
Abstract
The objective of this study was to clarify the occurrence, phenomenology, and risk factors for novel psychiatric disorder (NPD) in the first 12 months after mild traumatic brain injury (mTBI) and orthopedic injury (OI). Children aged 8–15 years with mTBI (n = 220) and with OI but no TBI (n = 110) from consecutive admissions to Rady Children’s Hospital Emergency Department were followed prospectively at baseline, 3-, 6-, and 12-month postinjury with semi-structured psychiatric interviews to document the presence of NPDs that developed in each participant. Preinjury child variables (academic, adaptive, and cognitive function, and psychiatric disorder), preinjury family variables (family function, family psychiatric history, and socioeconomic status), and injury severity were assessed and analyzed as potential confounders and predictors of NPD that occurred at any assessment in the 12 months after injury. This study extends our analyses of counts of NPD that were limited to the first 3 months of follow-up published in this journal. In multipredictor analyses adjusted for potential confounders, NPD risk increased over time in children with OI: 6-month versus 3-month adjusted odds ratio (aOR) = 17.766, CI95 (1.712, 184.376), p = 0.020; 12-month versus 3-month aOR = 21.165, CI95 (1.481, 302.473), p = 0.020, but not in the mTBI arm, corresponding to a significant group-by-time interaction: adjusted ratio of ORs for mTBI versus OI at 6-month versus 3-month aROR = 0.029, CI95 (0.002, 0.411), p = 0.012, and at 12-month versus 3-month aROR = 0.024, CI95 (0.001, 0.496), p = 0.012. Higher NPD risk was associated in unadjusted analyses with preinjury lifetime psychiatric disorder (OR = 8.995, CI95 [1.935, 41.802], p = 0.003) and poorer preinjury family function (OR = 0.383, CI95 [0.171, 0.861], p = 0.014), and in adjusted analyses with poorer preinjury family function, adjusted OR = 0.491, CI95 [0.243, 0.989], p = 0.047, and with preinjury lifetime psychiatric disorder (OR = 5.081, CI95 [0.997, 25.901], p = 0.050). These findings demonstrate that when considering the entire first postinjury year, mild injury to the brain and OI had similar effects on psychiatric outcome, but the onset of deleterious effects was earlier in the mTBI group. NPD in the first year after mTBI and OI is predicted primarily by preinjury family function.
Introduction
Mild traumatic brain injury (mTBI) is an important public health problem in the United States. 1 Children with severe TBI are at increased risk for postinjury new-onset psychiatric disorder referred to as novel psychiatric disorder (NPD). 2 –6 However, studies of children with mTBI have methodological problems resulting in conflicting findings that generate controversy. There are no psychiatric interview studies of pediatric mTBI beyond a 3-month postinjury follow-up (of the same cohort investigated in this article) 7 that are free of problems related to the definition of mTBI, outcome measurements, lack of longitudinal design, control group selection, sample size, selection bias, or assessment of injury and psychosocial risk factors. 8
Authoritative reviews of behavioral outcomes of mTBI point to relatively benign consequences in well-designed studies. 9,10 However, these conclusions are challenged by findings of two large prospective studies of mTBI. 11,12 One study involved a birth cohort, 12 and the other study involved surveillance of computerized medical information of children consecutively treated for mTBI. 11 Both studies found that youth with mTBI had significantly more new-onset behavioral symptoms than controls. The main limitations of these studies include that the measure of psychiatric outcome was not generated from standardized psychiatric interviews, and there were no control groups of injured children. 13,14 The current analyses aim to elucidate behavioral outcomes in child and adolescent mTBI with a comprehensive psychiatric investigation utilizing standardized psychiatric interviews and a control group to overcome the methodological problems that plagued earlier studies. Our present investigation extends our previous analyses, 7 which were limited to the first 3-month postinjury on the same cohort, to encompass the entire first year postinjury.
