
Abstract
Increasing traumatic brain injury (TBI) among older adults constitutes a substantial socioeconomic burden, in step with the growing aging global population. Here, we aimed to investigate the profile of geriatric TBI in the CENTER-TBI China registry, a prospective observational study conducted in 56 centers of 22 provinces across China. Patients admitted to the hospital with a clinical diagnosis of TBI were enrolled in the study. Data on demographic characteristics, injury, clinical features, treatments, and survival at discharge were collected and assessed. The primary end point was survival state at discharge. We analyzed a total of 2415 patients aged ≥65 years, accounting for 18.34% of the overall population. The median age was 72 years (interquartile range [IQR]: 68–78), and 1588 (65.76%) were men. Incidental falls (n = 1044, 43.23%) were the leading cause of TBI, followed by road traffic injuries (n = 1034, 42.82%). Roads and homes were the main sites of injury. The median Glasgow Coma Scale (GCS) score was 13 (IQR: 9–15); 1397 (57.85%) patients had mild TBI (GCS 13–15), while 530 (21.95%) and 488 (20.21%) presented with moderate (GCS 9–12) and severe TBI (sTBI; GCS 3–8), respectively. A total of 546 (22.61%) patients underwent intracranial surgery. The overall in-hospital mortality rate was 8.24% (n = 199), and most survivors were transferred home. This study revealed that the demographic patterns and injury mechanisms are changing among elderly patients with TBI in China. More attention should be given to the high incidence of geriatric TBI to improve prevention and management strategies.
Introduction
As a significant cause of death and disability across all ages, traumatic brain injury (TBI) represents one of the most challenging global health care problems, with substantial health and economic burden to society. 1 The rapid aging of the population, especially in developed countries, has led to a global burden of late-life disease, which also prevails in low-middle-income countries like China. 2 –5
According to data reported by the National Bureau of Statistics of China, in 2020, there were more than 0.19 billion Chinese adults aged ≥65 years, and the proportion of the older adult population increased steadily from 2008 (8.30%) to 2020 (13.5%). 6,7 Older patients are more susceptible to chronic systemic comorbidities, such as cardiovascular and cerebrovascular disease. Moreover, older patients have more complications and a slower rehabilitation process after TBI and, thus, have worse functional and cognitive outcomes post-injury. 8,9
The epidemiology of older persons with TBI is changing as populations progressively age, resulting in an ever-growing demand for healthcare. 8 The median age of patients with TBI in high-income countries (HICs) has nearly doubled since the 1980s. 1 Preventive public health measures have significantly reduced TBI caused by motor vehicle accidents. An increased burden of fall-induced TBI, however, especially in HICs, increases the incidence of geriatric TBI. 8,10,11 Therefore, acknowledging the importance of this epidemiological transition will allow specific management strategies to be planned for geriatric patients with TBI.
There are several retrospective Chinese studies on TBI; however, the status of TBI in older patients is incomplete, and studies focusing on geriatric TBI remain absent in China. 12,13 The Collaborative European NeuroTrauma Effectiveness Research in TBI China Registry was a prospective, longitudinal observational study. 14,15 Given the specificities of older patients, in the present study, we examined the characteristics and outcomes of older patients with TBI (aged ≥65 years) from the CENTER-TBI China Registry to understand the current epidemiological patterns of geriatric TBI in China.
Methods
From December 22, 2014, to August 1, 2017, the CENTER-TBI China Registry enrolled patients from 56 Chinese neurosurgical centers. According to the study protocol, the main criteria for inclusion of the CENTER-TBI China Registry was the admission to the hospital with a clinical diagnosis of TBI and clinical indication for head CT scan. Patients who were discharged directly from the emergency department were excluded. No other inclusion or exclusion criteria apply for the Registry dataset.
Management guidelines and CT scans performed as part of clinical care followed the standard clinical practice of the hospital. Patients aged ≥65 years were analyzed in our study. Written informed consent was obtained from all enrolled patients. The protocol was approved by the Medical Ethics Committees of all participating centers and was conducted according to the relevant laws of China.
Informed consent procedures followed local and national requirements in all cases. For patients who were not physically capable of consenting themselves, the legal representative, usually one of the family members or the closest relatives who can decide on behalf of the patient, was to be approached for the assent of participation in the study or not. An independent staff from the local ethics committee and Institutional Review Board were be asked for approval when no legal representative was available in due time.
