
Abstract
Our previous studies on the treatment of spinal cord injuries with Mechanical Tissue Resuscitation (MTR) in rats have demonstrated that it can significantly improve the locomotor recovery and Basso Beattie Bresnahan scores. MTR treatment also reduced fluid accumulations by T2-imaging and improved the mean neural fiber number and fiber length in injured sites by fiber tractography. Myelin volume was also significantly preserved by MTR treatment. For further clinical application, a large animal model is necessary to assess this treatment. This study examined the effects of application of MTR on traumatic spinal cord injury in a swine model. Traumatic spinal cord contusion injuries in swine were created by controlled pneumatic impact device. Negative pressure at -75 mm Hg was continuously applied to the injured site through open cell silicone manifold for 7 days. In vivo magnetic resonance imaging for T2 and gradient echo (GRE) analysis employed a 3T machine, while a 7T machine was employed for diffusion tensor imaging (DTI) and fiber tractography. Histological hematoxylin and eosin (H&E) and Luxol fast blue staining were examined. MTR significantly reduced the mean injured volumes over 46% by T2-imaging in the injured sites from 477.34 ± 146.31 mm3 in non-treated group to 255.99 ± 70.28 mm3 in MTR treated group (p < 0.01). It also reduced fluid accumulations by relative T2 signal density in the epicenter of the spinal cord injury from 1.62 ± 0.27 in non-treated group to 1.22 ± 0.10 in the MTR treated group (p < 0.05). The mean injured tissue volume measured by H&E staining was 303.71 ± 78.21 mm3 in the non-treated group and decreased significantly to 162.16 ± 33.0 mm3 in the MTR treated group (p < 0.01). The myelin fiber bundles stained by Luxol blue were preserved much more in the MTR treated group (90 ± 29.71 mm3) than in the non-treated group (33.68 ± 24.99 mm3, p < 0.01). The fractional anisotropy (FA) values processed by DTI analysis are increased from 0.203 ± 0.027 in the untreated group to 0.238 ± 0.029 in MTR treatment group (p < 0.05). Fiber tractography showings the mean fiber numbers across the impacted area were increased over 112% from 327.0 ± 99.74 in the non-treated group to 694.83 ± 297.86 in the MTR treated group (p < 0.05). These results indicate local application of MTR for 7 days to spinal cord injury in a swine model decreased tissue injury, reduced tissue edema, and preserved more myelin fibers as well as nerve fibers in the injured spinal cord.
Introduction
Spinal cord injury (SCI) is a major cause of lifelong disability creating devastating personal, family, and societal consequences. Trauma remains the leading cause for 70% of SCI cases, with recent studies showing over 80% of the injuries could be attributed to motor vehicle accidents (41%) and falls 45%) with initial mortality rates between 5 and 20%. Patients over 70 have a greater in-hospital mortality of 27.7% versus 3.2% for younger patients. Lifelong potential complications for those that survive the initial injury include chronic pain, bladder and bowel dysfunction, susceptibility to major cardiac and respiratory pathologies, skin breakdown and repeated infections. The ability of these patients to return to preinjury occupation and earning capacity are extremely rare. There is still no effective treatment that leads to significant functional recovery of these patients. 1 -3 Thus, new and effective treatment modalities are desperately needed. 4,5
Mechanical Tissue Resuscitation (MTR) is a derivation of mechanobiology, the science of using mechanical forces to induce biological changes in living tissue. Our previous very extensive laboratory and clinical studies in a wide variety of tissues have repeatedly demonstrated that the application of a controlled sub-atmospheric pressure to compromised tissue facilitates a physiological environment that is more compatible with the survival of this tissue. 6,7 Cell survival is critical in compromised tertiary differentiated tissues such as neural and cardiac, where regrowth of functional tissue is minimal.
Our previous studies on the treatment of brain injuries in rats and swine have demonstrated that MTR can reduce edema, increase functional blood flow, remove deleterious debris, produce a normalization of metabolites, and decrease the ultimate size of tissue loss. 8,9 Likewise, our publication of MTR treatment of spinal cord injuries in rats has demonstrated that edema around the injury can be reduced, neural fiber number and length across the injury can be preserved, and survival of myelin volume at the injury can be increased. Most importantly, MTR treatment significantly increased locomotor recovery in these studies. 10
This study was performed to confirm our previous studies showing the efficacy of MTR for injury to the spinal cord in rat using a swine model. Swine models of SCI provide more translatable data because of the similarities of the swine spinal cord to humans in respect to osseous spine and spinal cord anatomy, vasculature, immune and inflammatory responses, and higher neural function. It is also similar in elastic properties with nearly identical myelin levels and water ratios as the human spinal cord, which is desirable to reproduce the effects of acute SCI. 11,12
Methods
Animals
All surgical procedures and animal care issues for this study were approved by the Institutional Animal Care and Use Committee of Wake Forest University Health Science and followed DHSS Guidelines. A total of 20 female domestic pigs weighing 16-25 kg were randomly assigned to either treated or non-treated groups after injuries were induced by an experienced group independent of the surgical treatment team. To minimize variables, all surgeries were performed by the same neurosurgeon in a specialized animal surgery room and cared for by the same team. All animals were trained to use a hind leg mobility cart prior to surgery to facilitate movement and improve quality of life after the cord injury. The animals were sedated with a combination of ketamine: acepromazine: xylazine (20:1:1 mg/kg) and radiographs with skin markers were taken to localize the impaction site between T10 and T13. Intubated animals were maintained with 1.5-2.0 % isoflurane (Drager North American AV, Telford, PA) during the preparation and impaction. Standard monitoring of heart rate, respiratory rate, end tidal carbon dioxide, and oxygen saturation were performed (SurgiVet, Dublin, OH). Urethral catheterization was performed on each animal and maintained for the entire treatment of 7 days. A 6-8 cm dorsal midline incision was made and the spinous processes and laminae of T10–T11 were exposed. A laminectomy was performed and a window over 1.0 cm wide was created to expose the dura of spinal cord adequately.
