
Abstract
Purpose: To examine associations between parameters of psychological well-being, injury characteristics, cardiovascular autonomic nervous system (ANS) control, and cognitive performance in persons with spinal cord injury (SCI) compared with age-matched uninjured controls. This is an observational, cross-sectional study including a total of 94 participants (52 with SCI and 42 uninjured controls: UIC). Cardiovascular ANS responses were continuously monitored at rest and during administration of the Paced Auditory Serial Addition Test (PASAT). Self-report scores on the SCI-Quality of Life questionnaires are reported for depression, anxiety, fatigue, resilience, and positive affect. Participants with SCI performed significantly more poorly on the PASAT compared with the uninjured controls. Although not statistically significant, participants with SCI tended to report more psychological distress and less well-being than the uninjured controls. In addition, when compared with uninjured controls, the cardiovascular ANS responses to testing were significantly altered in participants with SCI; however, these responses to testing did not predict PASAT performance. Self-reported levels of anxiety were significantly related to PASAT score in the SCI group, but there was no significant relationship between PASAT and the other indices of SCI-Quality of Life. Future investigations should more closely examine the relationship among cardiovascular ANS impairments, psychological disorders, and cognitive dysfunction to better elucidate the underpinnings of these deficits and to guide interventions aimed at improving physiological, psychological, and cognitive health after SCI.
Tetraplegia, paraplegia, blood pressure variability, cognitive, mood.
Introduction
Cognitive dysfunction is pervasive in the spinal cord injury (SCI) population. It has been suggested that more than 60% of individuals with SCI manifest cognitive deficits, 1 which are diverse, impact multiple domains, 2,3 and may differ by the neurological level of injury (NLI). 4 In fact, the relative risk of cognitive impairment is 13 times greater in the SCI population than in uninjured individuals, 5 with processing speed and working memory among the most commonly reported deficits. 2,6
Mood disturbances are also common in individuals with chronic SCI, with reported increases in levels of depression, anxiety, and post-traumatic stress disorder. 7,8 A recent meta-analysis estimates a significantly elevated prevalence of depression in the SCI population of 22% 9 compared with the estimated 16% in the general population. 10 Additional studies indicate that depressive disorders persist throughout the lifespan, and prescribed interventions for depression were ineffective in resolving symptoms in about 2/3rds of the patients with SCI studied. 11
Association between cognitive impairments and depression is reported in the general population, 12,13 which may negatively impact response to treatment of depressive disorders. 14,15 Relevant literature on the potential relationship between psychological disorders, in particular dementia and depressive symptoms, and cognitive dysfunction was recently reviewed and reported in the SCI population, suggesting a combination of biochemical, physiological, and behavioral factors may contribute to cognitive impairments after SCI. 16
Concomitant traumatic brain injury may contribute to the cognitive and mood disorders reported in the SCI population 17 ; however, we and others have begun investigating alternate etiologies including hypotension, 18 cerebral regulatory compromise, 2,19 and inadequate cerebral blood flow responses to neuropsychological (NP) testing. 20,21
An underlying factor that may be responsible for these physiological and regulatory maladaptive changes reported in the SCI population is impaired autonomic nervous system (ANS) function. In fact, we have reported the impact of the loss of descending cortical ANS control on systemic and cerebral hemodynamics during cognitive testing after SCI, 22,23 and others have suggested that the loss of direct sympathetic cerebrovascular control results from transient increases in blood pressure (BP) that occur during autonomic dysreflexia in rodents with T3 SCI. 24 A direct connection between ANS impairments and the cognitive and mood disorders reported after SCI, however, has not been explored.
There is a substantial body of evidence in the general medical literature describing associations between ANS impairment and increased levels of anxiety and depression using parameters of heart rate variability (HRV) as a valid estimate of both autonomic and emotional dysfunction. 25 Variability in heart rate (HR) can be assessed easily non-invasively with an electrocardiogram (ECG) to monitor beat-to-beat fluctuations in the interbeat interval between R-waves (ventricular depolarization).
Higher levels of HR fluctuations are associated with increased parasympathetic (vagal) nerve activity, which provides cardioprotection against myocardial infarction and heart failure. 26 The high frequency component of HRV (HF-HRV), which most directly reflects cardiovagal modulation, is an indicator of autonomic flexibility and has been used to assess emotional responses to psychological stress in everyday life. 27 Two recent meta-analyses have identified significant associations between low levels of HF-HRV and increases in anxiety disorders 28 and depression 29 in the general population.
While significant reductions in resting HF-HRV have been reported in the SCI population, regardless of the NLI or completeness of the injury as assessed by the American Spinal Injury Association (ASIA) impairment scale (AIS), 30,31 associations between low cardiovagal modulation and emotional unrest, anxiety, and depression have not been reported in individuals with SCI.
Yet, diminished HF-HRV in the SCI population may be related to the high prevalence of anxiety and depression, 32,33 because efferent parasympathetic cardiac innervation remains anatomically intact, regardless of the NLI. Further, an association between low resting HRV after SCI and depression was recently reported in male Sprague Dawley rats; 28% of rats exposed to SCI displayed symptoms of depression and HRV was significantly reduced in depressed rats compared with intact control animals. 32
In fact, reports suggest that an integral connection between the heart and the brain may be essential to emotional, psychological, and cognitive well-being. 34 Moreover, while vagal cardiac innervation remains anatomically intact after SCI, efferent sympathetic cardiovascular innervation is impaired in individuals with lesions at or above T6, leading to cardiovascular dysregulation and BP disorders including hypotension, orthostatic hypotension, autonomic dysreflexia and BP instability.