Data collection
Data collection was elementary and based on retrospective extraction from clinical records of data that are routinely collected clinically. No specific study interventions were performed. The following clinical data were collected by one or more dedicated and trained physicians in each center from medical records or personal interviews during a hospital stay: Patients' demographic, pre-injury factors, such as usage of anticoagulants and antiplatelets. Recorded injury details on arrival at the hospital, including Glasgow Coma Scale (GCS) score, Injury Severity Score (ISS), clinical symptoms, vital signs, imaging findings. Treatment of intracranial surgeries and survival status at discharge.
Pre-injury physical status of TBI victims was scored according to the first four-level ordinal scale of the American Society of Anesthesiologists Physical Status (ASA-PS) Classification system. A normal healthy patient was classified as ASA-PS grade 1, a patient with mild systemic disease was classified as ASA-PS grade 2, a patient with severe systemic disease was classified as ASA-PS grade 3, and a patient with severe systemic disease that is a constant threat to life was classified as ASA-PS grade 4. The GCS scores were stratified as mild (GCS 13–15), moderate (GCS 9–12), or severe TBI (sTBI, GCS 3-8). The ISS was stratified as mild to moderate (<9), serious (9–15), severe (16–24), and critical (25–75).
On arrival at the hospital, systemic hypotension was defined as systolic blood pressure ≤90 mm Hg, and hypoxia was defined as oxygen saturation ≤95%. According to study protocol of the CENTER-TBI China Registry, only survival states and discharge destination were collected at discharge. In the case of in-hospital death, the time and cause of death were recorded. Length of stay (LOS) in hospital was recorded for survivors. Patients with missing information on discharge status or essential clinical severity (e.g., GCS score and pupillary light reflex) were excluded from analysis. Missing values for other baseline characteristics were classified as unknown.
All data were collected using a web-based electronic case report form and the Common Data Elements scheme coded data. Study data were deidentified and stored in the study data space hosted by the International Neuroinformatics Coordinating Facility with headquarters at the Karolinska Institute and the Royal Institute of Technology, Stockholm, Sweden. 15
Statistical analysis
Continuous variables were described as mean and standard deviation (SD) or median and interquartile range (IQR). Survival state at discharge, presence or absence of abnormal clinical symptoms, injury mechanism, and imaging findings were described as categorical variables. Categorical data were reported as absolute and relative frequencies. Patients' characteristics and outcomes among groups were compared using the chi-square test or Fisher test for categorical variables and an analysis of variance, t test, or non-parametric test for continuous variables, depending on the nature of the variables.
A logistic regression model with 95% confidence intervals (CI) was applied to the odds of in-hospital death, and death from any cause was the event of interest. Based on the likelihood ratio test and Akaike information criterion, appropriate variables that were significant in the univariate analysis and judged clinically relevant were selected as the covariates for the final model that included age, GCS, pupillary reactivity, and hypoxemia, et. al. The days of hospitalization were described as continuous variables.
A two-tailed p value of ≤0.05 was used to define statistical significance. Statistical analyses were performed using R statistical software. (version 4.0.1), with Studio (version 1.3.959), used as the implementation integrated development environment.
Results
A total of 13,627 patients were enrolled in the CENTER-TBI China Registry study and 2500 (18.35%) were geriatric (aged ≥65 years). A total of 460 (3.38%) patients were excluded from the analysis because of incomplete data, of whom 85 (18.48%) patients were geriatric. Finally, 2415 patients aged ≥65 years were analyzed in this study, accounting for 18.34% of all analyzed participants in the Registry study. Detailed characteristics of geriatric patients with TBI who were excluded from the analysis are reported in Supplementary Table S1.
The baselines characteristics of all geriatric patients with TBI are summarized in Table 1. The median age was 72 years (IQR: 68–78), and men (n = 1588, 65.76%) accounted for almost two-thirds of the overall. The age distribution showed that the number of TBI cases decreased with age (Fig. 1). A total of 201 (8.32%) took both anticoagulant agents and antiplatelet agents before the injury.
