections.
Statistical analysis
Spontaneous seizures were evaluated based on visual observation of the animals and the review of video EEG recordings. The seizure activities following the PTZ challenge were analyzed using the following key measures: (1) seizure incidence (number of animals within an experimental group that experienced seizure events, expressed as the percentage of the group), (2) seizure severity scores (described previously), and (3) seizure latency (the time lapse [sec] between PTZ injection and the first seizure event). Rats that did not exhibit seizure activities were assigned 600 sec for the latency, which was the maximal length of observation for statistical analysis, but the mean latency of “seizure only” rats (excluding the assigned 600 sec data) was also calculated for each group. Group differences in seizure incidence were evaluated using the Fisher exact test (FET). Two way analysis of variance (ANOVA) was used to evaluate the effects of different injury trajectories, severities, and post-injury survival durations wherever appropriate. Sidak's multiple comparisons were used to compare individual groups in the event of significant effects in the two way ANOVAs across time and injury severity. The differences were considered statistically significant at a p value <0.05. All descriptive statistics are expressed as mean ± standard error of the mean.
Results
Spontaneous post-traumatic seizures
Spontaneous convulsive behavioral seizures were not detected in any brain-injured rats (n = 80 PBBI rats and n = 33 CHI rats) or sham rats (n = 59) out to 1 or 6 month(s) after the injury via intermittent visual observations. However, spontaneous non-convulsive seizures were detected by 10 day video-EEG monitoring in 12% (5/41) of all sham rats combined, 7.5% (6/80) of all PBBI rats combined (evenly distributed among different injury conditions), and 20% (4/20) of the CHI 6-mon group. It is important to note that among all rats with EEG detected non-convulsive seizures, only one rat from the CHI 6-mon group experienced recurrent seizures that persisted for 10 days at a frequency of 1.8 ± 0.4 seizures/day (range: 0–4 seizures/day), and the average seizure duration was 47.4 ± 8.6 sec. The EEG waveforms of these seizures showed rhythmic poly-spike discharges at a frequency of 2–4 Hz (Fig. 2B). By contrast, EEG-detected seizures in all other rats occurred only during the first 4 days after EEG electrode implantation without recurrence in the subsequent recording days. The majority of these rats only had one to three seizures on a given day during the 4 day period after EEG surgery, except for one rat which had a cluster of 27 seizures on the day after EEG electrode implantation. The average seizure duration was 42.5 ± 12.5 sec. The EEG waveforms of these seizures showed simple 1–2 Hz rhythmic spike discharges and were indistinguishable between sham and brain-injured animals (Fig. 2C). These seizure characteristics apparently did not meet clinical criteria for PTE, but more likely resulted as an unexpected complication of EEG surgery; for example, potentially from accidental subdural bleeding, not associated with the initial brain injury.
Increased seizure susceptibility after PBBI
Sham PBBI
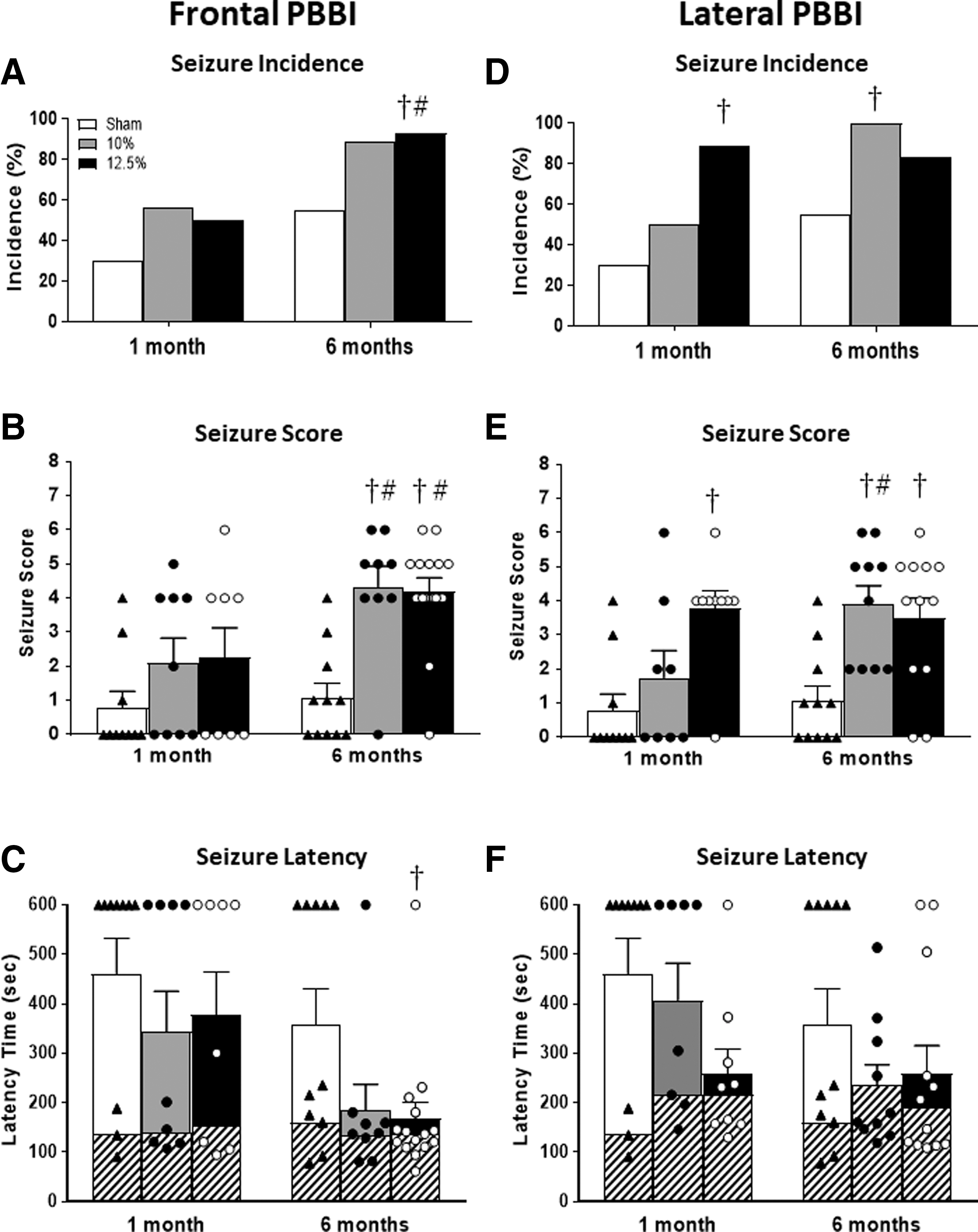
