
Abstract
Significant bowel-related issues after spinal cord injury (SCI) that affect morbidity and quality of life (QOL) include diminished bowel motility, loss of sphincter control, gastric ulcers, autonomic dysreflexia, pain, diarrhea, constipation, and fecal incontinence. Clinical diagnoses and research in humans have largely relied on anorectal manometry (ARM) procedures to increase understanding of the functional effects of SCI on colorectal motility and defecation physiology. Recent pre-clinical rodent studies have also used ARM to further our understanding of bowel-related dysfunctions post-SCI. In the present study, the benefits of different activity-based training (ABT) durations on bowel function were examined. Six groups of male rats including two non-training (NT; uninjured and SCI) and four ABT (quadrupedal [Quad or Q] stepping on a treadmill) groups. All ABT animals received 4 weeks of 1-h daily stepping beginning 2 weeks post-SCI followed by variable amounts for 4 additional weeks (none; daily; once a week; daily for final 4th week only). Outcome measures included fecal output (home cage; metabolic cage) throughout the study and terminal measurements (post 8-week ABT) of external anal sphincter (EAS) electromyography, resting anorectal pressure, and giant contraction (GC) activation under urethane anesthesia. The results indicate that treadmill training normalized defecation amount based on feces weight and food intake, as well as GC frequency, EAS latency and amplitude during fecal expulsion, and resting pressure in specific areas within the colorectum. The two intermittent training groups consistently showed recorded metrics comparable to the non-injured group. The results demonstrate bowel dysfunction in the rodent SCI contusion model with improvements in functional outcomes following ABT. Importantly, the benefits to bowel-related functions with versus without intermittent ABT illustrate the need for periodic therapy to maintain the functional gains of ABT.
Introduction
After traumatic spinal cord injury (SCI), neurological deficits adversely impact a multitude of bodily functions. Many studies have examined the physical, psychological, and general issues that together compromise quality of life (QOL) for people living with SCI. 1,2 When reported, persistent bowel complications represent a top-priority QOL issue, more highly rated than a return of mobility. 3 –6 Additionally, bowel complications impact morbidity and rehospitalization 7 and both correlate with and compound other SCI problems such as urinary issues, depression, and anxiety.
Fecal incontinence, constipation, abdominal distension, diarrhea, difficulty with evacuation, bloating, hemorrhoids, and fecal impaction are commonly reported secondary complications following SCI. 8 –12 Experiencing disrupted bowel function adversely affects QOL in several ways. Individuals with SCI may lack the ability to sense and control bowel function, resulting in lengthy time schedules necessary to complete a bowel program. Further, excessive time investment may lead many individuals with SCI to conduct their bowel program every other day, exacerbating ongoing dysfunction such as constipation, colonic and rectal distention, and bouts of autonomic dysreflexia (a sudden sharp rise in blood pressure with intolerable symptoms). These limitations, therefore, may impede and limit participation in many activities of daily life. 2,5,13 –15
Clinically, most SCIs are upper motor neuron lesions at or above the thoracolumbar sympathetic outflow. Parasympathetic stimulation via the vagus nerve remains unimpeded, 2,16,17 although it is likely indirectly impacted. 18 Sacral reflex circuits, however, are spared. 2,12 Baseline colonic motility is reduced, rectal tone and external anal sphincter (EAS) activity are elevated after chronic injury, and the EAS becomes spastic and dyssynergic, 2,12,13 causing difficulty with evacuation and constipation. 19 Conversely, the internal anal sphincter (IAS) has reduced tone, 12 compromising the ability to maintain continence. Cumulatively, complex coordination between the EAS, IAS, and colorectum is impacted, causing slower movement of material through the colon, or reduced colonic motility. 2,12
Sympathetic activation is inhibitory for defecation, which reduces colonic motility and increases IAS tone. For defecation to occur, excitatory parasympathetic activity must be increased. 2,20 Following SCI, slower motility of material through the colon is typically due to excessive segmental and reduced propulsive activity. 12 Observed reduced motility and slower transit times in patients with SCI 21 often require interventions such as laxatives or manual digital stimulation of the anus to relax the IAS and contract the rectum to initiate defecation. 3,4 A study that utilized manometric catheters and pressure transducers in individuals with SCI reported lower colonic measurements (motility index, activity, number of peristaltic waves, and mean amplitude of wave pattern) during food ingestion relative to controls. 22 Therefore, bowel dysfunction post-SCI causes numerous functional changes that impact the gastrointestinal (GI) tract's storage and evacuation capability.
Anorectal manometry (ARM) is utilized clinically to determine and investigate colonic dysfunction after SCI in humans. 23,24 It has been demonstrated that reductions in motility indices and mean contraction amplitude, 22 reduced colonic motility measures such as the velocity of peristaltic waves, 25 no resting state difference, 26 and increased colonic motility are present after SCI. 13,27 Pre-clinical studies using animal models have considerably improved our understanding of bowel dysfunction. Several rat studies with SCI at the T3–4 spinal level investigating baseline motility in both transected and severe SCI models demonstrated a marked reduction in motility of the distal colon and changes in giant migrating contraction frequency and amplitude. 28,29 A study in cats showed that SCI prolonged transit time significantly, which could be remedied by direct electrical stimulation of the colon. 30
Our recent study utilizing ARM in a rat T9 spinal level contusion model demonstrated baseline differences in rectal function such as increased pressure and contraction frequency and reduced colonic motility. 31 Activity-dependent plasticity resulting from repetitive sensory information has been shown to improve both locomotor and non-locomotor functions in the contused rat model. 32 –34 Exercise and locomotor training (LT) on a treadmill (a rehabilitative activity-based training [ABT]) in the SCI population are well-established therapies that benefit cardiovascular function, mobility, and bladder/urinary function. 35 –40 In parallel with our pre-clinical animal SCI ABT studies, clinical studies investigated bladder, bowel, and sexual function outcomes based on 1-h daily LT sessions and 1-h LT sessions with stand training on alternate days. Post-training results indicated a significant reduction in time taken for defecation, as well as an observed reduced frequency of defecation, and increased awareness of the need to defecate. 41
Therefore, the current investigation explored the impact of ABT on bowel function in a clinically relevant T9 spinal level moderate-severe contusion injury model. Outcome measures combined functional output (weekly metabolic cage and home cage fecal collections) and terminal post-training ARM assessments (baseline activity measurements, distention-induced contractile responses, and EAS electromyography [EMG]) to provide a comprehensive picture of bowel function and functional gains following LT. Intermittent durations of LT were also assessed as compliance to daily exercise regimens is unlikely and not always practical.
Methods
Animals
Animal procedures followed National Institutes of Health guidelines and were reviewed and approved by the Institutional Animal Use and Care Committee at the University of Louisville, School of Medicine. Seventy-four male Wistar rats (Harlan; Sprague Dawley, Inc., Indianapolis, IN, USA) were housed under 12-h light-dark cycle conditions with ad libitum food (Laboratory Rodent Diet) and water provided and soft-paper home cage bedding (∼4 mm2 squares; AlphaDry). All bowel functional assessments occurred prior to injury for baseline, daily post-SCI (Days 2–7), and then weekly throughout the recovery period. Terminal bowel assessments were conducted during the 10th week after injury.