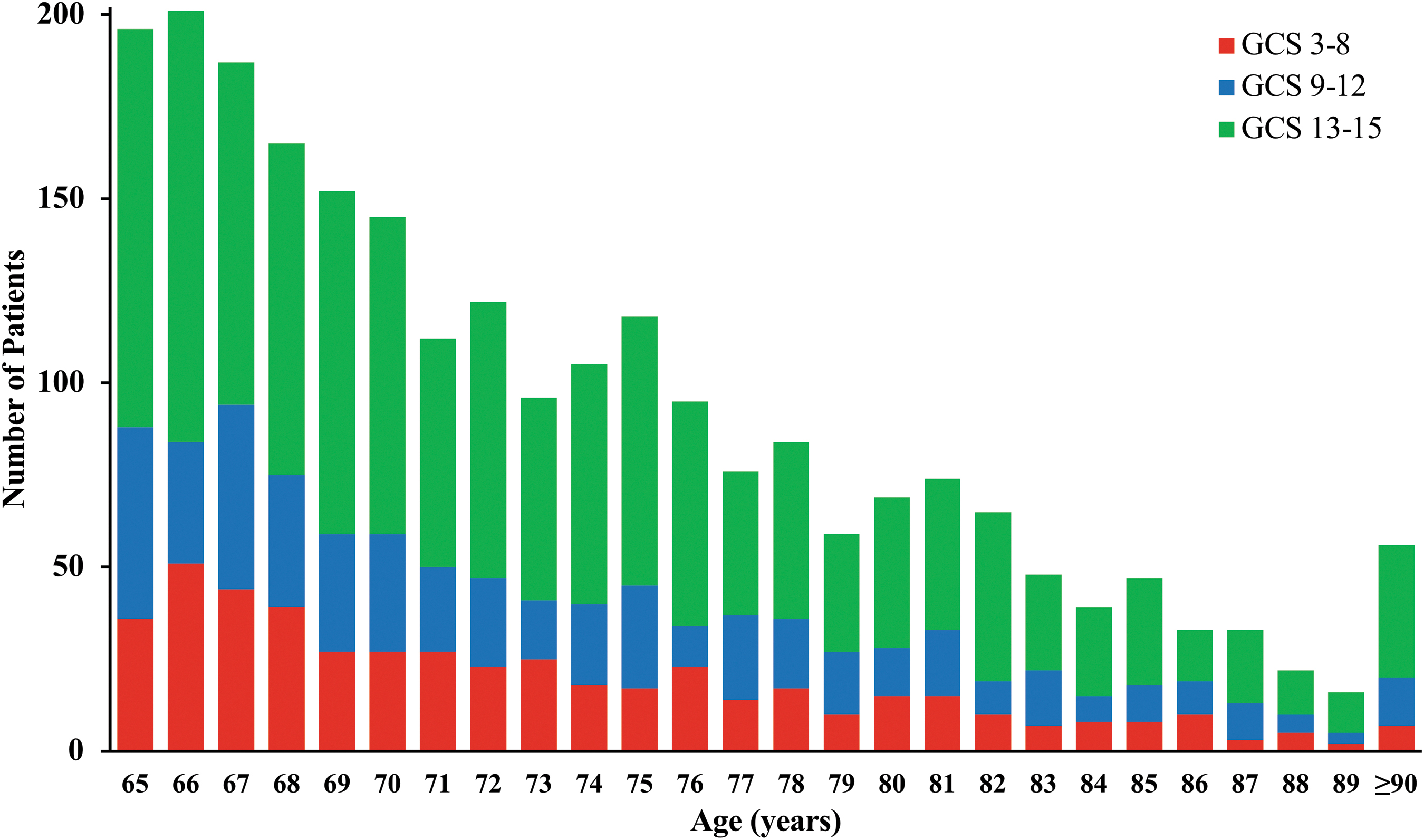
Age and Glasgow Coma Scale (GCS) score distribution of older patients with traumatic brain injury (TBI). The number of patients was arranged per age level from 65 to 90 years and older. The age distribution showed that the number of TBI cases decreased with age. Patients of each age level were stratified, using GCS score on arrival at the hospital, as mild (GCS 13–15), moderate (GCS 9–12), or severe TBI (GCS 3-8), with a different color. Color image is available online.