These BP disorders have been associated with maladaptive changes in cerebral blood flow, 35 cerebrovascular responsiveness, 36 and cognitive function. 18 Low frequency (LF) Mayer wave oscillations in systolic BP (SBP) (LF-SBP) reflect a non-invasive estimate of sympathetic vascular responses, 37,38 which can be assessed during cognitive testing in association with performance.
The purpose of this study was to examine associations between injury demographics, parameters of psychological well-being and ANS cardiovascular (HF-HRV and LF-SBP) responses at rest and during cognitive testing, to identify factors that may contribute to the increased reporting of cognitive dysfunction in people with SCI compared with age-matched uninjured controls (UIC).
Methods
Study participants
A total of 140 individuals participated in the study; 94 completed and returned the psychological surveys and are included in these analyses. Participants included 52 individuals with SCI and 42 UIC. Demographic characteristics of the study groups are presented in Table 1.
Participant Characteristics
Data are means ± standard deviation; n, number of participants; SCI, spinal cord injury; AIS, American Spinal Injury Association (ASIA) impairment scale; DOI, duration of injury.
Age did not differ between groups (95% confidence interval [CI] of the mean difference = -9.8 to 0.4 years), and there were more males in both the SCI (87%) and UIC (60%) groups. Of the participants with SCI, 30 had cervical (C3–C7) and 22 had thoracic (T1–T12) lesions, most (81%) were motor complete injuries (AIS A or B), none were ambulatory, and the duration of injury (DOI) was at least 12-months before testing. All participants were proficient in English and demonstrated visual acuity of at least 20/60 in the worst eye (with prescription eyewear).
Potential participants were excluded in the presence of acute illness or infection, a documented history of essential hypertension, diabetes mellitus, traumatic brain injury, stroke, epilepsy or seizure disorders, multiple sclerosis, Parkinson disease, psychiatric disorders (post-traumatic stress disorder, schizophrenia, bipolar disorder), illicit drug abuse within the past six months, Alzheimer disease, and dementia.
Before initiation of study procedures, individuals were administered the Mini Mental Status Examination (MMSE), which was adapted to eliminate motor requirements; participants scoring ≤22 on MMSE were excluded. The data reported represent secondary analyses from a cross-sectional observational investigation conducted at the Kessler Foundation (KF) in West Orange, NJ, and supported by investigators at the James J. Peters Veterans Affair Medical Center (JJPVAMC) in the Bronx, NY. The experimental protocol was approved by the institutional review boards of the KF and JJPVAMC, is registered on clinical
Study procedures
Participants arrived at KF between 9 am and 2 pm, remained in the seated position for a period of quiet rest, for instrumentation, which included placement of three ECG electrodes and a finger and a brachial BP monitor. After instrumentation, simultaneous resting beat-to-beat HR and finger BP were recorded continuously for 5 min, and brachial BP was recorded at 1-min intervals in the supine position. Participants were then passively moved into the seated position for administration of a complete NP test battery, the results of which have been reported previously, 2,4 with simultaneous recording of beat-to-beat HR and BP.
For this report, we document test results from the Paced Auditory Serial Addition Test (PASAT), 39 which places demands on both processing speed and working memory, 40 because these deficits are often identified in studies of cognition after SCI. Four trials are presented aurally, each containing 50 digits (i.e., maximum total of 200 digits); the speed at which the digits are presented increases with each successive trial, and participants are asked to add an aurally presented digit to the one immediately preceding it. The PASAT has high internal consistency and spilt half reliability (r = 0.96) is sensitive to processing speed deficits 40 and neurocognitive syndromes including concussion and diffuse cerebral damage.
Hemodynamic monitoring
The ECG and finger BP signals were continuously monitored at rest and during the PASAT. The ECG recording was collected using a bioamplifier (Model RESP 1 with ECG: UFI, Morro Bay, CA), with electrodes placed at the right and left midaxillary lines in the fifth intercostal space and at the right anterior axillary line. Continuous beat-to-beat BP (mm Hg) was assessed at the finger using photoplethysmography (Finometer PRO, Finapres Medical Systems B.V., the Netherlands) and once every minute at the brachial artery with automated auscultation (Series Wall Mobile Sphygmomanometers, Trimline Medical Products, Raritan, NJ). The ECG and photoplethysmography BP signals were viewed, in real time, on a computer screen, and the digital signals were stored for subsequent analysis using customized programs written with LabView graphical software.
Psychological well-being surveys
The SCI Quality of Life (QoL) questionnaires (SCI-QoL) focus on 22 conceptual subdomains that were developed from qualitative data obtained in individuals with SCI. 41 In this report we focus on five subdomains from the SCI-QoL: depression, 42 anxiety, 43 fatigue, 44 resilience, 45 and positive affect. 46 These questionnaires were sent home with each participant to be completed in privacy and were sent back to the research staff when finished; only 94 of the 140 participants returned a complete survey. The QoL data were analyzed and are reported here as the raw scores.
Data processing for cardiovascular autonomic assessment
Oscillations in the interbeat-intervals of R-waves (RRI) and SBP peaks were acquired at a sampling rate of 500 Hz/channel with a 16-bit analog-to-digital converter (AD board model #USB-6221, National Instruments, Austin, TX, USA). RRI (msecs) and SBP peaks (mm Hg) were analyzed using a customized program created with LabVIEW graphical software for instrumentation (National Instruments, Austin, TX, USA). All digital signals were visually inspected for artifacts and anomalies, and peak detection was performed on the QRS complexes.
