
Abstract
Patients with disorders of consciousness (DoC) after traumatic brain injury (TBI) recover to varying degrees of functional dependency. Dependency is difficult to measure but critical for interpreting clinical trial outcomes and prognostic counseling. In participants with DoC (i.e., not following commands) enrolled in the TBI Model Systems National Database (TBIMS NDB), we used the Functional Independence Measure (FIM®) as the reference to evaluate how accurately the Glasgow Outcome Scale-Extended (GOSE) and Disability Rating Scale (DRS) assess dependency. Using the established FIM-dependency cut-point of <80, we measured the classification performance of literature-derived GOSE and DRS cut-points at 1-year post-injury. We compared the area under the receiver operating characteristic curve (AUROC) between the DRSDepend, a DRS-derived marker of dependency, and the data-derived optimal GOSE and DRS cut-points. Of 18,486 TBIMS participants, 1483 met inclusion criteria (mean [standard deviation (SD)] age = 38 [18] years; 76% male). The sensitivity of GOSE cut-points of ≤3 and ≤4 (Lower Severe and Upper Severe Disability, respectively) for identifying FIM-dependency were 97% and 98%, but specificities were 73% and 51%, respectively. The sensitivity of the DRS cut-point of ≥12 (Severe Disability) for identifying FIM-dependency was 60%, but specificity was 100%. The DRSDepend had a sensitivity of 83% and a specificity of 94% for classifying FIM-dependency, with a greater AUROC than the data-derived optimal GOSE (≤3, p = 0.01) and DRS (≥10, p = 0.008) cut-points. Commonly used GOSE and DRS cut-points have limited specificity or sensitivity for identifying functional dependency. The DRSDepend identifies FIM-dependency more accurately than the GOSE and DRS cut-points, but requires further validation.
Introduction
Most patients with a disorder of consciousness (DoC) after traumatic brain injury (TBI) ultimately recover consciousness. 1 –3 However, studies of short, 1 medium, 2 and long-term 3 –5 outcomes in this patient population suggest that levels of function vary widely, from independent and employable to dependent for all basic needs. TBI clinical trials track recovery using standardized outcome measures, such as the Glasgow Outcome Scale-Extended (GOSE) 6,7 or the Disability Rating Scale (DRS), 8 and often collapse the distribution of scores into “favorable” and “unfavorable” groups to simplify analysis and interpretation. The precise cut-points used to generate these groups differ across measures and across trials. Although there is no universal definition for unfavorable outcome, in a recent study, most families of patients in the intensive care unit with severe brain injury reported that complete dependency, defined as requiring assistance with all physical and cognitive tasks, would not be an acceptable long-term outcome. 9 The accuracy of different GOSE and DRS cut-points for identifying complete dependency in patients recovering from TBI is unknown.
The Functional Independence Measure (FIM®), 10 a comprehensive instrument that scores level of assistance needed across 13 physical and five cognitive dimensions, provides a granular assessment of the severity of a patient's functional impairment. The FIM is used extensively as a research outcome measure in the rehabilitation setting and has been studied across the trajectory of recovery from non-neurological and neurological injury and illness, including TBI. 11,12 FIM scores reflect the time (hours per day) and type (supervision vs. assistance) of external support a patient requires 13,14 to complete basic tasks. A FIM total score <80 indicates complete dependence (i.e., FIM-dependency) and reflects a burden of care that cannot typically be provided in the home. 15 –18 The FIM is not commonly used in interventional TBI clinical trials, most established TBI outcome databases, or other medical disciplines, and is being phased out of routine use.
The GOSE, 6,7 an eight-item ordinal scale, is the most frequently used TBI outcome assessment and the only measure accepted by the U.S. Food and Drug Administration as a primary outcome in TBI trials. 19 However, each GOSE level encompasses a wide range of function and clinically meaningful differences in disability may be missed. 20,21 An alternative to the GOSE, the DRS, 8 was designed to reflect the full range of outcomes after TBI, from coma to return to competitive employment. 19,22 Limitations of the DRS include imprecision and ceiling effects. 4,20 Though both the GOSE and the DRS have individual items evaluating dependence, how well these measures align with the FIM, which was designed and validated to directly measure dependence, has not been established.
Using data from the Traumatic Brain Injury Model Systems (TBIMS) National Database (NDB), the largest prospective, longitudinal TBI cohort in the world, 23 we compared multiple methods of characterizing 1-year functional dependence in participants admitted to inpatient rehabilitation with DoC. Our primary aims were to: 1) characterize and compare the score distribution of three disability scales: the FIM, GOSE, and DRS and 2) assess the accuracy of GOSE and DRS dichotomization cut-points for identifying participants scoring in the dependent range on the FIM (i.e., FIM-dependency, total score <80). In exploratory analyses, we used a data-driven approach to derive optimal GOSE and DRS cut-points for classifying FIM-dependency. Finally, we developed a simple, binary dependency score derived from a subset of DRS items (the DRSDepend score), and compared this measure with the FIM, GOSE, and DRS total-score cut-points.
