
Abstract
Neurovascular coupling (NVC) uniquely describes cerebrovascular response to neural activation and has demonstrated impairments following concussion in adult patients. It is currently unclear how adolescent patients experience impaired NVC acutely following concussion during this dynamic phase of physiological development. The purpose of this study was to investigate NVC in acutely concussed adolescent patients relative to controls. We recruited patients presenting to a sports medicine practice within 28 days of a concussion or a musculoskeletal injury (controls). Transcranial Doppler ultrasound was used to measure changes in patients' posterior cerebral artery (PCA) velocity in response to two progressively challenging visual tasks: (1) reading and (2) visual search. Each task was presented in five 1-min trials (20 sec eyes closed/40 sec eyes open). Resting PCA velocity data were derived by averaging PCA velocity across a 2-min baseline period that preceded the visual tasks. Filtered task data were converted to time-series curves representing 40 consecutive 1-sec averages for each trial. Curves were then averaged across the five trials and time-aligned to stimulus onset (eyes open) to generate a single ensemble-averaged 40-sec curve representing NVC response for each participant for each task. Independent t tests were used to assess group differences (concussion vs. control) in resting PCA velocity. Separate linear mixed-effects models were used to evaluate group differences (concussion vs. control) in NVC response profiles for both visual tasks and group-by-task interaction. Twenty-one concussion patients (female = 8 [38.1%]; age = 14.4 ± 1.9 years) and 20 controls (female = 7 [35.0%]; age = 14.4 ± 1.9 years) were included in our analysis. Average resting PCA velocity did not significantly differ between concussion patients (36.6 ± 8.0 cm/sec) and controls (39.3 ± 8.5 cm/sec) (t 39 = 1.06; p = 0.30). There were no significant group differences in relative NVC response curves during the reading task (F 1,1560 = 2.23; p = 0.14) or the visual search task (F 1,1521 = 2.04; p = 0.15). In contrast, the differential response to task (e.g., increase from reading task to visual search task) was significantly greater in concussion patients than in controls (p < 0.0001). The NVC response to the visual search task was 7.1% higher than the response to reading in concussion patients relative to being 5.5% higher in controls. Our data indicate that concussed patients present with a significantly greater response to more difficult tasks than do controls, suggesting that concussed adolescents require increased neural resource allocation as task difficulty increases. The study provides insight into the neurophysiological consequences of concussion in adolescent patients.
Introduction
Following concussion, physiological recovery has been shown to take longer than clinical recovery, 1 suggesting that there is a window of physiological vulnerability 2 to which standard clinical examinations may not be sensitive. Physiological recovery is particularly important in adolescent patients, as they are experiencing ongoing neural development, including cognitive, social, and emotional development, which may result in greater susceptibility to the effects of concussion 3 and longer recovery times (within 4 weeks) 4 –7 relative to adults (within 10 days). 8 To objectively measure physiological state after concussion, recent research has examined the utility of physiological biomarkers such as the assessment of cerebrovascular function. 9
Following concussion, cerebral blood flow is immediately reduced, resulting in a mismatch between energy supply and demand, 10 potentially contributing to the brain's vulnerability to secondary ischemic injury. 11 Additionally, in traumatic brain injury, cerebral blood flow modulation appears to differ in adults and children, suggesting that age plays a role in cerebrovascular response. 12 Previous research using advanced neuroimaging techniques such as functional magnetic resonance imaging and near infrared spectroscopy has shown that cerebrovascular function is impaired acutely following concussion in college-aged and adult populations, 13,14 following a single-season of high school football 15 and girls' soccer, 16 and in retired male contact-sport athletes. 17 Less is known regarding cerebrovascular function in acutely concussed adolescent patients. Disruptions in cerebral vasoreactivity and autoregulation have been shown in acutely concussed patients 14–21 years of age 18 and reduced overall cerebral blood flow was found in a small sample of acutely concussed adolescent patients (11–15 years of age) compared with controls. 19 These studies have primarily focused on cerebrovascular mechanisms related to perfusion pressure, humoral factors, and overall cerebral blood volume. Little is known about changes in regional metabolic requirements influenced by the energy mismatch, described as neurovascular coupling (NVC), and how concussion may affect this cerebrovascular response to neural activation.
