
Abstract
According to in-hospital guidelines, the biomarker, S100 calcium-binding protein B (S100B), is used to rule out intracranial lesions in mild-moderate traumatic brain injury (TBI). It is currently investigated whether S100B is applicable in a pre-hospital setting. The aim was to compare S100B values and hemolysis index in blood samples drawn and stored under simulated pre-hospital conditions to standardized blood samples. Thirty patients undergoing craniotomy at Department of Neurosurgery, Aarhus University Hospital (Aarhus, Denmark) each had six blood samples drawn. Two samples, drawn in in-hospital standardized Beckton Dickinson tubes and pre-hospital Monovette tubes, respectively, were stored as references at 21°C for 30 min. Two samples were stored at 15°C and 29°C, respectively, one sample was stored at prolonged time (60 min), and one sample was transported for 30 min before centrifugation. S100B values were compared by equivalence test with a pre-defined equivalence margin of ±8.5%. There was no clinically relevant difference between samples stored in different tubes, at various temperatures, or time to analysis compared to reference samples. Transported samples had an 11.5% (90% confidence interval [CI], 6.55; 16.61) higher median S100B value and a 430% (95% CI, 279.6; 661.4) higher median hemolysis index compared to reference samples. Three of 30 (10%) patients had an S100B value above guideline cutoff in the transported sample, which was not found in reference samples (false positive). There were no false negatives. In conclusion, S100B values were not influenced by different tubes, temperatures, and time to analysis. Transported samples had higher median S100B values and hemolysis, icterus, and lipemia index compared to reference samples.
Introduction
Traumatic brain injury (TBI) patients present with a broad range of symptoms, varying from unconsciousness to no visible injuries. 1 –3 Scandinavian Neurotrauma Committee Guidelines stratify TBI patients based on Glasgow Coma Score (GCS) in minimal (GCS 15), mild (GCS 14–15 with accompanying symptoms), moderate (GCS 9–13), and severe (GCS 3–8). 1 Minimal-moderate TBI accounts for ∼95% of all patients. 1 According to the guideline, patients with minimal TBI should not be admitted to the hospital, whereas patients with mild-to-moderate TBI are referred for further examination with blood sampling and/or computed tomography (CT) scan for risk stratification. In the group of mild TBI patients, it is a classical clinical dilemma to identify the minority with intracranial lesions and to rule out the vast majority without.
In mild TBI patients 18–65 years of age with no antiplatelet/-coagulant treatment, no focal neurological deficits, and no seizures, the biomarker, S100 calcium-binding protein B (S100B), is currently used in emergency departments for clinical decision making to rule out intracranial lesion. If S100B and guidelines are applied correctly, the number of patients examined with CT scans can potentially be reduced with 30% in this patient group. 1,4
S100B is a small protein (9–14 kDa) that belongs to a family of intracellular, calcium-binding proteins predominantly found in intracranial perivascular astrocytes, but is also present in other central nervous system cells and from extracerebral sources.
5
Below the cutpoint 0.10 μg/L, S100B has a negative predictive value of >99% and a sensitivity of 97% in detecting CT visual pathology. S100B is detectable in peripheral blood within 15 min after TBI, presumably even earlier, and reaches peak blood concentration within 1–3 h—even though half-life has been suggested to be shorter within 60–120 min.
