
Abstract
The bulbocavernosus reflex (BCR) has been used during the initial evaluation of a spinal cord injury patient as a metric to determine prognosis and whether the patient is in “spinal shock.” This reflex has been less utilized over the last decade, and therefore a review was performed to assess the value of BCR in patient prognosis. The North American Clinical Trials Network (NACTN) for Spinal Cord Injury (SCI) is a consortium of tertiary medical centers that includes a prospective SCI registry. The NACTN registry data was analyzed to evaluate the prognostic implication of the BCR during the initial evaluation of a spinal cord injury patient. SCI patients were divided into those with an intact or absent BCR during their initial evaluation. Associations of participants' descriptors and neurological status on follow-up were performed, followed by associations with the presence of a BCR. A total of 769 registry patients with recorded BCRs were included in the study. The median age was 49 years (32-61 years), and the majority were male (n = 566, 77%) and white (n = 519, 73%). Among included patients, high blood pressure was the most common comorbidity (n = 230, 31%). Cervical spinal cord injury was the most common (n = 470, 76%) with fall (n = 320, 43%) being the most frequent mechanism of injury. BCR was present in 311 patients (40.4%), while 458 (59.6%) had a negative BCR within 7 days of injury or before surgery. At 6 months post-injury, 230 patients (29.9%) followed up, of which 145 had a positive BCR, while 85 had a negative BCR. The presence/absence of BCR was significantly different in patients with cervical (p = 0.0015) or thoracic SCI (p = 0.0089), or conus medullaris syndrome (p = 0.0035), and in those who were American Spinal Injury Association Impairment Scale grade A (p = 0.0313). No significant relationship was observed between BCR results and demographics, AIS grade conversion, motor score changes (p = 0.1669), and changes in pin prick (p = 0.3795) and light touch scores (p = 0.8178). In addition, cohorts were not different in surgery decision (p = 0.7762) and injury to surgery time (p = 0.0681). In our review of the NACTN spinal cord registry, the BCR did not provide prognostic utility in the acute evaluation of spinal cord injury patients. Therefore, it should not be used as a reliable marker for predicting neurological outcomes post-injury.
Introduction
The bulbocavernosus reflex (BCR) is a commonly examined reflex in the setting of an acute spinal cord injury. First described by Bors in 1959, it is often tested by squeezing the glans penis or the clitoris, resulting in contraction of the bulbocavernosus muscles and/or the external anal sphincter. 1 -3 A positive BCR indicates the presence of an intact spinal reflex arc of the S2-4 spinal cord segments via the pudendal nerve. 1 In neurologically intact patients without spinal cord injury, Blaivas and colleagues demonstrated the BCR was present in 98% of men and 81% of women. 2 Given the anatomy of the reflex arc that it tests, the BCR is often used to help distinguish a conus medullaris from a cauda equina injury. 1 However, the BCR is often used as a surrogate marker for the presence or absence of spinal shock or the for the severity of the spinal cord injury. 4 Despite its widespread use in evaluating spinal cord injuries, there is little data to support its importance during the acute evaluation of a spinal cord injured patient. The goal of this study is to determine if the BCR had any prognostic value when evaluating an acute spinal cord injury using the North American Clinical Trials Network (NACTN) for Spinal Cord Injury (SCI) registry.
Methods
NACTN SCI registry data were used for this project. Details of this registry and data preprocessing are described in the paper entitled “North American Clinical Trials Network (NACTN) Spinal Cord Injury (SCI) Registry: Methodology and Analysis” found within this special edition.
Participants who had a spinal cord injury, excluding those with cauda equina syndrome, and had a recorded BCR (performed within 7 days of injury or before surgery) at the time of their initial evaluation were included in the study. Demographic, initial clinical evaluation, American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade, complications and discharge files were screened to obtain characteristics and outcomes of the retained participants. The initial clinical status of the individual was also noted by measuring systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), and Acute Physiologic Assessment and Chronic Health Evaluation (APACHE) II score. Additional characteristics included comorbidities (high blood pressure, diabetes, heart attack, pulmonary, smoking, and drug abuse) and initial ASIA measures (AIS grade, motor scores, pin prick scores, light touch scores). Initial ASIA measurements were the first measures taken before surgery or within 7 days for those who did not undergo surgery. These variables were obtained directly from the database except for MAP, which was calculated as (SBP +2DBP)/3. The primary outcome was the AIS examination measures at the time of follow-up. Secondary outcomes were surgical intervention, length of stay, mortality, discharge disposition and complications.