NVC may be assessed by monitoring changes in posterior cerebral artery (PCA) blood flow velocity in response to visual tasks. 20 With an estimated 69% of adolescent patients (11–17 years of age) presenting with vision diagnoses following concussion, 21 NVC may uniquely measure the overlap of cerebrovascular and visual dysfunction in acutely concussed patients. Concussed young adult ice hockey athletes demonstrate increased NVC response to visual tasks relative to controls, 9 and enhanced NVC has been associated with impaired contrast sensitivity in uninjured Special Forces Operations combat soldiers, controlling for concussion history. 22 It is currently unclear how NVC is altered in concussed adolescent patients. Therefore, the primary purpose of this study was to investigate NVC response in concussed adolescent patients seen within 28 days of injury compared with controls. We hypothesized that concussed patients would demonstrate increased overall NVC response compared to controls.
Methods
This prospective cohort study recruited patients 12–18 years of age from the specialty care Minds Matter Concussion Program as a part of our Sports Medicine and Performance Center at the Children's Hospital of Philadelphia (CHOP). Concussed patients were eligible if they were initially seen within 28 days of injury and were diagnosed by a physician trained in concussion using the definition established in the 6th Consensus Statement on Concussion in Sport. 23,24 The consensus definition states that a concussion is “a traumatic brain injury caused by a direct blow to the head, neck or body resulting in an impulsive force being transmitted to the brain” and that injuries will not include any abnormalities on standard structural neuroimaging studies and result in “a range of clinical signs and symptoms that may or may not involve loss of consciousness.” 23,24 Control participants were recruited from patients being seen in the Sports Medicine and Performance Center for musculoskeletal injury and were included if they either had no concussion history or were experiencing no ongoing symptoms from a previous concussion. Patients were excluded if they reported a medical history of sickle cell anemia, 25 or were unable to consent or complete study procedures. All participants self-reported demographics, medical history, and concussion history. Concussed patients also self-reported symptoms using the Post-Concussion Symptom Inventory (PCSI) which asks patients to report the symptom severity. Participants completed the version of PCSI validated for their age group.
Thus, participants 13–18 years of age reported symptom severity on a scale from 0 (not a problem) to 6 (severe problem) (range = 0–132) and participants 12 years of age reported symptom severity on a scale of 0 (no) to 2 (a lot) (range = 0–34). 26 The PCSI was also divided into separate domains consisting of somatic (headache, nausea, light sensitivity, and noise sensitivity), vestibular-ocular (balance problems, dizziness, visual problems, and clumsy movement [teen version]), cognitive (answering questions slowly, difficulty concentrating, difficulty remembering, confusion [teen version], and feeling mentally “foggy”), sleep (drowsiness, feeling slowed down, sleeping more [teen version], and fatigue [teen version]), and emotional (feeling more emotional [teen version], nervousness, sadness, and irritability). Concussed patients were included regardless of the presence/absence of visual concussion symptoms. All participants were also prompted to report symptoms provoked by the task. The study was approved by the CHOP Institutional Review Board (IRB# 17-013875).