Among age-matched sham PBBI rats, 30% (3/10) of the Sham PBBI-1 group and 55% (6/11) of the Sham PBBI-6 group exhibited seizure activities when challenged by the sub-convulsant dose of PTZ. The average seizure scores were 0.8 ± 0.5 and 1.1 ± 0.4 and the average seizure latencies were 461.2 ± 71.1 sec and 359.6 ± 70.7 sec for the Sham PBBI-1 and Sham PBBI-6 groups, respectively (Fig. 3). It is noticed that the seizure susceptibility increased as the sham animals aged over time, but not to a significant degree.
Frontal PBBI
Data of three seizure measures (incidence, scores, and latency) on the PTZ challenge test for all frontal PBBI groups (two injury severity levels and two survival durations) are provided in Table 1 and Figure 3. As shown in Figure 3A–C, frontal PBBI enhanced PTZ-challenged seizure susceptibility evidenced by higher seizure incidence, more severe seizure manifestation (seizure scores), and shorter seizure latency than age-matched sham controls. Further analysis of brain injury effects (10% vs. 12.5% frontal PBBI) at each post-injury time point revealed a lack of discerned difference between the two injury severity levels. More specifically, at 1 month after frontal PBBI, 56% (5/9) of the F10% PBBI-1 group and 50% (4/8) of the F12.5% PBBI-1 group experienced seizures. The average seizure scores for these two groups were 2.1 ± 0.7 and 2.3 ± 0.9, and the average seizure onset latencies were 343.4 ± 81.6 sec and 377.4 ± 87.1 sec, respectively. At 6 months after frontal PBBI, 89% (8/9) of the F10% PBBI-6 group and 93% (14/15) of the F12.5% PBBI-6 group exhibited seizure activities. Their average seizure scores were 4.3 ± 0.6 and 4.2 ± 0.4, and their average seizure latencies were 184.3 ± 53.2 sec and 168.2 ± 32.8 sec, respectively. Although seizure susceptibility appeared not to be exacerbated by increase in injury severity, it was clearly enhanced as the post-injury survival duration extended from 1 month to 6 months (Fig. 3A–C). Statistical analysis further confirmed the presence of post-injury time effects and the absence of injury severity effects. For example, two way ANOVAs detected main injury severity effects on seizure scores (F[2,56] = 11.16, p < 0.0001) and seizure onset latency (F[2,56] = 3.282, p < 0.05), but the post-hoc analyses indicated that the significant differences only resided in the comparison between sham controls and injured animals at 6 months post-PBBI (Fig. 3B). Overall, F10% PBBI and F12.5% PBBI yielded very similar effects on PTZ-challenged seizure susceptibility across all three seizure measures at each respective time point. On the other hand, the two way ANOVAs detected main effects on post-injury durations (time effects), especially with regard to seizure scores (F[1,56] = 10.40, p < 0.01) for both the F10% and F12.5% PBBI groups (Fig. 3B). Post-hoc analyses revealed that these significances were featured by the comparisons between the F10% PBBI-1 and F10% PBBI-6 groups (p < 0.05, Fig. 3B) and between the F12.5% PBBI-1 and F12.5% PBBI-6 groups (p < 0.05, Fig. 3B). The significant time effects on seizure incidence were also evident for F12.5% PBBI (p < 0.05, F12.5% PBBI-1 vs. F12.5% PBBI-6, FET) but fell short for F10% PBBI (p > 0.05, F10% PBBI-1 vs F10% PBBI-6, FET).
Results of PTZ Challenge Test (Mean ± SEM)
PTZ, pentylenetetrazole; SEM, standard error of the mean; PBBI, penetrating ballistic-like brain injury; CHI, closed-head injury.