Spinal cord injuries
Surgical protocols have been published previously. 32,33,42,43 Briefly, all animals were anesthetized with a mixture of ketamine (80 mg/kg; Ketoset; Ford Dodge Laboratories, Fort Dodge, IA, USA) and xylazine (10mg/kg; Anased; Akorn, Inc., Lake Forest, IL, USA). Chlorohexiderm scrub (Dermachlor 4%; Henry Schein, Dublin, OH, USA) was applied to the incision site after shaving, and eye lubricant (Optixcare; CLC Medica, Ontario, Canada) was applied to maintain moisture. Rats received antibiotics including gentamycin (subcutaneous, 5 mg/kg, once daily for 5 days; Gentafuse, SparHawk Laboratories, Inc., Lenexa, KS, USA) and penicillin G (subcutaneous, 0.5 mL, prior to initial surgery as a prophylactic measure; Penject; Bimeda, Inc., Le Sueur, MN, USA). Meloxicam, an anti-inflammatory/analgesic (subcutaneous, 0.2 mL; Eloxiject; Henry Schein, Melville, NY, USA), was administered before surgery and then once daily for 3 days for pain management. Additional fluids were given (subcutaneous, 10 mL, 0.9% sterile saline; one 5 mL bolus over each hip) prior to surgery and administered as needed during the recovery period.
Rats received a T9 level contusion using the Infinite Horizon Impactor (Precision Systems and Instrumentation, LLC, Fairfax Station, VA, USA) set to our lab's standard force of 215 kDyne (yields a moderate-severe SCI with a mean white matter sparing of 16.0 ± 4.2% and gray matter sparing of 1.5 ± 1.6% at the lesion epicenter). 42 An initial midline thoracic vertebra incision and T8 laminectomy were then performed, exposing T7 and T9 spinous processes that were subsequently clamped to stabilize the spinal column prior to applying the contusion. Sham surgical rats (n = 9) received the same surgical protocol, minus the contusion. Following this procedure, the muscle was sutured with a 4-0 Ethicon non-absorbable surgical suture and the skin was closed with surgical autoclips (Mikron Precision, Inc., Gardena, CA, USA). Antibiotic ointment was applied to the incision area. Heating pads were utilized to help maintain body temperature during- and post-surgery and during recovery. Additional post-surgical care included manually emptying the bladder (Crede maneuver, 3 times a day for 5 days until fully reflexive 32,42,43 ), convenient food access via food pellets placed on the floor of the cage, visual inspection of the incision site, assessment of possible distress (poor grooming, grimacing, over-grooming, porphyrin staining, autophagia, bloody discharge), and cleaning soiled fur with water (room temperature) and blotting dry with paper towels to prevent urine scald.
Basso-Beattie-Bresnahan (BBB) testing
Observation of hindlimb function and mobility was conducted in an open field using Basso-Beattie-Bresnahan (BBB) criteria previously described and published. 32,33,42 Two observers conducted and confirmed testing (once pre-injury then weekly post-SCI). Collected data provided a supplement to histological measurements as an additional indicator of the severity, extent, and consistency of spinal cord lesions.
Activity-based training (ABT)
Our published ABT protocol 34 was utilized in this study with some adjustments in frequency specific to each training group. The total number of male rats used was 74, which includes 9 shams and a target of 12–15 per SCI group. Five SCI training groups were established in total (Fig. 1). Four groups received assisted quadrupedal (Quad or Q) stepping for 58 min on a treadmill 32,34 to varying degrees as follows: Quad (5 days per week for 8 weeks), Q4NT4 (5 days a week for 4 weeks followed by a 4-week non-training [NT] period), Q41D4 (5 days a week for 4 weeks followed by 1 day a week for 4 weeks [1D4]), and Q4NT3Q1 (5 days a week for 4 weeks followed by NT for 3 weeks then 1 week of training). Each group timeline is provided in Figure 1. Note that all ABT groups initially received 4 weeks of daily weekday training starting after a 2-week post-SCI recovery period.

Training protocol. Description of training group protocols, nomenclature, and timeline. ARM was performed at the end of the 8-week period. Numbers are weeks, except “1D” (1 day a week). ARM, anorectal manometry; NT, non-trained; Quad or Q, quadrupedal stepping. Color image is available online.
Feces collection
Feces data were collected over a 24-h period using two distinct methods per our published protocol 42 : home cage manual collections, and the Comprehensive Lab Animal Monitoring System (CLAMS; Oxymax, Columbus Instruments, Columbus, OH, USA). CLAMS measurements were collected in the following manner: twice prior to injury (baseline) and once weekly thereafter until and including the terminal week. Home cage measurements were collected at (pre-injury) baseline, Days 2–7 during the acute recovery period, and then once weekly until the terminal week. Metabolic cage collections contained feces with some embedded food particulates (crumbs), which were counted for the 24-h period. Feces from home cages were hand-collected and counted. All metabolic cage fecal material was air-dried under a fume hood for 2 h prior to being weighed to alleviate moisture content. Home cage fecal matter was desiccated due to exposure and proximity to paper bedding, and therefore were weighed immediately.
Anorectal manometry (ARM) procedure
Terminal testing and data collection required a replete, normal GI system. Accordingly, there was no food restriction or overnight fasting. On the day of ARM testing, rats were first anesthetized with urethane (1.2 g/kg, subcutaneous; Aldrich Chemistry, St Louis, MO, USA). The animal was placed ventrally on a heated water pad (38°C/100°F; Gaymar) to maintain body temperature with the tail elevated using a tail clamp to facilitate access to the anus for testing. Fine wire hook electrodes (stainless steel wire, 0.003” diameter; A-M Systems, Sequim, WA, USA) were bilaterally implanted into the EAS with a 27-gauge needle inserted at an oblique angle starting at the midline and then moving laterally through the muscle to a depth of approximately 1–2 mm. The electrodes remained securely in place due to the construction of a hook at the distal end of the electrode. The EMG signal was amplified (A-M Systems, four-channel differential AC amplifier), and then recorded using a CED Micro1401 acquisition unit and Spike 2 software (version 8.21).
The ARM testing procedure, previously published with illustrations and accompanying example data traces, 31 first involved EAS EMG testing, which was divided into four events in total. EMG recordings were first made during balloon catheter insertion (deflated) to approximately 2 cm from the anal verge, followed by inflation of the balloon (within 1–2 sec) with 0.8 mL water (size of a large fecal bolus), then a pause of 5 sec before the inflated balloon was very slowly retracted out through the anus over a period of approximately 7–10 sec to mimic a defecation stimulus. Lastly, EMG activity recordings continued post-balloon-expulsion to capture EAS closure.
Manometry pressure recordings were then collected by an in-house constructed balloon catheter 31 comprising a modified butterfly catheter with a 1-cm balloon made from a 2-cm2 piece of a non-lubricated latex condom, with two attached pressure sensors (Millar, SPR-524, 3.5F) affixed at 2 cm and 4 cm, respectively, from the rostral end of the catheter tubing using Parafilm (Bemis, USA). Pressures at nine positions were tested (2–11 cm) as previously described. The catheter probe was first inserted into the distal-most position depth and fixed in place using tape around the tail to prevent movement during inflation trials. Approximately 2 min (120 sec) of baseline pressure recording was collected, followed by stimulation trials that began with balloon inflation with 0.8 mL water for 6–8 sec before deflation. Responses to the balloon inflation were then recorded for a minimum of 60 sec, followed by repeating the procedure again for a total of four trials. At the conclusion of the fourth stimulation trial (60 sec), the probe apparatus was moved to the next level to be tested, repeating the procedure until all nine levels were measured. Lubrication was provided as needed during the procedure to facilitate movement (Surgilube; HR Pharmaceuticals, Inc., York, PA, USA).
In the present study we monitored the potential confound of fecal impaction during ARM testing by retracting and reinserting the balloon catheter after observing recording anomalies. In such rare cases, the presence of fecal matter on the balloon bolus, pressure lower than baseline, or the inability to progress the probe due to obstruction were observed and mitigated by pausing testing or filling/withdrawing the balloon to aid the passage of fecal matter.
EMG data quantification and filtering
Signals were captured using a four-channel differential AC amplifier (AM-Systems) and acquisition unit (CED Micro4 1401). EMG signals were also filtered using a 5–500 Hz band-pass filter application. All signals were then rectified (rectify/DC remove) and quantified for amplitude, duration, and latency (derived from either the balloon exit from the anus or inflation stimulation trials recorded on the balloon pressure channel).