NVC
Transcranial Doppler (TCD) ultrasound was used to monitor cerebral blood velocity. Ultrasound gel was applied to a 1.2 MHz Doppler probe (Lucid M1; NovaSignal, Los Angeles, CA) which was placed on the left temporal window. The left PCA was identified at ∼60–70mm from the probe and optimized according to previously published criteria. 25 If a PCA signal could not be optimized on the left side, an attempt was made to identify the PCA on the right side, as previous literature demonstrates no significant difference in PCA signals bilaterally. 27 This occurred in one concussed patient and three control patients. After the PCA was identified and optimized, the probe was locked in place using a fitted head frame. To assess NVC, the patient was seated upright in a chair ∼50–60 cm from a visual screen (61 cm desktop computer). To measure resting PCA velocity, the patient was instructed to focus on a fixation cross on the visual screen for 2 min. Participants then completed two visual tasks to measure NVC, the first of which was a reading task. For this task, the study team allowed the patients to pick an article that was most interesting to them from a collection of articles at least one grade level below their current grade. Patients then alternated between 20 sec of eyes closed and 40 sec of eyes opened for five trials, reading the article while their eyes were open. The patients then rested for at least 2 min. The second visual task was a visual search task in which patients completed five trials of 20 sec eyes closed and 40 sec eyes open to five unique Where's Waldo? challenges. Patients were instructed to search for the full 40 sec. In each Where's Waldo? challenge, Waldo was photoshopped out to encourage searching. If patients believed that they had found Waldo, they were shown images of and instructed to search for other characters (Wilma, Wizard Whitebeard, and Woof, Waldo's dog).
Raw TCD data were measured at 125 Hz and filtered using a dual pass 4th order Butterworth filter with a 2 Hz cutoff using custom Matlab scripts (v2022a; Mathworks; Natwick, MA). Average resting PCA velocity was derived by averaging the PCA velocity across the 2-min resting period. For the visual task data, filtered PCA velocity data were converted to time-series profiles representing 40 consecutive 1-sec averages for stimulus response during each trial. In order to adjust for unknown insonation angles, time-series profiles were calculated relative to the average PCA velocity 3–5 sec prior to stimulus onset. Profiles were then averaged across the five trials for each task, generating a single ensemble-averaged 40-sec profile representing relative NVC response for each participant.
Statistical analysis
Descriptive statistics were used to describe patient demographics. Independent samples t tests were performed to determine group differences (concussion vs. control) in continuous demographic variables (age, height, and weight). Chi-square tests were used for categorical variables (sex, race/ethnicity, sport participation in the last year [contact, limited-contact, and non-contact], 28 and concussion history). Group differences in resting PCA velocity were examined using independent t tests. To assess group differences in relative NVC response curves, ensemble-averaged responses to the NVC protocol were plotted to inform the mean structures of the statistical models, per prior literature. 29,30 Based on these plots, we employed separate linear mixed-effects models using a linear splice with one knot located at time = 6 for the reading task and at time = 5 for the visual search task. Differential response to task was modeled using an interaction between group (concussion vs. control) and task (reading vs. visual search) using a linear splice with one knot located at time = 7. All linear mixed-effects models were fit with unstructured covariance patterns, and empirical Wald tests were used to evaluate statistical significance. Age, sex, and symptom severity (concussion cohort only) effects were assessed for concussed and control cohorts separately for each visual task and explored as covariates for group differences models, but were not significant and were therefore dropped from the final models. Alpha was set to 0.05 a priori and all analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC).
Results
A total of 21 concussion patients (female = 8 [38.1%], age = 14.4 ± 1.9 years) and 20 control patients (female = 7 [35.0%], age = 14.4 ± 2.0 years) were included in analysis. One concussion patient was unable to complete the visual search task because of exacerbated symptoms (headache) caused by the task, and was excluded from the visual search task analysis only. Demographic information did not differ between concussed patients and controls (Table 1). Concussed patients completing the teen version of PCSI reported a median PCSI symptom severity of 25.5 (interquartile range [IQR] = 19.3,38.8) and concussed patients completing the child version of PCSI reported a median PCSI symptom severity of 15 (IQR = 4,21) (Table 2). Nine (42.9%) concussion patients and four (20%) controls reported task-provoked symptoms (Table 3). Concussion patients presented to the specialty care concussion program an average of 11.2 ± 6.6 days after injury. Control patients included both those with acute and those with chronic musculoskeletal injuries and therefore varied in days since injury, ranging from 5 days to having the chronic effects of a musculoskeletal injury that had occurred >1 year ago. Resting PCA velocity did not differ between concussed patients (36.6 ± 8.0 cm/sec) and controls (39.3 ± 8.5 cm/sec) (p = 0.30) (Fig. 1). There were no significant group differences in relative NVC response curves during the reading task (F 1,1560 = 2.23; p = 0.14) or the visual search task (F 1,1521 = 2.04; p = 0.15) (Fig. 2). When examining the interaction between group (concussion vs. control) and task (reading vs. visual search), we found that differential response to task (e.g., increase from reading task to visual search task) was significantly larger in concussed patients than in controls (F 1,3158 = 16.96; p < 0.001). The NVC response to the visual search task was 7.1% higher than the response to the reading task in concussion patients, relative to being 5.5% higher in controls (Fig. 3).