Baselines Characteristics of Older Patients with Traumatic Brain Injury
IQR, interquartile range; ASA-PS, American Society of Anesthesiologists physical status classification system; ISS, Injury Severity Score; GCS, Glasgow Coma Scale; hypoxia was defined as oxygen saturation ≤95% on arrival in hospital; systemic hypotension was defined as systolic blood pressure ≤90 mm Hg on arrival in hospital; ICU, intensive care unit.
Almost half of the patients (n = 1158, 47.95%) were in good physical condition before the injury episode (ASA-PS grade 1), 943 (39.05%) patients had mild systemic disease (ASA-PS grade 2), and the rest were associated with the morbid state (ASA-PS grade 3 or 4). The median GCS score of geriatric TBI was 13 (IQR: 9–15), 1397 (57.85%) were classified as mild TBI, 530 (21.95%) as moderate TBI, and 488 (20.21%) as sTBI. A total of 901 (37.31%) patients had been treated in intensive care units (ICU).
For the cause and place of injury, incidental falls (n = 1044, 43.23%) were the primary cause of injury in geriatric patients with TBI, with three-quarters being ground-level falls, closely followed by road traffic-related incidents (n = 1034, 42.82%). Road traffic-related incidents, however, were the primary cause of injury in patients aged <65 years (Table 2). In addition, the mechanisms of injury changed with age in geriatric patients, with the proportion of incidental falls increasing with age and the proportion of road-traffic injuries showing a reverse trend. Reversely, road-traffic injuries had a major and stable portion for most patients below 65 years (Fig. 2 and Supplementary Fig. S1).
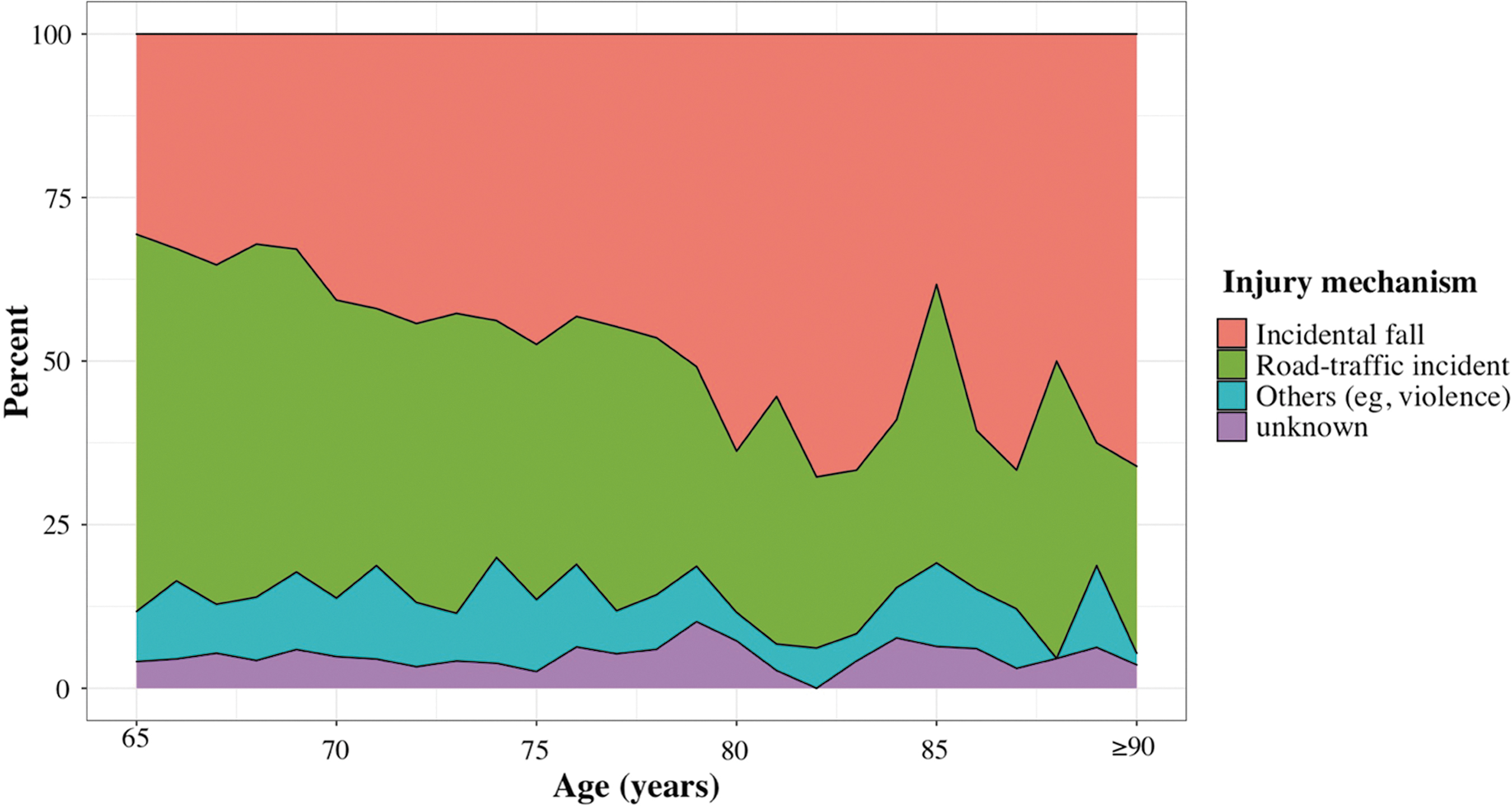
Injury mechanisms distribution of older patients with traumatic brain injury (TBI). The patients were arranged per age level from 65 to 90 years and older. The number of patients at each age level were stratified by mechanism of injury with a different color. The proportion of patients injured by incidental fall shows an increasing trend with the increase of age, where the proportion of road-traffic incidents indicates the contrary. Color image is available online.
Comparison of Injury Characteristics in Patients with Traumatic Brain Injury between Geriatric and Younger Patients
Other causes of injury include violence and suicide.