Methods
We conducted a retrospective analysis of a prospective longitudinal cohort study of participants enrolled in the TBIMS NDB. 23 Characteristics of this continuously enrolling database have been described previously. 1,24,25 The sample includes participants who survived acute hospitalization and were admitted to one of 16 inpatient rehabilitation centers in the United States that participate in the TBIMS program. This study was approved by the Massachusetts General Brigham Institutional Review Board (IRB; Protocol #2012P002476) and by IRBs at each participating center in the TBIMS NDB.
TBIMS procedures and study sample
As described previously, TBIMS participants are survivors of acute moderate or severe TBI and are 16 years or older at injury onset. 1,26 For this study, we included participants admitted to an inpatient rehabilitation facility with DoC, defined here and in prior studies 1,3 as an admission DRS motor item score >0 (i.e., absence of command following). We excluded participants who did not have a FIM score and either the DRS or GOSE acquired at 1-year (365 ± 60 days post-injury, as recommended by the TBIMS standard operating procedure). 26 Among 18,486 participants in the TBIMS database enrolled between October 1, 1988 and September 4, 2020, our final cohort included 1483 participants with DoC who met inclusion criteria (Fig. 1).
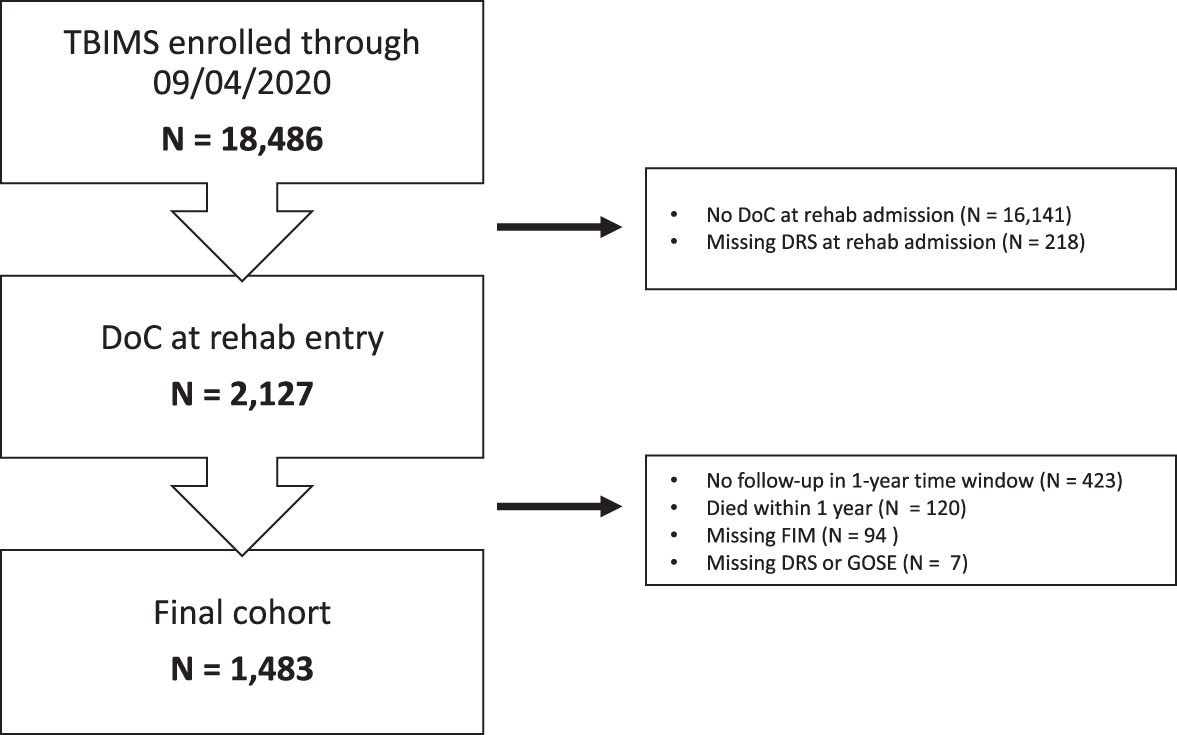
Cohort description. Study CONSORT diagram. DoC, Disorders of Consciousness; DRS, Disability Rating Scale; FIM, Functional Independence Measure; GOSE, Glasgow Outcome Scale Extended; TBIMS, Traumatic Brain Injury Model Systems.