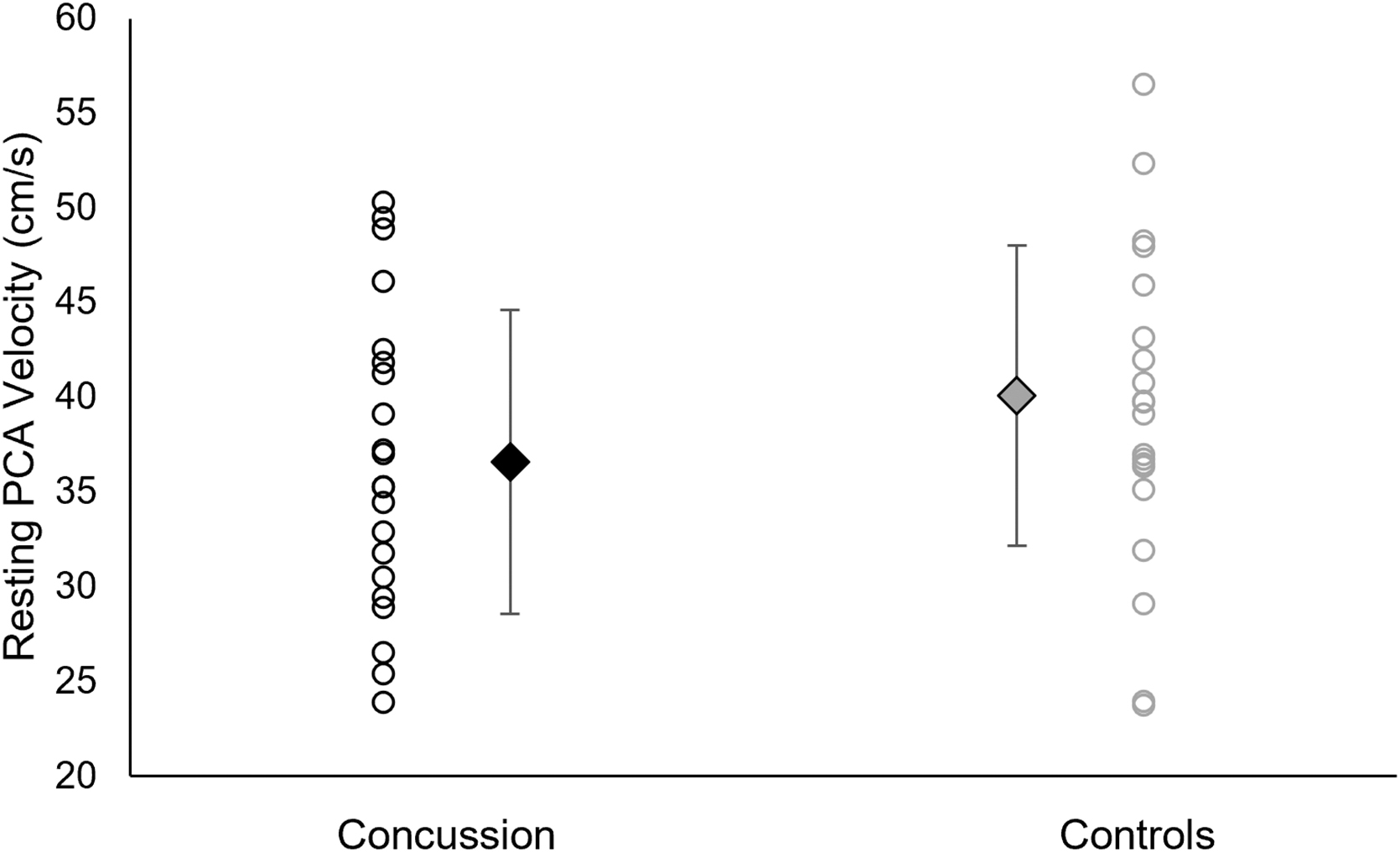
Resting posterior cerebral artery (PCA) velocity for concussion patients and controls. Dots indicate individual mean resting PCA velocities for each group. Diamond markers with standard deviation bars indicate group mean resting PCA velocities. No differences were observed between groups.