The RRI time series was interpolated and re-sampled at 10 Hz, channeled through a Hamming window function, and transformed into the power spectra using discrete Fourier transform algorithms. The power spectra were integrated, and the areas of interest quantified for HR and BP. The amplitude of the HF-HRV area (0.15-0.40 Hz) was integrated as an index of efferent vagal modulation of the SA-node, 47,48 and the Mayer wave frequency (LF: 0.07-0.10 Hz) of SBP variability was used as an index of sympathetic vasomotor tone. 37,38
Raw values were transformed using a natural log because of deviations from normality. The rate and depth of respiration was not controlled but was recorded to account for the influence of intrathoracic oscillations on the frequency spectra amplitudes.
Statistical analyses
Descriptive statistics were calculated from 94 participants who completed all testing. Baseline measures were compared with independent t tests and associated 95% CIs, and the condition (seated, PASAT) by group (SCI, UIC) analyses were performed with multi-level modeling. Overall, demographic and PASAT scores were reported as mean (M) ± and standard deviation (SD).
Questionnaire scores on the SCI-QoL and cognitive performance on the PASAT served as primary outcome measures, and multiple regression analysis was used to determine their relationships to the independent variables, which included age, sex, group (SCI, UIC), NLI (as an integer: C1 = 1, C2 = 2…), AIS (AIS A versus AIS B/C/D), HF-HRV, and LF-SBP.
Because many of the QoL variables exhibited floor and ceiling effects, group mean differences were assessed using 95% CI estimated with bootstrapping (10,000 resamples) procedures. In addition, Pearson correlations between measures of psychological well-being (depression, anxiety, fatigue, resilience, and positive affect), and ANS measures of HF-HRV and LF-SBP, were computed at rest and during the PASAT.
All statistical analyses were performed using R statistical software. Analyses of multi-level models was conducted using the lme4 package. Comparisons between regression models for superior model fit (e.g., main effects models vs. models including interactions) were conducted with the flexplot package, 49 from which Bayes factors were calculated.
Results
Cognitive function
As reported previously, the SCI group performed significantly more poorly on the PASAT then the UIC (105 ± 45 vs. 130 ± 37, respectively; 95% CI of the mean difference = -41.4 to -7.6) (Fig. 1). Bivariate regression analysis showed NLI, AIS, and DOI (years) were not significantly associated with PASAT scores in the SCI cohort (all p > 0.42).
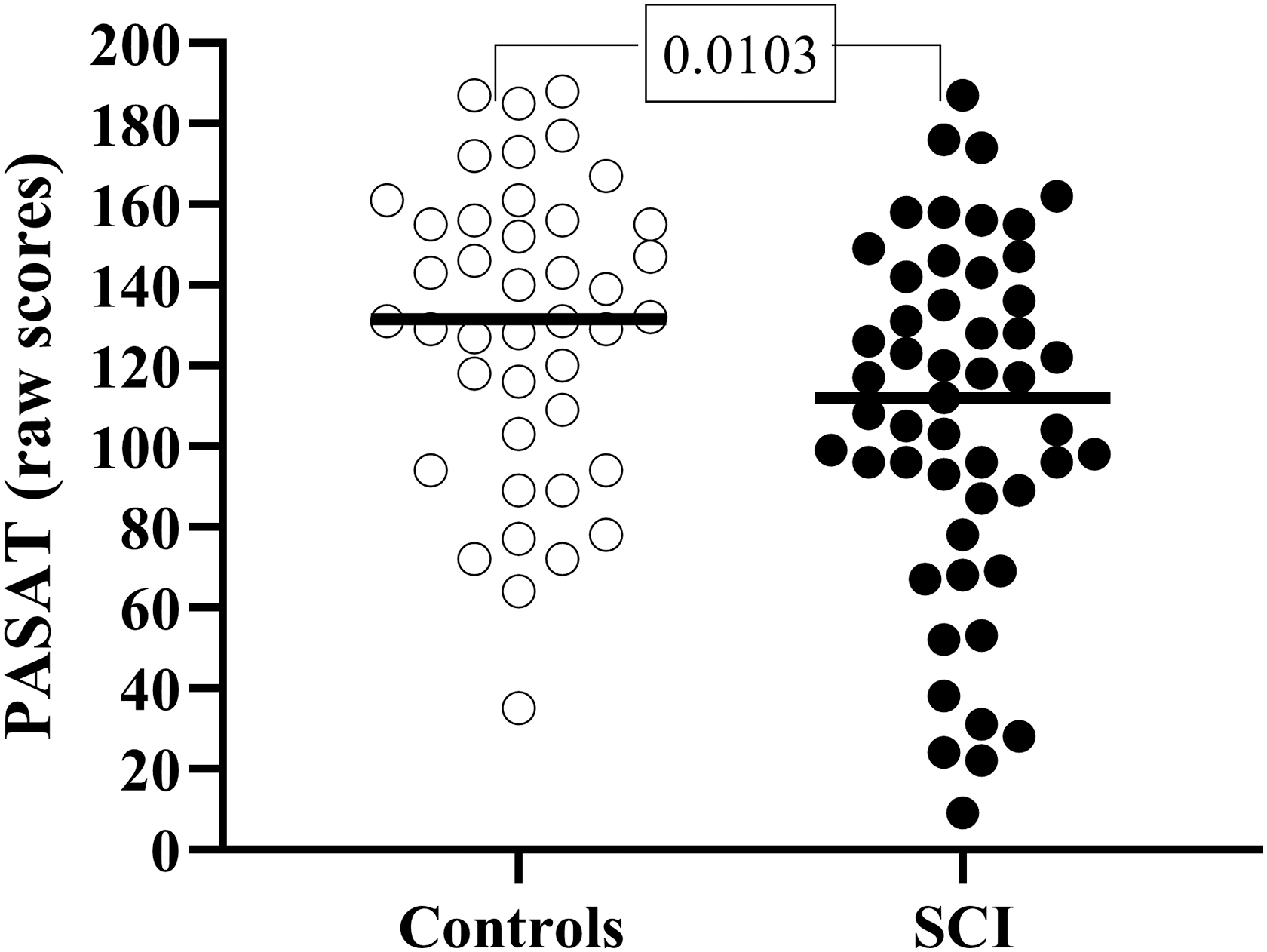
Paced Auditory Serial Addition Test (PASAT) scores in the uninjured controls (open circles) and participants with spinal cord injury (SCI) (closed circles).