Trans-cardiac perfusion and tissue collection
Following testing, animals were perfused after receiving an overdose bolus of urethane anesthesia (0.3 mL, 50% solution) and subsequently confirming lack of muscle reflex to a moderate toe pinch, shallow breathing, and reduced whisker movement. Animals were then rapidly perfused as previously described. 32,33,42 Heparinized phosphate-buffered saline (300 mL) was used for exsanguination, followed by 300 mL of 4% phosphate-buffered paraformaldehyde (pH 7.2) for tissue perfusion.
The rectum, distal colon, anus tissue, and left kidney were collected after exsanguination but before paraformaldehyde perfusion and either frozen or immediately processed for future biochemical analyses. During exsanguination, a surgical incision was made into the abdominal cavity (laparotomy) and continued along the perineum. Incisions were also made around the anus muscle using a combination of sharp and blunt dissection to gently free the rectum and the colon from ligament attachments. After exsanguination, the colon (approximately 12–14 cm in length) was then detached from the mesentery (using blunt dissection) and the anus was pulled through the pelvis and into the abdominal cavity. The colon was then clamped using a hemostat distal to the cecum and the entire tissue segment was removed. The left kidney was then clamped using a hemostat and removed. Both procedures required the perfusion pump to be off for approximately 30 sec before resuming and then switching over to paraformaldehyde infusion of the remaining tissues (fixation).
Histology and lesion site sparing quantification
SCI histology protocols have been previously published. 32,33,42 Briefly, SCI tissue was collected 1 cm rostral and caudal to the lesion site and placed in 4% paraformaldehyde for 48 h, then in 30% sucrose for a further 48 h. Tissue was then cut on a cryostat into coronal sections approximately 35 μm thick and mounted, and then thawed for later staining. Prior to staining, tissue slides were removed from −20°C storage and placed on a heated slide warmer (Fisher Scientific; 40–50°C) for approximately 2 h. Staining used cresyl violet for gray matter (Acros Organics) and luxol fast blue for white matter (Sigma) for sparing quantification. Micrographs were taken (SPOT RT3, 2MP microscope camera, Nikon Eclipse E400 microscope, 40 × magnification) and then quantified using established protocols. 32,33,42 Sparing percentages were calculated by first averaging the area (mm2) of white and gray matter in intact rostral and caudal sections from the lesion site. The averaged intact measurement was then compared with the lesion epicenter area (mm2) and a percentage of white and gray matter sparing was calculated.
Statistical analysis
Pre-SCI and terminal weight difference, post-SCI injury displacement and force, and terminal white matter sparing histology were analyzed using one-way analysis of variance (ANOVA) followed by Tukey's Honest Significant Difference (HSD) post hoc t-tests for multiple comparisons. Home cage, metabolic cage, food intake, baseline pressure probe 1/probe 2, and EAS amplitude data were analyzed using repeated measures ANOVA followed by Bonferroni post hoc t-tests for multiple comparisons (SPSS, v28). Outlier BBB (averaged left and right) score values that were
Confirmation using the Grubbs outlier test on the maximum (BBB) and minimum (displacement) scores yielded p-values <0.00071. Significant but even stricter p-values (0.0002 and 0.0014) were obtained using the >3 SD procedure, confirming comparable results when the data are normally distributed, and the sample size is very large (n = 58). BBBs were analyzed using repeated measures ANOVA followed by Bonferroni post hoc t-tests for multiple comparisons. EAS latency differences between groups were compared using the non-parametric Mann-Whitney U test. Probabilities
Principal component analysis (PCA) with varimax rotation was performed to identify relationships between outcome measures. Based on their interrelationships, 2–3 components (i.e., factors) were identified and accounted for 57.8–100% of the total variance. Separate PCAs for baseline, week 4, and week 8 outcome measures were performed for home cage fecal weight, metabolic cage fecal weight, and 24-h food intake for all groups. PCA for ARM EAS EMG included latency and amplitude data for all groups. Probe 1 and 2 ARM pressure was analyzed in separate PCAs for all groups from 0- to 6-cm depths. ARM giant contractions (GCs) were analyzed using Chi-square analysis to compare the frequency of occurrence for each experimental group.
Results
Animals
Six groups were tested, including a Sham group, an NT group, and four Quad stepping training groups (Fig. 1). Only rats that completed all data sets (66 of 74 total) were included in the analysis (Sham, n = 9; NT, n = 13, Quad, n = 11; Q4NT4, n = 10; Q4NT3Q1, n = 8, Q41D4, n = 15). Reasons for the few exclusions included a non-responsive EAS in EMG trials (n = 1, Quad group; n = 1, Q4NT4 group), a fecal blockage that prevented 10–11 cm ARM testing (n = 1, NT group), BBB and impactor force/displacement outliers (n = 1, Q4NT3Q1 group), and health complications during the post-SCI recovery period (n = 3, Q4NT3Q1 group; n = 1, Q4NT4 group).
Injury outcome parameters
As seen in Table 1, the mean force of impact did not differ across training groups (p = 0.320). Mean displacement also did not significantly differ across training groups, apart from the Q41D4 relative to the Q4NT4 SCI group (p = 0.035). Mean BBB scores were significantly reduced compared with the Sham group after injury (p < 0.001), and remained so throughout the study duration, regardless of training group. All injured groups had mean BBB scores around 10 by 14 days post-injury, a score indicating occasional weight-supported plantar steps and no forelimb-hindlimb coordination. White-matter-sparing mean averages for all injured groups were not statistically different (p = 0.159; Fig. 2), including the one group with a higher mean displacement impactor value that would be indicative of more epicenter damage (Q41D4).
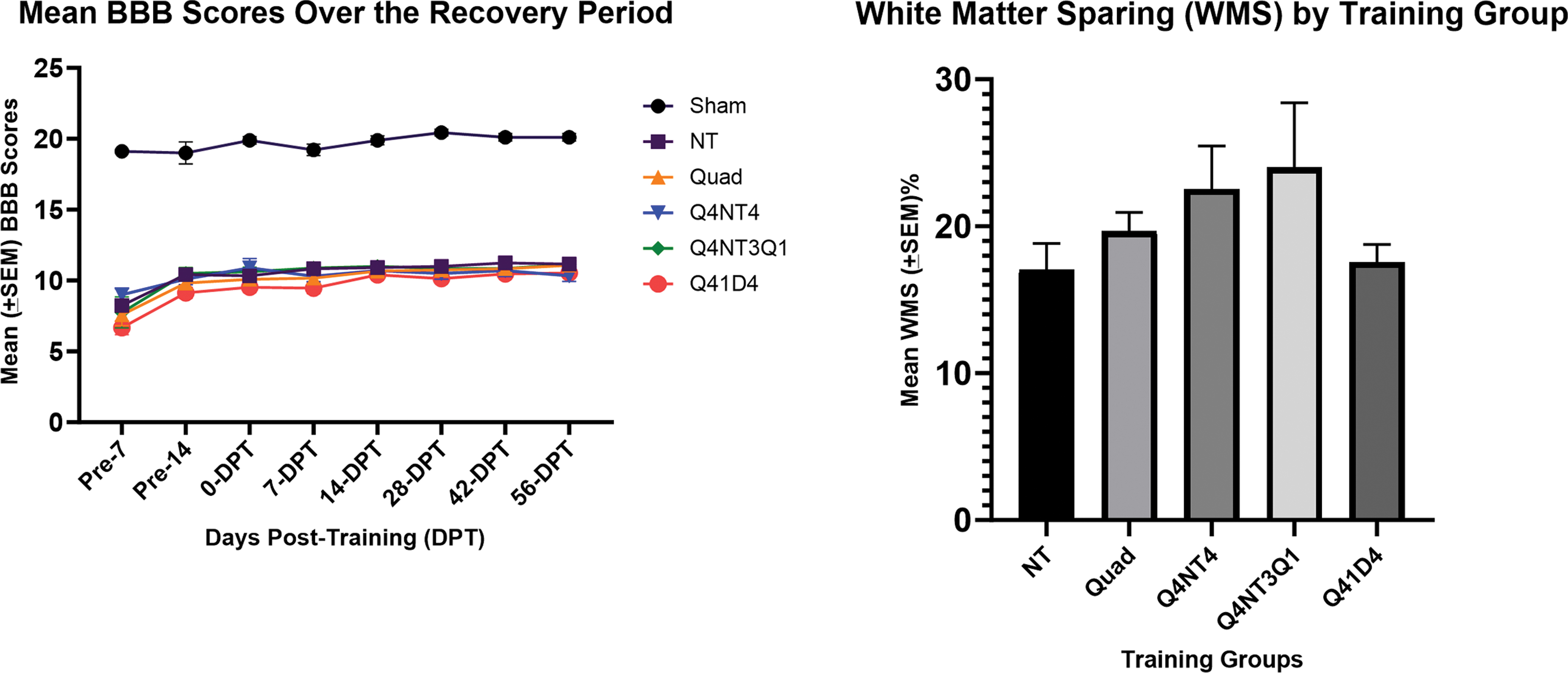
Mean BBB scores over the recovery period and white matter sparing (%) for all experimental groups. Note that there were no significant differences between groups at any time-point for BBB and for lesion histology at the end of the study. Pre-7 and Pre-14 indicate 2- and 2-week post-SCI time-points prior to the start of training. Groups per Figure 1. BBB, Basso-Beattie-Bresnahan; NT, non-trained; Quad or Q, quadrupedal stepping; SCI spinal cord injury; SEM, standard error of the mean. Color image is available online.