Measures
The TBIMS NDB includes demographics and TBI characteristics, as well as acute care hospital, rehabilitation, and follow-up outcome variables. 1,26 Follow-up assessments are conducted at 1 year, 2 years, 5 years, and every 5 years after injury until death or withdrawal from the study. Study investigators are trained to collect data from the medical record and to perform all assessments in accordance with quality control guidelines maintained by the TBIMS National Data and Statistical Center. 26 We selected the 1-year time-point for analysis, as it has been previously shown to reflect the range of longer-term outcomes in TBIMS participants with DoC on rehabilitation admission. 3
FIM
The FIM instrument includes a series of standardized questions assessing the degree of caregiver support required to accomplish basic cognitive and motor tasks, with total scores ranging from 18 (most dependent) to 126 (least dependent). 16 Based on external validation studies 13 –15,18 and recent observational studies in this cohort, 1 we defined functional dependency as FIM total score <80 (FIM-dependency). We used the FIM as our study reference standard because of its granularity and extensive validation in multiple previous investigations. 13 –15,18
GOSE
The GOSE is an 8-point scale ranging from 1 (Death) to 8 (Upper Good Recovery), based on degree of functional difficulties in major life domains. 20,27,28 Although the GOSE can be analyzed ordinally, 29 it is often dichotomized into favorable and unfavorable outcomes, with an unfavorable cut-point set at ≤3 (Lower Severe Disability, e.g., cannot be left unsupervised in the home for more than 8 h) 2,30 –32 or ≤4 (Upper Severe Disability, e.g., can be left unsupervised in the home for more than 8 h, but dependent outside the home). 33 –35 We assessed the performance of these cut-points and determined a data-derived optimal threshold for classifying FIM-dependency.
DRS
The DRS combines the three items of the Glasgow Coma Scale 36 with five additional measures. 8 These additional measures evaluate a subject's awareness of how and when to feed, groom, and toilet (0: complete awareness to 3: no awareness), level of functional dependence on others (0: completely independent to 5: totally dependent), and employability (0: not restricted to 3: not employable). The eight-item scores are then summed to generate a total score of 0 (least disabled) to 30 (dead). 8 Prior observational and interventional studies 2,37 have categorized DRS total scores into ad hoc clinical categories including None (0), Mild (1), Partial (2–3), Moderate (4–6), Moderately Severe (7–11), Severe (12–16), Extremely Severe (17–21), Vegetative State (22–24), and Extreme Vegetative State (25–29) (Supplementary Table S1). 8 We evaluated the performance of the Severe Disability cut-point (scores ≥12), as well as a data-driven optimal cut-point for classifying FIM-dependency.
DRSDepend
Based on the standardized survey instrument, the GOSE cut-points of ≤3 and ≤4 represent some degree of in-home dependence, 38 although not necessarily resulting from cognitive impairment. The DRS cut-point of Severe Disability (score ≥12) cannot be directly mapped onto level of dependence. We generated a binary DRS rating (the DRSDepend) using a subset of DRS items and tested whether this rating classified FIM-dependency better than the GOSE and total DRS. We defined DRSDepend as a DRS profile with Level of Functioning ≥4 (indicating the need for assistance with all activities at all times), and a score of >0 (some assistance needed) on at least one of the following items: Verbal, Feeding, Toileting, or Grooming. Participants meeting DRSDepend criteria, therefore, require the assistance of another person at all times, and that need is based, at least partially, on cognitive impairment. We evaluated the performance of the DRSDepend for classifying FIM-dependency.
Statistical analysis
First, we compared baseline demographics and injury characteristics of participants who completed the 1-year follow-up assessment (n = 1483) with those who missed the 1-year follow-up or died (n = 644) using T (continuous, normally distributed variables), Wilcoxon (continuous, non-normally distributed variables), or χ2 (categorical variables) tests (Table 1).
Demographic and Injury Characteristics of Participants Diagnosed with DoC on Admission to Rehabilitation
57% un-scorable (due to intubation + sedation/paralytic).
Bold text indicates a significant difference between groups.
DoC, Disorders of Consciousness; DRS, Disability Rating Scale; GCS, Glasgow Coma Scale; IQR, interquartile range; IVH, intraventricular hemorrhage; SD, standard deviation; SDH, subdural hemorrhage; SAH; subarachnoid hemorrhage; TBI, traumatic brain injury.
For the primary analysis, we measured performance characteristics for DRS and GOSE cut-points for classifying participants meeting our reference standard criteria for FIM-dependency. For each cut-point, we computed classification performance measures, including area under the receiver operating characteristic curve (AUROC), sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), using 95% confidence intervals (CIs) generated from 1000 bootstrapped samples, with performance assessed in the out-of-bag sample (R package: cutpointr). 39 An applied definition of each performance measure is provided in Supplementary Table S2.