Psychological well-being
Raw score results for subjective reporting of psychological well-being are shown for the SCI and UIC groups (Table 2). Although the SCI group tended to score more poorly than the UIC group on measures of psychological well-being, the group differences assessed using the bootstrap procedure were not significant for depression, anxiety, fatigue, resilience, or positive affect.
Psychological Well-Being: Raw Scores
Data are means ± standard deviation; 95% CI, 95 percent confidence interval of group differences; SCI, spinal cord injury.
Within the SCI group, bivariate regression analyses using NLI as an integer showed that higher cord lesions were associated with lower levels of resilience (slope (b) = -0.40, 95% CI = -0.7 to -0.1), and positive affect (b = -0.53, 95% CI = -0.99 to -0.09) and higher levels of fatigue (b = 0.18, 95% CI = 0.01 to 0.34). The effect of NLI on depression (b = -0.26, 95% CI = -0.59 to 0.06) and anxiety (b = -0.22, 95% CI = -0.07 to 0.52) were not significant.
Severity of injury, as indicated by AIS, was unrelated to the parameters of psychological well-being (all p > 0.39). Similarly, DOI (years) did not contribute significantly to depression (b = 0.12, CI = -0.05 to 0.29), anxiety (b = 0.04, CI = -0.12 to 0.20), fatigue (b = -0.01, CI = -0.10 to 0.08), resilience (b = -0.11, CI = -0.28 to 0.06), or positive affect (b = -0.06, CI = -0.28 to 0.16).
Autonomic cardiovascular control
Parameters of cardiovascular ANS function are presented in participants with SCI and UIC at rest, in the supine and seated positions, and during administration of the PASAT (Table 3). The change in the parameters of ANS cardiovascular function from seated rest to during administration of the PASAT is presented in Figure 2.
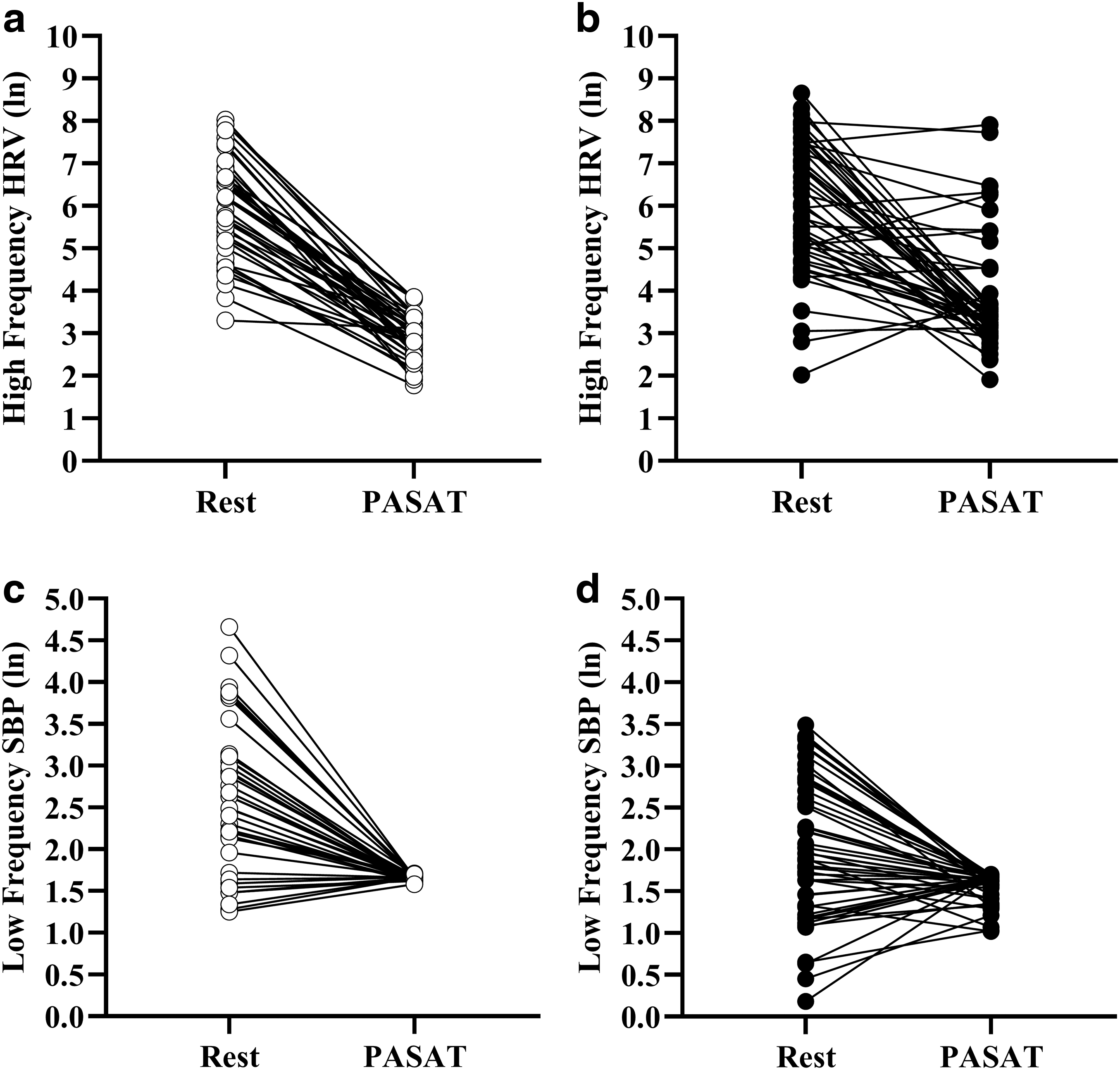
Change in cardiovagal tone (top: HF-HRV [high frequency component of heart rate variability]) and sympathetic vasomotor control (bottom: LF-SBP
Autonomic Cardiovascular Function
Data are means ± standard deviation; 95% CI, 95 percent confidence interval of group difference; SCI, spinal cord injury; HF-HRV, high frequency component of heart rate variability; LF = SBP, low frequency Mayer wave oscillations in systolic blood pressure; PASAT, Paced Auditory Serial Addition Test.