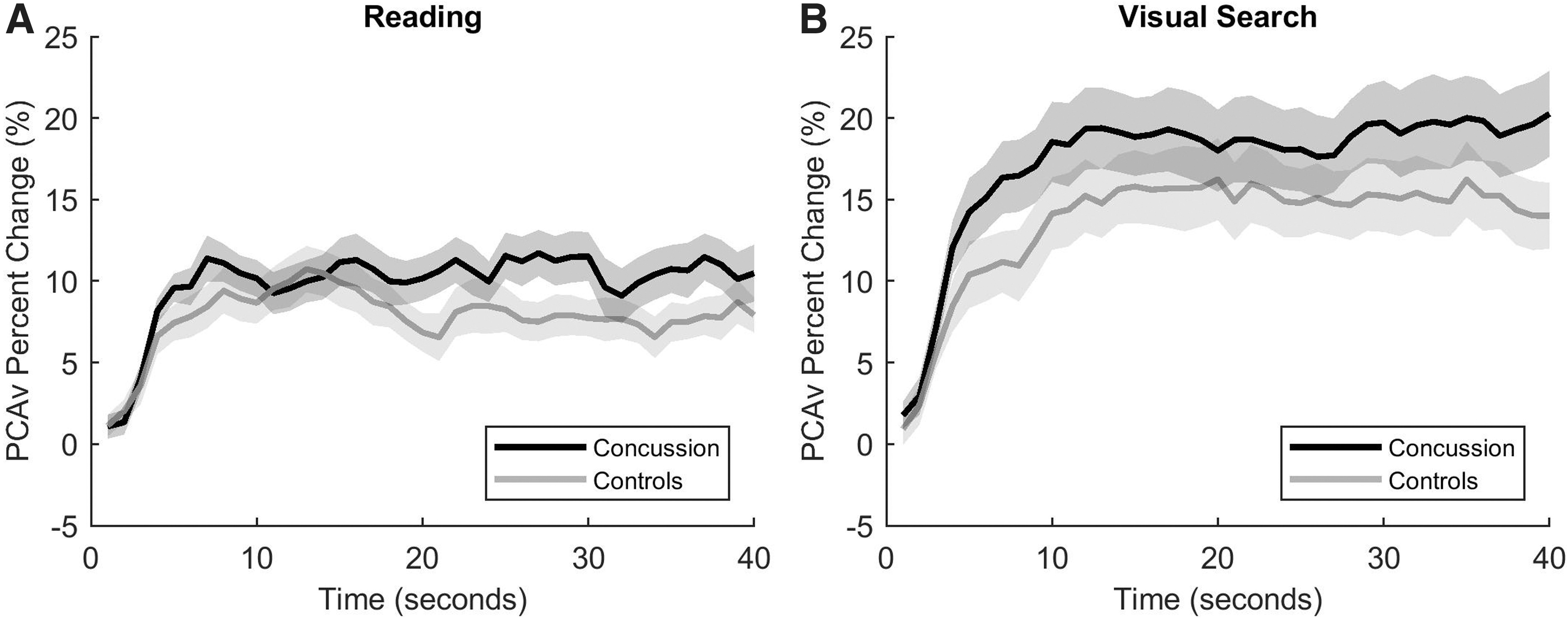
Relative posterior cerebral artery (PCA) velocity ensemble averaged across five trials in response to