In an exploratory analysis, we defined the optimal GOSE and DRS-based thresholds for identifying FIM-dependency. We serially assessed every possible GOSE and DRS dichotomization cut-point, finding the value for each scale that minimized the number of FIM misclassifications. We based our analysis on the assumption that false-positives (inappropriately classifying an independent patient as dependent) represent an error with more clinical consequences than false-negatives (inappropriately classifying a dependent patient as independent) and assigned a 2:1 false-positive to false-negative misclassification penalty (R: cutpointr). 39 We then compared the resulting AUROC of these data-driven thresholds with the DRSDepend using Delong's test.
Results
Study population
Within the TBIMS database (n = 18,486), 2127 participants met criteria for DoC on arrival to inpatient rehabilitation; 1483 survived and were assessed with the FIM and either a DRS or GOSE at 1-year post-injury (Fig. 1). In most participants (n = 1351, 91%), all three scores were acquired. In 36 participants (2%), the DRS was missing (i.e., only the GOSE and FIM were acquired at 1-year post-injury), and in 96 participants (6%) the GOSE was missing (i.e., only the DRS and FIM were acquired). Characteristics of the participants meeting criteria for DoC at rehabilitation admission are listed in Table 1. Compared with those who died or had missing outcome data at 1 year (n = 644), participants with follow-up (n = 1483) were younger (95% CI for age difference: −3 to −6 years, p < 0.001), had less severe DRS scores at rehabilitation discharge (95% CI for score difference: −2 to 0, p < 0.001), and were more likely to have had a high-velocity injury mechanism, intracranial hypertension, or intraventricular hemorrhage (Table 1). For a comparison of participants missing 1-year DRS with those missing 1-year GOSE scores, see Supplementary Table S3.
Score distributions for the FIM, GOSE, and DRS
The FIM, GOSE, and DRS total scores were non-normally distributed (all p for Shapiro-Wilk test <0.001). At 1-year post-injury, different proportions of participants met criteria for FIM-dependency (total score <80, 24%, Fig. 2A), Lower Severe Disability on the GOSE (scores <3, 44%, Fig. 2B), and Severe Disability on the DRS (scores ≥12, 15%, Fig. 2; χ2 = 312, p < 0.001). Whereas the FIM (median [1st quartile, 3rd quartile]: 112 [83, 121], mode: 126, Independent) and DRS (median: 5 [2, 8], mode: 0, No Disability) distributions skewed toward the no disability scale extremes, the GOSE distribution skewed toward the severe disability scale extreme (median 4: [3, 6], mode: 3, Lower Severe Disability).
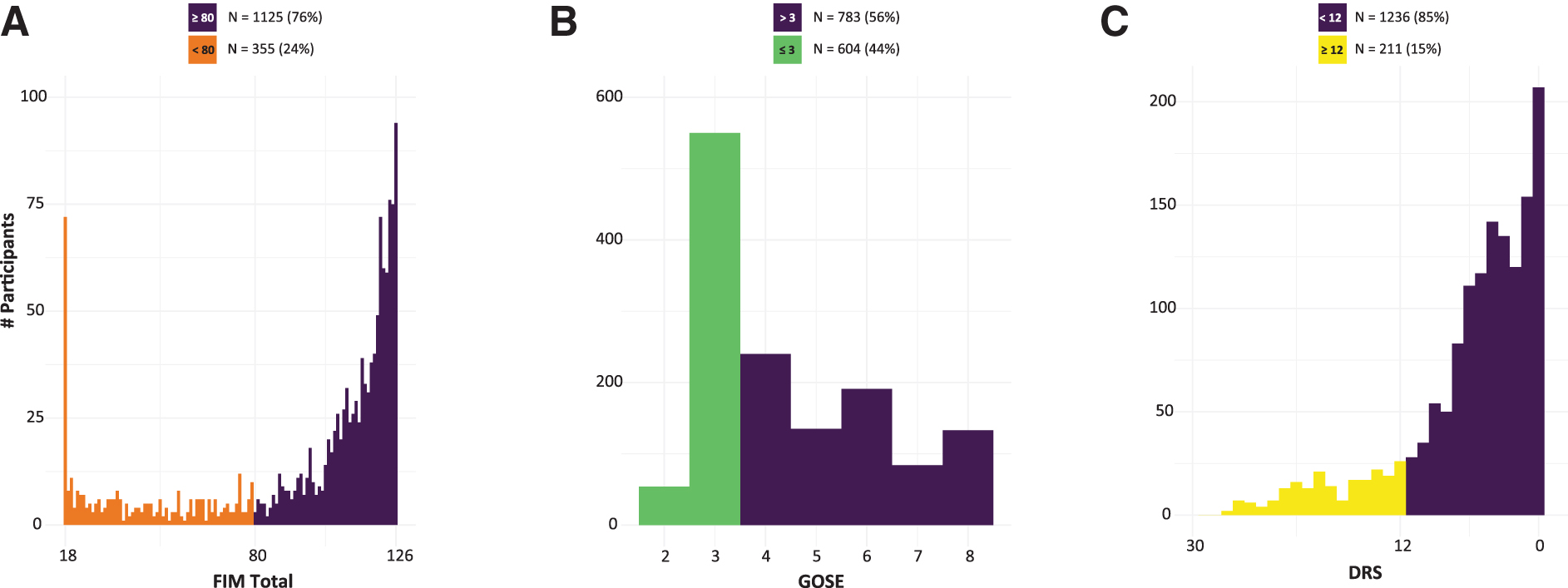
One-year outcome distribution differs by disability scale. Histogram of number of patients with each score on the
Cross-scale correlations and performance characteristics
We next evaluated cross-scale correlations and the performance of different GOSE and DRS thresholds in classifying participants with FIM-dependency.