Statistical analysis
Participant descriptors and outcomes were presented with summary statistics and compared between groups with two-sample t-test or Brown-Mood test as appropriate for continuous variables, and with chi-squared test or Fisher's exact test as appropriate for categorical variables. All tests were two-sided with a significance level of 0.05. Data analysis was performed in SAS 9.4 (SAS Inc., Cary, NC).
Results
Patient inclusion and bulbocavernosus reflex (BCR)
Of the 989 patients in the registry, 769 patients had a BCR test documented on their initial exam, and in these patients, the BCR was present in 311 patients (40.4%), while 458 (59.6%) had a negative BCR upon presentation. Six-month outcome data were available for 230 (29.9%) patients, of which 145 had a positive BCR while 85 had a negative BCR (Fig. 1).
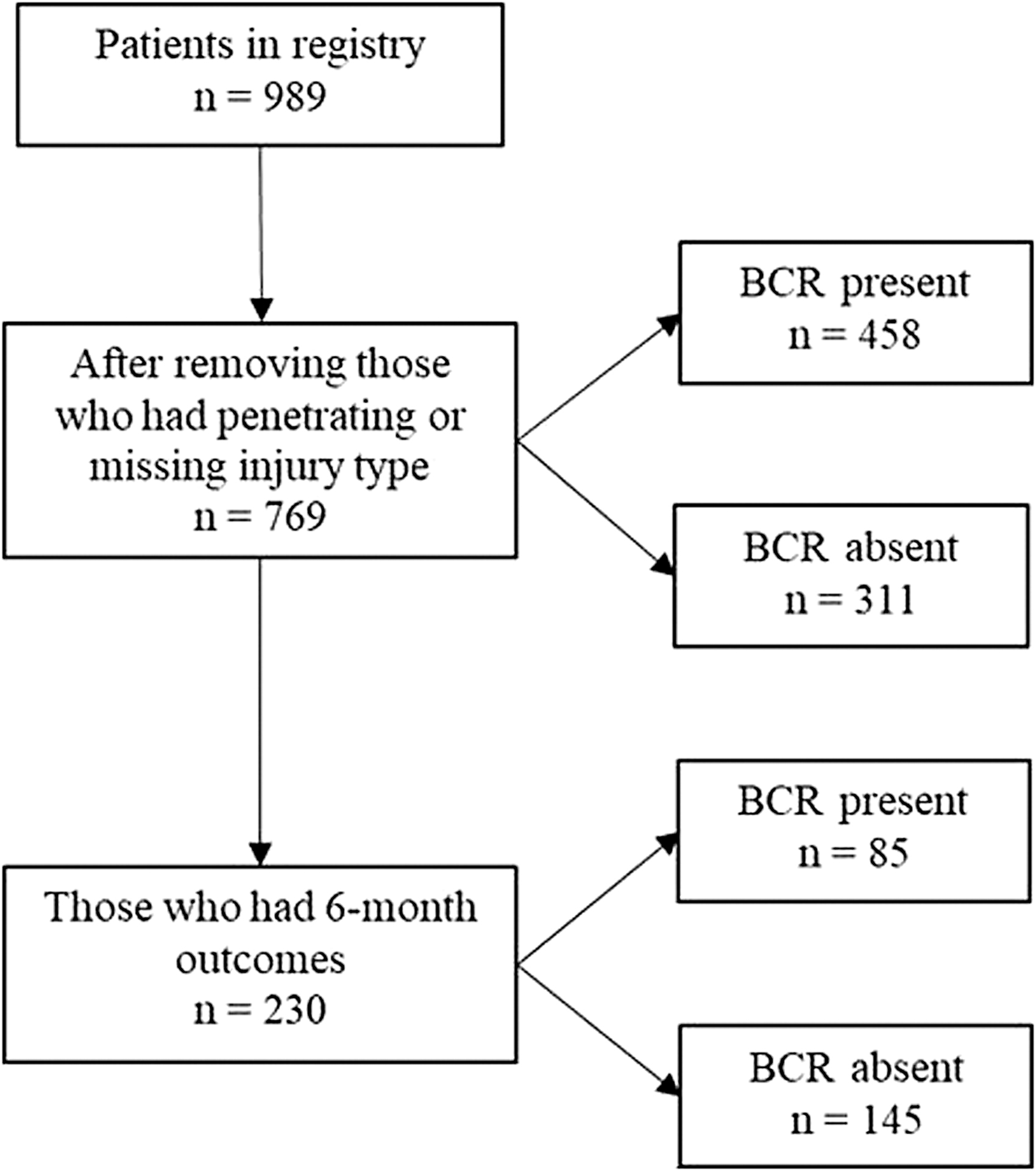
Flow chart depicting the data preparation and participant inclusion process
Patient characteristics and BCR
Among the 769 spinal cord injury patients, the median age was 49 years (interquartile range [IQR]: 32-61 years), and the majority were male (n = 566, 77%) and white (n = 519, 73%). Within participants, the most common comorbidities were high blood pressure (n = 230, 31%), diabetes (n = 168, 23%), and preexisting pulmonary conditions (n = 142, 19%). Motor vehicle accident (n = 310, 41%) and fall (n = 320, 43%) were the most common mechanisms of injury. The majority of the patients had cervical spinal cord injury (n = 470, 76%). Within included patients, 169 (36%) had central cord syndrome, while 16 (3%) had conus medullaris syndrome. During the initial clinical assessment, patients had a median SBP of 124 (IQR: 108-142), DBP of 73 (IQR: 62-85), MAP of 91 (IQR: 79-104), and APACHE II of 6 (IQR: 3-10). While assessing initial AIS grade, AIS grade A (n = 233, 40%), followed by AIS grade D (n = 184, 31%) were the most common. The median motor, pin prick, and light touch scores were 48, 62, and 67, respectively. A statistically significant relationship was noted between the BCR results and cervical SCI (p < 0.05), thoracic SCI (p < 0.05), conus medullaris syndrome (p < 0.05), and AIS grade A (p < 0.05).