Mean Impactor Force and Displacement for All Experimental Groups (
NT, non-trained; Quad or Q, quadrupedal stepping.
Animal weight
The amount of weight gained during the 10-week recovery period was not statistically significant between the Sham (mean = 146 ± 7.5 g) and NT (mean = 128 ± 9.8 g) groups. Mean weight gain differences (terminal vs. day of SCI weight) for the ABT groups were as follows: Quad (mean = 114 ± 13.5 g), Q4NT4 (mean = 183 ± 11.6 g), Q4NT3Q1 (mean = 166 ± 32.4 g), and Q41D4 (mean = 95 ± 8.7 g; p < 0.001). The disparity noted between animal weights, particularly the Q4NT4 and Q4NT3Q1 animals relative to other groups, can be partially explained by the cessation of training for 4 or 3 weeks as well as an unavoidable wait time between arrival at our facility and date of SCI.
Feces data
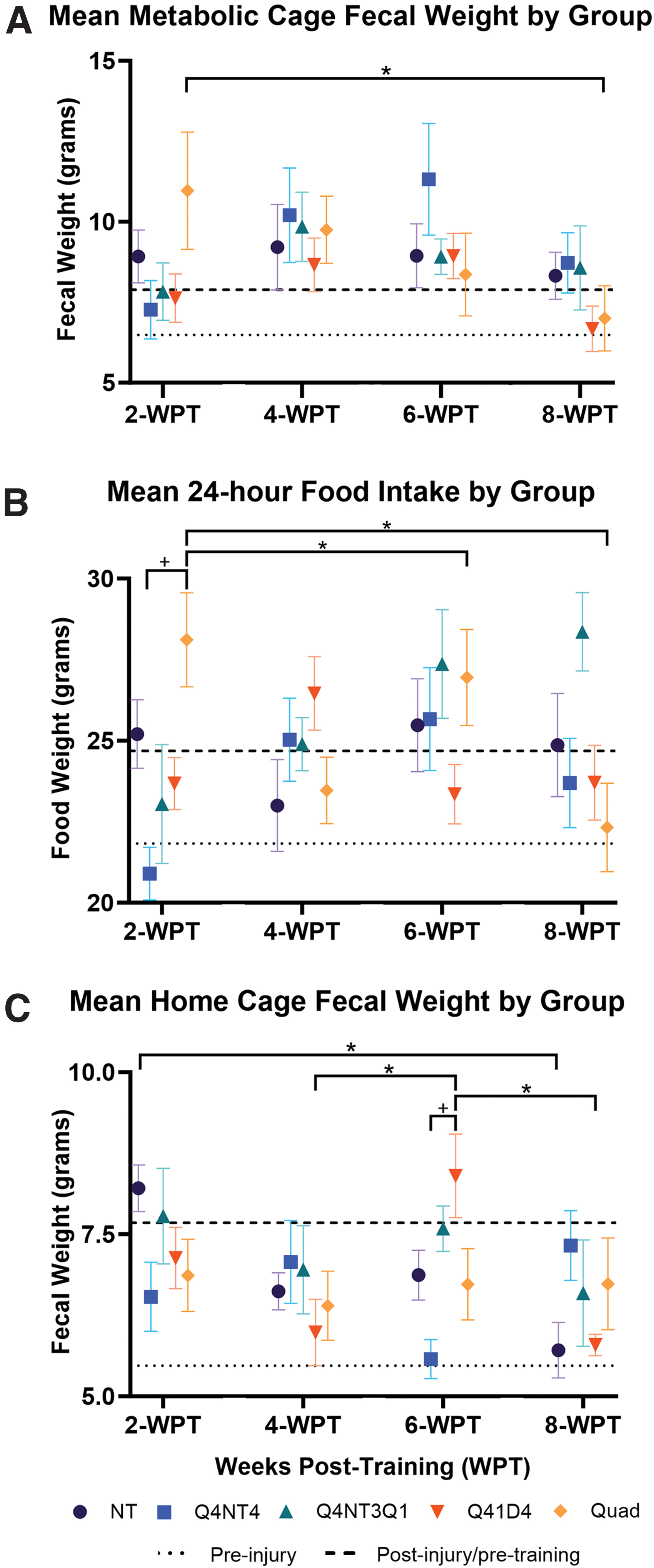
A summary of functional measures indicates an overall general pattern of fecal weight and food intake changes over time across groups (Fig. 3). For example, both metabolic cage fecal weight and food intake significantly increased (p < 0.001) as the recovery period progressed before returning to the post-injury average by 8 weeks post-training (WPT) (Fig. 3A,B). Feces weight for home cage collections were also significant (p < 0.001) and followed a similar pattern over time (Fig. 3C). Further evaluation using PCA was completed for metabolic cage feces and food intake collection data and home cage feces data at pre-injury (baseline), post 4 weeks training (week 4 time-point), and post 4 weeks of intermittent training (week 8 time-point). The analysis (Fig. 4) illustrates the close association between Sham group animals (encircled area containing black dots) and the Q41D4 training group (encircled area containing green hexagon) over time.