GOSE and FIM
Although there was a significant correlation between GOSE and FIM total scores (Spearman's rho = 0.8, p < 0.001), total FIM scores of participants with the most common GOSE score (i.e., 3, Lower Severe Disability) were distributed across the full range of the FIM (Fig. 3A). The performance characteristics of the GOSE <3 and GOSE <4 cut-points for classifying FIM-dependency are shown in Table 2. Whereas both cut-points had sensitivities and NPVs for FIM-dependency of at least 97%, the specificities were 74% (bootstrapped 95% CI: [71–77%], GOSE <3) and 51% ([48–54%], GOSE <4), and PPVs were 54% ([50–59%], GOSE <3) and 39% ([36–43%], GOSE <4). Although 99% of participants with GOSE scores >3 or >4 did not meet FIM-dependency criteria, only 54% of participants with GOSE scores <3, and 39% of participants with GOSE scores <4, met FIM-dependency criteria. These results were unchanged in the subset of participants (n = 1351) with no missing outcome measures (Supplementary Table S4).
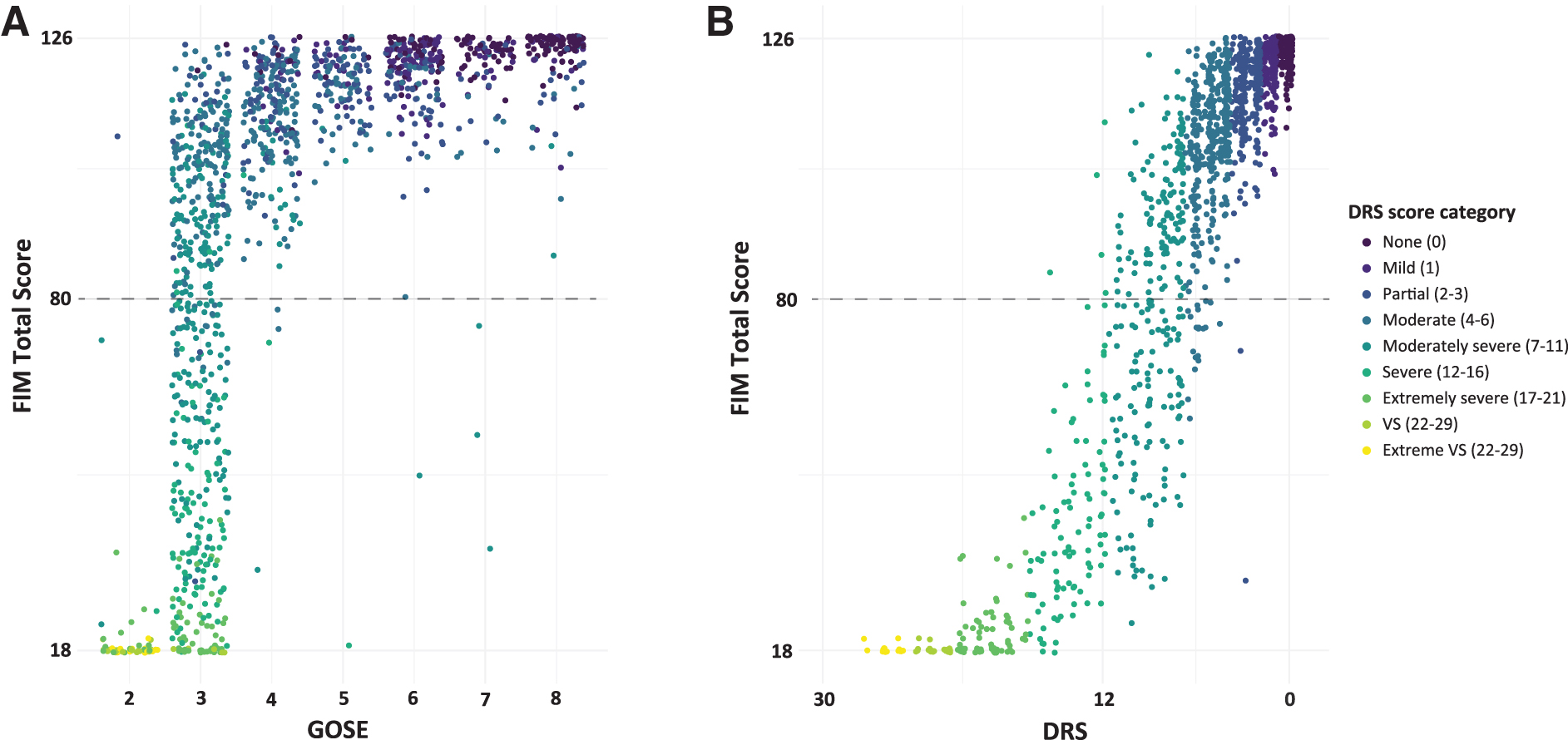
Distribution of GOSE and DRS scores compared with the FIM at 1-year post-injury. GOSE scores
Performance of GOSE and DRS Cut-Points for Identifying FIM-Dependent Participants
literature-derived cut-point; bdata-derived cut-point.