The traumatic spinal cord injury was induced in all animals with a modified pneumatic impact device (Model AMS 201, AmScien Instruments, Richmond, VA) shown in Figure 1. The chest of animal was fixated by a foam padded metal restraint which was then secured to the surgical table. The 8.5 mm diameter beveled impactor tip was centered over the exposed dura surface. An impact velocity of 2.8 m/sec and duration of 250 msec was employed to produce a spinal cord deformation of 7 mm during the impact. The impaction data from each animal was acquired using pneumatic impact device AMS 201 VI software. The impact resulted in a controlled contusion injury with minor lacerations of the dura usually at the margins of the impaction. None were deemed of sufficient size or severity to require closure. The bleeding at the lacerations ceased spontaneously without intervention.
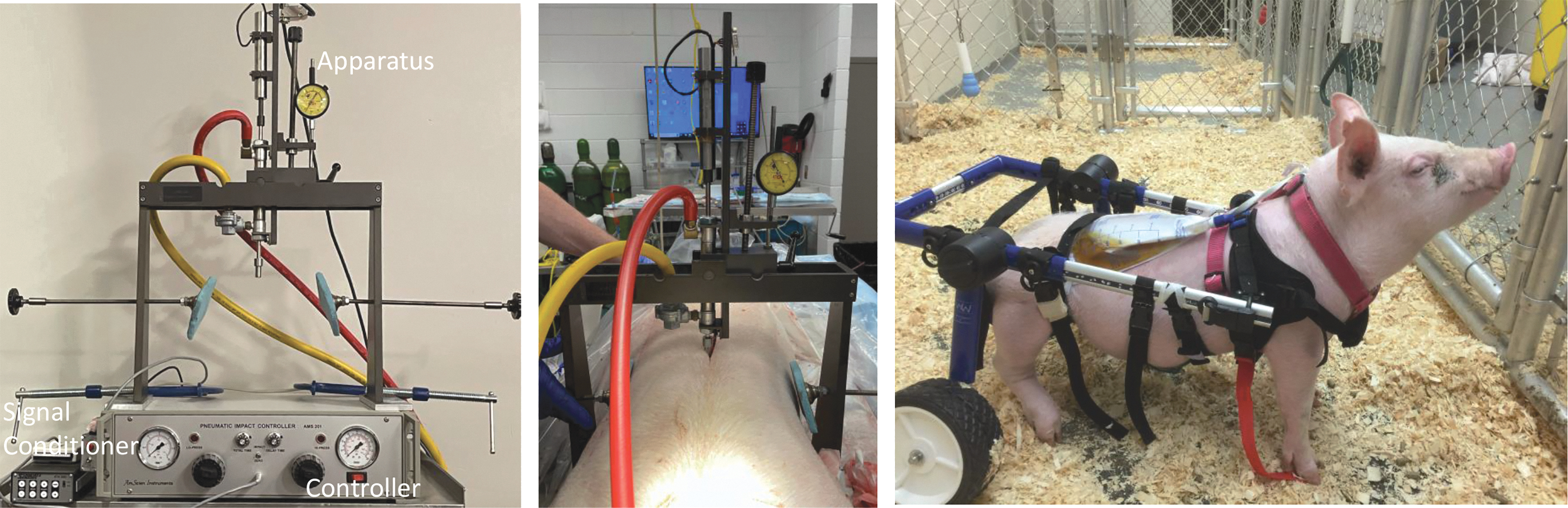
Modified pneumatic impact device used for creating pig traumatic spinal cord injury (SCI) model in left and middle of figures; The 8.5 mm diameter impactor tip is used in the pneumatic impact device. Also, the spinal cord injured swine in post care cart showed in the right figure. After urethral catheterization urine was collected as shown in the right figure.
A fenestrated poly L-lactic acid/polyglycolic acid sheet was bridged over the impacted cord and abutted on the surrounding bony lamina to prevent retraction or downward pressure on the cord during treatment. An MTR open cell silicone manifold was placed directly over the shell immediately above but not in direct contact with the injured spinal cord. The manifold is a custom fabricated open cell silicone matrix with a pore size that allows movement of fluids but is fine enough to prevent formation of granulation tissue. The manifold weight is approximately 0.5 grams. The manifold was connected by a flexible silicone tube to a custom fabricated computerized vacuum pump. Computer feedback mechanisms in the device measure the level of negative pressure at the treatment site and maintain that level continuously. The laminectomy site was left open, the skin was sutured close and an occlusive dressing placed. A sub-atmospheric pressure (75 mm Hg below ambient) was continuously applied for 7 days immediately after dressing placement. Similarly, the untreated animals had the skin closed but no device was placed. Our previous studies with negative pressure wound therapy (NPWT) devices have revealed that undrained matrices sequester blood and debris and become a nidus of infection that would produce spurious results. Based on this experience, it was elected not to place an undrained matrix in controls. No dressing changes were performed during the experiment. Animals could move freely with the mobility cart in the pen during treatment. (Fig 1).
