
Abstract
Children and adolescents with traumatic brain injury (TBI) can experience impaired self-awareness, or difficulty in accurately perceiving their personal abilities. This study aimed to identify the neuro-developmental and socio-environmental factors associated with self-awareness impairment and determine how self-awareness is associated with psychosocial functioning. Parents and their children age 8–16 years with TBI (n = 107, 65.4% male, mean [M] age = 12.66 years, standard deviation [SD] = 2.6 years) were consecutively recruited from an outpatient clinic over a 4-year period. Children completed the Paediatric Awareness Questionnaire (PAQ) to report their functional abilities, and the Beck Youth Inventories to report their self-concept, and anxiety and depression symptoms. Parents completed the PAQ and measures of family functioning, parenting style, and children's emotional and behavioral problems. Self-awareness impairments were defined as more negative parent-child discrepancy scores on the PAQ. Younger age at injury, more severe injury, and more family dysfunction were significantly associated with poorer self-awareness. Poorer self-awareness was associated with worse parent-rated child adaptive functioning and emotional and behavioral problems. However, poorer self-awareness was also significantly associated with more positive self-concept and fewer symptoms of depression and anxiety as rated by children. Overall, impaired self-awareness seems to be both a liability and a benefit depending on the reporter (parent or child) and outcome of interest (adaptive function/behavior or self-concept/mood).
Introduction
Children and adolescents with traumatic brain injury (TBI) can experience varying difficulties with physical, cognitive, emotional, social, and adaptive functioning. 1 –4 The significant variability in long-term outcomes has been attributed to a complex interplay of developmental, injury-related, and socio-environmental factors. 1,4,5 In general, developmental and injury-related factors appear to contribute most strongly to cognitive outcomes, 2 whereas socio-environmental factors have been found to have a greater influence on emotional and behavioral outcomes following pediatric TBI. 6 –8 These factors can have independent or synergistic effects on outcome. 1,4 In general, children with more severe TBI, earlier injury onset, and greater social disadvantage are more vulnerable to poor long-term functional outcomes. 1 Given that TBI can derail children's typical developmental trajectory, it is essential to understand how children and their parents perceive their post-injury impairments, and how discrepancies in these perceptions (i.e., impaired self-awareness) influence functional outcomes and psychological well-being. Such knowledge could inform novel interventions targeting children's self-perceptions throughout rehabilitation.
Impaired self-awareness refers to the tendency to overestimate one's functioning and is a key predictor of poorer long-term vocational and social outcomes after TBI in adulthood. 9 In contrast to research on self-awareness following TBI in adulthood, self-awareness after pediatric TBI has mainly received attention in research over the last decade. 10 –12 A systematic review by Lloyd and colleagues 13 identified 12 studies that employed relevant methodology for assessing impaired self-awareness. Overall, the review identified that children and adolescents with moderate to severe TBI displayed impaired self-awareness in relation to memory, executive functioning, and communication skills. There was some evidence that poorer self-awareness was associated with greater severity of TBI, 14 –16 but mixed findings concerning the influence of time since injury on self-awareness. 14 –17 Only one study examined the relationship between self-awareness and psychosocial outcomes, with better self-awareness found to be associated with lower self-esteem, 18 which is consistent with the adult literature. 19
Neuro-developmental factors related to self-awareness
Various injury-related factors have been found to influence self-awareness following TBI in adulthood. In particular, self-awareness has been found to improve with time since injury, which has been attributed to neuro-cognitive recovery and individuals' experiences of resuming familiar activities and learning about their functional limitations. 20 –22 Although some findings from the adult TBI literature may be applicable to children, the influence of neuro-developmental factors on self-awareness is particularly important to consider. There is now substantial evidence supporting the early vulnerability theory that children injured at a younger age, while the brain is in a state of rapid development, experience poorer neuro-cognitive outcomes. 23,24 In a pilot study investigating the reliability and validity of the Paediatric Awareness Questionnaire (PAQ), Lloyd and colleagues 12 found that children with TBI (n = 32) were more likely than typically developing controls to overestimate their functioning relative to parents' reports. In line with the early vulnerability theory, children who sustained their TBI at a younger age demonstrated poorer self-awareness than children injured at an older age.
Brain maturation processes and associated cognitive developments (e.g., autobiographical memory, self-monitoring, and perspective-taking skills), along with an increase in peer-based comparisons, are theorized to contribute to more realistic self-appraisals throughout childhood. 25,26 A severe TBI is likely to disrupt the emergence of cognitive skills that support the development of self-awareness. 27 Wolfe and associates 28 found that children with severe TBI showed poor self-awareness of their social functioning relative to peer judgments. More impaired executive functioning was associated with poorer self-awareness, which in turn was related to lower parent-rated social adjustment. These findings suggest that impaired self-awareness affects children's social competency or ability to relate to their peers.
Socio-environmental factors related to self-awareness
An important factor overlooked in pediatric TBI and self-awareness research to date relates to the influence of children's family environment. Parenting style (e.g., responsiveness and negativity) has been found to significantly influence behavioral adjustment after pediatric TBI. 8 Behavioral problems are more likely to emerge over time for children with severe TBI when they experience a parenting style that is authoritarian (low in warmth and responsiveness but high in limit-setting, discipline, and demandingness) or permissive (high in warmth and responsiveness but low in limit-setting, discipline, and demandingness), as opposed to authoritative (high in warmth, responsiveness, limit-setting, and demandingness). 8,29,30 According to findings from the adult literature, 31,32 self-awareness of functional changes develops when individuals receive sensitive and responsive feedback on tasks that pose the right level of challenge, in a manner that promotes independence and self-regulation. Parenting style and broader family interaction patterns (e.g., communication, affect, and behavior regulation) potentially affect how children receive feedback on and learn about their post-injury impairments, thus influencing their self-awareness.