Although resting HF-HRV did not differ significantly between the groups, the test by group interaction effect was significant (F (1, 94) = 7.93, p = 0.006), indicating a more pronounced decrease in HF-HRV during the PASAT in the UIC compared with SCI. Seated LF-SBP was significantly increased in the UIC compared with participants with SCI (Cohen d = 0.56, 95% CI of the mean difference = 0.13 to 0.87 [ln mm Hg 2 /Hz]).
Further, the test by group interaction effect for LF-SBP was significant (F (1,88) = 4.2, p = 0.04), indicating a more uniform and pronounced decrease in LF-SBP during the PASAT in the UIC compared with SCI. Closer examination of Figure 2 suggests that the SCI group exhibited more variable ANS responses to cognitive testing than the UIC.
We further examined the influence of injury characteristics on the ANS responses to cognitive testing in the SCI group. Neither NLI nor AIS contributed to the changes in parameters of ANS cardiovascular function from seated rest to during administration of the PASAT in the SCI group. While there was no influence of DOI on the change in LF-SBP from rest to test, the interaction effect for change in HF-HRV (seated, PASAT) by DOI was significant (F [1,52] = 11.4, p = 0.001), suggesting that the longer a person was injured the less pronounced the fall in HF-HRV from rest to test.
The relationship between DOI and HF-HRV appears to be driven largely by age, as the model fit for the interaction with age (F [1,52] = 41.4, p < 0.001) showed a markedly better fit than the interaction with DOI (Bayes Factor = 152126.7). This interaction effect indicates that in those with SCI, the relationship between age and HF-HRV differs when seated vs. when performing the PASAT. To further examine the interaction effect between age, HF-HRV, and condition (seated, PASAT) we expanded our analysis to include the UIC participants and the three-way (age, group, condition) interaction effect was significant (F [1,94] = 9.1, p = 0.003).
We then performed separate analyses by condition (seated, PASAT) to compare the relationship between age and HF-HRV by group. In the seated condition, the group effect was not significant (Fig. 3a); however, during the PASAT, there was a significant group by age interaction effect (F [1,89] = 30.7, p < 0.0001) indicating an increased HF-HRV during the PASAT with increasing age in SCI, which was not evident in the UIC (Fig. 3b).