Metabolic cage fecal weight
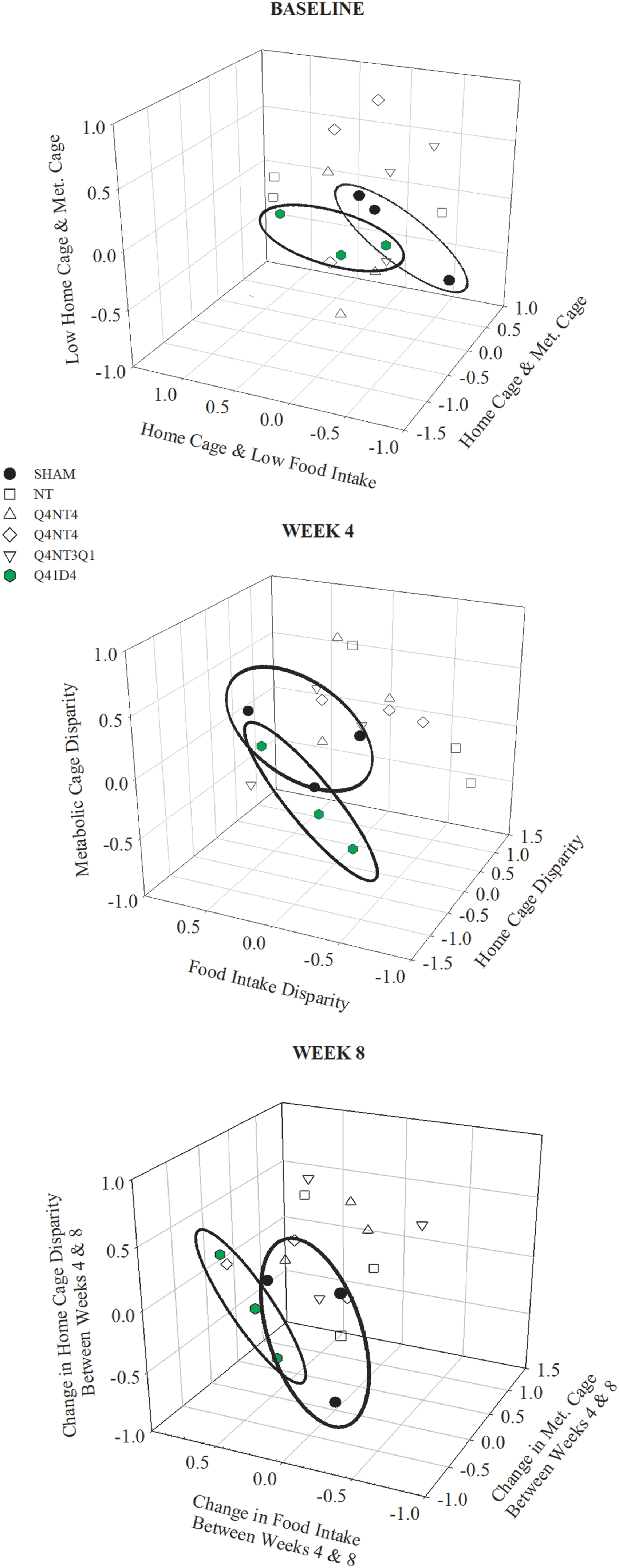
Metabolic cage feces and food intake and home cage feces principal component analysis for all study groups. Note that the Sham group was not treadmill trained and had no contusion injury and would therefore be expected to record negligible differences over the duration of the study for each of the three functional outcome measures. Importantly, the Q41D4 group, which went from training 5 days a week for weeks 1–4 post-training to 1 day a week for weeks 5–8 post-training did not show any measurable change in home cage/metabolic cage feces output/food intake input (week 4 vs. 8, respectively). NT, non-trained; Quad or Q, quadrupedal stepping. Color image is available online.
EAS EMG data
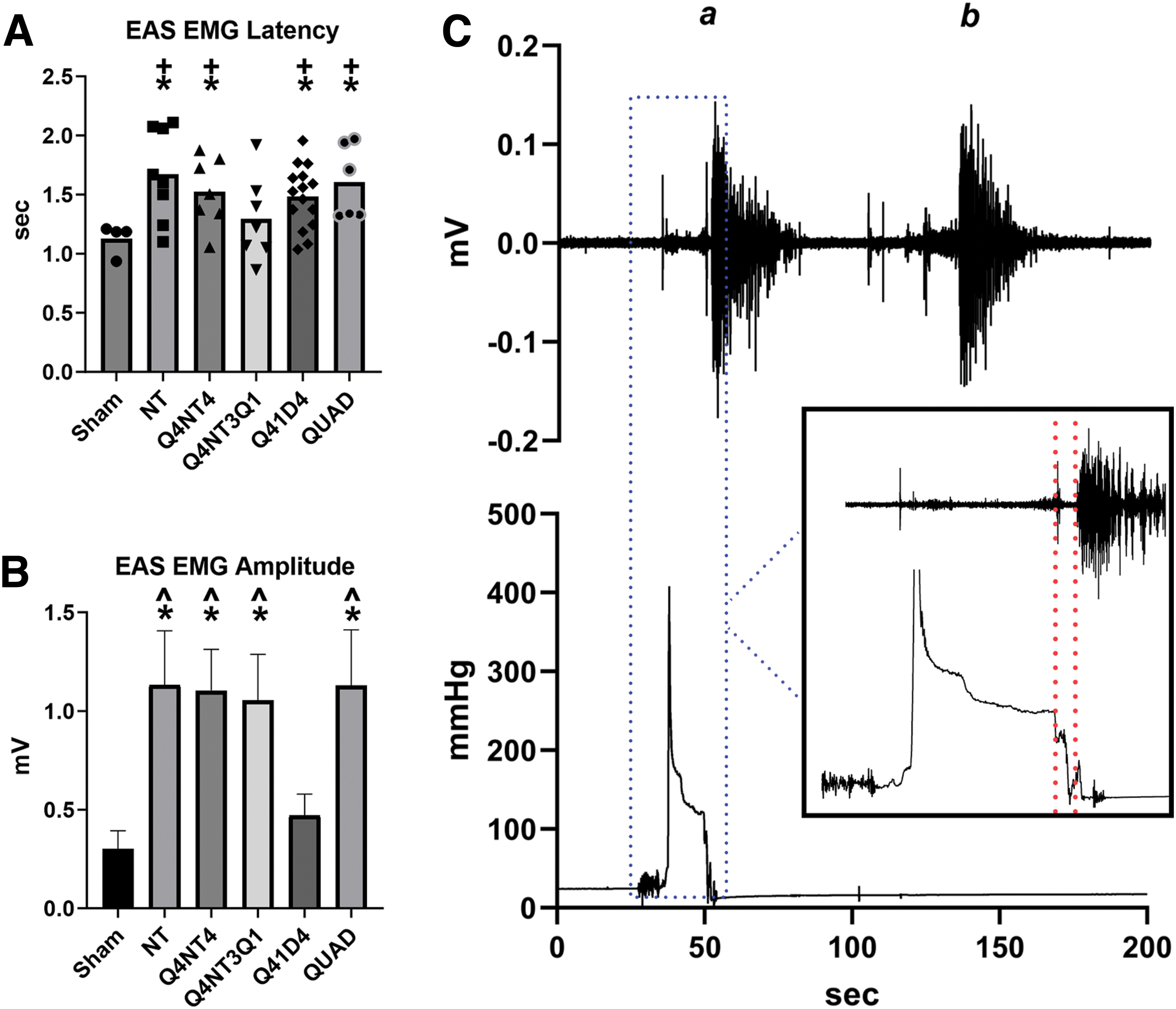
For the EAS data, there was a significant difference (p < 0.05) in delayed response latency in the SCI non-trained, Q4NT4, Q41D4, and Quad groups compared with Sham group animals and the Q4NT3Q1 training group (Fig. 5A). Analysis of response amplitude indicates a significant group effect (p < 0.015) with the SCI non-trained, Q4NT4, Q4NT3Q1, and Quad training groups recording larger mean responses than Sham and Q41D4 groups (Fig. 5B). There were no significant differences (p = 0.469) in the duration of the EAS excitatory response among any of the groups. An example showing an EAS response in a Sham group animal to balloon catheter stimulation of the anus and a similar response to fecal pellet expulsion is provided (Fig. 5C). Note in this example the similarities between amplitude, latency, and duration.