Lateral PBBI
Similar to the frontal PBBI, various degrees of increases in seizure susceptibility were observed at 1 and 6 month(s) after lateral PBBI compared with the age-matched sham controls. Data of seizure measures from each lateral group are presented in Table 1 and Figure 3 D–F. For the 10% lateral PBBI groups, 50% (4/8) and 100% (10/10) of the animals exhibited seizure activities, with average seizure scores of 1.8 ± 0.8 and 3.9 ± 0.5, and seizure latencies of 407.6 ± 74.3 sec and 235.6.3 ± 41.0 sec, at 1 or 6 month(s) post-injury, respectively. For 12.5% lateral PBBI groups, 89% (8/9) and 83% (10/12) of the animals exhibited seizure activities with average seizure scores of 3.8 ± 0.5 and 3.5 ± 0.6, and seizure latencies of 258.8 ± 49.7 sec and 259.5 ± 56.0 sec, at 1 or 6 month(s) post-injury, respectively. A major difference between the frontal and lateral PBBI in response to PTZ challenge was the lack of time effects. The two way ANOVAs yielded (F[1,54] = 2.502, p = 0.1195) for the time effect on seizure score and (F[1,54] = 3.204, p = 0.0791) for seizure latency. Further examination of seizures at 1 and 6 month(s) post-injury showed that this lack of time effect was likely the result of more enhanced seizure susceptibility detected as early as 1 month after L12.5% PBBI (L12.5% PBBI-1 group) compared with that of the age-matched Sham PBBI-1 group, such that similar degrees of seizure activity measures were observed for both the L12.5% PBBI-1 and L12.5% PBBI-6 groups (Fig. 3D,E). Statistical analysis showed that seizure incidence was significantly higher in the L12.5% PBBI-1 group than in the age-matched Sham PBBI-1 group (p = 0.0198, FET, Fig. 3D). Similarly, a main effect of injury severity on seizure score was also observed (F[2,54] = 12.89, p < 0.0001). Post-hoc analyses revealed that the L12.5% PBBI-1 group had significantly higher seizure scores than the age-matched sham group (p < 0.05, L12.5% PBBI-1 vs. Sham PBBI-1).
Increased seizure susceptibility after closed-head brain injury
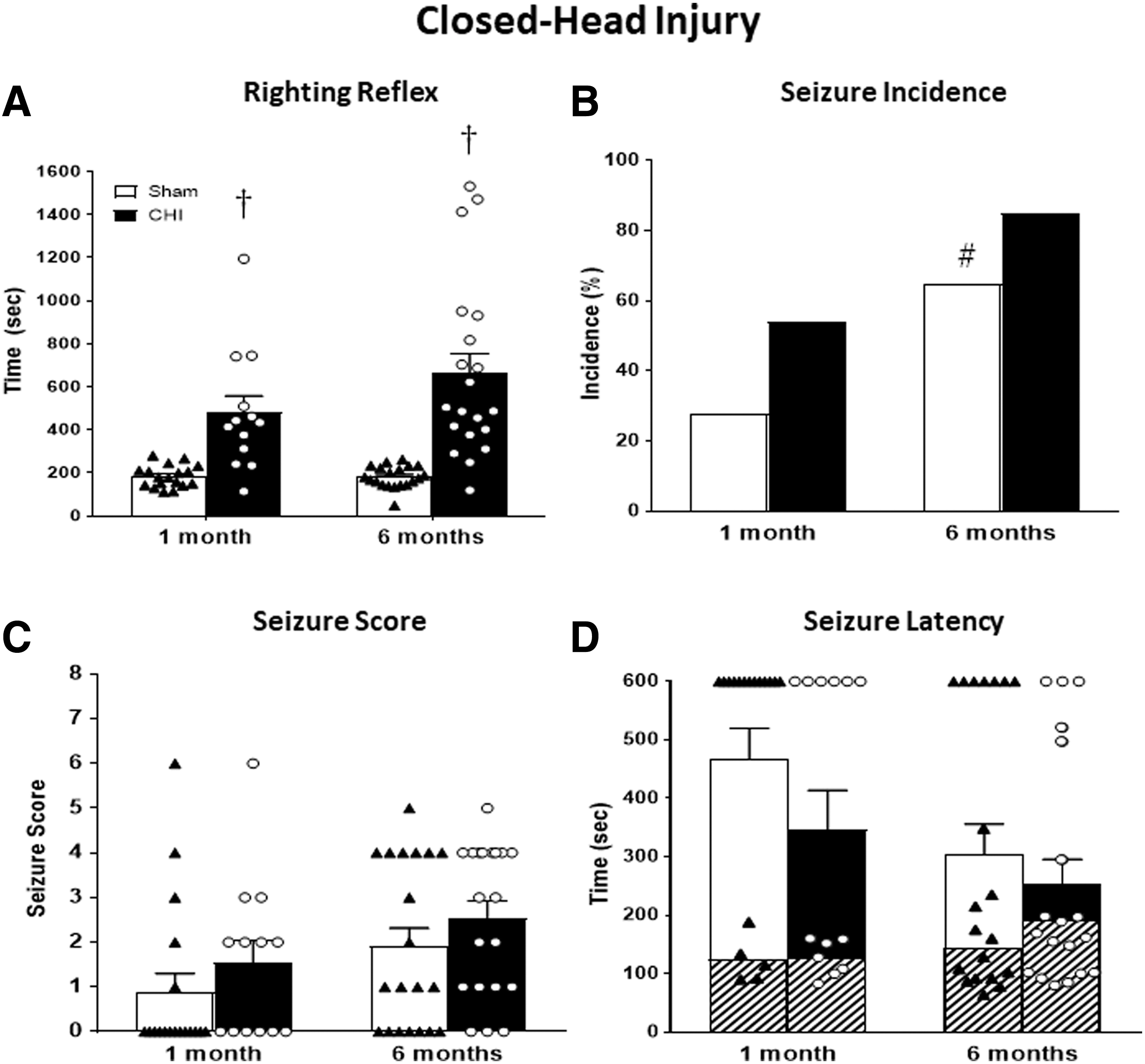
Rats were under deep anesthesia for CHI or sham procedures. The righting reflex times recorded for the sham groups were 176.7 ± 9.8 sec and 181.6 ± 11.5 sec for the Sham CHI-1 and Sham CHI-6 groups, respectively, which reflected the duration of waking from the anesthesia. However, following CHI, the righting reflex durations were significantly prolonged to 658.3 ± 90.5 sec and 661.2 ± 92.1 sec for the CHI 1-mon and CHI-6-mon groups, respectively (p < 0.05), indicating a severe concussive consequence versus age-matched sham group. Subsequent analysis of the relationship between the righting reflex time and the seizure scores did not reveal significant correlations between the two measures for each group (R2 < 0.1, and p > 0..05, data not shown).