AUROC, area under the receiver operating characteristic curve; CI, confidence interval; DRS, Disability Rating Scale; GOSE, Glasgow Outcome Scale-Extended; NPV, negative predictive value; PPV, positive predictive value.
DRS and FIM
The DRS and the FIM were also correlated (Spearman's rho = −0.9, p < 0.001, Fig. 3B). Similar to participants with GOSE scores of 3, we found that subjects with modal DRS scores (Moderate Disability, total scores: 4–6) spanned a wide range of FIM scores (Fig. 3B, blue-green). Whereas the DRS cut-point of Severe Disability or worse (DRS >12) had specificity and PPV for FIM-dependency of greater than 98%, the sensitivity was 60% (54–66%) and the NPV was 89% (87–91%). Although 98% of participants with DRS scores >12 met criteria for FIM-dependency, only 60% of participants who met criteria for FIM-dependency also had DRS scores >12. These results were unchanged in the subset of participants with no missing outcome measures (Supplementary Table S4).
Exploratory analyses
The data-derived optimal cut-points for identifying FIM-dependency were GOSE <3 and total DRS >10 (Table 2). As measured by the AUROC, there was no difference in the discriminative capacity between the optimal GOSE (GOSE <3: AUROC 0.85 [0.84–0.87]) and DRS (DRS >10: AUROC 0.86 [0.83–0.88]) cut-points (p = 0.7).
DRSDepend
We assessed the classification performance of a DRS-based functional dependency metric, the DRSDepend. The DRSDepend classified FIM-dependency with 83% (78–87%) sensitivity, 94% (93–96%) specificity, PPV of 82% (78–87%), NPV of 95% (93–96%), and an AUROC of 0.89 (0.86–0.91; Table 2 and Fig. 4). The DRSDepend discriminated FIM-dependency better than the data-derived optimal GOSE (p = 0.01) and DRS (p = 0.008) cut-points.
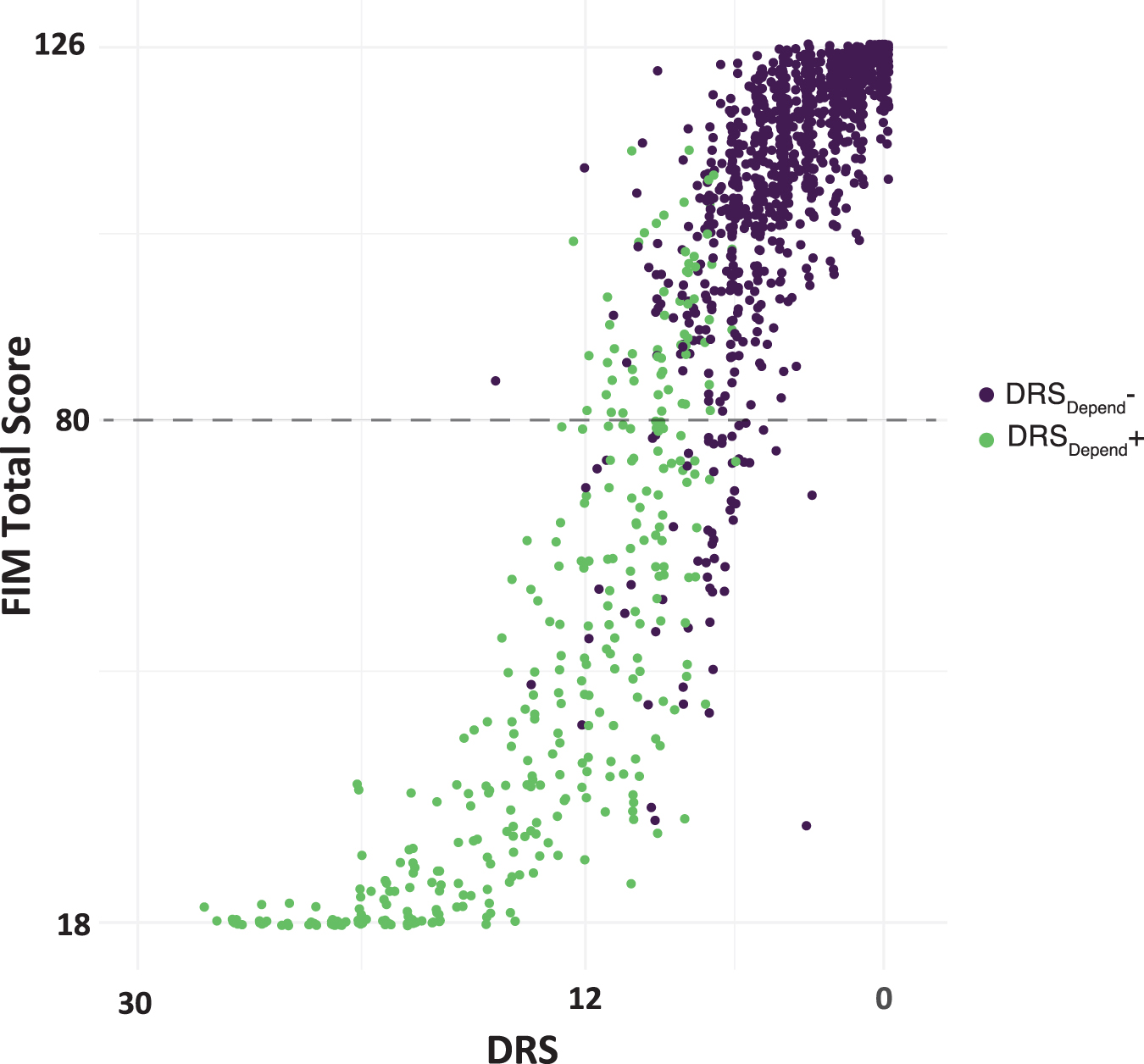
DRSDepend classifies patients with FIM scores <80. DRS scores are plotted against FIM total scores. Points are randomly jittered to avoid overlap. Green color indicates the participant met criteria for DRSDepend, a novel DRS-based measure that seeks to identify participants dependent on others to meet basic needs, and whose impairment is at least partly due to cognitive impairment. The dashed line signifies a FIM total score of 80. DRS, Disability Rating Scale; FIM, Functional Independence Measure.
Discussion