Mean EAS EMG response latency
ARM testing—baseline pressure
A summary of results for baseline pressure is presented in Table 2. Resting baseline pressure for the NT SCI group was significantly lower than the Sham group at all tested depths (0–9 cm) on probe 1 (p < 0.0001), consistent with higher normal tonal pressure that is necessary for movement of content. 44 Overall, there was a significant group effect (p < 0.0001) and depth effect (p < 0.002) for baseline pressure. For example, Sham and Q41D4 groups were not significantly different at 0-, 3-, and 7-cm depths. The Q41D4 group baseline pressure was significantly different from the NT group at all tested depths and the Quad group was significantly different from NT animals at 0-, 1-, 5-, 6-, 7-, 8-, and 9-cm depths (p = 0.005). Sham and Quad groups were not significantly different at 1- and 7-cm depths.
Baseline Pressure (mm Hg) for Probe 1 and 2 at All Tested Depths (± SEM)
Significantly lower than sham (p < 0.05).
Significantly higher than NT (p < 0.05).
NT, non-trained; Quad or Q, quadrupedal stepping.
Baseline pressure results on probe 2 recorded both significant group effect (p < 0.0001) and depth effect (p < 0.0001), but the only significant difference between Sham and SCI NT groups was recorded at 1 cm depth (p = 0.005). The Q4NT4 group baseline pressure was significantly higher than NT animals at 0-, 1-, 2-, 4-, 5-, 6-, and 7-cm depths and the Q41D4 group was significantly higher than the NT group at 0-, 2-, and 3-cm depths (p = 0.005). The Quad group was significantly higher at 2-cm depth (p = 0.032; Table 2). PCA was completed for baseline pressure data for all groups for pressure probes 1 and 2 (Fig. 6). Each component axis determined a positive or negative correlation for pressure disparity, low pressure, and improved pressure, respectively, for all groups. Note that tonal differences between probes likely relate to proximity relative to the uninflated balloon.
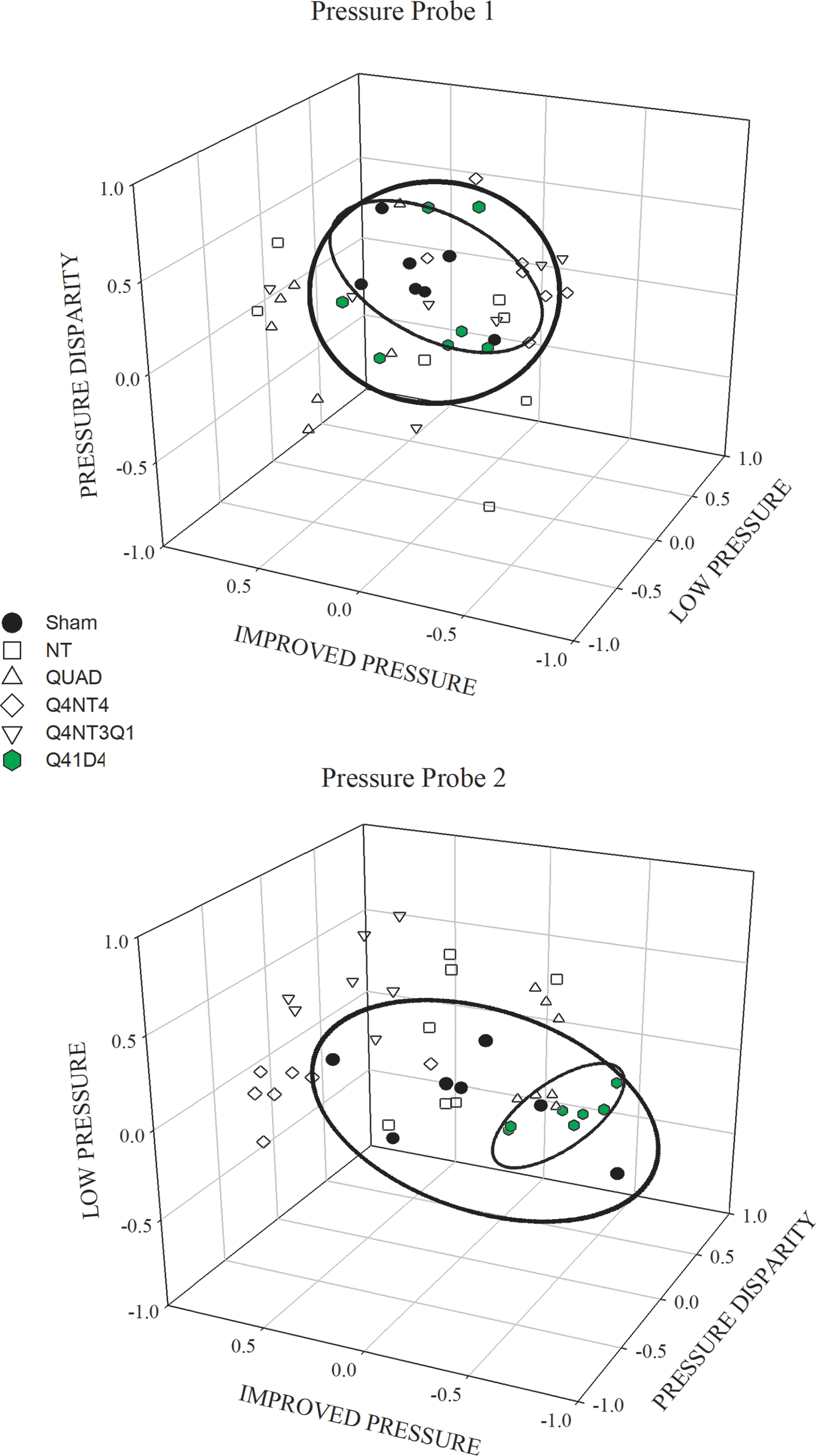
Resting baseline pressure for all groups on pressure probe 1 and probe 2 from 0–7 cm depth. Sham and Q41D4 training group data output overlap on pressure probe 1, indicating similar higher resting baseline pressures. In contrast, Sham group pressure data on probe 2 was not significantly higher than the Quad, Q4NT4, or Q41D4 groups at 2, 3, 4, and 5 cm, as shown for the pressure disparity and improved pressure axes. NT, non-trained; Quad or Q, quadrupedal stepping. Color image is available online.
