
Abstract
Although experience suggests a shift in the epidemiology of spinal cord injury (SCI) toward an older demographic, population studies are lacking. We aimed to evaluate (1) how the epidemiology and age profile of SCI have changed over time, and (2) how increased age impacts health outcomes up to 15 years post-injury. A population-based cohort study was performed in Ontario including adults diagnosed with traumatic SCI between 2002 and 2017. Older and younger SCI cohorts were created based on an age cutoff of 65 years. An older cohort of uninjured persons was matched to the older SCI cohort based on age, gender, and comorbidity status. Changes in crude incidence were reported as average annual percentage change (AAPC). Survival, readmissions, and costs were compared between the older and younger SCI cohorts as well as the between the older SCI and older matched uninjured cohorts. The incidence of SCI increased among females (AAPC 2.2; 95% confidence interval [CI] 0.1, 4.3), driven by a marked rise (4%/year) among elderly females (AAPC 4.3; 95% CI 0.1, 4.3). Although no change in incidence was detected for males, there was a trend toward increased incidence among older males (AAPC 1.2; 95% CI −1.3, 3.8). There were a higher proportion of cervical, incomplete, and fall-related injuries in the older than in younger SCI cohorts. Being over 65 years of age was associated with a sixfold increased risk of death (hazard ratio [HR] 5.75; 95% CI 4.72, 7.00). In comparison with the older uninjured cohort, the older SCI cohort had double the risk of death (HR 2.23; 95% CI 2.00, 2.50). Older persons with SCI had higher odds of readmission and higher costs. The incidence of SCI among the elderly is increasing, particularly among women. Prevention through fall reduction and education to improve outcomes are needed.
Introduction
Traumatic spinal cord injury (SCI) is a devastating event with permanent life-altering consequences for the individual affected and for that person's family and entire support network. 1,2 There is a need to reduce the burden of injury not only through development of improved treatments, but also through implementation of targeted prevention strategies based on an enhanced understanding of injury epidemiology.
Historically, SCI was considered a problem of youth, given that most injuries were encountered among adolescents and young adults as a result of motor vehicle accidents, sport-related trauma, and violence. 3,4 However, increases in life expectancy have led to an expansion of the elderly demographic and an aging of the population. 5 Among the elderly, the combination of poor bone quality and pre-existing spondylosis/spinal stenosis, as well as high propensity for falls, places them at high risk for spinal trauma and SCI. In recent years, several studies have suggested a shift in the epidemiology of spinal trauma toward an older demographic. 6 –10 Such a shift, if present, would have significant implications for primary prevention, injury education, and awareness, as well as for directing the focus of SCI research. However, existing studies are largely based on institutional disease-specific data sets, and hence are poorly suited to informing how changes in epidemiology are occurring at a population level.
In addition, if an increasing proportion of SCI is occurring in the elderly, and this trend is likely to continue, it is important for healthcare providers and administrators to understand the impact of increased age on post-injury mortality, resource utilization, and outcomes, both in the short and long term.
In this population-based study, we evaluated SCI epidemiology and outcomes over a 15-year period in Ontario, Canada. Specifically, we aimed to evaluate (1) how the incidence and age profile of SCI have changed over time, and (2) how increased age impacts short- and long-term health outcomes after SCI.
Methods
A longitudinal population-based cohort study was performed in Ontario between 2002 and 2017. Ontario is the most populous province in Canada, with 14,000,000 residents, accounting for almost 38% of the Canadian population as of 2017. 11 All analyses were based on Ontario administrative health data sets accessed through the Institute of Clinical Evaluative Sciences (ICES). These data sets were linked using unique encoded identifiers and analyzed at ICES. Further details surrounding data sets utilized are included in the Supplementary Text. The use of data in this project was authorized under section 45 of Ontario's Personal Health Information Protection Act, supplanting the need for individual patient-level consent. Research ethics and privacy impact assessment was approved centrally through ICES.
Cohort creation
Primary SCI cohort
All persons who sustained a traumatic SCI in Ontario between April 1, 2002 and March 31, 2017 were identified using the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Canada (ICD-10-CA) codes on discharge abstracts from acute hospitals (Table S1). The codes utilized are considered valid, and are consistent with those used in other epidemiological studies of SCI. 12,13 All records in the Discharge Abstract Database in which an SCI code was the most responsible diagnosis between April 1, 2002 and March 31, 2017 were eligible for inclusion in the primary SCI cohort. Exclusions criteria were being >105 years of age or <16 years of age, having been discharged after March 31, 2017, and having an SCI as a result of a non-traumatic injury or injuries to the cauda equina.