Overall, preliminary research in the pediatric TBI literature suggests that younger age at injury and more severe injury is associated with poorer self-awareness. 12,13 However, these studies typically had small samples and did not examine socio-environmental factors and psychosocial outcomes related to self-awareness. In the only two studies to have examined psychosocial outcomes, poorer self-awareness was related to higher self-reported self-esteem, 18 but worse social functioning as rated by parents. 28 This is consistent with research on adults with TBI, demonstrating that poorer self-awareness was associated with lower emotional distress on self-reports but less favorable long-term functional outcomes (independence, work, and relationships) as rated by relatives. 20
The current study had two aims. The first aim was to identify neuro-developmental (i.e., age at injury, severity of injury, and time since injury) and socio-environmental (i.e., family functioning and parenting style) factors associated with self-awareness following pediatric TBI. Regarding neuro-development, it was hypothesized that children and adolescents with poorer self-awareness would have a younger age of injury, have more severe injury, and have less time since injury. Regarding socio-environmental influences, it was expected that children and adolescents with poorer self-awareness would have more authoritarian and permissive parenting and more family dysfunction.
The second aim was to investigate the relationship between self-awareness and the psychosocial outcomes of adaptive, emotional, and behavioral functioning. It was hypothesized that children and adolescents with poorer self-awareness would have worse adaptive functioning and more emotional and behavioral problems as rated by parents. Conversely, it was hypothesized that children and adolescents with poorer self-awareness would self-report fewer symptoms of depression and anxiety and more positive self-concept.
Methods
Participants
Children with TBI and their parents were recruited based on consecutive appointments between February 2016 and June 2019 at outpatient clinics at the Queensland Paediatric Rehabilitation Service at the Queensland Children's Hospital, in Brisbane, Australia. Children were initially screened by treating clinicians to determine whether they met the following inclusion criteria: age 8–16 years, a medical diagnosis of TBI, medically stable (including not in post-traumatic amnesia [PTA]), and sufficient cognitive and language abilities to complete the questionnaires. Children were excluded from the study if they had a prior history of a psychiatric or neurological disorder, a developmental disability, or a background of suspected abuse or neglect, as identified by medical records, discussion with treating clinicians, and self-report. Children were also excluded if they or their parents had significant, current mental health concerns or acute distress that precluded them from completing questionnaires. Further, children were excluded from the study if either the parent or child PAQ was not completed, due to the relevance of this self-awareness measure to all analyses.
Measures
Self-awareness
Children and their parents completed the child and parent versions of the PAQ. 12 The PAQ is a 37-item measure used to assess in children (children and adolescents, age 8–16 years) competency across a range of functional areas typically affected by TBI, including cognition, physical functioning, activities of daily living, interpersonal skills, and emotional/behavioral status. Consistent with the Patient Competency Rating Scale 33 developed for adults, the child with TBI and a significant other rate the ease with which the child is currently able to perform functional activities, using a 6-point Likert-type scale (“Can't do” = 1, “mostly hard” = 2, “a bit hard” = 3, “a bit easy” = 4, “mostly easy” = 5, “very easy” = 6). Example items include: “I can get through all activities in a day without feeling tired,” “I can wait to let others take their turn,” and “I can calm myself down when I am feeling angry.” Ratings on each item are summed to yield a total score ranging from 37 to 222, with a higher score indicating more positive functioning.
An awareness discrepancy score is calculated by subtracting the child's total score from the parent's total score, with a larger difference (either negative or positive) reflecting more discrepancy in ratings. A negative discrepancy score indicates that the child typically rated his or her functioning as higher relative to the parent. Thus, a lower (i.e., more negative) discrepancy score indicates more impairment. Scores in the current study ranged from −101 to 49. Psychometric properties of the PAQ have previously been reported, 12 with the measure demonstrating excellent internal consistency, test-retest reliability, and evidence of known groups and convergent validity. For the current sample, internal consistency of the PAQ items was excellent for the parent (α = −0.96) and child (α = 0.95) versions, and for the discrepancy score (α = 0.93).
Demographic and injury characteristics
Parents completed a socio-demographic background questionnaire detailing the child's age,sex, ethnicity, parental education, and household income. Injury characteristics were collected via review of medical records; these included date and age at injury, cause of injury, lowest Glasgow Coma Scale (GCS) score, and duration of PTA. Imaging (computed tomography [CT] or magnetic resonance imaging [MRI]) data were also obtained from medical records when available.
Socio-environmental factors
The socio-environmental factors assessed included family functioning and parenting style. To measure family functioning, parents completed the 12-item general functioning scale of the McMaster Family Assessment Device (FAD). 34 Each item is rated on a 4-point scale (1 = “strongly agree” to 4 = “strongly disagree”), with composite scores formed by averaging all items, whereby a higher score represented more family dysfunction. The FAD is commonly used to assess family functioning after TBI. 30,35
To measure parenting style, parents completed the Parenting Practices Questionnaire (PPQ), 36 a 62-item measure that assesses authoritarian (27 items), authoritative (20 items), and permissive (15 items) parenting. Each item is rated on a 5-point scale (1 = “never” to 5 = “always”). Total scores were used for each dimension, with higher scores indicating more authoritarian, authoritative, or permissive parenting. Scores could range from 87 to 143 for the Authoritarian scale, 26 to 65 for the Authoritative scale, and 20 to 50 for the Permissive scale. The measure has satisfactory reliability and validity, 37 and has been used previously in pediatric TBI research. 30,35
Adaptive behavior
Parents completed the Adaptive Behavior Assessment System, third edition (ABAS-3) 38 parent/primary caregiver form (age 5–21 years). The ABAS-3 is a 232-item questionnaire that measures the child's current functional status or daily living skills across three domains (conceptual, social, and practical) that reflect the following skill areas: communication, community use, functional academics, health and safety, home or school living skills, leisure, self-care, self-direction, and social functioning. The ABAS-3 has sound reliability, including internal consistency (α = 0.98–0.99), and test-retest reliability (r = 0.90). 38 Convergent validity with other measures of functional status has been demonstrated. 38 All items were summed to produce a global adaptive composite (GAC) score, whereby higher scres indicated more adaptive behavior.