In this study, we examined the concordance between FIM, GOSE, and DRS scores acquired 1-year post-injury in TBI survivors diagnosed with DoC on arrival to inpatient rehabilitation. We quantified the performance of literature-derived and data-driven GOSE and DRS cut-points at identifying participants who meet criteria for complete dependence on the FIM. Two common GOSE cut-points for unfavorable outcome (i.e., ≤3 and ≤4, Lower and Upper Severe Disability, respectively) overestimated functional impairment, classifying as “dependent” 46–61% of participants who did not meet FIM-dependency criteria. Conversely, a DRS cut-point of Severe Disability failed to correctly identify 40% of participants meeting FIM-dependency criteria. Finally, we defined and evaluated the DRSDepend, a composite, binary rating of functional dependency due, at least in part, to cognitive impairment. We found that the DRSDepend demonstrated better FIM-dependency classification performance than either the GOSE or DRS cut-points.
Our findings highlight the wide range of functional impairment within dichotomized GOSE and DRS categories and demonstrate fundamental differences in the calibration of these outcome scales. Most participants in this study achieved a 1-year GOSE score of 3 (Lower Severe Disability), just one category above Vegetative State and typically considered an unfavorable outcome. 2,30 –35 GOSE ≤3 was a highly sensitive but non-specific marker for FIM-dependency. Nearly all participants with FIM-dependency also had GOSE scores ≤3, but almost half of participants with GOSE ≤3 did not meet FIM-dependency criteria—with total FIM scores that spanned nearly the full range of the FIM scale. The specificity of the often-used GOSE ≤4 cut-point was even lower. More than 60% of participants with GOSE ≤4 did not meet FIM-dependency criteria.
In contrast to the GOSE, the distribution of DRS scores skewed toward the milder end of the scale, suggesting a greater potential for determining meaningful functional differences between patients with DoC after TBI. However, like the GOSE ≤3 category, we found that common DRS total score groupings reported in prior studies (e.g., Moderate and Moderately Severe), 2,8,37 also spanned a wide range of FIM total scores. Although there is less precedent for dichotomizing the DRS, we found that a cut-point of at least Severe Disability (DRS >12) was a specific, but insensitive marker of FIM-dependency. Indeed, 40% of participants with FIM-dependency had DRS scores of Moderately Severe Disability or better.