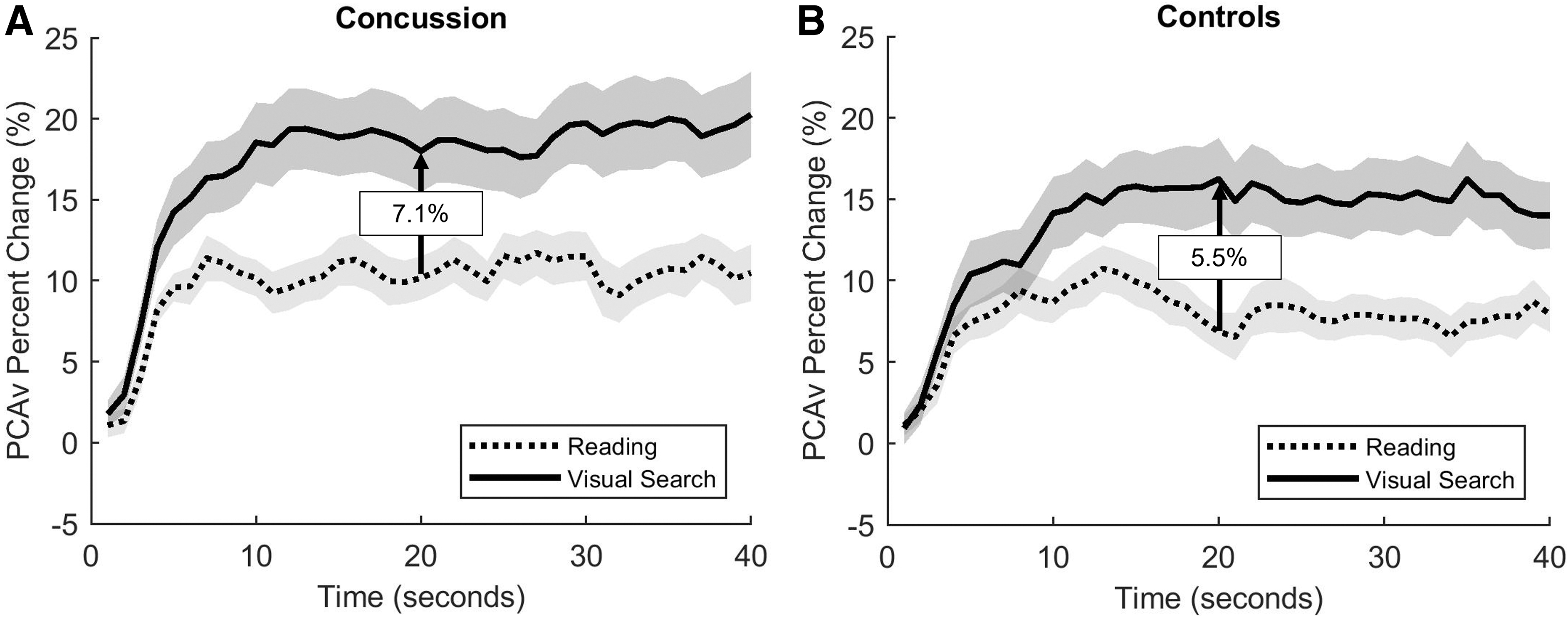
Differential task response for
Demographic Information for Concussion Patients and Controls
SD, standard deviation.