Emotional and behavioral functioning
Children completed the self-concept, anxiety, and depression scales from the Beck Youth Inventory, second edition (BYI-2). 39 The scales each consist of 20 items and were designed for children age 7 to 18 years. Children rate how frequently each item typically applies to them on a 4-point Likert scale (0 = “never” to 3 = “always”). Lower scores on the depression and anxiety scales and higher scores on the self-concept scale reflect better emotional well-being. Raw scores are converted to T scores based on age and sex norms. 39 The three scales have excellent internal consistency (α = 0.89–0.95), acceptable test-retest reliability (r = 0.77–0.92), and good evidence of convergent validity. 39
Parents completed the Child Behavior Checklist (CBCL), 40 a 113-item questionnaire assessing children's internalizing and externalizing behavior. The CBCL total scale represents a global measure of behavioral functioning, with higher scores reflecting more behavioral difficulties. The CBCL has excellent internal consistency (α = 0.78–0.97), test-retest reliability (r = 0.90), and inter-rater reliability (r = 0.93) and is frequently used with pediatric brain injury populations. 35,40,41
Procedure
The study was approved by the Children's Health Queensland Human Research Ethics Committee and the Griffith University Human Research Ethics Committee. Children with TBI were screened for eligibility and recruited to the study from outpatient clinics by treating health professionals. Children and their parents were provided with information on the study, and both the parent and child were asked to provide informed consent. Following consent procedures, children and parents independently completed the PAQ.
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences, version 24. Data were missing on the complete measure of the ABAS-3 (n = 8), PPQ (n = 7), CBCL (n = 4), and the FAD (n = 2); and the Self-Concept scale (n = 4), and the Anxiety and Depression scales (n = 2) of the BYI-2. Data were found to be missing completely at random, according to Little's test. 42 Missing data were managed using a pairwise deletion approach in relevant analyses.
Chi-Square tests and t tests were used to compare the demographic and injury characteristics of children who participated in the study and those who were eligible but did not participate. Pearson's correlation and multiple regression analyses were conducted to examine associations between neuro-developmental and socio-environmental variables and self-awareness. The same analyses were used to examine the associations between self-awareness and adaptive behavior and psychosocial outcomes.
In terms of sample size considerations, for the first aim concerning neuro-developmental and socio-environmental factors (10 independent variables) associated with self-awareness, a minimum participant to variable ratio of 10:1 was deemed appropriate for the regression analysis, thus requiring at least 100 participants. For the second aim, it was of specific interest to determine whether self-awareness accounted for significant variance in adaptive behavior and psychosocial outcomes after controlling for relevant neuro-developmental and socio-environmental factors (e.g., sex, severity of injury, age at injury, time since injury, parental education, family functioning, and parenting styles [authoritatrian, authoritative, and permissive]). A power analysis was conducted using G*Power 43 with a small to medium effect size (change in R2 = 0.08) anticipated for the additional variance accounted for by self-awareness. A sample size of 93 participants would have 80% power to detect significant associations (p < 0.05) between self-awareness and adaptive behavior and psychosocial outcomes, controlling for relevant covariates.
Results
Sample characteristics
Figure 1 shows that after screening, 216 children with TBI met the eligibility criteria during the recruitment period. Of these, 21 families were unable to be contacted following initial screening, and 88 declined participation in the study or withdrew prior to completing relevant measures. The final sample consisted of 107 children with TBI (65% male; mean [M] age = 9.43 years, standard deviation [SD] = 4.5). Demographic and injury characteristics of the sample are summarized in Table 1. Children were on average 3.23 years post-injury and age 9.43 years (SD = 4.5) at the time of injury. Age at injury was categorized into five groups (i.e., infancy; early, middle, and late childhood; and adolescence) based on age at injury, consistent with previous pediatric TBI studies. 23,41 Injury severity was classified as mild, moderate, or severe, based on the lowest GCS score in the first 24-h post-injury (note: for injured children under age 5 years, the pediatric version of the GCS was used), 44 PTA duration, or both indices, with injuries classified according to the index indicating more severe injury. Most children had sustained a severe TBI (46.7%) with neuroimaging results indicating diffuse or multi-focal injuries for approximately half of the sample (51.4%).