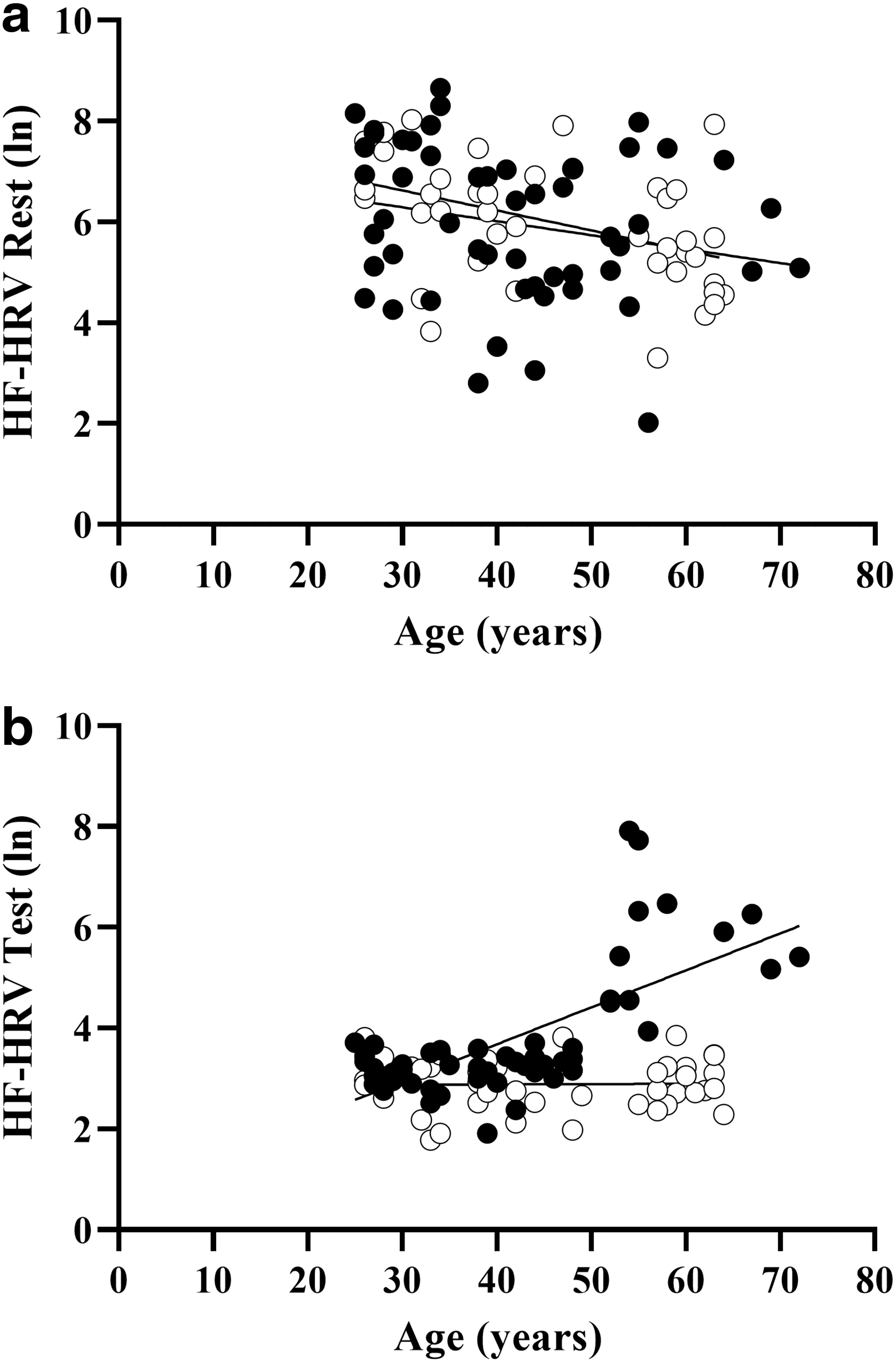
Relationship between the age (years) and cardio-vagal tone (HF-HRV) at rest
Correlative associations
In the participants with SCI alone (n = 52), we constructed a bivariate correlation matrix to determine significant correlates of PASAT scores. Factors included in these analyses were age, sex, injury characteristics (NLI, AIS, DOI), scores on the measures of psychological well-being (depression, anxiety, fatigue, resilience, and positive affect.), and the change in HF-HRV and LF-SBP from rest to test.
The only significant correlate of performance on the PASAT was anxiety (r = -0.32, 95% CI = -0.55 to -0.05), which was inversely associated with PASAT raw score (Fig. 4). As expected, all parameters of psychological well-being were significantly correlated with one another, but the two estimates of ANS cardiovascular function were unrelated to the parameters of well-being or PASAT performance.
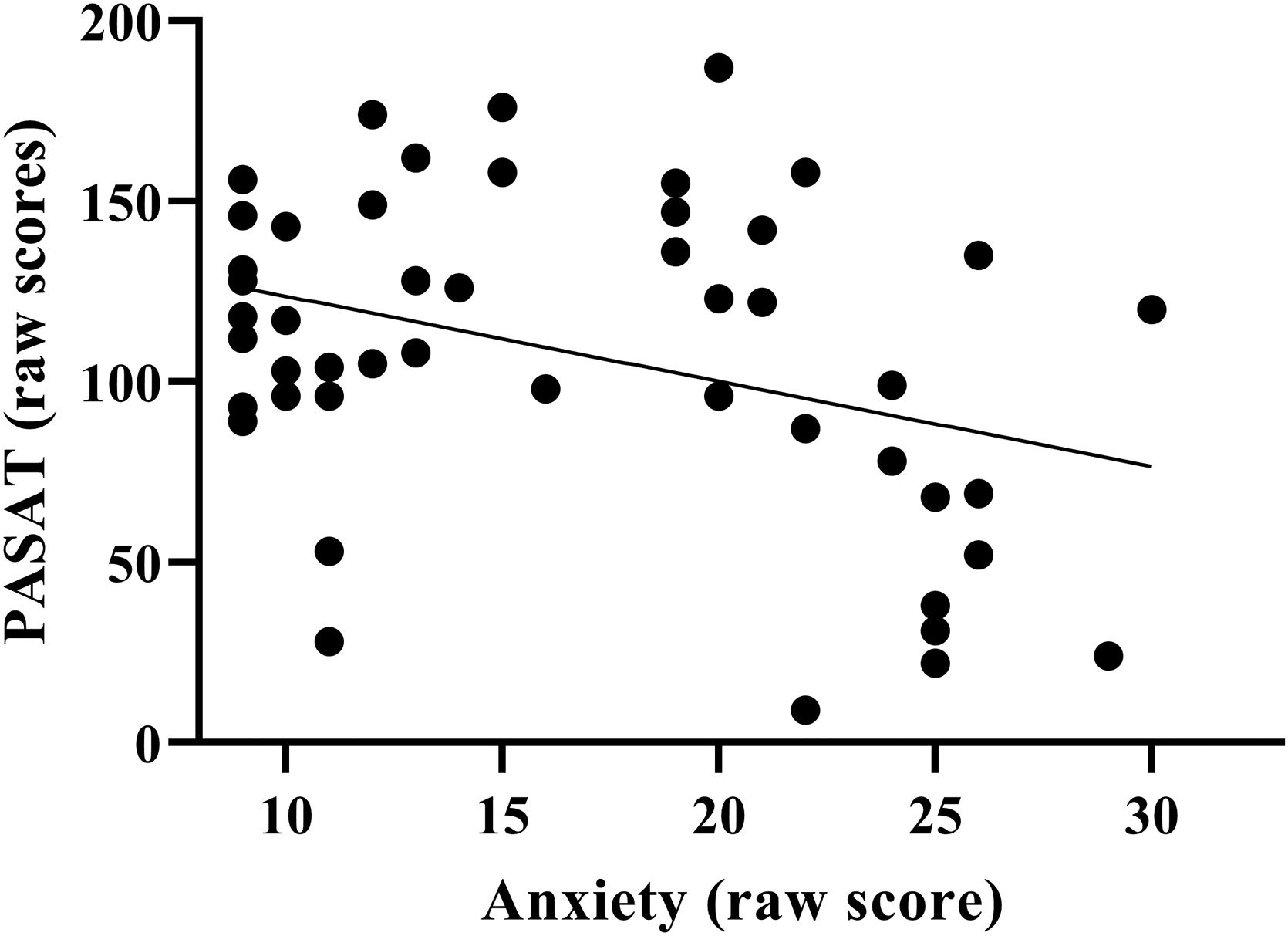
There was a significant inverse relationship between anxiety and PASAT score in participants with SCI (Pearson's correlation; r = −0.32, 95% CI = −0.55 to −0.05), such that individuals with higher self-reported levels of anxiety scored more poorly on the PASAT.
Discussion
Individuals with SCI performed significantly more poorly on the PASAT compared with UIC, by approximately one-half SD, and although ANS mediated changes in cardiovascular function during testing differed between the groups, this difference did not account for poor test performance in the SCI group. While the group differences in mood disorders between UIC and SCI participants did not reach significance, within the SCI group higher cord lesions were associated with poorer resilience and positive affect and higher levels of fatigue.
Although these results have been reported previously independent of one another in the SCI population, the interrelationships between mood, ANS cardiovascular control, and cognitive function have not been reported as potentially interrelated in a large cohort of healthy participants. As such, these data provide novel evidence of the potential connection between mood disorders, ANS dysfunction, and cognitive impairment, which will help guide development of effective treatment strategies for the diverse cognitive deficits and high levels of depression and anxiety that are reported in the SCI population. 2 –4
As reported previously, individuals with SCI performed more poorly on the PASAT compared with matched UIC. 2,4 During the PASAT, uniform changes in cardiovagal tone, as estimated by the HF-HRV, and in peripheral sympathetic vasomotor tone, as estimated by the LF-SBP, were evident in the UIC, whereas these ANS cardiovascular responses were much more variable in the participants with SCI.
Although we did not find that alterations in cardiovascular ANS response to testing accounted for a significant amount of variance in PASAT performance, previous reports indicate associations between cognitive dysfunction in the SCI population with ANS cardiovascular and cerebrovascular dysfunction. 20,21 Further, the impact of DOI on these ANS cardiovascular responses to testing was significant for HF-HRV, indicating that the longer an individual was injured, the more likely was an inappropriate cardiovagal response to testing.