2,6
Six hours after trauma, S100B values are too ambiguous to be used for clinical decision making. Thus, based on S100B kinetics, an even earlier sampling of S100B (i.e., in the pre-hospital setting) may make it possible to utilize S100B in a higher number of TBI patients. In addition, if S100B could be measured using point-of-care testing (POCT) in the ambulance, diagnostic clarification and rule-out of TBI may be possible already in the ambulance. Thus, unnecessary ambulance transports can potentially be avoided and the use of CT scans further reduced. In addition, pre-hospital triage based on high S100B values may facilitate direct transport to a dedicated neurotrauma center, bypassing a local hospital. This potential for pre-hospital S100B sampling and the association between pre-hospital values, in-hospital values, and intracranial pathology is currently examined in clinical studies (
In ambulances, blood samples are stored and transported at varying ambient temperatures and exposed to different time to analysis depending on distance to the hospital. These pre-analytical factors can potentially affect the quality of the sample material and thereby give rise to erroneous biomarker results affecting both clinical decision making and the validity of research projects. It is especially important to ensure that values are not falsely low given that this could lead to false negatives and undertriage if using S100B for rule-out. Thus, it is important to investigate whether biomarker results in blood samples stored under various non-standardized conditions are comparable to standardized in-hospital reference samples.
The aim of this study was to compare S100B values and hemolysis index in blood samples drawn and stored under simulated pre-hospital conditions to those of standardized in-hospital blood samples. We hypothesized that mean S100B values in blood samples are equivalent across different tubes, temperatures, storage times, and after transportation. Moreover, the hemolysis-icterus-lipedema index (HIL index) is below the threshold for clinical interpretation of S100B values.
Methods
The study was designed as a prospective, observational equivalence study conducted at Department of Neurosurgery, Aarhus University Hospital (Aarhus, Denmark) from November 14, 2018 to February 21, 2019.
Patient recruitment
Patients undergoing intracranial neurosurgical procedures suffer from damage to brain tissue, leading to peri- and post-operative increase in S100B levels. These levels are comparable to patients suffering TBI. 7,8 Eligible participants were selected by a consultant physician at Department of Anesthesiology, Aarhus University Hospital among patients admitted for elective neurosurgery. The first contact took place before surgery in connection to a scheduled pre-operative anesthesiological assessment. Patients met inclusion criteria if they were >18 years of age, admitted before scheduled, elective, non-emergent intracranial neurosurgery with suspected tissue damage, and had an arterial line routinely placed for monitoring during surgery. Informed consent was obtained from all patients before inclusion. Adult patients unable to give informed consent and those not equipped with an arterial line were excluded from the study.
Data collection
Patient-related data (age, sex, diagnosis, and type and length of surgery) were collected from the electronic patient record. Six blood samples were drawn from each patient at the end of surgery from the arterial line placed pre-operatively. Time of blood sampling and duration of surgical intervention were registered. The six samples were drawn into one of five adaptable Sarstedt Serum Monovettes® as used in the pre-hospital setting (MV-ref, MV-A, MV-B, MV-C, and MV-D) containing 5.5 mL and one Beckton Dickinson Tube® (BD-ref) as used in standard in-hospital blood sampling containing 5 mL. All blood samples were drawn and processed by the primary investigator. Two samples were stored as reference samples (BD-ref and MV-ref) at 21°C for 30 min to coagulate. One sample was stored for a prolonged time of 60 min at 21°C (MV-A). Two samples were stored at 29°C and 15°C, respectively, for 30 min (MV-B and MV-C). The last sample (MV-D) was placed in the pocket of the primary investigator's uniform and brought to a car, where it was placed in the center console and transported for 30 min before it was returned to the laboratory and centrifuged along with the other samples.
The six samples from each patient were collected in pre-defined random order to avoid systematic sampling bias. All samples were drawn from patients at the operation room, brought to the laboratory, and stored in thermoboxes to ensure correct and stable temperature during the coagulation time except for the transported samples, which were brought to the car in the pocket of the primary investigator (Fig. 1). Handling of blood samples simulates pre-hospital conditions in respect to varying summer and winter temperatures. Based on presumed temperature variations from driving ambulances in the Central Denmark Region during summer and winter, temperatures were set at 29°C and 15°C. Pre-hospital condition also includes prolonged coagulation time (60 min) and transportation by car.