Similar to sham PBBI animals, at 1 month after sham CHI, 28% (5/18) of the animals (Sham CHI-1 group) exhibited seizure activities in response to PTZ challenge with an average seizure score of 0.9 ± 0.4 and an average seizure onset latency of 467.7 ± 52.0 sec. Seizure susceptibility of the Sham CHI-6 group was also noticeably enhanced as this cohort of animals aged, such that 65% (13/20) of the Sham CHI-6 group exhibited seizures with an average seizure score of 1.9 ± 0.4, and average seizure latency of 304.2 ± 51.8 sec.
Following CHI, the seizure susceptibility to PTZ challenge was relatively milder than that following PBBI, showing a moderate but non-significant increase at both time points for all seizure measures as compared with the age-matched sham CHI controls. As shown in Table 1 and Figure 4, 54% (7/13) of the CHI 1-mon group and 85% (17/20) of the CHI 6-mon group exhibited seizures in response to PTZ challenge. Their average seizure scores were 1.5 ± 0.5 and 2.6 ± 0.4, and their average seizure latencies were 345.4 ± 68.3 sec and 252.6 ± 43.0 sec, respectively. With regard to the post-injury time effects, increase in seizure incidences were observed in both the sham and CHI groups from 1 to 6 months post-injury, but the significant difference was detected only in the sham groups (p < 0.05, FET, Sham CHI-1 mon vs. Sham CHI-6 mon). Two way ANOVAs also identified main effects of time following CHI injury for seizure score (F[1,67] = 5.621, p < 0.05) and latency (F[1,67] = 5.774, p < 0.05), but post-hoc analysis failed to detect significant difference across any individual comparisons.
Histopathology
The frontal and lateral PBBI caused acute laceration of brain tissues along the injury track. The initial brain damage expanded into a large permanent cavity at 1 and 6 month(s) post-injury. The frontal PBBI affected the right frontal and parietal cortices, striatum, and caudate-putamen. The lateral injury affected the left parietal cortex, striatum, and hippocampus (Fig. 5). The average lesion volumes (mm3) of the frontal PBBI were 64.7 ± 8.0 (F10% PBBI-1), 78.3 ± 21.3 (F10% PBBI-6), 114.7 ± 11.7 (F12.5% PBBI-1), and 106.5 ± 10.3 (F12.5% PBBI-6). The average lesion volumes (mm3) of the lateral PBBI were 94.4 ± 10.9 (L10% PBBI-1), 117.3 ± 9.7 (L10% PBBI-6), 133.3 ± 12.7 (L12.5% PBBI-1), and 130.4 ± 4.5 (L12.5% PBBI-6). (Fig. 6). Although the two way ANOVAs revealed an injury severity effect for both frontal PBBI (F[1,21] = 7.196, p = 0.0139) and lateral PBBI (F[1,23] = 4.525, p = 0.0443), post-hoc analysis failed to identify significant difference between the two injury severities for either trajectory. Within each injury trajectory, no significant post-injury time effects were detected when lesion volumes were compared between 1 and 6 month(s) across different injury severities. Further, there were no correlations between brain lesion volumes and any measures of PTZ-induced seizures for all PBBI groups.