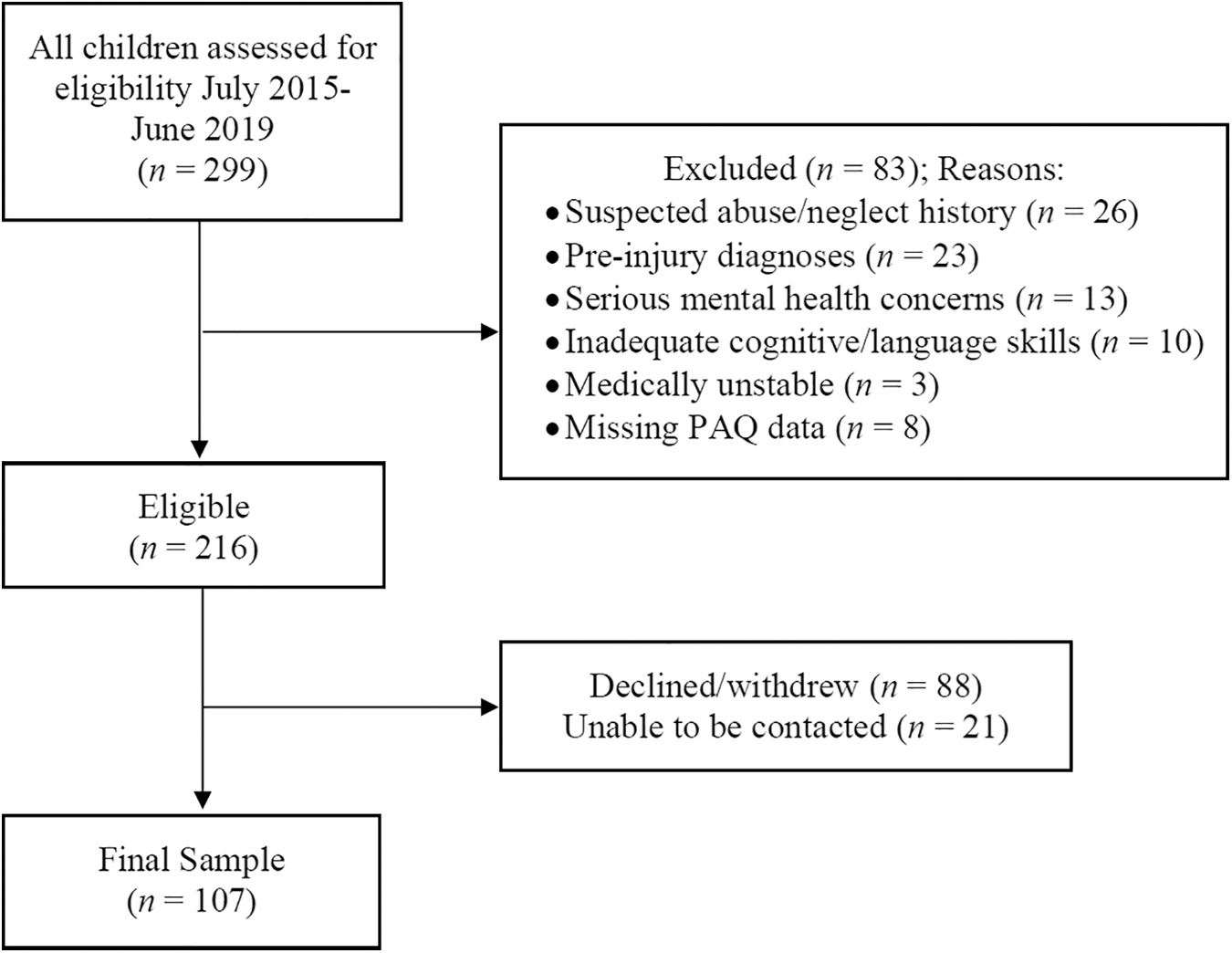
Participant recruitment flow diagram. PAQ, Paediatric Awareness Questionnaire.
Demographic and Injury Characteristics for the Sample
Bosnian, Chilean, Zimbabwean.
Household income was coded as: 1 = <$40,000, 2 = $40,000–$60,000, 3 = $60,001–$80,000, 4 = $80,001–$100,000, 5 = $100,001–$120,000, 6 = $120,001–$140,000, 7 = $140,001–$160,000, 8 = $160,001–$180,000, 9 = $180,001–$200,000, 10 = >$200,000.
M, mean; PTA, post-traumatic amnesia; SD, standard deviation.
A comparison of the current sample (n = 107) and children who were eligible but did not participate or who did not have both child and parent PAQs completed (n = 117) indicated no significant differences in terms of sex, χ 2 = 0.06, p = 0.82; ethnicity (classified as Caucasian vs. non-Caucasian), χ 2 = 2.44, p = 0.51; age at assessment, t(209) = −0.01, p = 0.99; age at injury, t(220) = −0.02, p = 0.98; or GCS score, t(162) = 1.01, p = 0.31.
Descriptive data
As shown in Table 2, on average, children rated their functioning as better than rated by their parents, resulting in a negative discrepancy score (M = −10.81, SD = 29.5), which indicated impairment in self-awareness. Children's adaptive behavior ranged from extremely low (GAC score = 50) to high average (GAC score = 120). Levels of adaptive functioning significantly differed according to injury severity: F[2, 96] = 8.87, p < 0.001, np 2 = 0.16. Children with mild TBI had better adaptive functioning (M = 102.2, SD = 16.78) than those with moderate TBI (M = 87.61, SD = 14.52, p = 0.001) and those with severe TBI (M = 87.85, SD = 15.48, p < 0.001). On the CBCL, 41.8% of children were in the clinical range (T ≥ 64) for the total score, 42.7% for the internalizing scale, and 27.2% for the externalizing scale. There were no significant differences in overall emotional and behavioral symptoms (CBCL total) according to severity of injury: F[2, 100] = 1.66, p = 0.20, np 2 = 0.032. The proportion of children with clinically elevated internalizing symptoms was 35.5% for those with mild TBI, 50% for those with moderate TBI, and 43.8% for those with severe TBI (χ 2 = 1.2, p = 0.55). The proportion of children with clinically elevated externalizing symptoms was 16.1% for those with mild TBI, 33.3% for those with moderate TBI, and 31.3% for those with severe TBI (χ 2 = 2.78, p = 0.25).
Descriptive Data for All Measures
ABAS-3, Adaptive Behavior Assessment System, third edition; BYI-2, Beck Youth Inventory, second edition; CBCL, Child Behavior Checklist; FAD, McMaster Family Assessment Device; M, mean; PAQ, Paediatric Awareness Questionnaire; PPQ, Parenting Practices Questionnaire; SD, standard deviation.
Self-ratings on the BYI-2 indicated that 16.5% of children were in the clinical range (T > 60) for depression, 21.0% were in the moderate to severely elevated range (T > 60) for anxiety, and low self-concept (T < 40) was evident for 23.8% of children. Level of self-concept, anxiety, or depression did not differ according to severity of injury (respectively, F[2, 102] = 0.33, p = 0.72, np 2 = 0.006; F[2, 102] = 0.32, p = 0.73, np 2 = 0.006; F[2, 100] = 0.04, p = 0.96, np 2 = 0.001).
Factors associated with self-awareness
As can be seen in Table 3, younger age at injury, longer time since injury, lower GCS score, and greater family dysfunction were significantly associated with poorer self-awareness. Notably, in this sample longer time since injury was strongly associated with younger age at injury, due to the outpatient clinic providing long-term support to children injured at a very young age. There were no significant associations between self-awareness and age at assessment, duration of PTA, years of parental education, and parenting styles.
Correlations between Self-Awareness (PAQ Discrepancy Score) and Neuro-Developmental and Socio-Environmental Factors
Transformed to address normality violation.
p < 0.05, ** p < 0.01, *** p < 0.001.
FAD, McMaster Family Assessment Device; GCS, Glasgow Coma Scale; PAQ, Paediatric Awareness Questionnaire; PPQ, Parenting Practices Questionnaire; PTA, post-traumatic amnesia.