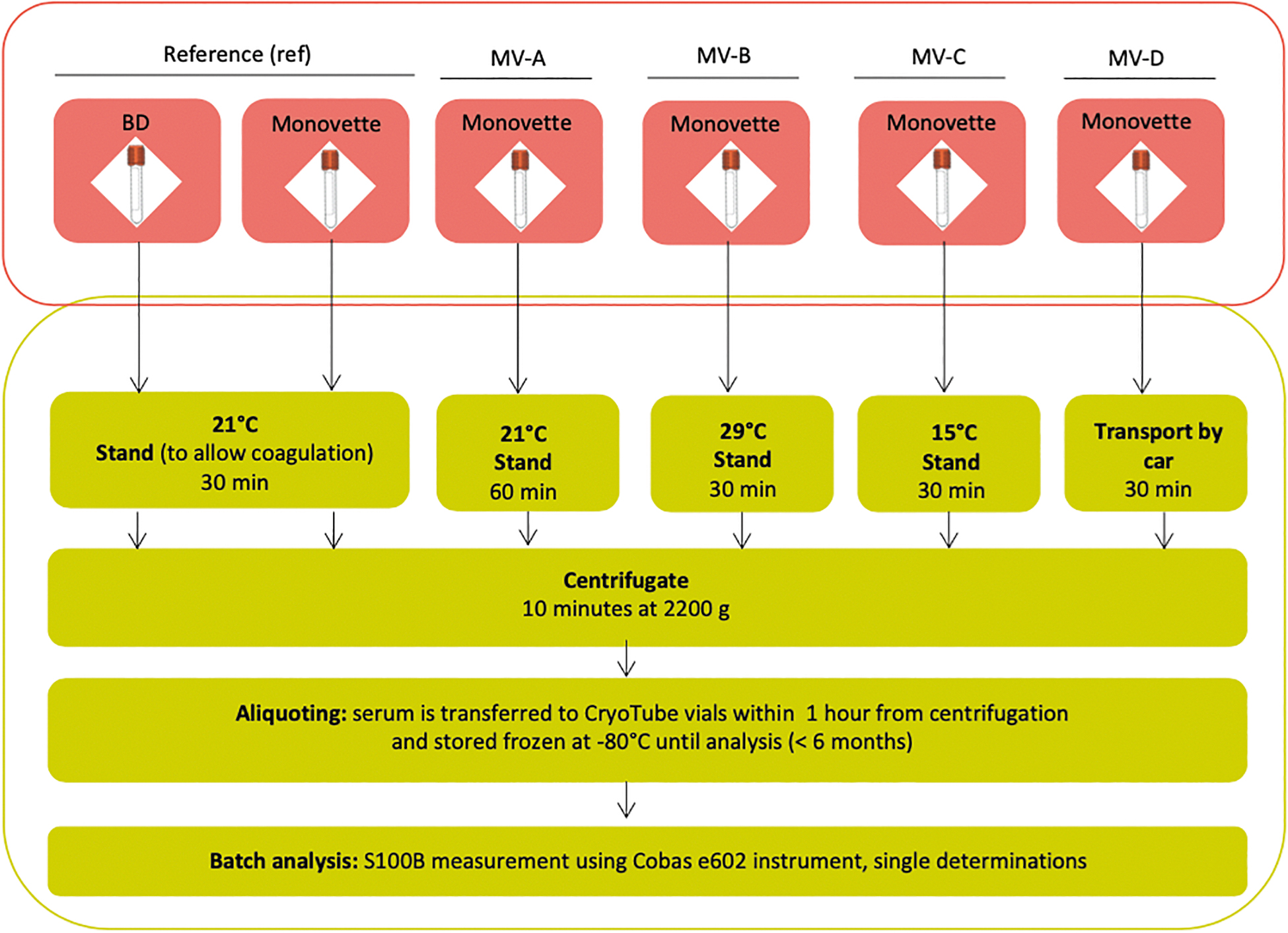
Study design showing the six samples from each patient (one BD tube and five MV tubes) and the different handling before centrifugation, aliquoting, and analysis. BD, Beckton Dickinson Tube®; MV, Sarstedt Serum Monovettes®.