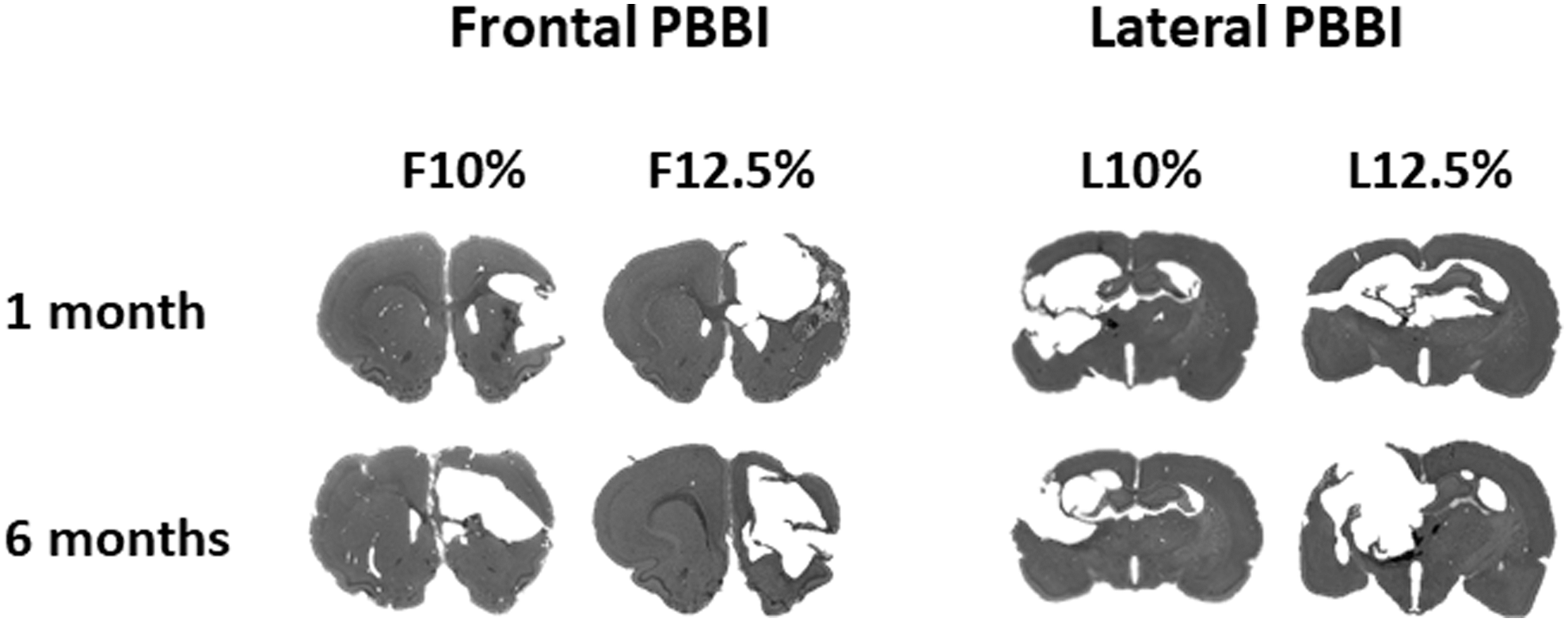
Examples of brain images showing permanent lesion cavities resulted from frontal and lateral penetrating ballistic-like brain injury (PBBI) at 1 month and 6 months post-injury.
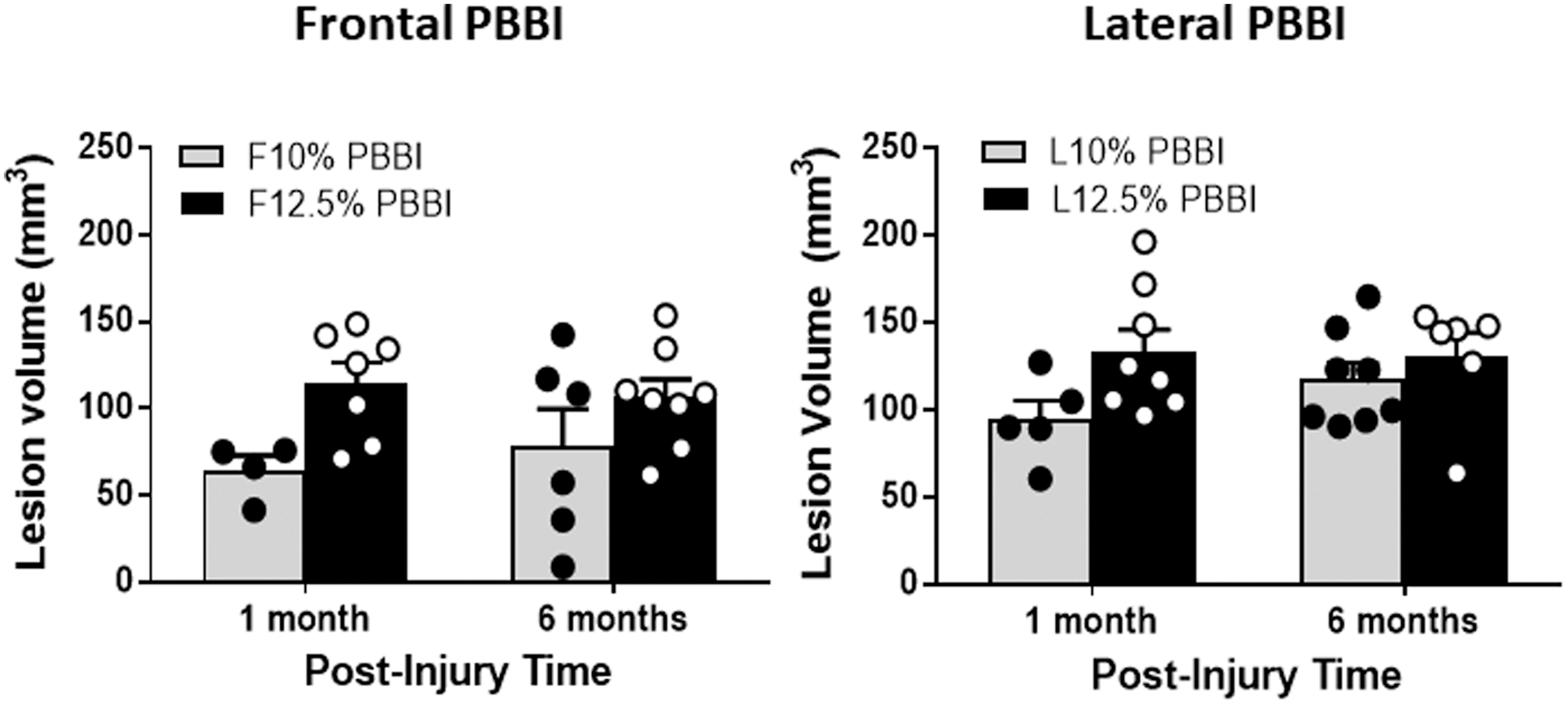
Lesion volumes resulted from frontal and lateral penetrating ballistic-like brain injury (PBBI) at different injury severity levels and survival time points. Although two way analyses of variance (ANOVAs) revealed an injury severity effect for both frontal and lateral PBBI, post-hoc analysis failed to identify a significant difference between the two injury severities for either trajectory. Within each injury trajectory, no significant post-injury time effects were detected when lesion volumes were compared between 1 month and 6 months across different injury severities.