Our study is styled after Yeates et al. 15 –18 who focused on postconcussion symptoms (PCS). “Post-concussional disorder” was significantly more common in a group with mTBI versus an orthopedic injury (OI) control group 2 weeks postinjury (51% vs. 30%), but not after that in the first postinjury year (19–27% vs. 19–21%). 19 We reported only 3-month postinjury findings that the number of NPDs was greater in mTBI versus OI, and in children with preinjury lifetime psychiatric disorder, high family psychiatric history ratings, and lower socioeconomic status. 7
If mTBI is not the primary factor that influences behavioral outcomes beyond the first weeks to months postinjury, it is imperative to determine the role of variables not attributable to injury to the brain. 20 Additional analyses from the study led by Yeates revealed that injury characteristics predicted PCS in the first months after mTBI but showed a decreasing contribution over time. In contrast, noninjury factors, such as demographics, preinjury child symptoms, and family variables, were more consistently associated with persistent PCS. 21 The mTBI literature regarding preinjury child and family factors predictive of NPD is restricted to studies of consecutively hospitalized children, that is, children with more serious injuries than the present cohort. In those studies, NPD was predicted by preinjury lifetime psychiatric disorder in children with mild to moderate TBI. 2,22,23 Other preinjury predictors of NPD associated with mTBI included psychosocial adversity, socioeconomic status, adaptive function, estimated preinjury reading, and estimated preinjury academic function. 24 –26
The major objective of this study was to clarify the occurrence, phenomenology, and risk factors for NPD in the first 12 months after mTBI. This work extends our investigation of NPD in this cohort from analyses covering the first 3-month postinjury 7 to include longitudinal analyses of the pattern over the entire first year postinjury. The use of an OI group controlled for variables that predispose children to accidents, as well as controlled for the psychological trauma associated with an injury and related treatments. Based on the above-reviewed literature, our first hypothesis was that NPD in children would occur with significantly higher frequency in children with mTBI versus comparable OI controls in the first 3-month postinjury, but not thereafter. The second hypothesis was that the frequency of NPD in children in the first 12-month postinjury would be predicted by child variables (lower preinjury child adaptive function, lower preinjury cognitive function, lower preinjury academic function, and presence of preinjury lifetime psychiatric disorders) and preinjury family variables (lower preinjury family function, more intense family psychiatric history, and lower socioeconomic status) in children with mTBI and OI.
Methods
Methods detailed here have been described in this journal in a study that incorporated only the preinjury function, injury characteristics, and 3-month postinjury function outcome assessments from the same cohort of participants. 7 Additional specifics regarding methods beyond the 3-month outcome assessments are provided here. This prospective, longitudinal, parallel-arms observational study enrolled 220 children aged 8–15 years consecutively treated at an emergency department (ED) for mTBI and 110 children with mild OI from patients seen at the same ED matched at the group level by sex and age. The University of California, San Diego institutional review board approved the study. Written informed consent was obtained from parents, and children provided written consent or assent, depending on their age. To ensure that children with “a bump to the head” but with no brain trauma were excluded, the mTBI group included children only if they incurred a closed head injury that resulted in an observed loss of consciousness, a Glasgow Coma Scale (GCS) 27 score of 13 or 14 or if GCS score was 15, there had to be at least two concussion symptoms as reported by the ED medical staff (e.g., vomiting, nausea, headache, diplopia, dizziness, post-traumatic amnesia that persisted from the time of the injury to presentation in the ED, transient neurological deficits). Hospitalization was not an automatic exclusion factor. However, children with delayed neurological deterioration (e.g., GCS <13) were excluded. Children were excluded if loss of consciousness was >30 min or they had a GCS score of <13. The GCS was obtained from the electronic medical record.
Other exclusion criteria for the mTBI group included the following: (1) associated severe injury documented with the Abbreviated Injury Scale (AIS) 28 score >3; (2) associated injury likely to interfere with cognitive testing (e.g., dominant upper limb injury); (3) hypotension, hypoxia, or shock associated with the injury; (4) drug, alcohol ingestion, or child abuse involved with the injury; (5) documented history of previous TBI that met the above criteria for at least mTBI; (6) preinjury schizophrenia, autism spectrum disorder, neurological disorder, or intellectual deficiency; (7) any medical contraindication to MRI; (8) injury requiring neurosurgical intervention; or (9) self-reported illegal immigrant status.
Inclusion criteria for children with OI were the presence of lower or upper limb fractures associated with AIS scores of 3 or less. Exclusion criteria included (1) injury to the head or TBI and (2) exclusion criteria 1–9 listed above for the mTBI group.
The youth’s preinjury function was assessed retrospectively at baseline (mean = 17.7 ± SD = 5.8 days postinjury), and postinjury outcome was assessed at 3-month (mean = 103.1 ± SD = 16.9 days), 6-month (mean = 197.4 ± SD = 18.0 days), and 12-month (mean = 380.4 ± SD = 20.1 days) postinjury.
Assessment of preinjury child function
Lifetime preinjury psychiatric status
Lifetime preinjury psychiatric disorder was assessed with the Schedule for Affective Disorders and Schizophrenia for School-Aged Children: Present and Lifetime Version (K-SADS-PL) Interview. 29 The KSADS-PL has high interrater reliability and validity. 29 The Neuropsychiatric Rating Schedule (NPRS) 30 interview was administered to document the DSM-IV diagnosis, Personality change due to TBI. 31 The NPRS reliably and validly identifies subtypes and symptoms of personality change due to TBI. 6
The Teacher’s Report Form 32 (TRF) was used to assist the psychiatric interviewer in reaching a “best-estimate” diagnosis. 33 The interviewers discussed their diagnoses by presenting all cases to the first author, a board-certified child and adolescent psychiatrist, who was blind to group affiliation.