The design allows investigation of the influence of time to analysis, storage temperature, and transport on S100B levels.
Biochemical analysis
All tubes were centrifuged for 10 min at 2200g after 30 and 60 min, respectively. Within 1 h after centrifugation, serum was aliquoted in CryoTube™ Vials and stored at −80°C in a research biobank until blinded batch analysis of S100B in the laboratory using the Cobas 8000 e602 analyzer from Roche Diagnostics (Indianapolis, IN). All blood samples were analyzed for hemolysis, and the HIL index was generated on an Abbott Architect c16000 (Abbott Laboratories, Abbott Park, IL). All biomarker measurements were performed in a single batch, thereby eliminating day-to-day analytical variations and lot variation on test solution.
Outcome measurements
The primary outcome was the mean statistical difference of serum S100B between groups across transport, tubes, time to analysis, and temperature. Secondary outcomes were 1) dichotomized HIL index of all samples within clinical acceptance for usefulness of S100B value (yes/no) and 2) misclassification of patients according to guideline cut-off value of 0.10 μg/L.
Statistical analysis
Sample size was calculated based on pilot data of paired samples, which revealed a correlation between repetitive samples of S100B determined on Roche Cobas e602 of 0.995 and a coefficient of variation of 0.31 yielding a sample size of N = 4 to obtain a power of 0.8 with a significance level of 0.05. It was deemed that a correlation between samples handled under different conditions would probably not exceed 0.9, so to achieve a power of 0.8, a sample size of N = 30 was needed. The sample size was estimated based on guideline cutoff for S100B of 0.10 μg/L with maximum allowable bias at 8.5% based on biological variation data. 9,10
Normality was assessed by inspecting histograms and Q-Q plots of the differences and standardized residuals, resulting in log-transformation of data. Scatter plots and Bland-Altman plots were used to inspect the data. Between-group differences were assessed by paired-samples t-tests or mixed analysis of variance (ANOVA) model with group as fixed effect and patient as random effect. A two-tailed p value of ≤0.05 was considered statistically significant.
Equivalence tests were performed to evaluate the clinical significance of biomarker value variations. Median values were considered equivalent on a 5% level if a 90% confidence interval (CI) for the median ratio was within the equivalence margins ±8.5% (index limits of 1.085; 1/1.085 corresponding to 0.92; 1.085), which represents the maximum clinically acceptable difference. Analyses were performed using Stata software (StataCorp LCC, 2017; Stata statistical software, Release 15; StataCorp LP, College Station, TX).
Ethics
The study was approved by the National Committee on Health Research Ethics (1-10-72-273-18) and is registered at The Danish Data Protection Agency (1-16-02-438-18). The study was performed in accordance with the Declaration of Helsinki. All collected data adhere to current legislation in the Danish Data Protection Act. Patients were not exposed to additional invasive procedures or alteration of treatment. There were no physical or physiological advantages or disadvantages. Participation caused neither patient nor system delay. Participants could, at any time, withdraw from the study. Participants did not receive any compensation or fee for participation in the project.
Results
A total of 30 patients undergoing elective intracranial neurosurgical procedures were included in the study between November 14, 2018 and February 21, 2019. Median age was 63 years, and 46.7% were male. Patient diagnosis was subdivided into six groups based on type of tumor with glioblastoma accounting for 1 of 3 (10 patients; Table 1).
Baseline Characteristics of Patients
IQR, interquartile range.