Magnetic resonance imaging
The first magnetic resonance imaging (MRI) was performed immediately post-impaction to quantitate the injury using a 3-Tesla (3T) Siemens Skyra magnetic resonance imaging system. The second MRI was performed 7 days post-injury. Several MRI sequences, such as T1 transverse turbo spin-echo (TSE) acquisition (repetition time [TR] 2400 msec, echo time [TE] 9.90 msec, thickness 2 mm, field of view [FOV] 200), T2 TSE transverse acquisition (TR 9830 msec, TE 114 msec, thickness 2 mm, FOV 200), T1 TSE sagittal imaging (TR 2310 msec, TE 10 msec, thickness 2 mm, FOV 280), T2 TSE sagittal sequence (TR 9010 msec, TE 104 msec, thickness 2 mm, FOV 280), T2 fl2d GRE transverse imaging (TR 1020 msec, TE 19.90 msec, thickness 2 mm, FOV 200), and T2 fl2d GRE sagittal imaging (TR 754 msec, TE 19.90 msec, thickness 2 mm, FOV 280) were performed for detecting injury, edema, hemorrhage and blood degraded products. MRI measurements were performed on a TeraRecon workstation (version 4.4.13.P3).
Diffusion tensor imaging and quantitative fiber tractography
After the second 3T-MRI scan, animals were deeply anesthetized, the chest opened, and transcardially perfused with phosphate-buffered saline and 4% paraformaldehyde. The vertebral column was excised and post-fixed in 4% paraformaldehyde for 48 h at 4°C.
Ex vivo MRI scans were then performed on a 7T MR scanner system (Bruker BioSpin) with the following diffusion tensor imaging (DTI) parameters: TR = 5000 msec, TE = 18.65 msec, thickness 1.0 mm, FOV 40, matrix size = 96 × 60. T2 TurboRARE sequence were also performed as following parameters: TR = 4500 msec, TE = 30.0 msec, thickness 0.60 mm, FOV 40, matrix size = 256 × 256. MediNRIA software (version 1.9.4) was used for diffusion tensor imaging and the fiber tractography process was the same in as our previous rodent study. 10,13 One axial screen in the most damaged epicenter was selected to delineate regions of interest (ROIs). All values, including fractional anisotropy (FA), apparent diffusion coefficient (ADC), three eigenvalues λ1 λ2 λ3, relative anisotropy (RA), volume ratio (VR), linear tensor index (Cl), planar tensor index (Cp), and spherical tensor index (Cs) are presented in Table 2. For fiber tractography, the axial full screen mode was used to outline a ROI on cross-sectional images collected every 1.25 mm. The total length was one vertebra body (average 22.5 mm) extending from injured center core to both cranial and caudal sides. Images were analyzed for tractography with a variety of parameters including number of fibers, volume of fibers and mean length of fibers. 10
Histologic analysis
The thoracic spinal cord centered on the lesion was harvested, post-fixed in 4% paraformaldehyde for 24 h at 4°C, and cryopreserved after 20% sucrose treatment; 20-μm thickness sections were serially cut every 1 mm for an overall total cord length of 30 mm. Sections were stained with hematoxylin/eosin to determine the total volume of neuronal tissue damage, cavity formation, local reactions of microglia and macrophages, and infiltration of neutrophils and leukocytes. Additional sections were stained with a Luxol fast blue-cresylecht violet stain kit (American MasterTech, Lodi, CA) to stain for myelin and Nissl substances in neurons.
For quantitative analysis of tissue damage, all cross H&E sections were scanned by Keyence BZ-X810 microscope and the injured tissue areas in each spinal cord were measured by Keyence software. For evaluation of spared neuronal fibers, cross-sectional fast blue staining images were photographed with an internal ruler and processed with ImageJ software (National Institutes of Health, MD). The preserved myelin fiber area was delineated for blue staining in each section. The total spared (living) volume in the 10 mm long epicenter of the injured cord was calculated from continuous sections.
Statistical analysis
All data were acquired and analyzed blindly by investigators and statisticians and are shown as mean ± standard deviation. The Wilcoxon Rank Sum test was performed for small unpaired samples by SAS (version 9.4, Cary, NC, USA). A p value less than 0.05 (p < 0.05) was considered to be significant for all comparisons. (*p < 0.05, **p < 0.01 used in figures and table). There was no adjustment made for multiple tests; all tests were conducted at the same level of significance for consistency. 14
Results
Of the original 20 animals, seven in each group completed the study (total of 14). Two animals were euthanized during preparation before the impaction injury: one could not be successfully intubated and another could not be catheterized into bladder. Of the animals that received spinal cord injury, one animal died and one was euthanized prior to completion of the study due to serious complications related to maintaining urethral catheterization. One animal died from peritonitis secondary to pylorus ulceration of unknown cause. The sixth animal (non-treated group) was euthanized early post-injury due to uncontrollable agitation and pain.
No significant hind limb or tail movements were observed with the rump and knees on the ground following the impaction injury. The injury was classified as a “severe injury” according to the Porcine Thoracic Injury Behavioral Scale (PTIBS). 15 No obvious behavior changes were observed during the 7 days of treatment with MTR. The fluid drainage by MTR was 5-10 mL serosanguineous fluid initially and rapidly decreased and cleared after 1-2 days.