Preinjury adaptive behavior function
The adaptive behavior composite was measured using the Vineland Adaptive Behavior Scales (Vineland II) interview with the parent. 34
Preinjury intellectual and academic function
The Wechsler Abbreviated Scale of Intelligence (WASI-II) 35 Matrix Reasoning and Vocabulary subtests were administered at baseline to estimate the preinjury Full-Scale IQ standard score. The Wide Range Achievement Test–Fourth Edition (WRAT-4), 36 which assesses sentence comprehension, calculation skills, word recognition, and spelling, was administered at baseline. Standard scores of calculation skills and sentence comprehension were used in the analyses. Studies have demonstrated that these measures of “crystallized ability” are relatively insensitive to the effects of mTBI when measured shortly after the injury. 17,37
Assessment of preinjury family status
Family function
The McMaster Structured Interview of Family Functioning (McSIFF) 38 was administered by research assistants with household family members at baseline to measure preinjury family function retrospectively. The interview is a tool used to derive scores on a rating scale entitled the Clinical Rating Scale (CRS). 38 Preinjury family function, documented by the McSIFF, is a consistent predictor of NPD after TBI. 2 The global CRS score is a reliable and valid method of family assessment. 38,39 The General Functioning Scale of the McMaster Family Assessment Device (FAD), 40 which was completed by the injured child’s primary caretaker at baseline, is a valid and reliable 12-item rating scale that provides an overall measure of preinjury family functioning 41 that was used in the analyses.
Family psychiatric history
The Family History Research Diagnostic Criteria, 42 modified to DSM-IV-TR criteria, is a semi-structured interview with the parent that assesses for psychiatric diagnoses in first-degree family members. The analyses used the overall family psychiatric history ratings on a 4-point scale: 0 = no psychiatric disorder; 1 = at least one family member met criteria for a psychiatric disorder but did not receive treatment; 2 = a family member met criteria for a psychiatric disorder and had outpatient treatment or was arrested for antisocial behavior; and 3 = a family member met criteria for a psychiatric disorder and had psychiatric inpatient hospitalization or was incarcerated. 2 Participants were documented as having either low (scores of 0–1) or high (scores of 2–3) intensity family psychiatric history for the analyses.
Socioeconomic status
Socioeconomic status (SES), expressed as a z-score, was determined using a composite of maternal education and median income for the census tract of the family’s residence. The composite was derived by averaging the sample z-scores of the two variables. This composite score functions well as a measure of SES in studies of TBI. 43
Assessment of injury severity and brain imaging
The Injury Severity Score (ISS) from the Abbreviated Injury Scale (AIS) was calculated from electronic medical record data. 28 The ISS is the sum of the squares of the highest AIS code in each of the three most severely injured ISS body regions. A research MRI was conducted at the 6-month follow-up. A board-certified neuroradiologist (J.R.H.), blind to the participant’s history, independently reviewed each scan with specific reference to definite trauma-related features such as focal encephalomalacia and hemosiderin deposition. 44 White matter hyperintensities and/or dilated Virchow–Robin spaces were not considered to be evidence of definite trauma-related abnormalities. 44
Postinjury psychiatric outcome
The K-SADS-PL, NPRS, and TRF were repeated at 3, 6, and 12 months. The interviewer generated “best-estimate” clinically significant psychiatric diagnoses by integrating the information from these measures. 33 Consistent with previous studies, 2,5 an NPD diagnosis was given in two circumstances: First, this could occur in a child with no preinjury lifetime psychiatric disorder who subsequently develops a psychiatric disorder. Second, this could occur in a child with a preinjury lifetime psychiatric disorder who develops a different psychiatric disorder; for example, a child with a preinjury lifetime history of major depression who develops oppositional defiant disorder following the injury would receive the classification, but would not if only a new episode of major depression developed. Duration criteria for psychiatric disorders, except for bipolar disorder and major depression, were waived to examine the phenomenology of emerging postinjury disorders. Similarly, consistent with our previous work, for attention-deficit/hyperactivity disorder (ADHD), the age of onset criterion was waived to study the phenomenology of this specific NPD. 2
The interviewers attempted to remain blind to group membership (mTBI vs. OI control), although at baseline, this was often difficult because of physical residuals of TBI and OI. However, the baseline psychiatric assessment only assessed preinjury psychiatric status, which was not the outcome of interest. Therefore, the study design ensured that the interviewer who conducted the baseline assessment for a specific participant did not conduct postinjury psychiatric assessments for that participant. Thus, the psychiatric interviewer who conducted the 3-, 6-, and 12-month assessments was blind to injury group. The interviewers presented all cases to the first author, who was blind to group affiliation.