Given the significant association between age at injury and self-awareness, a one-way analysis of covariance (ANCOVA) was conducted to compare age at injury groups, controlling for time since injury. There was a significant overall effect of age at injury on self-awareness: F[4, 101] = 3.28, p = 0.014, np 2 = 0.12 (see Fig. 2). The covariate of time since injury was not significant (p > 0.05). Post hoc tests with an adjusted alpha (p < 0.01) revealed that children injured during infancy had significantly poorer self-awareness (M = −38.87, SD = 20.64) than those injured during middle childhood (M = −4.44, SD = 26.79; t[38] = −4.47, p < 0.001), late childhood (M = −8.32, SD = 23.24; t[30] = −3.91, p < 0.001), and adolescence (M = 0.97, SD = 28.28; t[42] = −5.21, p < 0.001). Further, children injured during the pre-school years (M = −23.71, SD = 31.84) had significantly poorer self-awareness than those injured during adolescence (t[46] = −2.77, p < 0.01). However, there was no significant difference in self-awareness between children injured during infancy and those injured during pre-school years (p > 0.01), or between groups of children injured during middle childhood, late childhood, and adolescence (p > 0.01).
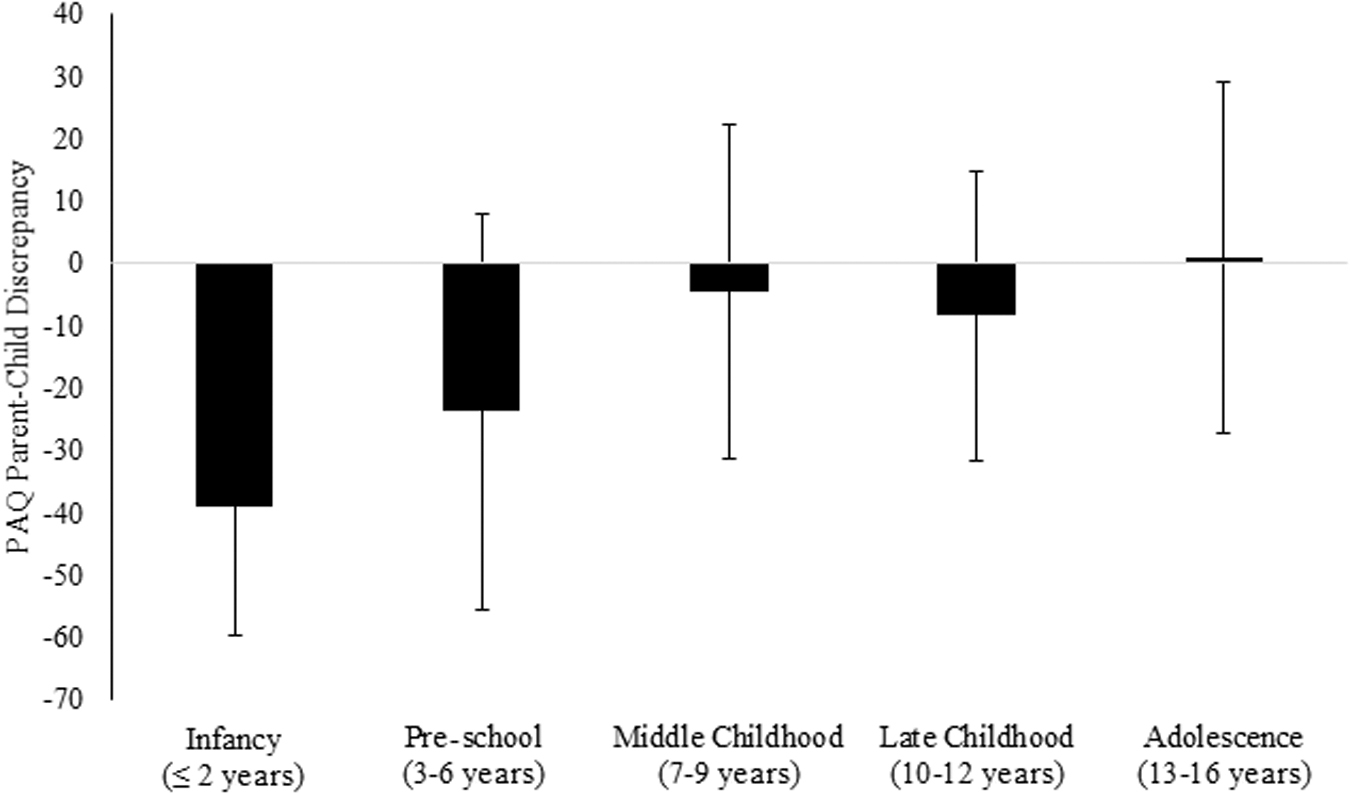
Differences in self-awareness according to age at injury. PAQ, Paediatric Awareness Questionnaire.
Due to the inconsistent findings for GCS score and PTA, the association between severity of injury and self-awareness was further examined using the mild, moderate, and severe injury classification (see Table 1). A one-way analysis of variance (ANOVA) identified that self-awareness significantly differed by injury severity classification: F[2, 104] = 3.94, p = 0.022, np 2 = 0.07. Post hoc tests revealed significant differences between the mild (M = 1.13, SD = 23.97) and moderate TBI (M = −16.04, SD = 27.31) groups (p = 0.027) and between the mild and severe TBI (M = −15.83, SD = 31.96) groups (p = 0.01), but not between the moderate and severe TBI groups (p = 0.98). Injury severity was dichotomized into mild and moderate-severe groups for subsequent analyses. A one-way ANOVA identified no significant differences in self-awareness according to lesion location (coded as: diffuse/multiple lesions, focal lesions, or no abnormality): F[2, 94] = 1.20, p = 0.31, np 2 = 0.025.
A standard multiple regression was conducted to determine the relative contribution of neuro-developmental and socio-environmental factors to self-awareness (see Table 4). In combination, severity of injury, age at injury, time since injury, and family functioning accounted for 18.0% of the variance in self-awareness: F[4, 100] = 5.50, p < 0.001. Only age at injury accounted for significant unique variance in self-awareness (β = 0.34, t = 2.25, p = 0.027; sr 2 = 0.04); children who were older at the time of injury had less impairment in self-awareness.