For all subjects, age, sex, income quintile, and rurality were identified using linked census databases. Rurality was measured using the Rurality Index of Ontario and classified as rural, small urban, and large urban. 14 Clinical characteristics were identified using diagnosis codes, including injury level (cervical vs. thoracic vs. lumbar), severity (Injury Severity Scale), completeness (complete vs. incomplete) and cause. To account for pre-injury comorbidity, we utilized the Johns Hopkins ACG® System Version 10 (The Johns Hopkins University) to quantify individuals' healthcare utilization from the year prior to injury. This was then translated into a resource utilization band (RUB) score for each individual, ranging from 0 (no comorbidity/resource use) to 5 (very high comorbidity/resource use). 15
Age-based SCI cohorts. Age-based SCI cohorts were created by identifying all persons from the primary cohort who were ≥65 years or older at time of injury (older SCI cohort) and all patients <65 years of age at injury (younger SCI cohort). Although it is recognized that definitions of “elderly” are shifting, the decision to employ age 65 as the cutoff to define the older cohort was based on definitions employed by Statistics Canada and the United States Census Bureau, both of which use ≥65 years of age as the definition of “elderly.” 16,17
Older uninjured cohort
To compare older individuals with SCI with older uninjured individuals, a cohort of matched controls was created by taking a random sample of all adults in the province >65 years of age without SCI during the study period. From this group, we then matched 4:1 (4 older uninjured persons for every older person with SCI) on age, sex, and RUB. Matching was performed through a “greedy” approach. 18
Outcomes and analyses
Epidemiological analyses
We calculated the gender-specific annual crude incidence of SCI for the years 2002–2017 per million people using the primary SCI cohort and Ontario census data. Annual incidence was calculated as the number of persons with a newly identified SCI between April 1 and March 31 of the following year, divided by the susceptible population. Separate SCI incidence rates were also calculated by year for older (≥ 65 years old) and younger (< 65 years old) individuals. Age standardized rates using an Ontario census population from 2006 were also generated.
Comparative analyses and outcomes
To understand outcomes among older SCI patients, we compared (1) outcomes between the older and younger SCI cohorts, and (2) outcomes between the older SCI cohort and the matched older uninjured cohort.
In these analyses, three central outcomes were considered (1) survival post-injury, including survival rates at 30 days, 1-year, and 10-years; (2) acute care readmissions at 1- and 5-years post-diagnosis; and (3) health system costs from the perspective of the health system payer.
To calculate the public payer costs, patient level costs were computed by identifying each individual's encounters with the health system, and then attaching unit costs to these services through a micro-case costing approach. All direct costs for inpatient acute hospitalization, inpatient rehabilitation, outpatient physician costs, and publicly funded home care were summated for each patient for the 1st year following injury. Details of the macro used to derive costs has been previously published. 19 All costs are in 2018 Canadian dollars.
Statistical analysis
All statistical analyses were performed using SAS 9.4 (SAS Institute Inc., 2013), with the exception of the joinpoint analyses performed using the Joinpoint Regression Program (National Cancer Institute, 2018). Sociodemographic and clinical characteristics of patients within the SCI and matched uninjured cohorts were described using frequencies, counts, and χ 2 tests for categorical variables, and means, t tests, medians, and Kruskal–Wallis tests for continuous variables. All tests were two sided and considered significant at the 0.05 level. A complete case approach was utilized given that the rate of missing data among outcome and predictors variables was <5%.
Joinpoint analyses
Joinpoint regression analysis was used to assess the significance of changes in SCI crude and age-standardized incidence rates. Use of this approach allows for quantification of changes in incidence over time by reporting the average annual percentage change (AAPC) expressed with 95% confidence intervals (CIs).
Survival analyses
Two sets of Kaplan–Meier curves were generated to compare (1) survival in the older SCI cohort with survival in the younger SCI cohort and (2) survival in the older SCI cohort with survival the older uninjured cohort. Corresponding to these, two separate sets of Cox proportional hazards regression analyses were performed with respect to the outcome of death during the study period. In the first set, age at injury, and in the second, presence of SCI (older SCI vs. older uninjured), were considered as covariates of interest. For the first set, unadjusted and adjusted analyses were performed, with adjusted analyses incorporating covariates of known prognostic significance including gender, complete versus incomplete injury, injury level, RUB, income, and rurality. Age was a binary variable (dichotomized at 65) and a continuous predictor. For the second set, only unadjusted analyses were performed given that the older uninjured cohort had been matched to the older SCI cohort. Effect estimates were adjusted hazard ratios with 95% CIs. Proportional hazards assumptions were assessed using Martingale and Schoenfeld residuals, with no violation of assumptions encountered. Death was the only mechanism for censoring of patients.
Examining acute care readmissions
Two separate sets of logistical regression analyses were performed with respect to the binary outcome of acute care readmission post- diagnosis. In the first set, age at injury, and in the second set, presence of SCI (older SCI vs. older uninjured), were considered as the covariates of interest. For the first set, both unadjusted and adjusted analyses were performed, with adjusted analyses incorporating additional covariates known to affect health utilization, including sex, level of injury, completeness of injury, RUB, injury severity score (ISS), income quintile, and rurality. For the second set, only unadjusted analyses were performed given that the older uninjured cohort had been matched to the older SCI cohort on age, gender, and RUB. Effect estimates were expressed as adjusted odds ratios with 95% CIs.