As for the site of injuries, roads and homes were the leading injury hotspots for both older and younger patients (Table 2). Home (n = 903, 37.39%) was the primary site of both ground-level falls (n = 535, 70.03%) and falls from a height (n = 189, 67.50%) in geriatric TBI, followed by roads and public places where incidental falls occurred (Supplementary Fig. S2). For geriatric patients injured in traffic accidents, most patients were pedestrians (n = 509, 49.23%), while a small number were passengers (n = 96, 9.28%). Notably, motorcyclists injured in a traffic accident had the highest proportion (29.13%) of sTBI (Supplementary Fig. S3). The median time of geriatric patients with TBI from injury to arrival in hospital was 2.17 h (IQR: 1.00–6.00), and most patients arrived in hospital within 24 h post-injury.
Regarding surgical treatments, 546 geriatric patients with TBI underwent intracranial surgery, accounting for 22.61% of all. Among them, 405 (16.77%) patients underwent a craniotomy, 361 (14.95%) underwent a decompressive craniectomy including 10 (2.77%) of whom underwent a secondary decompressive craniectomy, 237 (9.81%) underwent intracranial pressure monitoring, and 127 (5.26%) underwent external ventricular drainage (Table 3). Some patients underwent more than one intracranial operative treatment simultaneously.
Comparison of Surgery Rate in Patients with Traumatic Brain Injury between Geriatric and Younger Patients
ICP, intracranial pressure; ASDH, acute subdural hematoma; EDH, epidural hematoma.
Geriatric patients had a higher incidence of acute subdural hematoma (ASDH) and contusion, but a lower incidence of epidural hematoma (EDH). Compared with the patients below 65 years, geriatric patients indicated a lower proportion of intracranial surgeries, both in an overview or for specific diagnoses of ASDH, EDH, contusion, and corresponding surgeries (Table 3). Besides, the proportion of each intracranial surgery decreased with increasing age among older adults aged 65–74 years, 75–84 years, or ≥85 years (Supplementary Table S2). Characteristics of geriatrics were compared between surgically treated patients and those who underwent conservative treatments (Supplementary Table S3). Surgically treated patients were younger and had better pre-injury status, worse clinical presentation.