All six blood samples were successfully drawn and analyzed from each patient. S100B was detected in all samples (n = 180) with a range from 0.025 to 0.484 μg/L. No significant difference was found between median S100B values in BD and MV tubes (Table 2; Fig. 2). No significant difference was found in samples stored at 21°C with prolonged coagulation time (60 min) compared to reference samples. Samples stored at 29°C had 1.8% (90% CI, 0.69; 2.83) higher median values compared to the MV reference; however, values were within the pre-defined equivalence margins (±8.5%) and thereby not clinically relevant. No significant difference was found in the group of samples stored at 15°C with standard coagulation time for 30 min compared to reference samples. S100B values measured in the transported samples had 11.5% (90% CI, 6.55; 16.61) higher median values than the MV reference samples, exceeding the pre-defined equivalence margins and thus being significant.
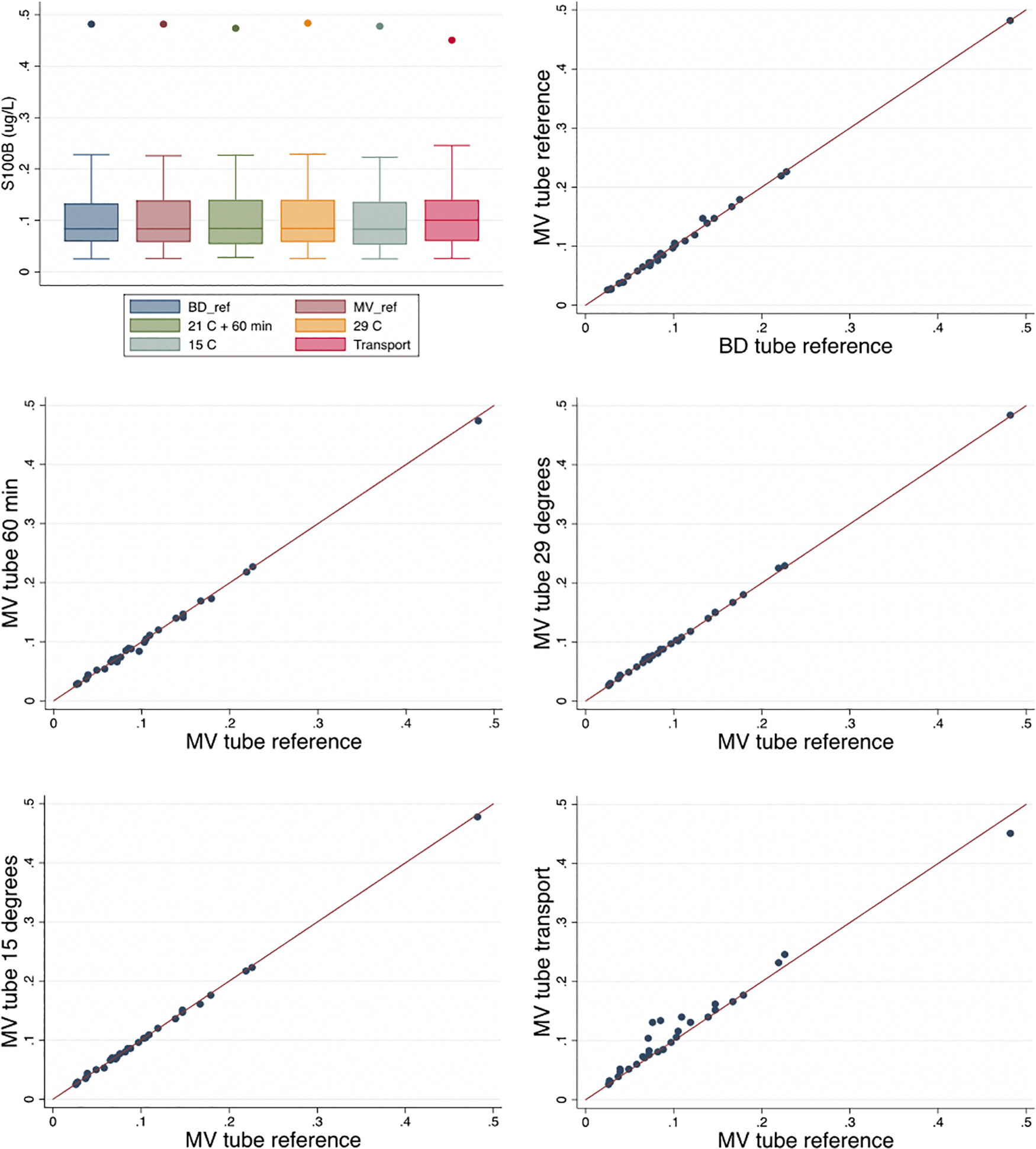
Mean S100B values (μg/L) displayed as box plot (all groups) and scatter plots (each group individually). BD, Beckton Dickinson Tube®; MV, Sarstedt Serum Monovettes®; S100B, S100 calcium-binding protein B.