Transverse T2-weighted in vivo magnetic resonance images from 3T MRI were used to measure the severity of total injury including edema, deformation, hemorrhage, and cyst formation. (Fig. 2A, 2B). T2 injury volumes were determined at Day 0 immediately after the impaction and before any treatment. Average initial volume of injury in the non-treated group was 465.85 ± 92.21 mm3 (n = 7) and 478.35 ± 75.55 mm3 (n = 6) in the MTR treated group. There was one animal in the MTR treated group whose data was lost by technical scanner failure. There is no significant difference in the initial injury volume between the two groups at Day 0 (p = 0.797), indicating consistent injured volumes created by our impaction device in both groups. (Table 1)
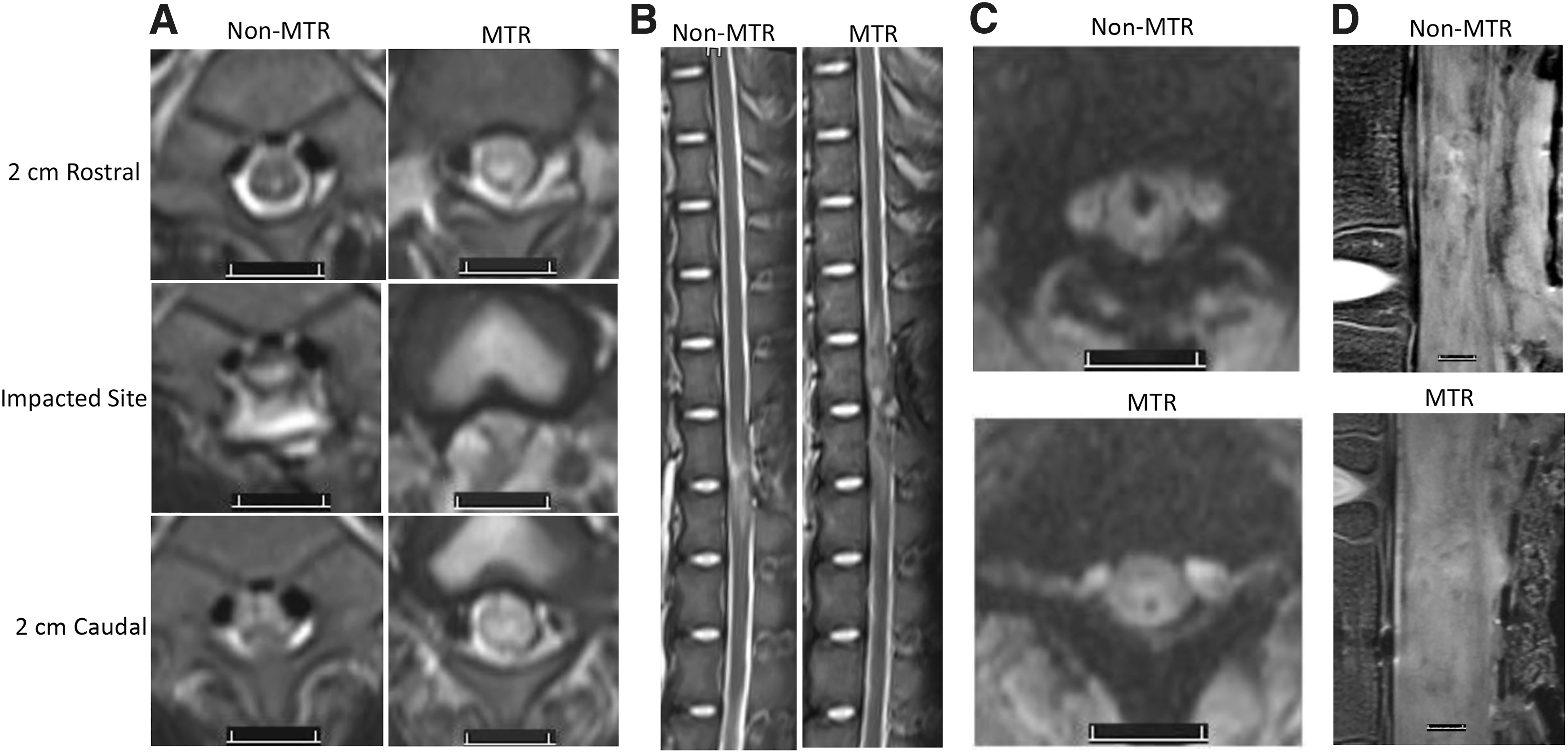
Representative magnetic resonance (MR) images of spinal cord injury (SCI) with Mechanical Tissue Resuscitation (MTR) application for 7 days.
Measurements of Tissue Injured Volume, Relative T2 Tissue Density, and Hemorrhage Volume in MR Images in Swine Spinal Cord Injury Model
MRI, magnetic resonance imaging; MTR, mechanical tissue resuscitation; SC, spinal cord; GRE, gradient echo.
After 7 days, the mean T2 injured volume was 477.34 ± 146.31 mm3 in non-treated group (n = 6). There was one animal in this group, whose 3T MRI data was lost by technical scanner failure. There were no significant statistical differences in injured volume between Day 0 and Day 7 in non-treated group. In the MTR treated group at Day 7 the mean T2 injured volume decreased to 255.99 ± 70.28 mm3 (n = 7) from 478.35 ± 75.55 mm3 (n = 6) at Day 0. There is a significant statistical difference (p < 0.01) between Day 0 and Day 7. There is a 46% reduction in injured tissue volume in the treated group compared with the non-treated group with a significant statistical difference (p < 0.01). When paired comparison was performed to compare injured volume at Day 7 versus Day 0 in same animal as (Day7-Day0)/Day0, their mean change percentage was 3.96% ± 28.3% in non-treated group and -49.8% ± 9.12% in MTR treated group, this reduction is statistically significant (p < 0.01; Table 1).