Overall, the in-hospital mortality rate of older adults in this study was 8.24% (n = 199), which was higher than the younger patient (Table 4). The primary causes of death in geriatric TBI were initial injury (n = 119, 59.80%); 45 (22.61%) died from secondary intracranial damage. A higher proportion of geriatric patients died from medical complications than younger patients. As for injury mechanism of death in geriatric patients, pedestrian traffic-related incident was primary, followed by ground-level fall and fall from height. But fall from height was the primary injury mechanism of death in younger patients.
Comparison of Treatment and Discharge in Patients with Traumatic Brain Injury between Geriatric and Younger Patients
LOS, length of stay; IQR, interquartile range.
Other causes of injury include violence and suicide.
The median LOS of geriatric survivors was 14.5 days (IQR: 8.0–24.8); however, this was not significantly different from the younger patients (Table 4). Potential predictors for in-hospital death in multi-variable logistic regression indicated that the following variables were significantly associated with in-hospital death for geriatric patients: increasing age, a poor physical condition pre-injury (ASA-PS grade 3 or 4), higher ISS score, lower GCS score, and absence of bilateral pupillary light reflex (Fig. 3). As for survivors' discharge destinations, geriatric patients and younger patients had a similar proportion of patients who were transferred to local hospitals, rehabilitation centers, and nursing homes (Table 4). A lower proportion of geriatric patients, however, were discharged home with self-care than younger patients.
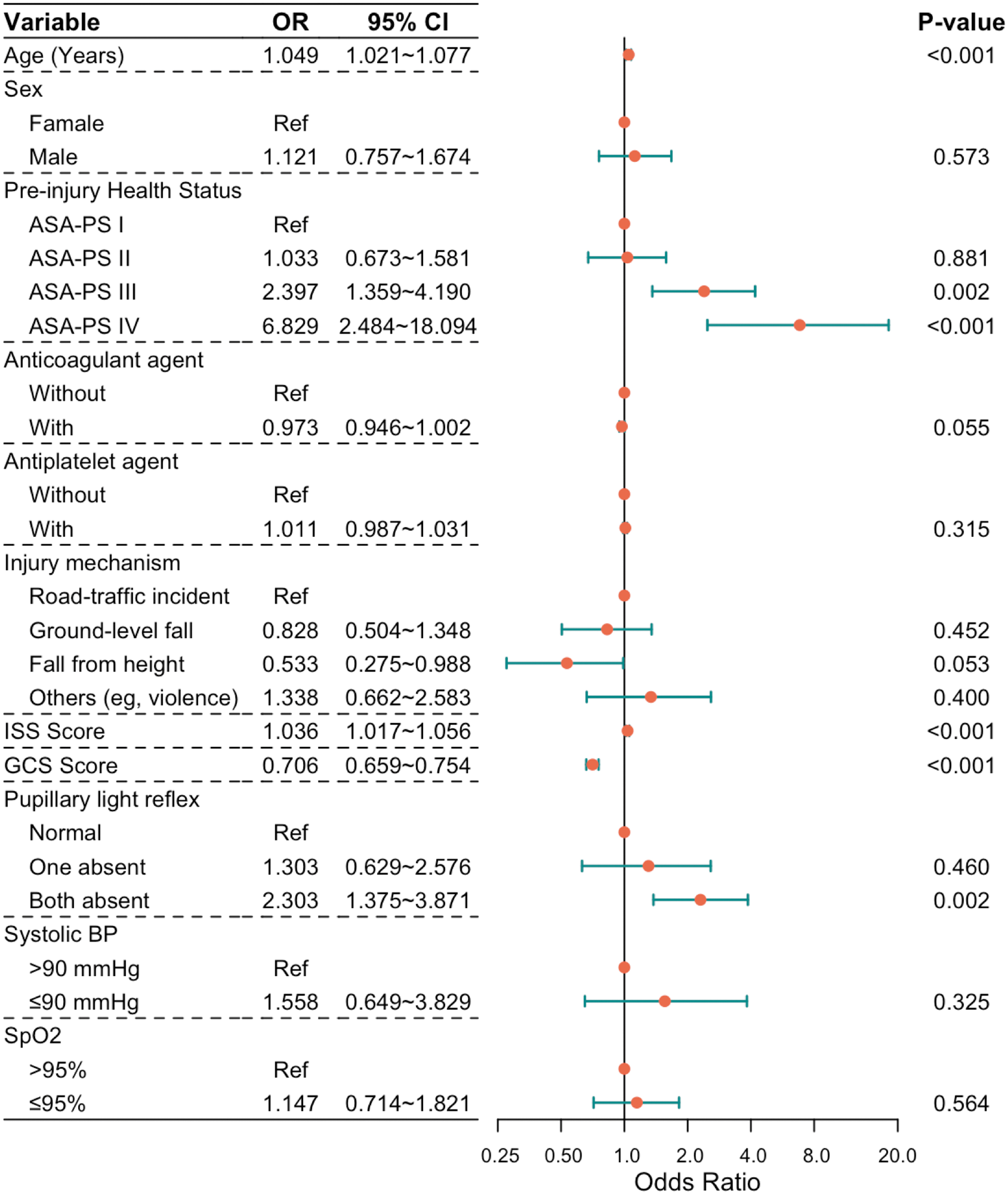
Forest plot of predictors for inhospital death of older patients with traumatic brain injury (TBI). Forest plot of multi-variable logistic regression model for risk factors (odds ratio with 95% confidence interval) showed that inhospital death predictors for older patients with TBI included increased age, pre-injury health status, Glasgow Coma Scale (GCS) score, Injury Severity Score (ISS), and pupillary reflex. ASA-PS, American Society of Anesthesiologists Physical Status; BP, blood pressure; SpO2, oxygen saturation. Color image is available online.
Discussion
This study reported a socioepidemiological overview of older adults with TBI based on China's prospective longitudinal observational study. In addition to presenting an overview of Chinese geriatric TBI with regard to general characteristics and clinical presentation, we further compared some significant issues of geriatric TBI with younger patients, including the injury characteristics, surgeries, and outcome.
With the rapid growth of the global elderly population, various studies have reported an increased incidence of TBI in older adults. In some investigations, the incidence rate of geriatric TBI has even exceeded the aged population growth rate. 16 –20 In our study, the incidence of geriatric TBI was 18.34%, while the proportion of adults aged ≥65 years in China ranged from 10.1% to 11.4% between 2014 and 2017. 6 Compared with a 2008 observational study, which reported that the incidence of geriatric TBI in China was lower than 10%, our study revealed that the incidence of geriatric TBI has almost doubled. 12