Our data-driven analysis identified the optimal GOSE and DRS cut-points for identifying participants meeting criteria for FIM-dependency. The optimal GOSE cut-point was ≤3, a threshold commonly used in TBI studies. 2,30 –32 Because even this optimal cut-point has a PPV of only around 50% for FIM-dependency, dichotomizing outcomes using the GOSE should be done cautiously in studies enrolling patients with severe brain injury. We found that the data-derived optimal DRS cut-point of >10 did not have an overall better discriminative performance (as measured by the AUROC) than GOSE ≤3. However, the higher specificity and PPV of the DRS cut-point relative to the GOSE results in fewer participants falsely characterized as having complete dependency.
Finally, we derived and evaluated the DRSDepend, a novel metric that identifies participants who are dependent on others to meet basic needs, and whose impairment is at least partly due to cognitive impairment. The DRSDepend outperformed data-derived optimal GOSE and DRS cut-points at identifying participants with FIM-dependency. External validation, as well as caregiver and patient perspectives on whether the DRSDepend accurately discriminates between acceptable and unacceptable outcomes, 9 requires further investigation.
Limitations
Our findings should be interpreted in the context of several limitations. First, there is no internationally accepted gold standard for quantifying disability and defining functional dependency. We chose the FIM as our reference standard because it is associated with daily hours of required functional assistance (burden of care), 11 –14,16 has an established cut-point (total score <80) for defining complete dependency, 15,16 and was previously used in this population to define dependency. 1 Nonetheless, how this FIM threshold compares with the ground truth level of impairment is unknown. We did not employ the more comprehensive FIM + Functional Assessment Measure 40 combined assessment, as it is not acquired as part of the TBIMS standard operating procedure.
Our study included only participants enrolled in the TBIMS with DoC on admission to inpatient rehabilitation. Restricting the study to participants with DoC may have resulted in an excess of 1-year GOSE >3 scores relative to all patients with moderate or severe TBI. Analyzing such a skewed GOSE distribution may have yielded systematically lower estimates of cross-scale concordance and classification performance. In addition, whether our results generalize to individuals with DoC who do not receive inpatient rehabilitation requires further investigation.
Conclusion
The GOSE, DRS, and FIM have markedly different score distributions in patients recovering from DoC at 1-year after TBI. Literature-derived GOSE cut-points have low specificity and DRS cut-points have low sensitivity for identifying participants with FIM-dependency. A novel and simple DRS-based metric of dependency, the DRSDepend, identifies patients meeting criteria for FIM-dependency better than GOSE or DRS total-score cut-points. As such, clinical studies seeking a binary dependency end-point in severely brain injured subjects should consider using the DRSDepend in addition to GOSE or DRS total scores.
Footnotes
Acknowledgments
This article was developed under grants from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR; Spaulding Rehabilitation Hospital and Indiana University). The NIDILRR is a center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this article do not necessarily represent policy of the NIDILRR, ACL, or HHS, and endorsement by the federal government should not be assumed.
This article was previously submitted as a preprint to medRxiv (
Funding Information
S.B.S. receives funding from the American Academy of Neurology (Clinical Research Training Scholarship). R.G.K. receives funding from the National Institutes of Health (NIH) National Institute of Neurological Disorders and Stroke. F.M.H. receives funding from the NIDILRR (grants 90DPTB0002, 90DPHF0006, 90DPTB0017, and 90RTEM0008); the NIH (UG3NS117844 and 1R01NS118009); the Patient-Centered Outcomes Research Institute (PCORI; UWSC9923/PCS-1604-35115); the Department of Defense (W81XWH-18-1-0796); the University of California, San Francisco; and the University of Michigan (SUBK10416CSPR-002). S.I. receives funding from the Neurocritical Care Society (Research Fellowship Award). B.L.E. receives funding from the NIH National Institute of Neurological Disorders and Stroke (R21NS109627, RF1NS115268); the NIH Director's Office (DP2HD101400); the James S. McDonnell Foundation; and the Tiny Blue Dot Foundation. Y.G.B. receives funding from the NIH National Institute of Neurological Disorders and Stroke (U01-NS1365885, U01-NS086090); the NIDILRR, ACL (90DPCP0008-01-00, 90DP0039); the James S. McDonnell Foundation; and the Tiny Blue Dot Foundation.
Author Disclosure Statement
S.B.S. is a site investigator on a Biogen-funded clinical trial unrelated to this work. R.D.Z. has received royalties from Springer/Demos for the text Brain Injury Medicine, and serves on the scientific advisory boards of Myomo and One
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.