For the CHI animals, examination of gross pathology of rat skulls immediately after CHI revealed that 78% of these rats had skull fracture and 92% had subcutaneous/subdual hemorrhage. The histopathology analysis showed that 55% of the CHI 1-mon group and 65% of the CHI 6-mon group had various degrees of cerebral lesion cavity near the impact site and subcortical regions. There was no significant difference in lesion volumes between the two groups: (CHI 1-mon: 18.8 ± 7.5 mm3, and CHI 6-mon: 21.2 ± 6.9 mm3, p > 0.05, data not shown). Two rats in the CHI 6-mon group had significantly large lesions (> 2 standard deviations [SD] of the mean) and were excluded from the lesion analysis. Similar to the PBBI animals, no positive correlations between seizure susceptibility and gross pathology (skull fracture and hemorrhage) or histopathology (lesion volume) were detected after CHI.
Discussion
The purpose of this study was to extend animal modeling of PTE to two new rat models of penetrating and closed-head TBI in order to broaden our knowledge of the validity and limitations of pre-clinical models of PTE. The key findings of this study were the following: (1) spontaneous convulsive seizures were difficult to induce or detect by intermittent visual observations out to 6 months following a penetrating brain injury in rats, and the same difficulty was encountered in a severe rat closed-head brain injury model; (2) when EEG monitoring was applied, spontaneous non-convulsive seizures were detected in one CHI rat that had the characteristics of clinical PTE, whereas the non-convulsive seizures detected by EEG in other rats were likely confounded by the EEG electrode implantation surgery; and (3) when challenged with a sub-convulsant dose of PTZ after TBI, the majority of TBI rats demonstrated increased seizure susceptibility compared with the age-matched sham controls, and the enhanced seizure activities were associated with TBI modalities (frontal vs. lateral injury, and penetrating vs. closed-head) and post-injury durations. Collectively, our results highlighted the difficulties of inducing or detecting delayed spontaneous post-traumatic seizures that signify clinical PTE. However, the increased seizure susceptibility to sub-convulsant PTZ challenge following TBI may indicate an existence of vulnerable risk of post-traumatic epileptogenesis, which can be considered as an alternative tool for pre-clinical studies of PTE.
In humans, PTE is a unique secondary sequelae of TBI because it evolves in a subpopulation of patients over an unpredictable latent period (weeks to years) after various types of brain trauma (penetrating vs. closed-head brain injury, focal vs. diffused injury). Pre-clinical modeling of this chronic disease has made considerable efforts to replicate clinical PTE in several well-established animal models of TBI. To date, sporadic delayed (> 2 weeks post- injury) spontaneous convulsive and non-convulsive seizures have been reported in rodent models of controlled cortical impact brain injury, 6,8 lateral fluid percussion brain injury, 7,10,41 and penetrating brain injury. 9 In these models, most seizures were detected by continuous or intermittent EEG recordings. Two characteristics of these TBI models that are associated with human risk factors of PTE are injury severity 7,10,41 and focal/diffuse nature of the injury. 42 The controlled cortical impact and penetrating brain injury produce a very focal brain damage aimed at the hippocampus of the brain, whereas the FPI causes a semi-focal and diffused brain injury. In these animal models, seizure incidence ranged between 5% and 50%, depending on the injury severity. 5,6,9,43 By contrast, an animal model of weight drop represents a milder and more diffused brain injury, and rarely induces spontaneous PTE. 42
Taking these risk factors into consideration, in this study we employed a rat model of penetrating brain injury that produced a unique ballistic impact to simulate severe military-relevant TBI and caused defined focal brain damages along the ballistic injury tract. Although the frontal PBBI did not aim at the hippocampus directly, the ballistic impact from the balloon inflation inside the brain indeed affected the hippocampus, as evidenced by our previous studies that showed significant activation of astrocytes and microglial cells in the hippocampus following frontal PBBI. 25 The lateral PBBI aimed at the brain region directly anterior to the hippocampus and resulted in the formation of a large hippocampal cavity. We also manipulated the injury severity and trajectory. Nevertheless, no credible spontaneous post-traumatic seizures were detected out to 6 months following either 10% or 12.5% PBBI of both frontal and lateral trajectories. These results appeared to be counterintuitive against clinical observations of the association between severe penetrating brain injury and the development of PTE. However, further histopathological examination of the brain damage of PBBI rats revealed that the ballistic impact of the PBBI model caused a large lesion cavities that, by 1 month post injury, completely eroded injurious penumbra along the injury track. The lesion cavity almost matured by 1 month post-injury, showing no significant expansion at 6 months post-injury (Fig. 5). It is postulated that this void of brain tissue might be inadvertently responsible for the failure of generating spontaneous seizures in our rat PBBI model because of the absence of anatomical tissue substrates that are necessary for post-traumatic epileptogenesis. This might also be the reason for the lack of injury severity effects following 10% and 12.5% PBBI, as the large lesion cavity was indistinguishable between the two cohorts of animals.