Description of health payer costs of SCI
Costs were analyzed descriptively by examining the means, standard deviations, medians, and interquartile range of inpatient, outpatient, home care, and inpatient rehabilitation costs, and overall health system costs for the younger SCI, older SCI, and older uninjured cohorts. Given the skewness of cost data, Mann–Whitney U tests were used to compare the median costs between the cohorts.
Results
Cohort description
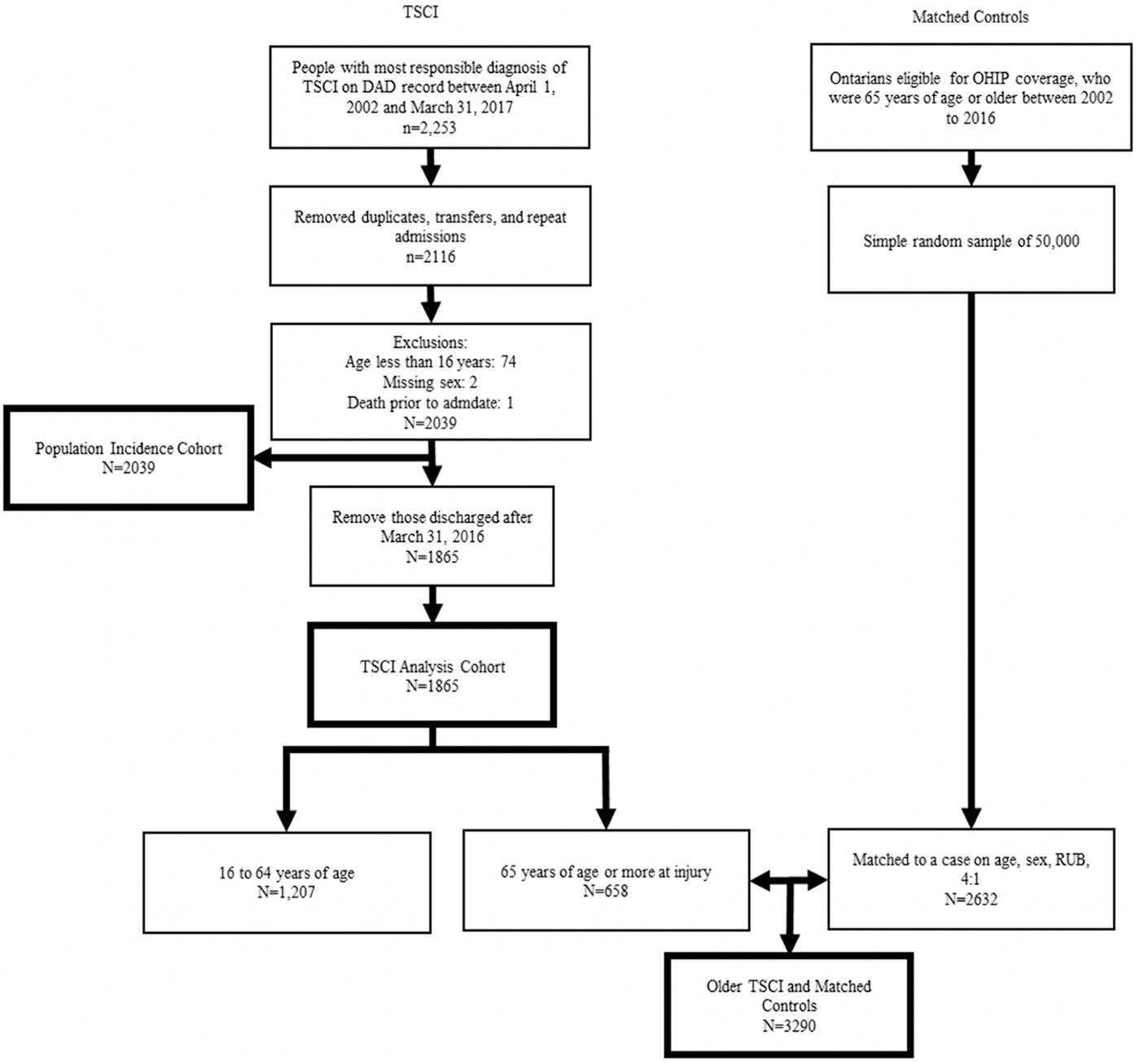
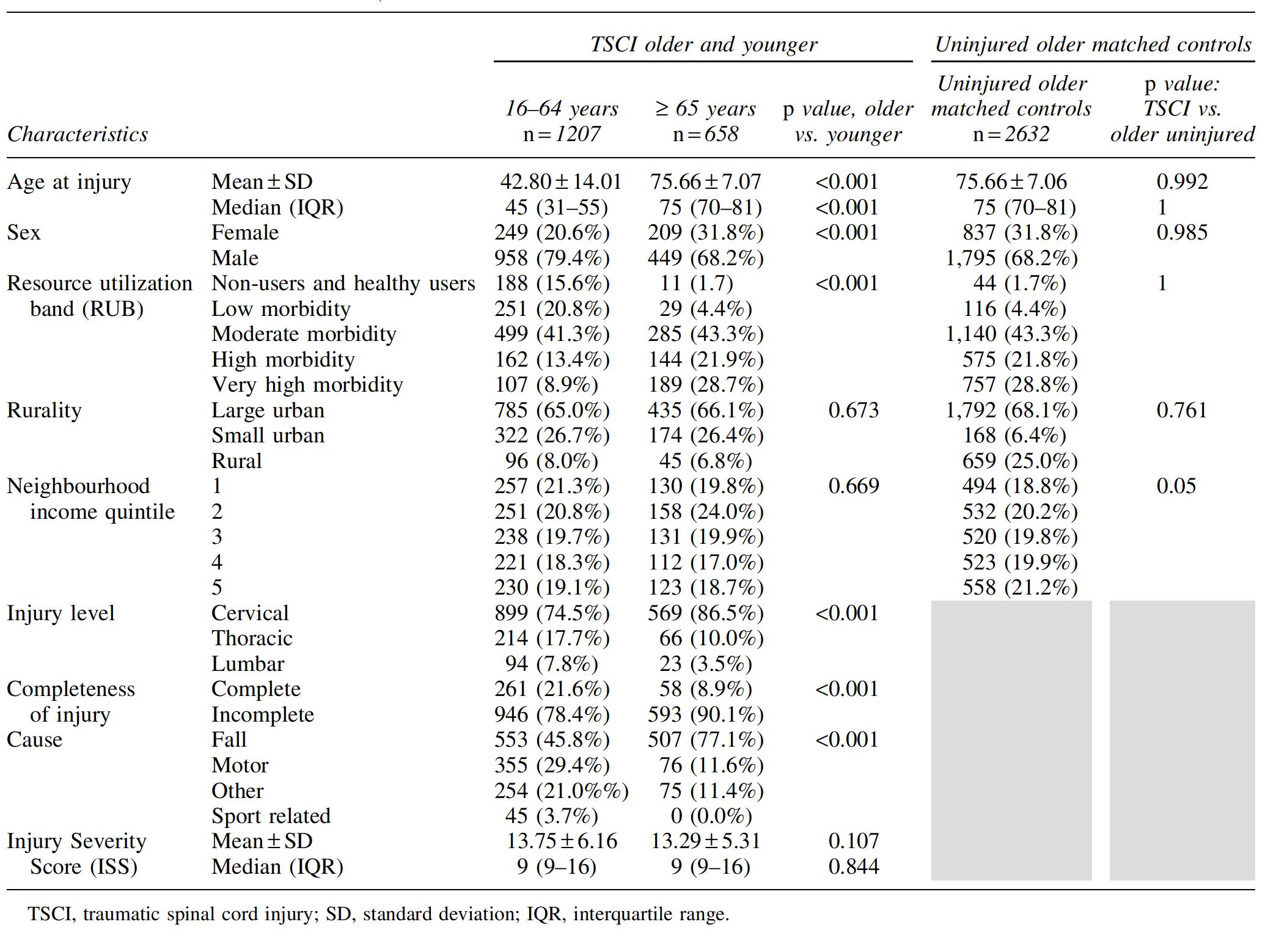
Figure 1 depicts the Consolidated Standards of Reporting Trials (CONSORT) diagram for study cohort creation. Between 2002 and 2017, 1865 people experienced traumatic SCI in Ontario and met eligibility for the primary SCI cohort. Of these, 658 (35.3%) were ≥65 years of age at the time of injury (older SCI cohort) and 1207 (64.7%) were <65 years of age (younger SCI cohort). In the older uninjured cohort, we included 2632 individuals matched 4:1 to patients in the older SCI cohort. Table 1 compares the characteristics of the age-based SCI and uninjured cohorts. There was a higher proportion of women in the older (31.8%) than in the younger (20.6%) SCI cohort (p < 0.01). In addition, there were a significantly higher proportion of patients with cervical level of injuries, incomplete injuries, and fall-related injury mechanisms in the older than in the younger SCI cohort (p < 0.01). There were no significant differences between individuals in the older SCI cohort and those in the older uninjured cohort.
Cohort creation details.