Relationship of BCR with peri-operative outcomes
Within included participants, 702 (95%) underwent spinal surgery. No statistically significant relationship was observed between BCR results and the decision to recommend surgery (p = 0.7762), or time from injury to surgery (p = 0.0681; Table 1). No significant relationship was observed between timing of BCR assessment, and time from injury to arrival (p = 0.1183), arrival to surgery (p = 0.6432), and injury to surgery (p = 0.6432; Fig. 2). A statistically significant relationship was observed between BCR results and incidence of gastrointestinal/genitourinary (GI/GU) complications (p = 0.0007; Table 2).
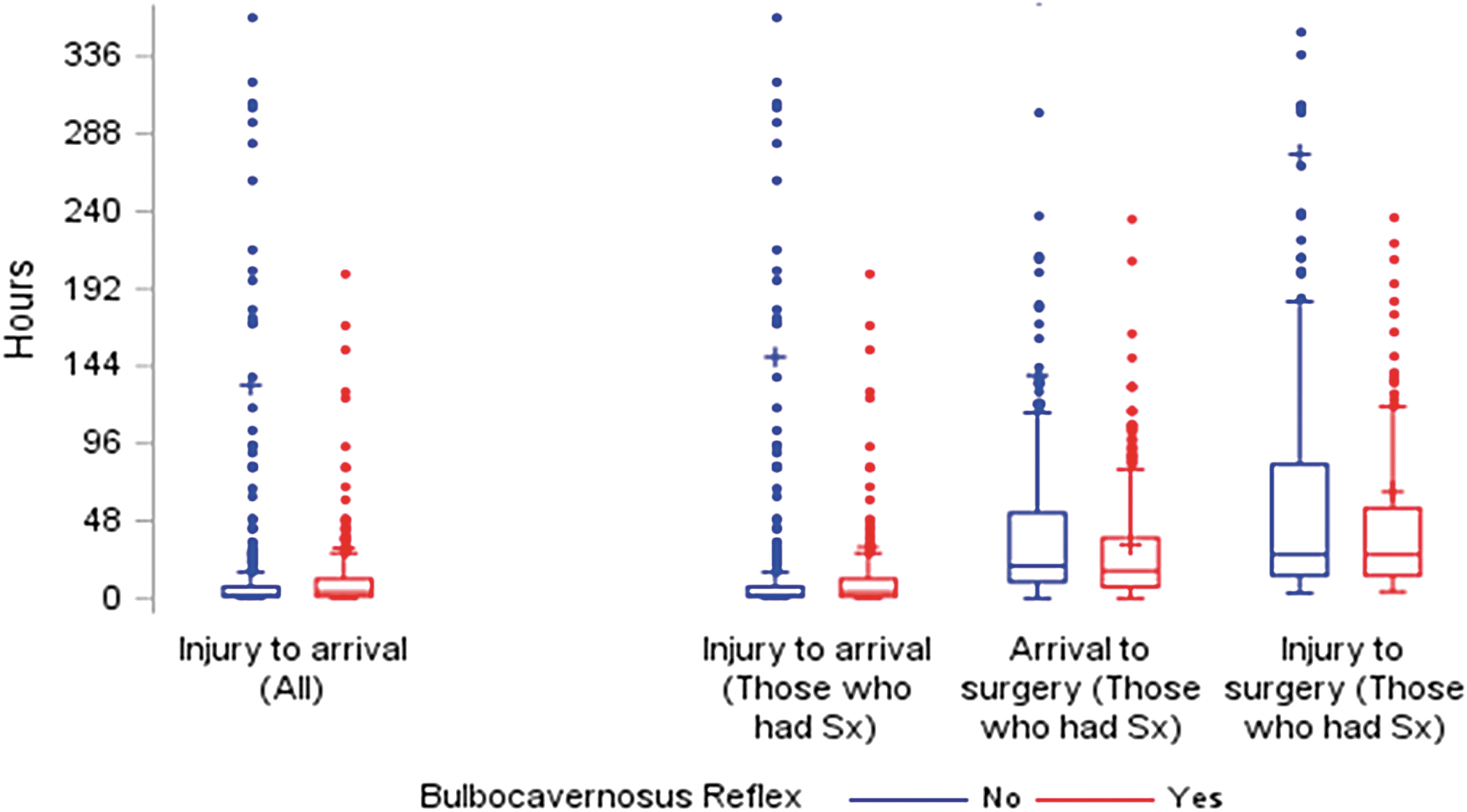
Timing of injury to arrival and surgery stratified by presence or absence of bulbocavernosus reflex (BCR).