To evaluate edema level in the impacted area, T2 signal density in the epicenter of the SCI and the normal area at least two segments away from impacted site were measured in the same T2 sagittal image to avoid variation of signals between different scans. (Fig. 2B) The ratio of T2 density in the epicenter versus density in normal area distant to the injury 7 days after the injury was calculated. The mean ratio was 1.62 ± 0.27 in non-treated group (n = 6) and 1.22 ± 0.10 in the MTR treated group (n = 7). There is a significant statistical difference (p < 0.05) indicating less edema in the MTR treated animals.
Transverse in vivo T2 images clearly outlined cerebrospinal fluid (CSF) as a circular bright ring surrounding the spinal cord in uninjured animals. When the spinal cord was impacted, intact dura was damaged and differing amounts of CSF potentially could be lost or sequestered around the injured area. (Fig. 2A) Presence of CSF in scans rostral or caudal distal to the impaction epicenter in total 30 continuous scans (2-mm thickness) were quantitated in each animal. CSF existing on T2 transverse images as a bright ring surrounding over 50% of the cord were counted. An average of 21.67 ± 1.51 scans in the non-treated group and 21.86 ± 1.56 scans in the treated group revealed CSF at 7 days after injury. (Table 1) There is no statistical difference between two groups indicating that removal excessive or sequestration of CSF was not a confounding factor.
The excised vertebral column was used for ex vivo MRI scans on a 7T MR scanner and their T2 injury volumes were determined from T2 sagittal image (Table 1). The mean T2 injured volume was 523.80 ± 87.84 mm3 in non-treated group (n = 7), In the MTR treated group, their mean T2 injured volume decreased to 381.81 ± 110.09 mm3 (n = 7) with significant statistical difference (p < 0.05). Since these samples were kept 48 h at 4°C after fixative perfusion, their T2 injured volumes from ex vivo images are not comparable to the T2 injured volumes measured from in vivo T2 images by 3T MR scanner.
The hemorrhagic volume within spinal cord was measured in the GRE transverse imaging from in vivo 3T MRI. (Fig. 2C) The mean hemorrhage volumes at Day 0 were 30.57 ± 13.43 mm3 (n = 7) in non-treated group and 25.09 ± 13.83 mm3 (n = 6) in MTR treated group. There is no statistical difference between two groups (p = 0.49). At 7 days post-injury, the mean hemorrhage volumes were 39.65 ± 22.13 mm3 in the non-treated group (n = 6), and 11.68 ± 8.24 mm3 in the MTR treated group (n = 7). There is a statistical difference between these two groups (p < 0.05; Table 1) When comparing the hemorrhage volume from Day 7 to Day 0 in non-treated group, there was no significant statistical difference (p = 0.38). The decreased hemorrhage volume in MTR treated group at Day 7 compared with Day 0 nearly shows significant statistical difference (p = 0.053). When paired comparison was performed to compare hemorrhage volume at Day 7 versus Day 0 in same animal as (Day7-Day0)/Day0, their mean change percentage was 32.8% ± 73.7% (n = 6) in non-treated group and -45.5% ± 34.5% (n = 6) in MTR treated group, this reduction is statistically significant (p < 0.05; Table 1).
Results for the DTI analysis identified a significant difference in FA between the untreated group (FA 0.203 ± 0.027, n = 7) and the MTR treatment group (FA 0.238 ± 0.029, n = 7; p < 0.05), indicating less neuronal fiber damage in the treated group 7 days post-injury (Table 2).
Measurements From Diffusion Tensor Image (DTI) in Swine Spinal Cord Injury With or Without MTR Treatment
Measurements from diffusion tensor image (DTI) in the epicenter of the pig spinal cord injury from 7T magnetic resonance imaging without treatment (n = 7) and with MTR treatment (n = 7). Various parameters measured from the injured epicenter are fractional anisotropy (FA), relative anisotropy (RA), Lambda1 and 2 and 3, apparent diffusion coefficient (ADC), linear coefficient (Cl), planar coefficient (Cp), spherical coefficient (Cs) and volume ratio (VR). Values reported are mean ± standard deviation, with p values from their comparison. Significant differences in FA value indicating less tissue damage in MTR treated group (* p < 0.05).
MTR, mechanical tissue resuscitation.