Median S100B Values in Each Group
S100B, S100 calcium-binding protein B; MV, Monovette; BD, Beckton Dickinson.
By mixed ANOVA analysis, no systematic difference between samples drawn as number 1 through 6 was demonstrated, and S100B values in the transported samples were still significantly different from the MV reference samples.
Median HIL index was measured in all blood samples (Table 3). All sample groups (BD-ref, MV-ref, MV-A, MV-B, MV-C, and MV-D) had an HIL index below the clinical acceptable limit (10g/L). 9 However, the transported sample had a 430% (95% CI, 279.6; 661.4) higher median value compared to the MV reference samples. By ANOVA, we found a positive association between HIL index and S100B values, but when adjusting for HIL index, the transported samples still had significantly higher S100B values compared to reference samples.
Median HIL Index in Each Group
HIL, hemolysis, icterus, and lipemia; MV, Monovette; BD, Beckton Dickinson; IQR, interquartile range.
In 3 of 30 patients, we found false positives, meaning S100B values above cutoff in the transported sample but below cutoff in the reference sample. No false negatives were found.
Discussion
The main findings of this study were a 11.5% (90% CI, 6.55; 16.61) higher median S100B value and a 430% (95% CI, 279.6; 661.4) higher median HIL index in blood samples drawn in MV tubes and transported under simulated pre-hospital conditions compared to reference MV samples stored under standardized conditions (i.e., room temperature, coagulation for 30 min, and no transport).
We demonstrated no significant difference between samples drawn in the standard in-hospital BD tube and the MV tube used in the pre-hospital setting. In two of the MV groups (29°C and transported samples both at standard coagulation time), a statistically significant difference in median S100B values were found compared to the MV reference samples. The 1.8% difference between the 29°C sample and the reference samples was within the pre-defined equivalence limit (±8.5%), but transported samples had a 11.5% higher median S100B value. Based on individual values, using transported samples clinically would translate into a falsely high S100B value leading to false positives in 10% of samples.
As stated in the Introduction, the use of the Scandinavian guidelines could potentially reduce CT examinations with up to 30%. However, it is important to consider adherence to guidelines in this assumption. Recent studies by Minikkinen and colleagues and Ananthaharan and colleagues have shown an overall adherence to guidelines of 80.7% and 63%, respectively, and a general overtriage in patients with mild low-risk TBI. 11,12 In the study by Minikkinen and colleagues, 29% of the mild low-risk group had an S100B < 0.10 μg/L, but only 14.5% were discharged without CT examination. In the study by Ananthaharan and colleagues, 37% of the mild low-risk group had an S100B <0.10 μg/L, but only 20% were discharged without CT examinations. Based on these studies, a high degree of adherence to guidelines is essential to avoid overtriage and reduce CT examinations. To avoid unnecessary overtriage in the pre-hospital setting, adequate adherence to guidelines is required as well.
In concordance with the present study, a previous study by Raabe and colleagues has demonstrated that S100B is unaffected by time to analysis and temperatures as low as 4°C. 10 Although within the equivalence limits, a higher-than-standard temperature that may realistically be observed in an ambulance during summer (29°C) may affect S100B values. Based on the present study, likely not to a clinically relevant degree when isolated to temperature changes only. However, temperatures in the transported samples were not regulated, and a higher temperature and prolonged coagulation may, in combination with transportation, potentially affect S100B values.