The incidence of geriatric TBI-related hospitalizations is even higher in developed countries. 8 A population-based study in Finland reported an estimated overall annual increase of 2.9% during 2004–2014. 20 A concurrent European CENTER-TBI core study reported that older adults aged ≥66 years accounted for 28% of the overall TBI population, and the incidence had significantly increased compared with previous studies with an incidence of 10%. 21,22 This suggests that TBI should no longer be considered a disease predominately affecting young populations. Predictably, the incidence of TBI among geriatric patients in developing countries may reach levels comparable with that of HICs in the future, causing sharp increases in public health burden. 1
Changes in the epidemiological pattern of TBI can also be observed when we consider the causes of TBI in older patients. Road-traffic accidents are still the primary cause of TBI in China, followed by incidental falls. 13,23 On the contrary, falls are the leading cause of TBI in HICs, especially in older patients. 17,19,24 –28 Fall-induced TBI accounted for 82.9% of TBI hospitalizations in older adults, increasing by an estimated 8.4% per annum from 1998 to 2011, as reported by a population-based Australian study. 16 In our study, we observed the proportion of incidental falls increased with age in geriatric TBI, while traffic-related injury declined.
Moreover, the proportion of falls surpassed traffic-related incidents at the age of 70 years, becoming the leading cause of TBI. This is earlier than what was reported in a previous study where incidental falls were the primary cause of TBI at 75 years. 12 More chronic disorders, impaired balance, and sensory neuropathy in older adults may have contributed to an increase in fall-related TBI. 29 Given the increasing aging population and the decreasing proportion of traffic-related incidents, falls may become the leading cause of TBI in China in the future, which would match the epidemiological patterns of TBI in HICs. 1,30
Therefore, further studies are needed to investigate the reasons underlying the increase in fall-related TBI among geriatric patients so that effective interventions that prevent falls and injuries can be planned. 31,32 Injury prevention, specifically related to fall-induced geriatric TBI, was previously recommended as a primary public health intervention to reduce the burden of TBI. 32 In our study, most falls occurred at home and in public areas, which is consistent with previous studies. 10,16,27,33,34 Bathroom safety interventions may be helpful because Gillespie and associates found that falls at home were twice as likely to occur in bathrooms compared with living rooms. 35 Other specific environmental modifications, such as the antislip function of stairs or steps, may further reduce fall-induced injury. Nevertheless, a more rigorous analysis of the effectiveness of preventive measures for fall-induced TBI is vital. 36,37
As for treatment, advanced age may also influence the decision of surgery because the younger patients had a higher operation rate in our result (Table 4). In addition, among geriatric patients, surgically treated patients were younger than those who were conservatively treated (Supplementary Table 3).