A total of 12 of the 14 samples were able to fit in the fiber tractography modeling process, with one sample from each group unable to fit. 10 The mean fiber numbers across the impacted area were 327.0 ± 99.74 in the non-treated group (n = 6), and 694.83 ± 297.86 in the MTR treated group (n = 6). There is a statistically significant difference between the two groups (p < 0.05), with the non-treated group having only approximately 46% of the number of fibers seen in the MTR treated group. (Fig. 3)
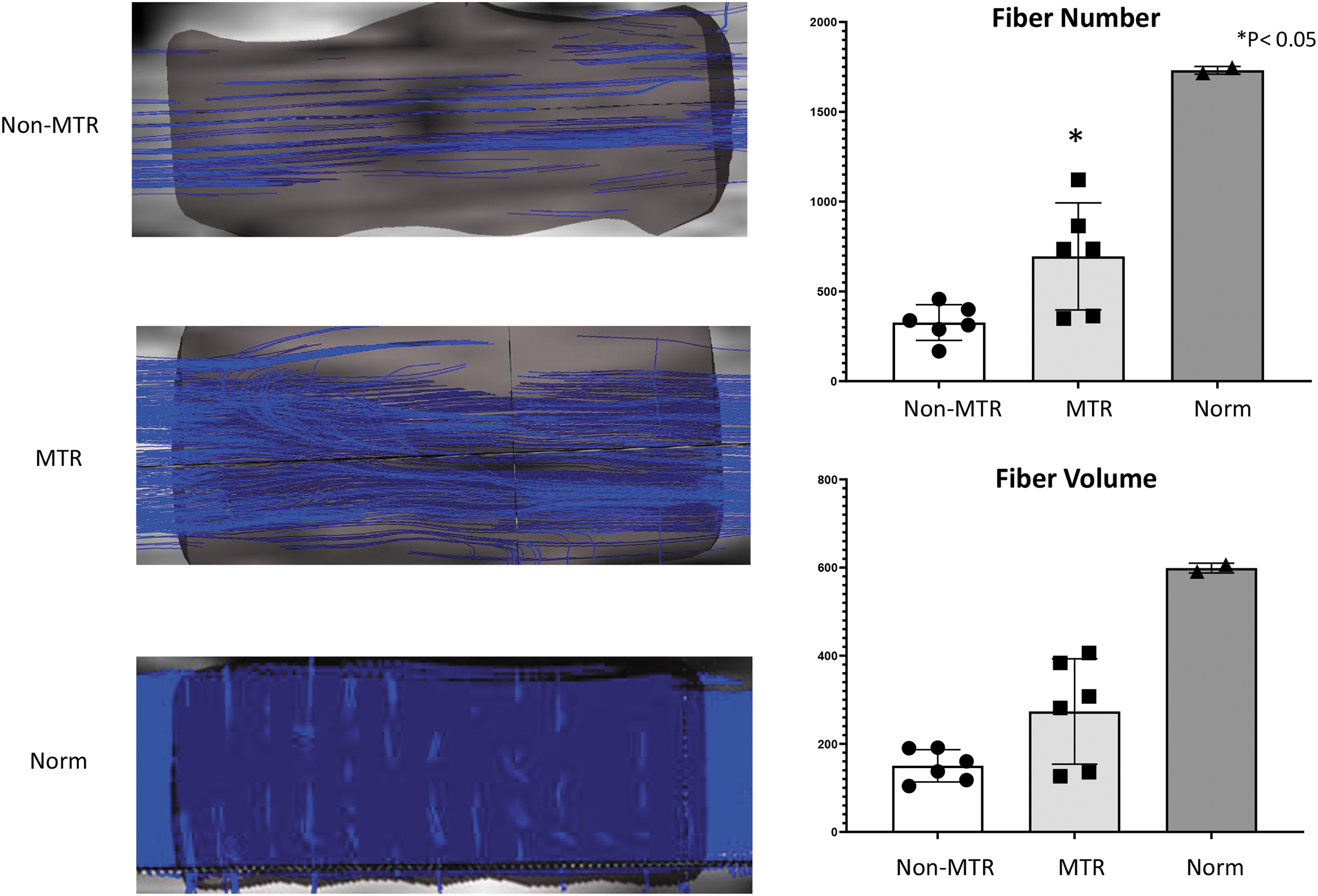
Sample images of fiber tractography from 7T magnetic resonance imaging in spinal cord injury model with Mechanical Tissue Resuscitation (MTR) application. Two normal spines were used as reference. Blue lines show extracted fibers from the spared white-matter tracts in injured spinal cords (left upper), injured with MTR treatment (left middle) and normal spinal cord (left bottom). The mean fiber count and fiber volume measured by fiber tractography as shown in bar graphs. MTR treatment (n = 6) significantly increases fiber numbers compared with Non-MTR (n = 6; *p < 0.05).
The mean fiber volumes were 150.15 ± 36.63 mm3 in the non-treated group (n = 6), and 273.47 ± 119.59 mm3 in the MTR treated group (n = 6). Although the mean fiber volume in the non-treated group is approximately 55% of the volume in the MTR treated group, there is no statistically significant difference between the two groups (p = 0.13). The median fiber lengths were 8.20 mm in the non-treated group (n = 6), and 5.71 mm in the MTR treated group (n = 6); there is also no statistical difference in these two groups (p = 0.13).
Histological H&E staining was used for assessing total injured area 7 days after the spinal cord injury. The mean injured volume measured under Keyence microscopy was 303.71 ± 78.21 mm3 in the non-treated group (n = 7) and 162.16 ± 33.0 mm3 in the MTR treated group (n = 7). There is a significant statistical difference (p < 0.01; Fig. 4). A column including bar graph beneath). Hematoma was found in 6 of 7 animals in non-treated group, and their hematoma volume ranged from 0.17 to 50 mm3, mean volume was 16.03 mm3. Hematoma was found in two of seven animals from MTR-treated group and their volumes were 0.31 and 1.21 mm3. Those numbers were smaller compared with the volumes measured from 3T MR GRE, which also detect surrounding degraded blood products.