Participants Undergoing Surgery and Timing of That Surgery Stratified by Presence or Absence of Bulbocavernosus Reflex (BCR)
Hospitalization Outcomes for Participants Included in This Study Stratified by Whether They Had Bulbocavernosus Reflex (BCR) or Not
LOS, GIGU.
Relationship between follow-up ASIA conversion and BCR
Of 769 patients with spinal cord injury, 230 were followed up at 6 months post-injury. At 6 months, there was no difference in outcomes regarding regression (p = 0.2805), and no change (p = 0.5605) or improvement in their AIS grade (p = 0.3691), based on the initial presence or absence of BCR. During follow-up, no significant change was observed in median motor (p = 0.1669), pin prick (p = 0.3795), and light touch scores (p = 0.8178) in patients based on their initial BCR results (Table 3). At 6 months post-injury, no statistically significant ASIA conversion was noted for patients based on BCR results.
AIS Change From Initial AIS Within 7 Days of Injury to 6 Months Post-Injury
Discussion
The results of this study show that a statistically significant relationship exists between BCR findings and patients presenting with cervical or thoracic SCI, conus medullaris syndrome, and AIS grade A injuries. Moreover, BCR results significantly correlated with the incidence of GI/GU complications post-injury. However, the presence or absence of the BCR did not affect the decision to perform surgery or the time from injury to surgery. At 6 months follow-up, no significant ASIA conversion was noted for patients based on BCR results.
A review of the literature shows a paucity of data related to the BCR in the acute period and what it signifies. Specifically, the BCR in the acute period has not been previously reported as being a useful prognostic indicator to predict neurological recovery, complete versus incomplete lesions, the presence of spinal shock, or bladder function. The reason for attempting to identify prognostic factors in the early period after a spinal cord injury is an attempt to determine the best treatment strategies to include the need for surgical and medical management that would result in the best outcome for the patient with the least amount of risk. This may include decisions to perform early surgery, ultra-early surgery, or novel medical therapies. 5 -7
A complicating factor in the early period after spinal cord injury is the concept of spinal shock, a period of depressed or absent reflexes occurring below the level of injury after a patient suffers a spinal cord injury. 8 It is often incorrectly assumed that the absence of the BCR indicates spinal shock after a SCI and the return of the BCR equates to the resolution of spinal shock. In a study by Ko and colleagues, the delayed plantar response was the first reflex to typically return after an initial period of areflexia after a SCI. 4 With careful neurological examination, they found that most complete SCIs had two or more reflexes present, including the BCR, during an initial evaluation occurring within 3 h of injury. However, they found that the presence of reflexes during the acute period had no bearing on ambulation status at follow-up. Additionally, there was no difference between the return of the BCR in complete versus incomplete injuries. 4
In an attempt to offer a new definition of spinal shock, Ditunno and colleagues identified four phases of spinal shock that can last for weeks to months. 8 The initial phase of spinal shock in this model is present during the first day and is associated with areflexia to hyporeflexia. During Phase 2 of their paradigm of spinal shock, ending within the first 3 days after a SCI, the BCR along with other cutaneous reflexes can start to return and become stronger. 4,8 While often an early reflex to recover, the BCR is not the last reflex to return after a SCI. This model goes on to describe the final two stages of spinal shock starting around Day 4 and lasting for months afterwards, incorporating the development of hyperreflexia and spasticity.