The relationship between DOI and HF-HRV responses to cognitive testing is explained in large part by age, and of interest is that during the PASAT, the interaction between age and HF-HRV differs significantly in the SCI compared with the UIC group. As evident in Figure 3b, older individuals with SCI (50+ years) appear to have higher cardiovagal tone during testing compared with older UIC participants.
Several reports have documented significant associations between age, resting HRV, and cognitive performance, which suggest that lower levels of resting HRV are associated with poorer cognitive performance. 50 –54 These cross-sectional studies have been conducted in hundreds or thousands of older (60+) participants and have noted deficits in executive function, 52 memory and language, 50 matrix reasoning, 51 and processing speed 54 in association with various parameters of HRV. To our knowledge, this is the first report to document significantly aberrant HRV responses to cognitive testing in older participants with SCI compared with age-matched UIC, which should be explored in greater detail.
The SCI leads to lifelong ANS dysfunction with multiple serious consequences for which there is no adequate treatment. 55 –58 The SCI, especially at or above the T6 level, disrupts the dynamic balance between the sympathetic and parasympathetic branches of the ANS that normally maintain internal homeostasis. 58 For the estimated millions of people living with SCI globally, 59 impaired ANS regulation results in cardiovascular dysfunction, adverse changes in bowel 60 and bladder 61 control, abnormal sudomotor, 62 and temperature regulation, 63 disrupted immune function, 64 and may contribute to the increased prevalence of cardiometabolic syndromes. 65 –67
Additional evidence in the SCI population suggests that, regardless of the NLI, 68 ANS deficits profoundly impact the ability to sit upright for prolonged periods, which diminishes independence, self-care, cognition, and QOL. 69 –71 Cardiovascular deficits that result from ANS impairment in individuals with SCI lead to BP instability, increasing daytime sleepiness, which detracts from participation in daily activities, health, and well-being. 72
Further, in the uninjured population, ANS disorders of chronic hypotension and orthostatic hypotension are associated with an overall sense of hopelessness, 73 increased reporting of depressive symptoms, 74 and a poor self-reported sense of well-being. 75 Importantly, persons with SCI prioritize restoration of ANS functions (i.e., restoring bowel, bladder, and sexual function) higher than regaining the ability to walk. 76
Although the current findings do not indicate a significant association between cardiovascular ANS dysfunction and cognitive performance, there were marked aberrations in the HRV and BPV responses to testing in our participants with SCI that should be examined more thoroughly.