A study by Beaudeux and colleagues has shown S100B to be unaffected by hemolysis. 13 In addition, biochemical guidelines allow an HIL index of 10 g/L in samples used for clinical decision making based on S100B measurements. 9 Before conducting the current study, we suspected that the manual vacuum applied by use of the MV tubes may lead to more hemolysis than the BD tube with automated vacuum. No difference was found between the MV reference tube and the BD reference, indicating that the Monovette technique does not induce significantly more hemolysis than the BD tube technique. In all samples, HIL index values were lower than the pre-defined limit for clinical decision making of 10 g/L—the highest value being 1.60 g/L (Table 3). Nevertheless, the transported samples had 4 times higher median hemolysis index compared to the reference samples. This indicates that the higher S100B values observed in the transported samples may, in part, be caused by a higher degree of hemolysis. ANOVA analysis confirmed a positive association between hemolysis and increased S100B, but also showed that hemolysis cannot explain all of the differences observed. However, based on this study, the recommended HIL index of up to 10 g/L may be too high.
Most blood samples had S100B values close to the guideline cut-off limit (0.10 μg/L) used in clinical decision making. One patient had outlying high values (0.451–0.484 μg/L). This patient was the only one diagnosed with oligodendroglioma; otherwise, no differences in baseline characteristics were found.
Considering future point-of-care testing of S100B, the most important factor influencing S100B values seems to be transport rather than differences in tubes, temperatures, or time to analysis. The transportation element will, in part, be eliminated given that blood will be applied directly to the POCT equipment when available. However, for studies analyzing S100B in transported blood samples (
Strengths and limitations
A strength of this study is the design, which allowed us to isolate the potential influencing factors pointed out by the research group before the data collection. Unfortunately, because of practical feasibility, the transported samples were not stored in a thermobox and the temperature was therefore not constant, which is an important limitation that prevents us from concluding on the exact cause of the increase in S100B values noted with transportation.
However, to our knowledge, no other study has investigated the isolated influence of transport and temperatures above room temperature. In addition, our setup mimics the actual work procedure in which blood samples are being transported in the pre-hospital setting. The setup did not allow us to investigate the influence of blood samples being drawn by ambulance personnel in emergent situations rather than laboratory technicians. Further, the blood samples were transported by a regular car obeying traffic regulations and speed limits and therefore not directly comparable to an ambulance. The difference we found in the transported samples in this study may be even greater if samples had been transported by an ambulance.
A previous study by Welch and colleagues has demonstrated S100B levels in neurotrauma patients in the range of 0.07–0.41 μg/L, which compares well to the levels measured in current blood samples (0.03–0.48 μg/L) from the elective patients undergoing neurosurgery, and our data seem generalizable to trauma patients. 14 However, the IQR of our S100B values were 0.05–0.14 μg/L, with only approximately 30% of the values above the values for healthy individuals. This could be a potential limitation to the study, given that S100B levels may vary more in samples with higher S100B values.
Conclusion
Different tubing, variation in temperature, and times to analysis did not clinically impact on S100B values. Blood samples subjected to transport in a simulated pre-hospital setting had higher median S100B values that would clinically translate into a false-positive result in 10% of cases, but no false-negative results.
The findings of this study are promising for the use of pre-hospital POCT in management of TBI patients, given that the transportation element can be eliminated. However, these findings should give rise to precaution in clinical studies based on transported blood samples, and underlines that validation of point-of-care equipment should be carried out in standardized in-hospital settings.
Footnotes
Funding Information
All expenses were held by the Department of Research and Development, Prehospital Medical Services, Central Denmark Region.
No external funding was received.
Author Disclosure Statement
No competing financial interests exist.