ARM testing—giant contractions
GCs were first quantified and the threshold defined using the Sham group recordings. All contraction amplitude values above 10 mm Hg from shams were included in the analysis. From these data, amplitude ranges were normally distributed and calculated (minimum, maximum, range, mean, quarterly percentile). Any amplitude value at or above the pre-selected 75% percentile was used as the amplitude threshold value for a GC. A GC
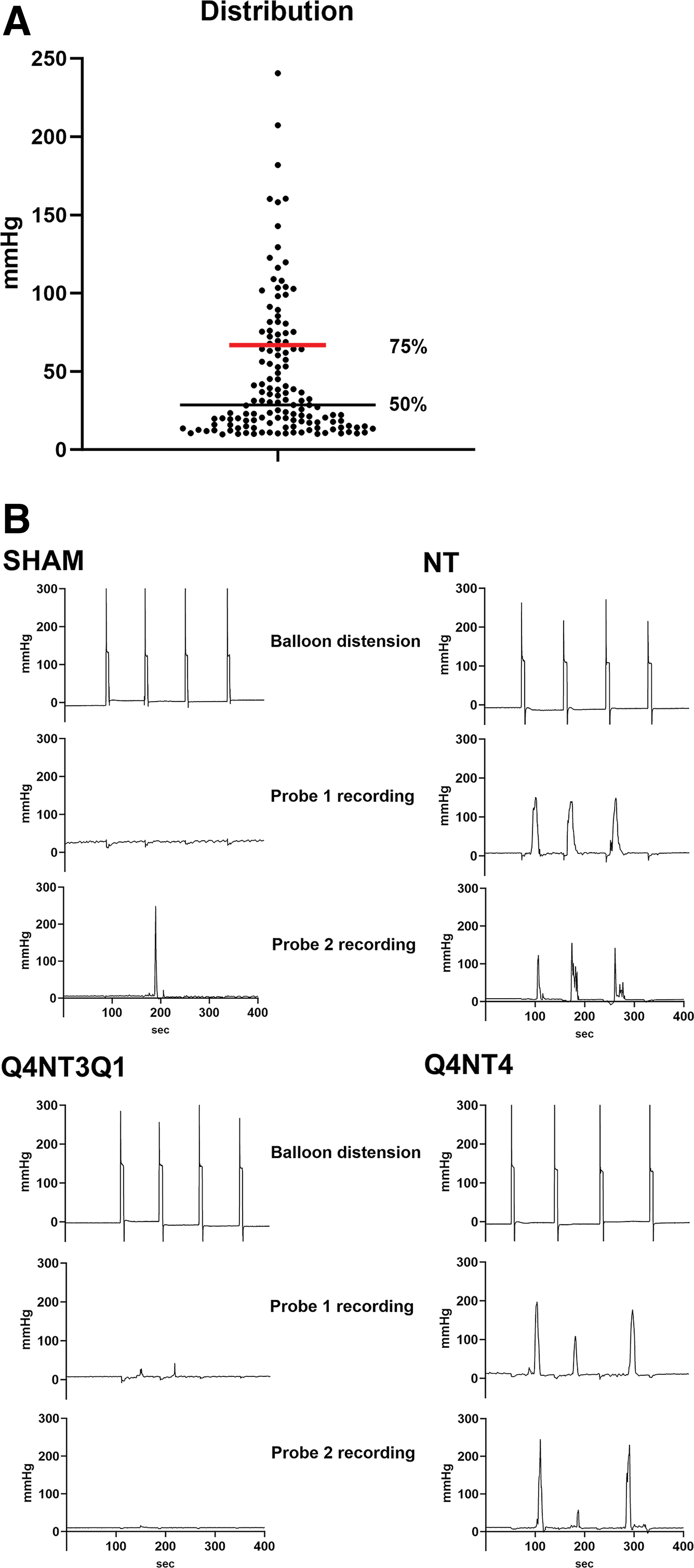
GC recordings.
Most (93%) GCs for all groups for probe 1 and probe 2 were found between 2 cm and 5 cm, thus representing a “hotspot” for elevated activity, an area approximating the rectum and distal colon regions. The results from the Chi-square test for all groups within the hotspot, regardless of the probe, showed a statistically significant (*p = 0.015) training effect for GC frequency (Table 3; for sum based on n values). Note that training for the Q4NT3Q1 group, as illustrated in Figure 7B, reduced the incidence of GCs to sham levels, and both Quad and Q4NT4 group GCs were significantly lower than NT animals. These findings are consistent with baseline pressure data where higher tone in shams necessitates fewer GCs and lower tone post-SCI requires the presence of more GCs for movement of contents.
Giant Contraction Frequency by Anorectal Location
Significantly lower than NT, Quad, Q4NT4, and Q41D4 groups (p = 0.015).
NT, non-trained; Quad or Q, quadrupedal stepping.
Discussion
Our previously published study confirmed that utilizing ARM procedures in pre-clinical animal research highlighted bowel dysfunction in a rodent SCI contusion model (pressure/tone, contraction frequency, EAS hyper-reflexia). Further, that data discussed the occurrence and amplitude of GCs and potential mechanisms and described functional fecal output, colonic motility, and possible GI distress. Data from the current group of experiments demonstrate the beneficial impact of ABT relative to baseline rectal dynamics, particularly in the groups having intermittent days of weekly training versus daily or no training. Also observed, per our previously published studies, were computer-generated injury parameters, lesion-level tissue sparing percentages, and BBB locomotor scores consistent with the intended moderate-severe contusion, as described elsewhere. 31 –34,42
Fecal output assessments (home cage, metabolic cage) indicated a significant increase in fecal pellet excretion during the acute/sub-acute injury period (0–7 days post-injury) for all injured animals. Additionally, all SCI groups indicated a significant increase in food intake during the same period. Fecal pellet wet weight has been previously demonstrated to change in composition post-SCI over the course of the recovery period and was again observed in the present study. 31 Briefly, over time fecal pellets become larger with greater mass weight and lower daily total output, suggesting some degree of slower colonic motility and constipation, as observed in human studies after SCI. The mean transit time for stool through the colon in humans with SCI is significantly longer than that observed for normal adults. 1,2 Larger fecal pellets are indicative of slower intestinal activity or a hypotonic bowel. 21 Animal studies after thoracic cord transection and loss of supra-lesional input and facilitation to the bowel have shown reduced transit and decreased colonic motility. 28 Over the course of the recovery period and as ABT group training diverged, fecal output data indicated a significant shift relative to sham animals. During this period, Q41D4 group data did not change due to a reduction in ABT from 5 days to 1 day a week, maintaining a significant correlation with sham functional outputs throughout the study.
EAS EMG results indicate sphincter muscle hyper-reflexia in injured rats consistent with previous studies 47,48 and published data. 31 Maximum EAS amplitude and latency of contraction were significantly increased. Cumulatively, the EAS had a delayed yet elevated response post-SCI. The duration values for EAS activity trended lower, but were not significant, consistent with EAS hyper-reflexia data 6 weeks after recovery following SCI in rats, which found duration to be not significantly different from sham animals. 48 At the end of the training period, Q41D4 and Q4NT3Q1 ABT group measures of baseline EAS latency and amplitude data, respectively, were comparable to sham levels, indicative of significant functional improvement.
Chronic SCI impacts the descending inhibitory circuitry and induces neuroplasticity, resulting in defecatory dysfunction and hyperactive reflexes such as those observed with colonic motility and the EAS in the present study. Pudendal motoneurons innervating the sphincters (anal and urethral), located in the dorsomedial and dorsolateral nuclei of the ventral horn (Onuf's nucleus) are known to display evidence of synaptic plasticity over time following SCI. 47,48 Bowel function is regulated by both spinal and vagal nerve circuitries and supraspinal input to the lumbosacral spinal cord from the caudal nucleus raphe obscurus (nRO) to cells in the intermediolateral (IML) cell column of the thoracic cord. 49,50 Tracing studies have identified important medullary neuron projections to the lumbosacral spinal cord such as the IML and the dorsomedial nucleus (DM). 51 –53 nRO activation through electrical stimulation, via upregulation of serotonin (5-HT) or thyrotropin-releasing hormone neurotransmitters, has been implicated in the inhibition of anorectal activity. 48 5-HT is known to regulate spinal cord reflex function, 54 –56 and 5-HT fibers have been demonstrated as a source of descending input to pudendal motoneurons, impacting functional recovery post-SCI through serotonergic sprouting. 48,54 Spared/residual serotonergic fibers may be present in the lateral margins of the lesion and thus present in the lumbosacral area. 48
Improvements in colonic motility and EAS hyper-reflexivity for Q41D4 and Q4NT3Q1 ABT groups as demonstrated in the present study may therefore have benefited from improved descending serotonergic control and serotonergic reinnervation of EAS motoneurons over the course of the recovery period. Future studies will examine these possible underlying mechanisms.