Following CHI, the lesion cavity was relatively smaller and present only in some animals, indicating a milder brain injury inflicted. Yet, only one of these rats developed PTE. The neuropathological and histopathological examination of this rat revealed that it had prolonged righting reflex latency (∼ 24 min vs. average 11 min), severe skull fracture, subdual hemorrhage, and a significantly larger lesion cavity (excluded from the lesion analysis). Apparently this particular rat experienced a more severe CHI than other CHI rats. Clinical studies have shown that loss of consciousness or amnesia over a long period of time; for example, >24 h, 1 depressed skull fractures, 16,17,44 intracerebral or subdural hemorrhage, 1,16,44 and brain contusion 44 are all high risk factors for the development of PTE. It is possible that all these factors combined in this CHI rat could have attributed to the development of spontaneous PTE. In the majority of the other CHI rats, skull fractures and subdural hemorrhage did not result in substantial brain lesions, and none of them exhibited repetitive spontaneous seizures, suggesting that the injury severity of CHI is a risk factor for epileptogenesis of PTE.
It is important to take into account that EEG monitoring was performed for only 10 consecutive days for each time point examined in this study. It is possible that spontaneous seizures might have occurred outside the EEG recording time frame and were not captured. Although longer recording time is undoubtedly preferred for this type of study, logistical difficulties and resource limitations are always a concern, especially when the animal model of PTE is intended to be used for relatively high-throughput studies of therapeutic intervention, which require multiple groups of animals for even a single drug testing to determine the dose-response efficacy and pharmacokinetic profile. However, extending EEG recording to 14 days could be a feasible compromise, considering that seizures have been detected during intermittent 2 week recording episodes in the lateral fluid percussion and controlled cortical impact brain injury models. 5 On the other hand, it is equally important to recognize seizures that were likely provoked by the EEG electrode implantation. The distinction between “post-traumatic” seizures and “post-operative” seizures that resulted from complications of EEG surgeries have also been reported by other researchers in sham and naïve rats. 45,46 Therefore, it is necessary to allow 4–5 days of recovery after EEG electrode implantation before initiating EEG recording to avoid seizures provoked by the EEG surgeries.
Human studies of PTE have been explored, especially the mechanisms that underlie the epileptogenesis; 47,48 however, difficulties exist with respect to limited accessibility. The purpose of pre-clinical modeling of human PTE is to allow the use of laboratory animals to study clinical problems that are not easily studied in human patients; that is, investigation of the time course of epileptogenic mechanisms, PTE biomarkers in cerebrospinal fluid, and novel therapeutic development using relatively large number of subjects at low cost. The animal models of TBI mentioned here have shown that rodents are indeed prone to the development of PTE when the experimental conditions permit, albeit that detecting these seizures can be technically challenging to the extent that it hinders high-throughput investigations. To overcome this difficulty, alternative approaches have been adopted to study seizure susceptibility as a measure of PTE based on the assumption that the post-traumatic seizures, although latent or not emerging, can be elicited by a secondary inducer. Such seizure inducers include PTZ, 12,14,30,36 FeCl3, 49,50 tacrolimus, 46 copper, 9 and pilocarpine, 51 among which PTZ is most commonly used for this purpose. In this study, a sub-convulsant dose of PTZ successfully demonstrated enhanced seizure susceptibility following penetrating brain injury and, to a lesser degree, following the CHI as well. Interestingly, in the PBBI model, the injury severity and trajectory appeared to have a lesser impact on the degree of seizure susceptibility than the post-injury duration did. However, these post-injury time effects were somewhat confounded by unexpected age effects observed in the matching sham control rats, as older sham rats also became more sensitive to PTZ challenge.
The “age” effects of PTZ-evoked seizures have been reported previously in different strains of rats, which showed an age-dependent decrease in PTZ-induced seizure thresholds in Wistar and WAG/Rij rats. The authors showed that as the animals aged from post-natal days 26 to 220, a lower dose of PTZ was needed to induce seizures, and the latency to the onset of clonic and tonic seizures became shorter. 39 Although age-related changes of sensitivity to PTZ challenge are not fully understood, the aging process of the cerebral GABAergic system, such as decreases in GABA release or binding, was implicated in older rats. 39 Pharmacokinetic study of PTZ also suggested that age-dependent alteration in the brain uptake and systemic absorption and elimination of PTZ might be responsible for the changes in sensitivity to PTZ in developing rats. 52 This natural aging effect on PTZ-evoked seizure sensitivity might have confounded the post-injury time effects observed in this study. However, compared with the respective age-matched sham controls, the post-injury time effects were still salient across most TBI groups, especially following PBBI. The exception to this was the L12.5% group, which showed substantial sensitivity to PTZ as early as 1 month post-injury. Therefore, brain trauma might have exacerbated the aging factor, or vice versa, with respect to the increased risk of developing PTE over time. Compared with the counterpart of frontal PBBI, animals that sustained a L12.5% PBBI appeared to be more prone to post-traumatic epileptogenesis as early as 1 month post injury, which likely masked the aging effect by 6 months post injury.