Results of Regressing PAQ Self-Awareness Discrepancy Scores on Neuro-Developmental and Socio-Environmental Factors
Transformed to address normality violation.
p < 0.05, *** p < 0.001.
FAD, McMaster Family Assessment Device.
Relationship between self-awareness and psychosocial functioning
Correlations
As shown in Table 5, poorer self-awareness was significantly correlated with lower adaptive functioning and greater emotional and behavioral problems as rated by parents. With respect to adaptive functioning, poorer self-awareness was significantly associated with lower social, conceptual, and practical functioning. Poorer self-awareness was significantly related to both greater internalizing and externalizing behaviors (see Table 5). Yet, poorer self-awareness was associated with more positive self-concept and fewer symptoms of depression and anxiety as self-rated by children. Notably, children's self-reported emotional functioning was significantly associated with parent reports, with poorer self-concept and greater anxiety and depressive symptoms significantly related to lower adaptive function and greater emotional and behavioral problems.
Correlations between Self-Awareness (PAQ Discrepancy Score) and Children's Adaptive, Emotional, and Behavioral Functioning
Transformed to address normality violation.
p < 0.05, ** p < 0.01, *** p < 0.001.
ABAS-3 GAC, Adaptive Behavior Assessment System, third edition, global adaptive composite; BYI-2, Beck Youth Inventory, second edition; CBCL, Child Behavior Checklist; PAQ, Paediatric Awareness Questionnaire.
Multi-variate analyses
To determine the unique contribution of self-awareness to adaptive functioning and emotional and behavioral outcomes, other neuro-developmental and socio-environmental variables significantly related to each outcome were identified and entered into hierarchical multiple regressions. First, a hierarchical multiple regression was conducted to determine whether self-awareness was significantly related to parent-reported adaptive functioning after controlling for relevant neuro-developmental and socio-environmental variables (see Table 6). In step 1, severity of injury, age at injury, time since injury, parental education, family functioning, and permissive parenting style were entered and accounted for 34.9% of the variance in adaptive functioning: F[6, 89] = 7.96, p < 0.001. With the addition of self-awareness in step 2, the variance accounted for in adaptive functioning significantly increased by 7%: F[1, 88] = 10.03, p < 0.002. In the final model, self-awareness (β = 0.28, t = 3.17, p < 0.01, sr 2 = 0.07) remained significantly associated with adaptive function, even after adjusting for other variables.
Hierarchical Regression of the Relationship between Self-Awareness and Adaptive Functioning, Controlling for Neuro-Developmental and Socio-Environmental Factors
Transformed to address normality violation.
p < 0.05, ** p < 0.01, *** p < 0.001.
FAD, McMaster Family Assessment Device; PAQ, Paediatric Awareness Questionnaire; PPQ, Parenting Practices Questionnaire.
Second, a hierarchical multiple regression was conducted to determine whether self-awareness was significantly related to parent-reported emotional and behavioral symptoms(CBCL total) after controlling for neuro-developmental and socio-environmental variables (See Table 7). In step 1, age at injury, time since injury, family functioning, and authoritative and permissive parenting styles accounted for 32.7% of the variance in emotional and behavioral functioning: F[5, 93] = 9.02, p < 0.001. The addition of self-awareness in step 2 accounted for a significant further 3% of variance: F[1, 92] = 4.42, p = 0.038. In the final model, self-awareness (β = −0.19, t = 2.10, p < 0.05, sr 2 = 0.03) remained significantly associated with emotional and behavioral functioning, even after adjusting for other variables.
Hierarchical Regression of the Relationship between Self-Awareness and Parent Reports of Children's Emotional and Behavioral Functioning (CBCL Total Problems)
Transformed to address normality assumption.
p < 0.05, ** p < 0.01, *** p < 0.001.
FAD, McMaster Family Assessment Device; PAQ, Paediatric Awareness Questionnaire; PPQ, Parenting Practices Questionnaire.
Finally, three hierarchical multiple regression analyses were conducted in which sex (depression) and adaptive functioning (self-concept, anxiety, and depression) were entered in the first step, and self-awareness was entered in the second step. As shown in Table 8, in the second step of each model, self-awareness accounted for significant additional variance (16–24%) in depression, F[1,92] = 19.89, p < 0.001; anxiety, F[1, 95] = 22.64, p < 0.001; and self-concept, F[1,95] = 34.72, p < 0.001. Therefore, even after adjusting for parental reports of adaptive functioning, children with better self-awareness reported poorer self-concept and greater symptoms of depression and anxiety.
Hierarchical Regression of the Relationship between Self-Awareness and Child Self-Reported Emotional Functioning
p < 0.05, ** p < 0.01, *** p < 0.001.
ABAS-3 GAC, Adaptive Behavior Assessment System, third edition, global adaptive composite; BYI-2, Beck Youth Inventory, second edition; PAQ, Paediatric Awareness Questionnaire.
Discussion
Self-awareness is a key determinant of psychological adjustment and functional outcomes after TBI in adulthood, but this relationship has received little attention in children. This study aimed to identify the factors related to self-awareness and determine the relationship between self-awareness and psychosocial outcomes after pediatric TBI. In relation to the first aim, poorer self-awareness was related to younger age at injury, greater injury severity, longer time since injury, and greater family dysfunction. Younger age at injury was the only variable independently associated with poorer self-awareness. For the second aim, poorer self-awareness was associated with lower levels of adaptive functioning and emotional and behavioral problems based on parent ratings. Yet, poorer self-awareness was associated with more positive self-concept, and fewer symptoms of anxiety and depression as self-rated by children.