Uncoordinated defecation, constipation, and fecal incontinence are indicative of frequently reported symptoms of colorectal dysfunction following SCI. The GI system maintains control through a complex interaction between autonomic and somatic innervation of the intrinsic enteric nervous system, which has two main plexuses, the myenteric (Auerbach) plexus, and the submucosal (Meissner) plexus, which together coordinate segmental motility and some peristaltic movement, 57 with global colonic movements controlled by spinal-cord-mediated reflexes via pelvic nerves. After SCI, uncoordinated segmental peristalsis has been observed in humans with spinal cord lesions above the level of the conus medullaris or lumbar (L1, L2) level. Baseline colonic activity is described as spastic (rectum), with diminished resting sphincter tone and disordered evacuation. 12
In addition to the loss of supraspinal control of somatic and autonomic circuitry of the spinal cord, recent evidence has emerged that considers enteric neuromuscular remodeling of colonic tissue. Collagen deposition and reduced myenteric neuronal density within the longitudinal muscle layer have been observed in both humans 58 and rats with chronic SCI. 29 The role of cholinergic-mediated impairment 59 and neurokinin receptor modulation 60 of colonic smooth muscle contractions following SCI holds promise for improving understanding of enteric and spinal neuron remodeling and functional reflex recovery following SCI. 29 In humans, there is evidence that different exercise protocols can induce distinct neuroplasticity processes, altering the two-way relationship between the enteric nervous system and the central nervous system or gut–brain axis, influencing serotonergic neurotransmission and change in gut microbiome diversity. 61 In athletes, a correlation between physical stress during exercise and GI microbiota composition has been observed, 62 and high-intensity exercise has been shown to negatively impact colonic motility, peristaltic activity, and sphincter tone and relaxation. 63 Thus, we postulate that benefits associated with intermittent versus more frequent ABT in the current study may achieve a more effective balance that positively influences the interactions between the enteric and autonomic nervous systems.
GCs are typically accompanied by an increase in colonic tone that is thought to occlude the lumen and allow for effective propagation over long distances producing mass movement and evacuation. 15 In the present study, injured animals differed in baseline rectal function with reduced tone and higher GC incidence, suggesting an increase in disordered segmental contractions contributing to colorectal dysfunction. The Q4NT3Q1 ABT group was particularly effective at significantly reducing GCs, and the Q41D4 ABT group was effective at significantly increasing resting baseline tonal pressure. Note that SCI contusions at spinal level T3 (300 kDyne, 15-sec dwell) in rats have been shown to significantly reduce giant migrating contraction amplitude in the distal colon after 3 days, but not at 3 weeks. 29
Although the present study did not determine the same significant reduction in GC incidence chronically following SCI, it is possible methodological differences between studies (fasting overnight before euthanasia, transducer location/placement, balloon inflation) and location/severity (T3/T9, 15-sec/1-sec dwell) could account for the observed difference. Of potential relevance is the well-established role of acetylcholine, a neurotransmitter acting as a primary excitatory mediator for colonic smooth muscle contractile activity. Decreased cholinergic responses have been observed in ex vivo colon muscle after SCI 59 and forceful propulsive contractions such as high-amplitude propagating contractions were not detected, only bursts of low-amplitude pressure waves. 64 Note that the GC results in the current study for SCI-injured animals mimic irritable bowel syndrome observations in humans, specifically, the increase in high-amplitude propagating contractions 65 and vigorous clusters or bursts of small bowel contractile activity. 66
As with the functional improvement of EAS hyper-reflexia noted in the Q41D4 and Q4NT3Q1 ABT groups, the same two training regimes improved tone and GC frequency, respectively, suggesting a common mechanism. As it is known that exogenous 5-HT inhibits acetylcholine release and 5-HT antagonists stimulate release, 67 it is possible that serotonergic reinnervation and improved descending serotonergic control may be impacted by intermittent ABT and inhibit cholinergic excitatory input. Damage to 5-HT fibers following SCI has been implicated in promoting over-excitation that contributes to autonomic dysreflexia, pain, and spasticity, as has the inhibitory neural excitation capacity of 5-HT. 56 Therefore, 5-HT mediated myenteric neurons, and neuronal nitric oxide synthase (nNOS)-positive enteric inhibitory neurons 68 may be a contributing mechanism for functional improvement following intermittent ABT. nNOS neurons are susceptible to disruption and loss following SCI. 69,70 Myenteric neuron density loss observed in the rat colon after SCI 29 may alter both cholinergic excitatory input and 5-HT mediated transmission to myenteric neurons in the distal colon. 56 Cumulatively, the complex interaction between these two neurotransmitters and their role in rat enteric nervous system control of colonic muscle movement and peristalsis warrants further investigation.
Interpreting distal colon GC data and enteric nervous system innervation as it relates to human and rat phenotypes merits caution. Vagal parasympathetic innervation of the colon is reduced at the splenic flexure in humans but projections to the distal colon are known to occur in rats. 71 Healthy human manometric recording data are characterized by low amplitude, non-propagating segmental contractions, infrequent peristalsis, and the absence of regular cyclic colonic motility. 72 Additionally, the role of pelvic floor puborectalis muscle innervation by the pudendal nerve and potential dysfunction associated with the EAS and fecal incontinence due to constrictive abnormalities may influence human functional outcomes, 73 but not rat data. A future area of interest for further study of rat colon peristalsis and the role of GC and baseline tonal pressure should seek to categorize contractions by type, for example, the role and identification of rhythmic phasic contractions crucial to post-prandial motility function as opposed to ultra-propulsive contractions such as migrating and retrograde GCs, and tonic contractions. The latter generates sustained tonic contraction via circular smooth muscle cells, such as those found in the IAS, aiding in lumen occlusion and improved colonic motility via activation of enteric inhibitory neurons. 74
Conclusions
Based on the results of this study, it is evident that the ARM model can detect changes in tonal pressure, GCs, and EAS hyper-reflexia in an anesthetized rat after SCI and that intermittent ABT significantly improves bowel dysfunction. The manometry data are broadly consistent with previous literature in humans (reduced colonic motility and spastic rectum) and therefore have great value for assessing mechanisms (propulsive peristalsis following cholinergic excitatory input and 5-HT mediation of myenteric neurons) and testing possible treatments. Additionally, studies utilizing ARM in a rat SCI model are relatively inexpensive, benefit from homogeneity in injury parameters, and the collection of output measurements from metabolic/home cage significantly furthers functional understanding of colonic motility.
Transparency, Rigor, and Reproducibility Summary
The rat is a widely used model both in the SCI and bowel fields due to the many similar injury responses and colonic functional features to humans, albeit quadrupedal versus bipedal and on a smaller size scale. Additionally, (1) a substantial database exists on SCI rat models; (2) bowel function can be easily monitored and measured with functional output and anorectal manometry, a standard for clinical assessments; and (3) the injured rat demonstrates similar bowel signs to those of individuals with SCI.
A statistical power analysis was performed for sample size estimation based on data from our previous studies evaluating functional output of the bowel (weekly fecal measurements) and terminal ARM measurement with external anal sphincter EMG under urethane anesthesia. A sample size of at least 8 per group was estimated to detect an effect size at a significance level of α = 0.05. Additional animals allow for a 20% potential attrition rate. In total, 66 rats were utilized in the study to perform a well-established manometry procedure to discern the effect of LT after SCI on bowel function. All data analyses were confirmed by an independent statistician. The study was limited because more precise fecal weight analyses such as ash weight/longer drying protocols could not be performed due to the volume of samples generated by animal collection frequencies. Other factors that need further study are bowel contractions by type, quantitative morphology of colonic tissue, and refinement of intermittent LT.
Footnotes
Acknowledgments
We thank James Armstrong for technical assistance, Christine Armstrong for surgical assistance, and Dr. Robert Hoey for experimental input and guidance.
Authors' Contributions
The authors contributed as follows. JDF: investigation (lead), writing—original draft (lead), formal analysis (equal), review and editing (equal); DMA: investigation (supporting), formal analysis (equal), writing—review and editing (equal), DAB: formal analysis (equal), writing—review and editing (equal); CHH: conceptualization (lead), writing—original draft (supporting), writing—review and editing (equal).
Funding Information
Funding support for this work was provided by the Department of Defense (Award #W81XWH1810675) and the Kentucky Spinal Cord Head Injury Research Trust (KSCHIRT, Grant #17-5).
Author Disclosure Statement
No competing financial interests exist.