Baseline Characteristics of Patients with TSCI 16–64 Years of Age, and ≥65 Years of Age, and Characteristics of Matched Uninjured Controls
Epidemiological analyses
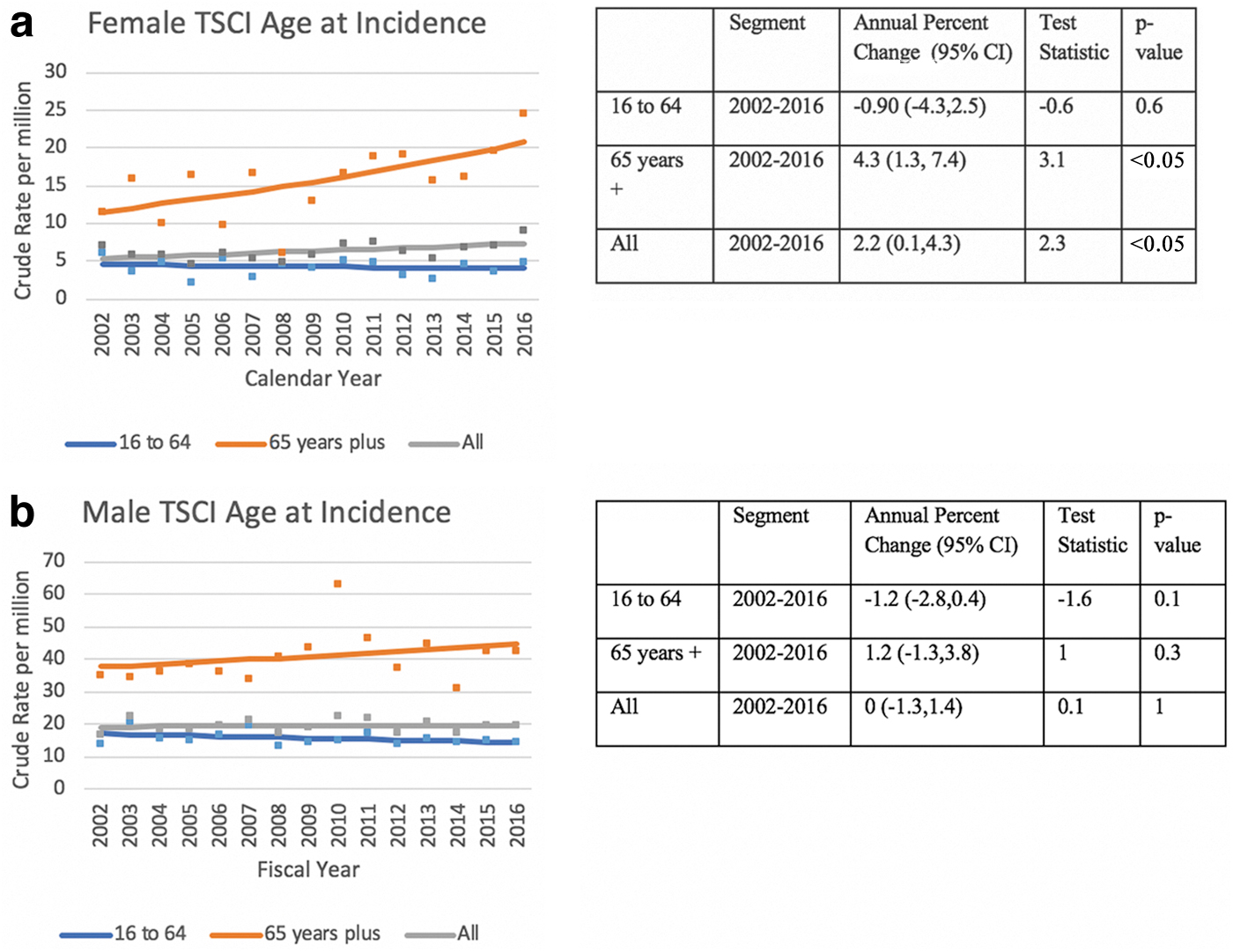
The incidence of SCI in 2002 was 6.93 per million for females and 16.76 per million for males, whereas in 2016 the incidence was 9.07 per million for females and 19.63 per million for males (Table 2). Crude incidence rates among females (Fig. 2a) increased over the study period (AAPC 2.2; 95% CI 0.1, 4.3) but particularly among the older female group, in which incidence increased on average 4% per year (AAPC 4.3; 95% CI 0.1, 4.3). Incidence rates among younger females saw a non-significant decline during the study period (AAPC −0.90; 95% CI −4.3, 2.4). There was no change in incidence for males over the study period (AAPC 0; 95% CI −1.3, 1.4) (Fig. 2b). Among older males there was a trend towards an increase in incidence (AAPC 1.2; 95% CI −1.3, 3.8), whereas there was a trend toward a decrease in incidence among younger males (AAPC 0; 95% CI −1.3, 1.4). After age standardization, there were no significant changes in incidence rates observed in males or females over the study period.
Crude and Age Standardized Incidence, Stratified by Sex, for Fiscal Years 2002–2016
CI, confidence interval.