While higher self-reported levels of depression were associated with poorer performance on the PASAT in the entire study cohort (n = 94: data not shown), this does not indicate a causal relationship, and the small amount of explained variance (i.e., 6.6%) should be interpreted with caution. A previous report in newly injured patients with SCI suggests a weak association between depressive symptoms and cognitive performance, 77 and a more recent report found that cognitive dysfunction, assessed at admission and discharge from inpatient rehabilitation after injury, was predictive of increased anxiety and depression at a six-month follow-up. 78
We reported increased levels of depression in a group of hypotensive individuals with chronic SCI with memory deficits, 18 but a lack of a relationship between depression and cognitive performance was recently published in community dwelling adults with SCI. 79 Given the increased prevalence of depression reported in the SCI population, 77,80 identifying the impact of mood disorders on neuropsychological function should be a high priority.
Although the relationship between depression and PASAT score was not significant within the SCI group alone, higher levels of anxiety were significantly associated with poorer test performance. Possible associations between negative mood and cognitive performance should be more extensively studied in a group of individuals with SCI who received a diagnosis and treatment for depression and anxiety.
Although not significant, the SCI group tended to score more poorly on measures of psychological well-being than the UIC group, as reported previousy. 81 This finding is troublesome and worthy of further longitudinal investigation. An argument can be made that damage to the spinal cord impairs afferent transmission of somatic markers to the brain, thereby blunting subjective emotional experiences over time, and there is speculation that individuals with SCI experience a blunting of positive affect, due, in part, to attenuated ANS afferent feedback. 81 Future studies should examine, in more detail, the possible association between the underlying ANS mechanisms of inhibitory control with psychological well-being and neuropsychological function in the SCI population.
We excluded individuals with a documented history of traumatic brain injury; however, many individuals, if not most, who break their spine probably hit their head during the traumatic event. While we cannot distinguish those with and without lasting cerebral damage, we believe that this damage may be at the nexus of the cognitive, mood, and ANS impairments noted within these results and in the literature.
Limitation
This report represents subanalyses within two larger clinical trials aimed at determining the effects of aging and loss of cardiovascular and cerebrovascular ANS control on cognitive performance in people with chronic SCI. As such, these findings should be interpreted cautiously, and follow-up studies, aimed at the a-priori determination of the contribution of mood and ANS responses during testing to cognitive performance in the SCI population should be considered. Moreover, capturing 24-h HRV data would be more reflective of cardiovagal tone during routine activities of daily living, which may have illuminated the relationship between ANS impairment, mood, and cognitive function in the SCI group and should be considered in a future investigation.
Heterogeneity in injury characteristics among participants with SCI may have influenced the cardiovascular ANS impairments, and the relatively small sample size in the SCI group, particularly those with high thoracic lesions (T1–T5, n = 4) did not allow for adequate power to detect this influence. Although age did not contribute significantly to performance on the PASAT, there was wide variability in age (range 26–72 years), which may have affected cardiovascular ANS function and cognitive performance independently.
The psychological surveys were self-reported by participants in the home environment and therefore do not accurately represent clinical symptomology or diagnoses. There were more males than females in both the SCI and UIC groups, and although sex did not contribute significantly to the associations reported herein, sex differences cannot be ruled out and should be examined in larger groups of females with and without SCI.
Future studies should examine the influence of mood disorders on cognitive performance in people with SCI who have received a diagnosis of depression or anxiety compared with those with SCI not with a diagnosis of these conditions. Finally, these associations should be examined in individuals with SCI using brain imaging tools such as fMRI or encephalography, because there may be structural damage to regions of interest that control mood, cognition, and ANS cardiovascular control.
Conclusion
This is the first investigation to examine the potential interrelationships among highly prevalent conditions of psychological distress, autonomic cardiovascular impairment, and cognitive dysfunction in people with SCI. The results suggest that compared with UIC, participants with SCI performed more poorly on the PASAT, tended to report lower psychological well-being, and demonstrated significantly altered cardiovascular ANS responses to testing. While altered cardiovascular ANS responses to testing did not relate to test performance, higher levels of anxiety were associated with poorer test performance in the SCI group.
Future investigations should more closely examine the relation among cardiovascular ANS impairments, psychological disorders, and cognitive dysfunction after SCI to better elucidate the underpinnings of these mutual deficits and to guide interventions aimed at improving functional, psychological, and cognitive health after SCI.
Footnotes
Authors' Contributions
J.M.W. conceptualization (lead); writing – original draft (lead); review and editing (equal), prepared figures and tables (lead). J.P.W. formal analysis (lead); review and editing (equal). C.G.P. drafted manuscript (equal); review and editing (equal). E.W. analysis (equal); review and editing (equal). G.R.W. review and editing (equal). N.C.C. conceptualization (equal); analysis (equal); review and editing (equal).
Funding Information
This project was funded by the New Jersey Commission for Spinal Cord Injury Research (Grant #CSCR13IRG018 & #CSCR16IRG010) and supported by the Department of Veterans Affairs, Veterans Health Administration, Rehabilitation Research & Development Service Center for the Medical Consequences of Spinal Cord Injury (Grant #B9212-C, #B2020-C).
Author Disclosure Statement
No competing financial interests exist.