In this study, the lateral PBBI trajectory entered the rat brain anterior to the hippocampus, but the ballistic force severely damaged the ipsilateral hippocampus and very likely impacted the contralateral hippocampus. Because the hippocampus has been implicated in epileptogenesis in human temporal lobe epilepsy 53 as well as in animal models of PTE, 6,7 including PTZ-induced enhancement of seizure susceptibility, 12,18,54 the lateral PBBI should be favored with regard to studying post-traumatic seizure susceptibility, especially considering that early detection of increased risk of PTE epileptogenesis could significantly reduce experimental duration.
The use of increased seizure susceptibility to PTZ challenge as a measure of PTE has raised concerns about its clinical relevance. These concerns are rooted in the argument that the mechanisms of PTZ-induced seizures are not necessarily the same as those of the spontaneously occurring seizures in PTE. Although this argument is true, a strict demand for clinical relevance may adversely impede the applicability of current animal TBI models to high-throughput study of PTE with respect to therapeutic intervention and mechanisms that require relatively large numbers of animals. As a result, a valid animal model of clinical disease may lose its value as a research tool. In fact, in human TBI patients, the initial brain injury may not be the sole cause of PTE epileptogenesis. Other physical and health conditions, such as sleep deprivation or chronic alcoholism, which are implicated in non-TBI originated epilepsy, 55 –59 may also synergistically contribute to the development of PTE. Although we cannot equate PTZ challenge to these risk factors, nor should we use PTZ-challenged seizure susceptibility as a biomarker for clinical PTE or as a measure of epileptogenesis because of its “instantaneous” and “non-spontaneous” nature, the ability of PTZ to elicit seizure activities at a sub-convulsant dose suggests that vulnerable risks of epileptogenesis in animal models of TBI do exist and can be brought to light when conditions permit. Therefore, the seizure susceptibility test could be considered as a compromise to the current lack of better alternatives, and accepted as a surrogate animal model of PTE because of its feasibility for pre-clinical research. In fact, previous studies by others have demonstrated the usefulness of PTZ tests in studies of various treatment strategies to attenuated PTZ-induced seizure susceptibility and the associated mechanisms. 36,60,61
In this study, the PTZ-induced increase in seizure susceptibility was also evident in the rat models of penetrating and closed-head concussive brain injuries. Although these results appeared to be supplementary to the reports already available in the literature, the important significance of this study lies in the novel TBI models used, especially the military-relevant model of PBBI. Penetrating brain injury is a well-recognized high risk factor for the development of PTE among military veterans, 22,62 yet no animal TBI models have addressed military PTE to date. One of the hallmarks of our PBBI model is the EEG-detected early non-convulsive seizures during the first few days after injury, 23 which have been well characterized, 23 and which contributed significantly in our previous studies of antiseizure drug therapy. 24 –26 The current study was a continuation of our efforts to address military-relevant post-traumatic seizures/epilepsy. Although the results in detecting delayed spontaneous seizures did not meet our expectations, the PTZ-induced increased seizure susceptibility in both TBI models has validated findings by others using different TBI models, and therefore supports the use of PTZ challenge test in our future studies of therapeutic intervention against military relevant PTE.
Conclusion
In summary, in this study we explored animal modeling of PTE in rats that sustained penetrating or closed-head brain injury. Spontaneous post-traumatic seizures were not detected out to 6 months following PBBI and were only evident in one CHI rat at 6 months post-injury. The lack of detectable spontaneous post-traumatic seizures that meet the criteria for clinical PTE in the majority of the TBI animals could be the result of the caveats of these TBI models; for example, too severe an injury following PBBI, which caused an extensive lesion cavity, or a not severe enough injury following CHI, or it could be the result of the limited EEG detection duration (e.g., only 10 days of continuous EEG recording). Future studies are needed to extend EEG detection duration and vary TBI conditions, including aiming at the hippocampus of the brain. Nevertheless, increased seizure susceptibility measured by PTZ challenge in a novel penetrating brain injury model may serve as a feasible research tool for relatively high-throughput pre-clinical studies of therapeutic intervention against military-relevant PTE.
Footnotes
Funding Information
This study was funded by Canbat Casualty Care Research Program of the Department of Army (H_029_2014_WRAIR).
Author Disclosure Statement
No competing financial interests exist.
Material has been reviewed by the Walter Reed Army Institute of Research. There is no objection to its presentation and/or publication. The opinions or assertions contained herein are the private views of the authors, and are not to be construed as official, or as reflecting true views of the Department of the Army or the Department of Defense Research was conducted under an approved animal use protocol in an AAALACi accredited facility in compliance with the Animal Welfare Act and other federal statutes and regulations relating to animals and experiments involving animals and adheres to principles stated in the Guide for the Care and Use of Laboratory Animals, NRC Publication, 2011 edition.