Survival analyses
Older versus younger SCI cohort
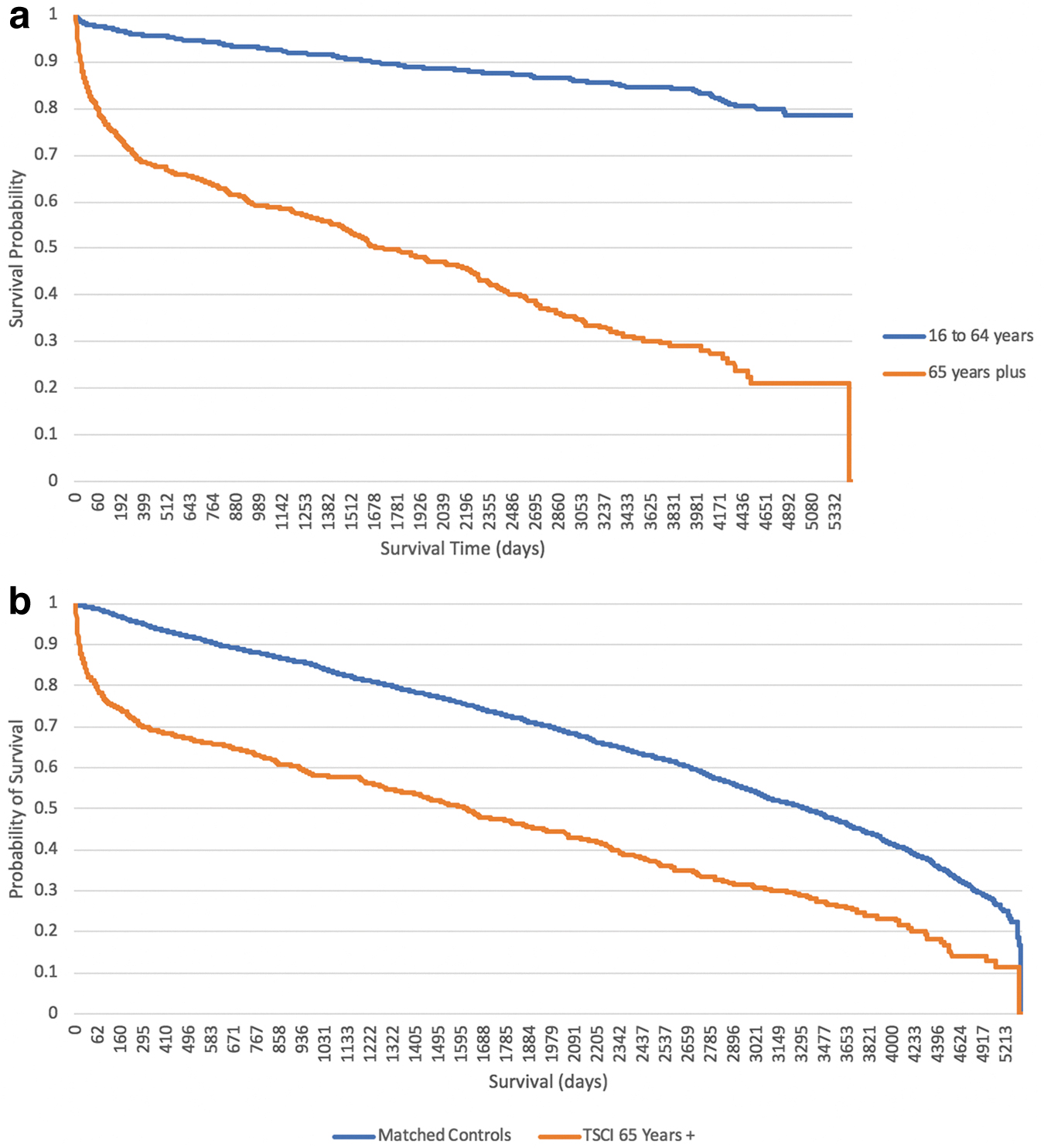
Figure 3a displays the Kaplan–Meier estimator curves for the age-based SCI cohorts. Survival rates among the older SCI cohort at 30 days, 1 year, and 10 years were 83.6% (95% CI 0.806, 0.862), 69.2% (95% CI 0.655, 0.726), and 22.8% (95% CI 0.172, 0.297) respectively. Among the younger SCI cohort, survival rates at these same time points were 97.9% (95% CI 0.9696, 0.9859), 95.9% (95% CI 0.947, 0.969), and 85.7% (95% CI 0.820, 0.887). In unadjusted and adjusted Cox regression analyses, the hazard ratios for death among SCI patients >65 years of age were 6.69 (95% CI 5.61, 7.98) and 5.75 (95% CI 4.72, 7.00) respectively (Table 3) . In both unadjusted and adjusted Cox regression analysis in which age was considered as a continuous variable, the hazard ratios for age was 1.07 (95% CI 1.06, 1.08) (Table 4).