Post-Concussion Symptom Inventory (PCSI) Symptom Severity and Domain Severity for Concussed Patients
IQR, interquartile range.
Task-Provoked Symptoms
Discussion
Our data suggest that adolescent patients seen on average 2 weeks after concussion have a greater differential NVC response to task than do control patients. Specifically, the concussion cohort had a greater difference in the NVC response between the reading task and the visual search task than controls with musculoskeletal injuries. Additionally, when assessing the reading and visual tasks separately, concussed patients demonstrated greater relative NVC response to both tasks relative to control patients, although these did not reach statistical significance. Our findings demonstrate that concussed patients experience cerebrovascular impairment following injury and that NVC assessment may be a sensitive means to measure the physiological consequences of concussion.
During a typical NVC response, increased extracellular glutamate from neural activity triggers both astrocytes and neurons to transmit vasoactive signals to appropriately distribute cerebral blood flow. 20 The stimulation of both astrocytes and neurons leads to a fourfold greater increase in cerebral blood flow relative to the energy needed to complete the neural task. 20,31 Following concussion, NVC response has shown to be elevated in the acute phase relative to controls in adults, 9 suggesting that there is a compensatory mechanism characterized by increased cerebrovascular response to support neural metabolic demand from an inefficient neural network, impaired by injury. 9 Similar to in previous studies in young adult ice hockey athletes, 9 our study found that concussed patients experienced a 2.2% greater NVC response to the reading task and a 4.1% greater NVC response to the visual search task. These differences, however, were not statistically significant, which may be because there was a longer window between injury and visit compared with in the previous study (72 h 9 vs. within 28 days). The same study examined patients at 2 weeks and 1 month post-injury, finding that NVC dynamics had recovered to pre-season values by 1 month. 9 Our study used a 28-day window for inclusion, to reflect the typical recovery time for our study population (pediatric and adolescent patients) 32 and to represent patients reporting to a clinic setting who are less likely to be seen immediately post-injury. Additionally, the difference in findings may be the result of a smaller sample size in our study and/or a slightly younger age range (Wright and coworkers 9 average age = 19.6 years ±1.5 vs. current study average age = 14.4 years ±1.9). Future research should longitudinally evaluate NVC metrics at additional acute and subacute time points to comprehensively describe the time course of cerebrovascular function following concussion through to physiological recovery.
Our study found that concussed patients had a 1.6% higher differential NVC response to task than control patients. This finding appears to be driven by the greater NVC response to the visual search task in concussion patients, as NVC response to the reading task was more similar between groups. This suggests that when going from the reading task to a more difficult visual search task, concussed patients required a greater increase in neural activation to complete the task than do control patients. The visual search task is a more complex task because of greater fixation durations and increased saccadic eye movement, 33 whereas a reading task is more linear, with patients focusing on a singular line of text and potentially not actively visually processing all available information because of word skipping. 34 Our results indicate that this increased complexity of the visual search task requires greater cerebrovascular compensation following concussion compared with the control cohort. Although there is a dearth of literature assessing these outcomes in adolescent concussion patients, this greater cerebrovascular response aligns with previous research in Special Forces Operations combat soldiers, which found a greater differential NVC response to task in soldiers with a history of three or more concussions than in soldiers with a history of one or two concussions. 35 This may suggest that NVC dysfunction following neural injury may be more comprehensively described when assessed during increasingly complex visual tasks. As the mildest form of mild traumatic brain injury, concussions may require particularly sensitive assessment tools in order to identify subtle physiological impairments that are not otherwise clinically apparent, in order to avoid ceiling effects in assessment. Future research should assess visual performance (e.g., eye tracking) and its relation to NVC response changes as well as measure NVC in response to increasingly difficult and ecologically valid tasks, to understand the clinical meaningfulness of these findings.