Factors associated with self-awareness
The significant association between greater injury severity and poor self-awareness is in line with many prior studies on self-awareness in both the pediatric 12,14,16,28 and adult TBI literature. 45 –47 Unlike children with moderate to severe TBI, children with mild TBI did not typically display impaired self-awareness. This may partly be accounted for by their better functional status, as reported by parents on the ABAS-3. As Hart and co-workers noted, individuals with less severe TBI may have smaller discrepancy scores on awareness questionnaires because of their better functioning, which means there is less scope for disagreement with collateral raters. 22 Contrary to the hypothesis, longer time since injury was associated with poorer self-awareness. This may be explained by the strong negative association between age at injury and time since injury, whereby children injured at a very young age who were still receiving follow-up reviews from outpatient services at age 8–16 years (i.e., an eligibility criterion for this study) were more long-term post-injury than children injured at an older age. Importantly, age at injury was an independent predictor of self-awareness in the regression analysis, after controlling for injury severity, time since injury, and family dysfunction.
The finding that children injured at a younger age demonstrated poorer self-awareness reinforces our earlier pilot study (n = 35) on the PAQ 12 and is consistent with other pediatric TBI research identifying that earlier injuries are prognostic of poorer cognitive and functional outcomes, particularly after severe injury. 2,23 This has been attributed to the vulnerability of the developing brain and the child's lack of consolidated skills at the time of insult, whereby the TBI “derails” brain and cognitive development. 1
In the current study, injuries during infancy (<2 years) were associated with poorer self-awareness than injuries during middle or late childhood and adolescence (i.e., >6 years of age). The negative impact of very early injury on self-awareness may be due to the direct effects of TBI on maturation of brain networks underlying the capacity for self-awareness such as the fronto-parietal control network (e.g., anterior cingulate and insula). This area is commonly disrupted and is involved in performance monitoring and self-reflective processing. 48,49 Additionally, early childhood injuries may impede the development of other cognitive processes that support self-awareness, such as attention, memory, cognitive flexibility, perspective taking, and secondary representation, or the ability to consider multiple mental models simultaneously. 28,50 Longitudinal research is needed to identify whether there is a specific developmental period of brain maturation that supports processes underlying self-awareness.
A key novel finding is that greater family dysfunction, but not parenting style, was significantly associated with poorer self-awareness. Family functioning and parental responsiveness and negativity have previously been found to be related to behavioral problems in children. 51,52 Importantly, the FAD assesses the overall “health” of the family rather than specific parenting styles or behaviors. Family dysfunction on the FAD reflects problems with planning activities; making decisions together; expressing feelings, fears, and concerns; and ability to turn to other family members in times of crisis. Family interaction patterns such as communication style and emotional expression are likely to affect how children receive feedback on and learn about their post-injury impairments, thus influencing their self-awareness. Yet, children with poor self-awareness may also place strain on family members and alter their dynamics—for example, parents and siblings needing to more closely supervise or support the child with TBI. 53 Further research examining the potential reciprocal effects of pre-injury and post-injury family interaction patterns 52 on the development of self-awareness could guide family-based interventions for enhancing self-awareness after pediatric TBI.
The relationship between self-awareness and psychosocial functioning
Consistent with previous research, 1,4,52 a combination of neuro-developmental and socio-environmental factors were associated with parent reports of children's adaptive, emotional, and behavioral function. In the multi-variate analysis, lower parental education, greater family dysfunction, permissive parenting style, and poorer self-awareness were independently related to lower adaptive function. Higher levels of permissive parenting, along with increased time since injury, were independently associated with greater emotional and behavioral problems. This reinforces previous research indicating that behavioral problems are more likely to emerge for children who receive permissive parenting, and can persist or worsen over time, as they continue to struggle with functional changes. 6,8,29,30
However, an important novel finding is that poorer self-awareness was independently related to lower adaptive, emotional, and behavioral function. Children with poor self-awareness may fail to develop strategies to compensate for their functional difficulties (e.g., memory aids) and be less likely to monitor their behavior and develop effective ways to regulate their emotions. Similar to the findings for adults with TBI, lack of self-awareness may serve as a barrier to engagement in rehabilitation and hinder the use of supports and strategies that would otherwise enhance functioning. 20 A common underlying factor, such as impairments in executive functioning, may account for both poor self-awareness and low adaptive functioning, 28 with adverse consequences for their behavioral and emotional functioning.
With regard to children's self-reports, after controlling for sex and functional status, children demonstrating poorer self-awareness reported fewer symptoms of depression and anxiety and better self-concept. Of note, the proportion of children with a clinical level of internalizing problems on the parent-report CBCL (42.7%) was higher than the proportion based on children's self-reported emotional difficulties on the BYI-2 (17–24%). Associations between child report and parent report of emotional and behavioral functioning are typically modest at best in TBI research, 54 and there are several possible explanations for the difference in rates of distress in the current study.
First, caution is needed in comparing rates of distress across different instruments. There are very few items assessing somatic symptoms on the BYI, whereas the CBCL internalizing scale includes the somatic complaints subscale. Somatic symptoms may represent sequelae of TBI rather than emotional distress. Second, parent report of a child's internal state is inferred from observable behavior, whereas child self-report is inherently subjective and may not be consistent with outward emotional displays. 55 As such, the higher rates of parent-reported distress might suggest that children under-report their own emotional difficulties (as a result of poor self-awareness) or, alternatively, that the behaviors of children reported by parents on the CBCL are not always indicative of children's internal emotional distress. 54,55 Different insights are likely to be gained from each perspective, and therefore obtaining both parents' and children's reports of emotional and behavioral functioning is valuable. Impaired self-awareness has been found to be protective against psychological distress and low self-esteem in adults 27 and children. 18 At the same time, greater self-awareness of post-injury changes can increase motivation and improve self-regulation skills, which are integral to independence and management of emotions. 9,19
Implications
In terms of clinical practice, the findings highlight that children injured at a younger age (i.e., during infancy), those with moderate to severe TBI, and those with greater family dysfunction are more likely to have poor self-awareness. It may be beneficial to monitor changes in self-awareness throughout rehabilitation to gauge the impact on children's coping reactions, functional outcomes, and support needs. Better self-awareness may promote gains in adaptive skills and enhanced emotional and behavioral functioning from the parents' perspective, yet children with more accurate self-awareness may be at greater risk for developing mood symptoms and poor self-concept.