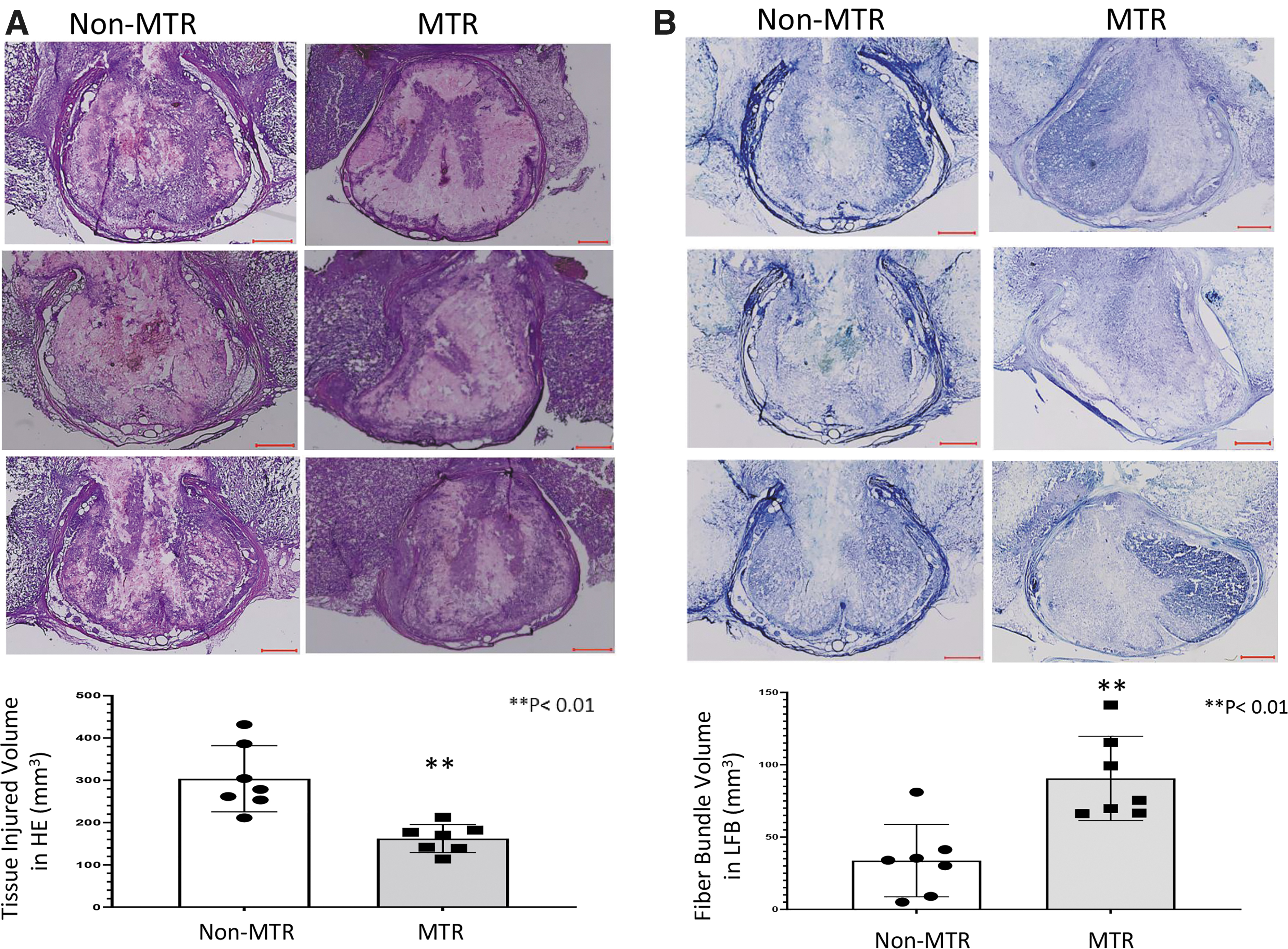
The representative histological images of hematoxylin and eosin (H&E) and Luxol fast blue staining of the injured spinal cord after Mechanical Tissue Resuscitation (MTR) application for 7 days.
The Luxol blue positive (surviving) myelin fiber area in each section was quantitatively determined by ImageJ, and the total volume in the 10 mm length of epicenter of the injury was calculated from continuous sections. The mean Fast Blue (FB) volume was 33.68 ± 24.99 mm3 for the non-treated group (Non-MTR, n = 7) and 90 ± 29.71 mm3 for the MTR treated group (n = 7). There is a statistically significant difference (p < 0.01), with the preserved myelin being approximately two times greater in the MTR treated group (Fig. 4 B column including bar graph).
Discussion
Our previous study indicated MTR to be an effective treatment for SCI in a rodent model. 10 Well known difficulties in translation of rodent studies to results in humans require studies in larger animals whose anatomy and response to injury are more similar to that of humans. 15 The average transverse diameter of our pig spinal cord at the impaction site is 5.3 mm (spinal canal width 9.5-10.6 mm), and 7.8 mm in depth if measured from the surface of dura to the back of spinal cord (including CSF) on MRI T1 imaging. When impacted to a depth of 7 mm, a reproducible contusion injury created a functional outcome that scored as 1-2 on the Porcine Thoracic Injury Behavioral Scale (PTIBS) at 1 week post-injury. These results were consistent with a similar model where a 50 g weight was dropped on the cord from a height of 40 cm to create a severe injury. 16,17
Extensive laboratory research, particularly in combination with MRI studies, have provided the clinician a better understanding of secondary phases of spinal cord injuries and revealed potential targets for treatment. 18 -20 Inhibition of progressive injury from cord ischemia, pooling of cellular debris, ion and cytokine imbalance, free radical production, disintegration of myelin fibers, and progressive osseous compression have become targets for potential therapies. Controlled negative pressure based research on a wide variety of soft tissue wounds has shown this application to the surface of the wound can remove soluble factors from the wound site, include those deleterious to healing. 7,21,22 Our previous publications on both traumatic brain and spinal cord injuries strongly suggest that MTR can directly mitigate many of these deleterious events in the central nervous system by the enhanced removal of edema and extravasated blood, improving local blood flow. 8 -10,23 In this study, T2 signal density results also demonstrated reduction of edema fluid accumulation in epicenter of SCI after MTR treatment.