Increasing age is known to be an independent adverse prognostic factor of outcome after TBI. 38,39 In our study, overall in-hospital deaths for older patients with TBI was double that of younger patients (Table 4). Physiological changes and pathological conditions associated with aging may affect the normal function of the geriatric population. Our results indicated pre-existing diseases were predictors of an increased mortality rate in post-TBI patients with ASA-PS scores of 3 and 4 pre-injury. Moreover, additional medical complications or comorbidities among older patients may contribute to higher mortality rates. 17
Fortunately, the improvement of TBI management has consistently reduced both overall and geriatric TBI deaths compared with those reported by epidemiologic studies decades ago. 26,40,41 A Chinese population-based longitudinal analysis evaluating trends in TBI deaths showed that patients aged >75 years exhibited a gradual and substantial decrease in TBI deaths between 2008 and 2013, from 62.29 per 100,000 population to 48.60 per 100,000 population. 42
Lower in-hospital deaths, however, do not imply better long-term outcomes, because TBI is a lifelong disorder with multiple necessities over time. 43 Sequelae develop in some older TBI survivors that later lead to death, and moderate and sTBI are associated with increased post-discharge mortality risk. 44,45
Rehabilitation could substantially improve long-term prognosis of older patients with TBI. 46,47 Only a few patients, however, were transferred to rehabilitation centers after discharge in our study, as well as the younger patients. Several studies have shown that patient age significantly influences referral decisions. 48,49 Referral decisions are also influenced by different expectations and financial concerns, which are complex issues in older patients' lives. 48,50 The suggestion that older patients have a reduced potential for rehabilitation is unfitting; instead, rehabilitation effectiveness should be evaluated based on the potential positive effects on older patients.
Our study provides essential indications because the number of studies assessing the epidemiological transition of geriatric TBI in China over the past decades is limited. This study, however, has some limitations that should be considered when interpreting the results. First, the data cannot represent the entire hospitalized geriatric TBI population in China because only 56 centers participated. Not every geriatric TBI admitted to the participating hospitals was captured in this study, details of screening logs were unavailable, and some patients with missing information were excluded from analysis; this resulted in selection bias and potential underestimates of deaths.
Second, the study did not record some key characteristics, such as pre-existing diseases, detailed complications, long-term functional outcomes, and quality of life, etc. This information bias and confounding bias impacted the statistical significance and, thus, our results here are only preliminary and require further validation.
Conclusion
The current study demonstrated that the epidemiological patterns of geriatric TBI in China are changing in terms of incidence, leading cause of injury, and other factors. These changes require further attention, and further population-based studies are urgently needed to fill current knowledge gaps, which may improve our understanding of geriatric TBI and help plan specific preventive measures.
Footnotes
Acknowledgments
We would like to thank all clinical investigators and research staff at the CENTER-TBI for their valuable contribution to this study.
Authors' Contributions
J.F., G.G., and J.J. contributed to study concept and design. C.Y., Z.H., and L.L. contributed to data acquisition and analysis. C.Y. and L.L. drafted the manuscript and figures. J.F. and C.Y. contributed to both data analysis and manuscript's critical revision. All authors reviewed and approved the final version of the paper.
Conflict of Interest
None declared.
Funding Information
The data were obtained from CENTER-TBI, a large collaborative project with the support of the European Commission 7th Framework program (grant number 602150). The work completed in China was supported by the National Natural Science Foundation of China (grant numbers: 81971699, 81671198, 82071358 and 81771317) and Shanghai talent development funding (grant number: 2018077).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.