Unadjusted and Adjusted Cox Regression Analysis Evaluating Impact of Age (Treated as Continuous Variable) on Survival after SCI
SCI, spinal cord injury; CI, confidence interval; RUB, resource utilization band; ISS, Injury Severity Score.
Unadjusted and Adjusted Cox Regression Analysis Evaluating Impact of Age (Treated as Binary Variable) on Survival after SCI
SCI, spinal cord injury; CI, confidence interval; RUB, resource utilization band; ISS, Injury Severity Score.
Older SCI versus older uninjured cohort
Figure 3b displays the Kaplan–Meier estimator curves for the older SCI cohort and the matched older uninjured cohort. Survival at 30 days, 1 year, and 10 years in the matched control cohort were 99.3% (95% CI 0.989, 0.996), 94.1% (95% CI 0.931, 0.949), and 44.3% (95% CI 0.406, 0.480), respectively. Compared with the older uninjured cohort, older persons with SCI had a 2.23 increased hazard of death (95% CI 2.00 2.50).
Acute care readmissions
Older versus younger SCI cohort
Among the SCI cohort, 465 patients (29.1%) at 1 year post-injury and 536 patients (51.4%) at 5 years were readmitted to acute care at least once. Of those readmitted, 138 patients (29.7%) at 1 year and 179 (52.0%) at 5 years were readmitted more than once. In adjusted analyses, the odds of readmission were 1.97 (95% CI 1.51, 2.55) times higher at 1 year and 2.26 (95% CI 1.61, 3.18) times higher at 5 years in the older than in the younger SCI cohort (Table 5) . For every additional year of age at injury, the odds of having an acute care readmission were 1.02 (95% CI 1.01, 1.03) times higher in the older than in the younger SCI cohort at 1 and 5 years (Table 6).
Unadjusted and Adjusted Logistical Regression Analyses Evaluating Impact of Age (Treated as Continuous Variable) on Odds of Hospital Readmission at 1 and 5 Years Post-Injury
n = 1042.
OR, odds ratio; CI, confidence interval; RUB, resource utilization band; ISS, Injury Severity Score.
Unadjusted and Adjusted Logistical Regression Analyses Evaluating Impact of Age (Treated as Binary Variable) on Odds of Hospital Readmission at 1 and 5 Years Post-Injury
OR, odds ratio; CI, confidence interval; RUB, resource utilization band; ISS, Injury Severity Score.
Older SCI versus older uninjured cohort
Compared with individuals in the older uninjured cohort, odds for acute care readmission in the older SCI cohort matched were 4.97 times (95% CI 4.02, 6.14) and 3.459 (95% CI 2.49, 4.81) higher at 1 and 5 years, respectively.
Health system costs
The median inpatient, rehabilitation, and home care costs were higher for the older than for the younger SCI cohort, with no differences observed for outpatient costs (Table 7) . The median inpatient, rehabilitation, home care, and outpatient costs were higher for the older SCI cohort than for the older uninjured cohort (Table 8).
Comparison of 1-Year Direct Healthcare Costs between Younger and Older SCI Cohorts
SCI, spinal cord injury; SD, standard deviation; IQR, interquartile range.
Comparison of 1-Year Direct Healthcare Costs between Older SCI and Older Non-Injury Cohorts
Comparison using Mann-Whitney U test.
SCI, spinal cord injury; SD, standard deviation; IQR, interquartile range.
Discussion
Over the 15-year study period, the overall incidence of SCI increased among females. This effect was driven primarily by a rise in SCI rates among elderly females wherein the incidence increased on average by 4.3% per year. In contrast, incidence among younger females experienced a non-significant decline during this period. With respect to males, although there were trends toward increased incidence among the elderly, there were no significant changes in incidence noted over the study period. The older SCI cohort, compared with both younger SCI and matched older uninjured cohorts, had inferior outcomes over the short and long term in terms of increased mortality, hospital readmission rates, and healthcare costs.
Unlike many previous reports that rely on either institutional data sets or a sample of hospitals representing larger groups, the current study is population based and is more likely to accurately depict epidemiological trends over time. Regardless, there seems to be consistency across the literature that SCI among the elderly is on the rise. In analyzing the United States national inpatient sample, Jain and coworkers reported that although the overall incidence of SCI (including injuries to the cauda equina) was unchanged between 1993 and 2012, rates among the elderly had markedly increased, and rates among the young had declined over the same time period. 12 Analysis of national SCI registries from Scotland, Finland, Spain, and Iceland have also reported higher incidence of SCI among the elderly, primarily in the context of fall-related injuries. 8,9,20 –22 When considering the drivers of this epidemiological shift, several factors are likely at play; namely, increased life expectancy coupled with the increased incidence of osteoporosis, spinal stenosis, and high propensity for falls among the elderly.