In line with clinical guidelines for adults 56,57 it is recommended that interventions to increase children's self-understanding of their TBI (e.g., psycho-education and feedback on abilities) involve closely monitoring children's emotional state. Although metacognitive interventions involving feedback on everyday tasks are a practice standard in rehabilitation for adults, 57 the development of interventions to improve self-awareness for children is in its infancy. 31 It is important that such interventions support children to process the meaning of changes in their abilities, develop effective coping strategies, and recognize their strengths and achievements. In this way, the potential liability of increased self-awareness for children's self-concept and mood may be offset by better functional outcomes, including social adjustment. 28
Given the finding that better family functioning was associated with children's greater self-awareness, interventions to improve family interaction patterns may have utility (see existing evidence-based approaches 58,59 ). Strategies to incorporate into these interventions include supporting parents and other family members to provide timely, sensitive, and balanced feedback on their child's strengths and weaknesses, and to present tasks at an appropriate level of challenge that concurrently facilitates gains in self-awareness and self-mastery. The latter focus is particularly important to buffer the potentially negative effects of increased self-awareness on mood and self-concept. Such interventions also need to be developmentally sensitive and account for the needs of children injured at a very young age, whose impairments often reflect disrupted development of skills rather than loss of acquired skills.
Study limitations and future research
In terms of sampling, participants were recruited from consecutive appointments at a hospital-based outpatient TBI clinic that provides long-term follow-up to children. Although the consecutive recruitment is a strength, this sampling approach increases the possibility of clinical ascertainment bias, and it is unknown to what extent the current sample is representative of the broader pediatric TBI population. Although there were no significant differences in demographic and injury-related characteristics between the current sample and children who were eligible but did not participate, there are likely to be differences between the families that attend follow-up and those that do not. Parents' typically high education levels (M = 14.08, SD = 2.9) suggest that the current sample may not adequately represent the children of families with lower socio-economic status. Further, the current sample displayed higher rates of clinically elevated internalizing symptoms relative to externalizing symptoms, whereas the reverse has been found in previous research. 6 Such findings highlight the need for some caution in generalizing the results to the broader pediatric TBI population.
Another key consideration is that measurement of self-awareness was based on the parent-child total discrepancy score, which assumes that parents provide an accurate representation of their children's functional abilities. Yet, parent ratings are subject to bias due to the impact of parental stress, mood concerns, and their own denial or self-illusory bias, as well as social desirability effects. 55,60,61 Such factors may potentially lead to either more negative ratings or overly optimistic perceptions of their children's functioning (i.e., on the PAQ, CBCL, or ABAS) and their own parenting and family functioning. 55
Further, as outlined by Hart and co-workers, 22 and discussed earlier, a limitation of the discrepancy-based method is that the size of the discrepancy score is in part dependent on the magnitude of parents' ratings. This means that children rated as having better functioning are likely to have smaller PAQ discrepancy scores because there is less scope for disagreement in the ratings. In future research it would be beneficial to assess self-awareness using a multi-faceted approach, which includes comparison of child, parent, and clinician ratings, as well as performance-prediction approaches. 13 The latter approaches involve individuals making prospective and/or retrospective judgments of their own performance on neuro-psychological measures or functional tasks that are then compared with actual performance. 13 Despite the benefits of providing a more objective or accurate measure of children's functioning, questionnaire-based assessments are necessary because performance-based approaches can only assess self-awareness in a particular domain (e.g., memory functioning) and are more time-consuming for each family, introducing barriers to research participation and clinical assessment. 60
The cross-sectional design limits inferences regarding the direction of associations between socio-environmental factors, self-awareness, and psychosocial outcomes. Although family dysfunction may contribute to poor self-awareness, children with poor self-awareness are likely to require greater support and supervision with everyday activities, which may alter family dynamics, placing greater strain on relationships. Similar to the reciprocal effects observed between parenting style and behavior, 53,62 this relationship may be bi-directional. Accordingly, prospective longitudinal research with early assessment of pre-injury family functioning could determine the early predictors of and psychosocial impacts of impaired self-awareness. Such research could also identify potential mediators of the relationship between younger age at injury and poor self-awareness, which may include neuro-cognitive (e.g., executive functioning) and psychosocial factors (e.g., parental protectiveness). The inclusion of an orthopedic control group would help to discern the effects of TBI on self-awareness relative to the broader effects of trauma on children's self-perceptions.
Finally, although a range of neuro-developmental and socio-demographic variables were included in the study, neuro-psychological variables (e.g., attention, memory, language, executive function, and theory of mind) were not assessed, and remains an important endeavor for future research. Further, more precise neuro-imaging data are needed to investigate neuro-anatomical correlates of self-awareness in children, potentially using functional tasks measuring online awareness of errors. 48
Conclusion
Overall, this study significantly extends the literature on self-awareness following TBI in childhood. The main findings were that younger age at injury, greater injury severity, and increased family dysfunction were associated with poorer self-awareness. Further, poorer self-awareness was related to lower adaptive skills and greater emotional and behavioral problems as rated by parents. Yet, children with poorer self-awareness reported fewer symptoms of depression and anxiety and better self-concept. These findings suggest that impaired self-awareness can be viewed as both a liability and a protective factor depending on the perspective (parent or child) and the outcome of interest (adaptive function, emotional and behavioral outcomes, or self-concept). This underscores the importance of monitoring developments in self-awareness over time and supporting children's emotional functioning as awareness increases. It is recommended that future development and evaluation of metacognitive interventions to improve self-awareness after pediatric TBI incorporate strategies for enhancing mood and self-concept.
Footnotes
Acknowledgments
This study was conducted in partial fulfilment for PhD requirements for the first author.
The authors thank all staff from the Queensland Paediatric Rehabilitation Service at the Queensland Children's Hospital for supporting the study and the families that so generously participated in this study.
Funding Information
This study was supported by a seed grant from the “Moving Ahead Centre of Research Excellence.” There was no specific grant number.
Author Disclosure Statement
No competing financial interests exist.