Recent DTI-derived from MRI is particularly useful in characterizing tissues with parallel tracts such as white matter axons in spinal tissue. In spinal cord injuries, this measurement is an indicator of myelin and neural fiber integrity, both of which are critical to functional preservation and patient recovery. Fractional anisotropy (FA), a major parameter in DTI derived from MedINRIA process in Table 2, indicates changes in anisotropic diffusion of water. Values reflect disruption of the microstructure of white matter secondary to axonal degeneration, infarction or hemorrhage, edema, and demyelination. FA has been previously demonstrated to be significantly decreased in areas of spinal cord injury in animal and human studies. 24 -26 For this study, the values seen in non-MTR animals indicate that the epicenter of the injury lost most neural pathways and few white matter structures remained intact. MTR treated animals had a statistically significantly greater number of intact neural pathways and white matter structures compared with non-treated animals at 7 days post-injury. Fiber tractography derived from DTI values is a technique that uses mathematical algorithms to obtain three dimensional reconstructions of brain and cord white matter tracts. These studies allow semi-qualitative and semi-quantitative values of the fiber projections penetrating the ROI. Quantitatively, the mean fiber numbers across the area of impaction injury are doubled in the MTR treated group, which predicted a more favorable recovery.
We have previously shown MTR therapy is effective in improving motor function recovery in a rat model of SCI with Basso Beattie Bresnahan scores significantly improved both after 3 and 4 weeks of treatment. 10 Because of complicated issues related to bladder drainage with indwelling catheterization in swine, the Institutional Animal Care and Use Committee and the study team determined that studies beyond one week to assess changes in recovery of function were not humanely appropriate and therefore were not performed. Every indicator in this study, however, is compatible with values seen in our previous rodent study where significant improvements in function resulted.
Summary
Following the creation of a severe spinal cord injury in a large animal model, application of MTR continuously for 7 days significantly decreased the volume of injury and preserved more normal spinal cord anatomy than in non- treated animals. Importantly, no complications of this therapy were observed at any time.
MTR treatment is a purely mechanical technique and does not preclude the use of additional pharmacologic or surgical therapies in conjunction with MTR. Early surgical decompression has been demonstrated to improve results by the Canadian Cohort Study. 27 Similarly, the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS) trial documented that early surgical decompression leads to significant improvement in clinical results. 28 In this study, non-MTR treated animals received what could be termed a limited spinal decompression as the laminectomy to produce the injury was left open and compared with a group with an identical decompression and additional MTR. This study suggests that adding MTR to surgical decompressions, procedures now being routinely clinically practiced, may increase the potential for improved results.
Transparency, Rigor, and Reproducibility Summary
The study design and analytic plan were not pre-registered at the Center for Open Science (https://www.cos.io/initiatives/prereg), because this study was started before the center was activated.
Based upon previous studies of spinal cord injury, a sample size of eight animals was recommended to detect a difference in means 0.9 and Standard Deviation at 0.200 with p value of 0.05 by statistical analysis t-test. Also sample size was eight animals per group was recommended to detect a significant effect as p < 0.05 by analysis of variance statistical analysis with >80% power in multiple group comparison. Our biostatistician informed us that a statistically significant difference was observed after seven animals in each group. Following Federal Animal Welfare Act guidelines further studies were unnecessary and were not performed. The entire procedure was blinded as much as possible. The animals to be treated were randomly selected after the contusion was performed by a different team. All surgical procedures were performed by a senior neurosurgeon. Animals were cared for by certified veterinary teams.
Data analyzers were blinded to all samples that were labeled by numbers. The assessments of imaging and histology were performed using identical parameters and standards for all samples. The final data were analyzed by an independent blinded biostatistician from in a freestanding Statistical Department.
The study is limited because possible long-term recovery of function could not be determined in this large animal model. Institutional review committees determined that because of protracted compromised mobility of the animal, fecal incontinence, and the need for long term indwelling bladder catheterization that the study should be humanely terminated at 7 days. Since data from this experiment very closely parallels the data from our previous rodent study where functional recovery was improved, the authors feel significant meaningful comparable results were obtained.
Other factors that need further study include the optimal length of treatment and determination of the allowable time interval between injury and treatment.
Footnotes
Acknowledgments
We thank Greg Russell, a senior biostatistician in the Department Biostatistics and Data Science of Wake Forest University Health Science for assistance with data process and statistical analysis. We also thank senior faculties Dr. Youngkyoo Jung, Dr. Christopher T. Whitlow, and Dr. Don Gage in Department of Radiology of Wake Forest University Health Science for help in MRI planning, imaging acquisition and data interpretation.
Authors' Contributions
Z.Z.: methodology, validation, investigation, data curation, original draft preparation and visualization of writing; D. C.: methodology, validation, investigation, review and editing of writing; F.A.: investigation and resources; R.R.: investigation and resources; R M.: investigation and data curation; L.A.: conceptualization, review and editing of writing, supervision and funding acquisition; M.M: conceptualization, review and editing of writing, project administration, supervision and funding acquisition.
Funding Information
This study was supported by the research endowment of the Department of Plastic and Reconstructive Surgery, Wake Forest University Health Science.
Author Disclosure Statement
Louis Argenta, MD, and Michael Morykwas, PhD, are currently emeritus faculty at Wake Forest University Health Sciences (WFUHS). WFUHS owns the patent estate related to Mechanical Tissue Resuscitation (MTR) described in this article, in which Drs. Argenta and Morykwas are named inventors. While Drs. Argenta and Morykwas were active faculty at WFUHS, the MTR technology was licensed to Renovo Concepts, Inc. (San Antonio, TX), for which both are founders and officers.
Daniel Couture, MD, is a member of the Clinical Advisory Board for Renovo Concepts, Inc., but has not been compensated by Renovo Concepts, Inc.
For the other authors, no competing financial interests exist.