The current study is one of the first to demonstrate a particular rise in the rate of SCI among elderly women. Perhaps, the known association between female sex and increased risk of osteoporotic fractures may partially explain this finding. Previous research indicates that at age 60, the lifetime risk of fracture for females is nearly double the risk of fracture for males (44% vs. 25%, respectively). 23,24 It is therefore possible that a similar trauma experienced by females may lead to higher rate of spinal fracture and subsequent SCI than males. That said, a significant proportion of SCI among the elderly occurs without fracture, and as a result, there may be an additional explanation for the observed findings, which should be explored in future research studies.
The increased risk of death among the elderly SCI cohort in the current study largely comports with findings from previous registry-based analyses. Furlan and coworkers, in an analysis of data from the National Acute Spinal Cord Injury Study (NASCIS) III study, associated each additional year of age at time of injury with an additional 8% risk of death, with Strauss and coworkers, in an analysis of data from the United States National Spinal Cord Injury Statistical Center database, finding an additional 7% risk of death per year of increase in age. 6,25 The cause for this finding is likely to be multifactorial; whereas elderly patients, by virtue of increased frailty and reduced physiological reserve, may be at higher risk for the development of secondary complications post-SCI, it is also possible that elderly patients receive less aggressive treatment in the way of surgical and intensive care unit management because of a perception of futility when such a serious diagnosis is encountered late in life. 26 As evidence of this, Ahn and coworkers and Wilson and coworkers have shown that elderly patients are less likely to undergo surgery within 24 h post-injury, a treatment known to improve clinical outcomes post-SCI. 27,28
In the current study, elderly SCI patients also had higher rates of hospital readmission at 1 and 5 years, and had higher direct healthcare costs related to acute inpatient, home care, and rehabilitation. Although previous analyses have not demonstrated age to be an important factor in predicting treatment-related costs, many of these have focused on one specific phase of acute care, rather than considering comprehensive evaluation of healthcare expenses in the 1st year after injury. 29,30 We speculate that the higher costs documented among the elderly are at least partially explained by higher rates of medical complications as well as longer duration of inpatient stay among the elderly with SCI, as has been established by previous studies.
From a prevention standpoint, this study highlights that there is a need for targeted prevention efforts surrounding fall reduction in the elderly, particularly among females, to help avert further rise in SCI among this demographic. Although the impact of falls as it pertains to hip and extremity fractures is well publicized and researched, fall-related SCI in the elderly is less discussed. Increased awareness and education on this topic, coupled with the development of spine-protective interventions/strategies for the elderly, are warranted. From a quality improvement standpoint, although a certain proportion of the increased mortality observed among elderly persons with SCI may be unavoidable, it is important to ensure that these patients have timely access to specialized care. To this end, there is a need for enhanced education among healthcare professionals surrounding SCI in the elderly, reinforcing the importance of early diagnosis and triage to a specialized SCI center for definitive care.
Limitations
The use of administrative data limited the availability of disease-specific data elements. As an example, findings from a detailed neurological examination, as well as functional and quality of life related data points, were not available. Second, in determining 1 year healthcare costs, only direct costs were considered, as data enabling the calculation of indirect costs were not available. Third, it is possible that a small fraction of individuals (< 5%) within the cohorts may have migrated away from Ontario during follow-up, leading to non-differential misclassification of outcome. Fourth, this analysis relied on the identification of persons with SCI through use of ICD-10 codes. Although previous studies have found these codes to be appropriate for use, it is acknowledged that these codes are not perfect, and that some patients may have been incorrectly included or excluded from the analysis. Finally, it is acknowledged that the decision to employ a cutoff age of 65 to define young versus older cohorts is somewhat arbitrary from a biological perspective. That said, this cutoff has societal relevance, and it is presently used by governments in both Canada and the United States as a threshold to define elderly.
Conclusion
This 15-year longitudinal cohort study has shown that incidence of traumatic SCI seems to be increasing among the elderly, particularly among females. Compared with younger persons with SCI, as well as with matched uninjured elderly persons, elderly persons with SCI had higher rates of mortality and of hospital readmission at 1 and 5 years, and higher healthcare costs. These results highlight the need for improved prevention strategies targeting fall reduction in the elderly, as well as quality improvement initiatives targeting improvements in the timely diagnosis and care of the elderly with SCI. Given the additional care burden associated with SCI in this age group, it is important for healthcare providers and administrators to recognize the need for increased resources to provide appropriate levels of care for this growing demographic of patients.
Footnotes
Acknowledgment
The opinions, results, and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred. Parts of this material are based on data and/or information compiled and provided by Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed in the material are those of the author(s), and not necessarily those of CIHI.
Funding Information
This work was supported by a Young Investigators Award from the Neurosurgery Research and Education Foundation. This study was performed through use of data sets housed at ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.