Our study is not without limitations. We recruited patients from our specialty care concussion program and based the study on the availability of the patients to participate in testing after their clinical visit. Therefore, our sample may be subject to selection bias. The study was also limited by a small sample size and an inability to blind data analysis. The concussed patients included in our study were seen on average 11 days since injury in a specialty care concussion program, and therefore, our results may not be representative of patients presenting at other times post-injury or of patients reporting to other healthcare settings (e.g., emergency department, primary care). Additionally, we were unable to quantify history of repetitive head impact exposure, although we recognize that this may influence cerebral hemodynamics. 29,36 We acknowledge the inherent limitations associated with using TCD to measure NVC. Because of unknown vessel diameters, TCD is unable to measure absolute cerebral blood flow volume and must assume that vessel diameter is constant. Although it is lacking in spatial resolution compared with other advanced neuroimaging techniques, TCD has excellent temporal resolution 25 and is a relatively inexpensive, non-invasive tool to measure cerebrovascular function.
Conclusion
In summary, there is a dearth of literature examining NVC as a physiological biomarker for concussion in adolescent patients. This study demonstrates that cerebrovascular function measured by NVC is impaired following concussion in this age group. Our findings indicate that concussed patients who present within 28 days of injury have a greater differential NVC response to visual tasks than do controls, which is driven by a greater response to the more challenging visual search task, indicating that there is greater neural resource allocation for a more difficult task required after concussion. Future research should explore NVC assessment at additional time points along the recovery trajectory and investigate the utility of NVC as a measure of physiological recovery.
Transparency, Rigor, and Reproducibility Summary
The study was not formally registered because it is not a clinical trial. The analysis plan was not formally pre-registered. A sample of 20 subjects per group was planned based on the availability of subjects. Participants were unable to guess the results of their assessments. Data collection and analyses were performed by investigators who were aware of relevant characteristics of the participants. Data were acquired between February 2021 and November 2022. Data were collected following the participants' clinical visit using transcranial Doppler ultrasound . Data were reduced and processed using Matlab (v2022a; Mathworks; Natwick, MA) and analyzed using SAS 9.4 (SAS Institute; Cary, NC). Data were processed separately, as participants were enrolled to ensure data quality and analyzed at the same time once enrollment was complete. The time required for pre-processing and analysis was ∼2–3 days. Specific equipment and software used to perform acquisition and analysis including the transcranial Doppler ultrasound and SAS may be available upon request from NovaSignal and the SAS Institute. The key inclusion criteria for our experimental group (diagnosed concussion) are established standards in the field. The primary clinical outcome is an emerging standard in the field. The sample sizes and degrees of freedom reflect the number of independent participants. Missing data have been handled via exclusion, as reported in the text. Methods that do not require correction for multiple comparisons were used. No replication or external validation studies have been performed or are planned/ongoing at this time, to our knowledge. Analytic codes used to conduct the analyses presented in this study are not available in a public repository. They may be available by e-mailing the corresponding author, Dr. Kristy Arbogast, as of April 12, 2023. The authors agree to provide the full content of the manuscript on request.
Footnotes
Acknowledgments
This abstract was previously published in Abstracts from The 39th Annual Symposium of the National Neurotrauma Society, including the American Association of Neurological Surgeons (AANS)/Congress of Neurological Surgeons (CNS) Joint Section on Neurotrauma and Critical Care. The symposium took place June 26–29, 2022 in Atlanta, Georgia, USA. The abstract is available at ![]()
Authors' Contributions
Patricia R. Roby: conceptualization (equal), data curation (lead), formal analysis (lead), funding acquisition (lead for T32NS043126), investigation (lead), methodology (equal), writing – original draft (lead), writing – review and editing (equal); Anne E. Mozel: conceptualization (equal), methodology (equal), writing – review and editing (equal); Matthew F. Grady
Funding Information
This study was funded by the National Institute of Neurologic Disorders and Stroke of the National Institutes of Health under award numbers R01NS097549 and T32NS043126 (Patricia R. Roby) and the Pennsylvania Department of Health.
Author Disclosure Statement
No competing financial interests exist.