In one of the only other articles to specifically examine the BCR and its prognostic value, Greciet and colleagues recently performed a retrospective review of 45 patients with a motor complete spinal cord injury without a conus abnormality to evaluate the association of the BCR with neurological and functional improvement at 6 to 12 months after injury. They found no statistical difference in the rate of ASIA grade conversion, improvement in level of injury, or functional scores between those with or without a BCR during the initial evaluation period. While the authors noted that the small sample size limited differences in outcome reaching statistical significance, they still concluded that a delay in the recovery of BCR in motor complete SCIs may indicate a worse prognosis for recovery. 9 Additionally, their findings challenged Ditunno and colleagues' time course of spinal shock recovery given that 40% of their patients did not recover their BCR by 7 days post-injury.
In 2003, Schurch and colleagues evaluated 55 patients with SCI from thoracolumbar fractures to evaluate the correlation of early neurological examination findings, and the presence of a neurogenic bladder and the potential for bladder function recovery. 10 The mean time for their initial neurological examination was 16 days ±23, with a mean of 9 days. They found no correlation between the presence or absence of the BCR and the degree of bladder dysfunction or the ability to voluntarily contract the external anal sphincter. Follow-up examinations occurred 698 ± 92.2 days, with a mean of 481 days. The authors found that those with incomplete injuries were much more likely to demonstrate a BCR. In patients with complete neurogenic bladder, a BCR was present in those patients with upper motor neuron lesions but not in those patients with lower motor neuron lesions. They concluded that the presence of the BCR correlates with completeness of the spinal cord injury. However, this was not able to be determined early in the injury course, but only after almost 2 years from the time of injury.
While the BCR may allow determination of an upper motor neuron from a lower motor neuron lesion during long-term follow-up it may not be the best test. Kirschblum and colleagues has advocated that the BCR be replaced by the anal reflex since it is less invasive, offers similar information, and is essentially already a part of the International Standards for Neurological Classification of Spinal Cord Injury examination. 11
This study has some limitations. First, we did not evaluate the use of BCR as a tool to detect spinal shock, and therefore cannot comment on its predictive accuracy for this condition. Secondly, we did not correlate BCR results with type of injury (complete vs. incomplete); therefore, we cannot ascertain its potential use to predict these different injuries. Lastly, since less patients had follow-up examinations at 6 months, more participants would ideally be required to assess correlation between BCR results and ASIA measures conversion.
Conclusion
BCR findings displayed no prognostic utility in the acute evaluation of spinal cord injury in this cohort. Moreover, no significant association was observed between BCR results and changes in AIS grade, motor, or sensory scores at 6 months post-injury. Therefore, our findings indicate that the BCR is not an accurate marker to predict neurological outcomes in patients presenting with spinal cord injury.
Footnotes
Acknowledgments
The views expressed in this manuscript are those of the author(s) and do not necessarily reflect the official policy of the Department of Defense of the U.S. Government.
Authors' Contributions
Daniyal Mansoor Ali: Investigation, methodology, project administration, visualization, validation, writing—original draft, writing—review and editing.
Ahilan Sivaganesan: Project administration, visualization, supervision, validation, writing – original draft, writing – review and editing.
Chris J Neal: Conceptualization, investigation, methodology, project administration, supervision, validation, visualization, writing—review and editing.
Sara Thalheimer: Project administration, writing—review and editing.
Beatrice Ugiliweneza: Data curation, formal analysis, methodology.
Elizabeth G Toups: Project administration.
Muhammad Abd-El-Barr: Supervision, validation, visualization.
George Jimsheleishvili: Data curation.
Shekar N Kurpad: Supervision, validation, writing—review and editing.
Bizhan Aarabi: Supervision, validation, visualization, writing—review and editing.
Christopher I Shaffrey: Supervision, validation.
Michael G Fehlings: Conceptualization, investigation, project administration, supervision, validation, visualization, writing—review and editing.
Charles H Tator: Supervision, validation, visualization, writing—review and editing.
Robert G Grossman: Conceptualization, supervision, validation, visualization.
James D Guest: Conceptualization, project administration, supervision, validation, visualization.
James S Harrop: Conceptualization, investigation, project administration, supervision, validation, visualization, writing—review and editing.
Funding Information
This material is based upon work supported by the U.S. Army Medical Research Acquisition Activity under Grant Nos.W81XWH-07-1-0361, W81XWH-10-2-0042, W81XWH-13-2-0040 and Contract No. W81XWH-16-C-0031, and the Christopher and Dana Reeve Foundation.
Author Disclosure Statement
No competing financial interests exist.