Interrater reliability for psychiatric diagnoses was conducted based on 12 video-recorded interviews (Supplementary Data). Consent was requested for video recording of the psychiatric interviews from all research participants and their guardians. The “best-estimate” current and past ratings required integration by the clinician of the child’s and parent’s video-recorded interview, teacher’s input when available, and clinical judgment of the child’s and parent’s reliability and child’s mental status. Agreement regarding psychiatric diagnosis was perfect in 10/12 (83%) cases, including agreement for all specific current and past diagnoses or absence of a diagnosis in a child. We conducted a Kappa analysis of interrater reliability for these categorical diagnoses. There was agreement between raters in 26/29 specific diagnostic data points and disagreement in 3/29, with Kappa = 0.80, that is, substantial agreement.
Statistical analysis
The eligible patients with mTBI who presented to the ED but who did not enroll in the study (n = 741) were compared with the patients with mTBI who did enroll (n = 220) with respect to age and GCS score using independent sample t-tests and with respect to sex using Pearson’s chi-squared test. Instead of Pearson’s test, Fisher’s exact test was used when the expected counts were ≤5 in any of the crosstabulation cells.
To determine the effect of mTBI on NPD in the first year postinjury (Hypothesis 1), the occurrence of NPD for each child was recorded at the 3-, 6-, and 12-month visits and was compared between the mTBI and OI groups using longitudinal mixed-effects logistic regression models with a child-specific random effect in unadjusted and adjusted analyses. The unadjusted analyses included group (mTBI vs. OI), visit, and their interaction. The adjusted analyses further accounted for potential confounders, which included demographics: age, sex, and race; preinjury child function: lifetime preinjury psychiatric disorder, WASI-II Full-Scale IQ, WRAT-4 Sentence Comprehension and Calculation Skills, and Vineland Adaptive Behavior composite; preinjury family status: family function (CRS and FAD), family psychiatric history, and SES; and injury status: ISS. Among these potential confounders, those that were significant at a screening p < 0.15 from individual-covariate models (described below) were included in the starting multipredictor model and were subject to backward model selection with a p < 0.15 threshold (adjusted analysis). The statistical tests and 95% confidence intervals (CI95) were based on the likelihood ratio test. Backward model selection with a loose threshold of 0.15–0.20 is suggested in regression models for determining causal effects in the presence of confounding. 45
Individual-covariate models investigated the association of each of the child or family characteristics listed above with the risk of NPD using longitudinal mixed-effects logistic regression models with child-specific random intercepts, which included as predictors the individual covariate, in addition to group, visit, and group-by-time interaction.
The effects of predictors are reported in terms of the odds ratio (OR) of NPD between any two groups under comparison, adjusted for the other predictors in the model. The ORs are conditional on the individual-level random effects and have an individual-level interpretation. Visit-by-group interaction comparing the change over time (6-month vs. 3-month and 12-month vs. 3-month) in the risk of NPD between the mTBI and OI groups was quantified via ratios of odds ratios. When comparisons were made at each visit, the p-values and CI95’s were Bonferroni-corrected.
To determine a multipredictor model for the NPD at any point in the first 12-month postinjury (Hypothesis 2), we similarly fit a multipredictor mixed-effects logistic regression model, where predictors with p < 0.15 in individual-covariate analyses were included in the starting model and the model was reduced using backward model selection with a threshold of p < 0.15. This is analogous to the analysis determining the effect of mTBI, except that mTBI exposure was also subject to model selection. 45
Mixed-effects longitudinal models, like those used here, provide unbiased inference in the presence of dropout, even with dropout that depends on treatment arm or other individual characteristics that are included in the model (dropout at random). All analyses used R version 4.2.2, and regression models were implemented with the package lme4 version 1.1-31.
Results
Representativeness of enrolled mTBI participants (see Fig. 1)
The enrolled group of children with mTBI (n = 220) was compared with those with mTBI who did not enroll (n = 741). The mean (SD) age of the enrolled group (12.3 ± 2.1 years) was significantly higher than the nonenrolled group (11.7 ± 2.2 years) (p = 0.0001). The enrolled mTBI and nonenrolled mTBI groups were not significantly different with regard to sex (145/220; 66.0% vs. 521/741; 70.3% males, respectively; p = 0.21), nor with respect to severity of injury documented by GCS scores (14.95 ± 0.21 vs. 14.97 ± 0.20, respectively; p = 0.44).
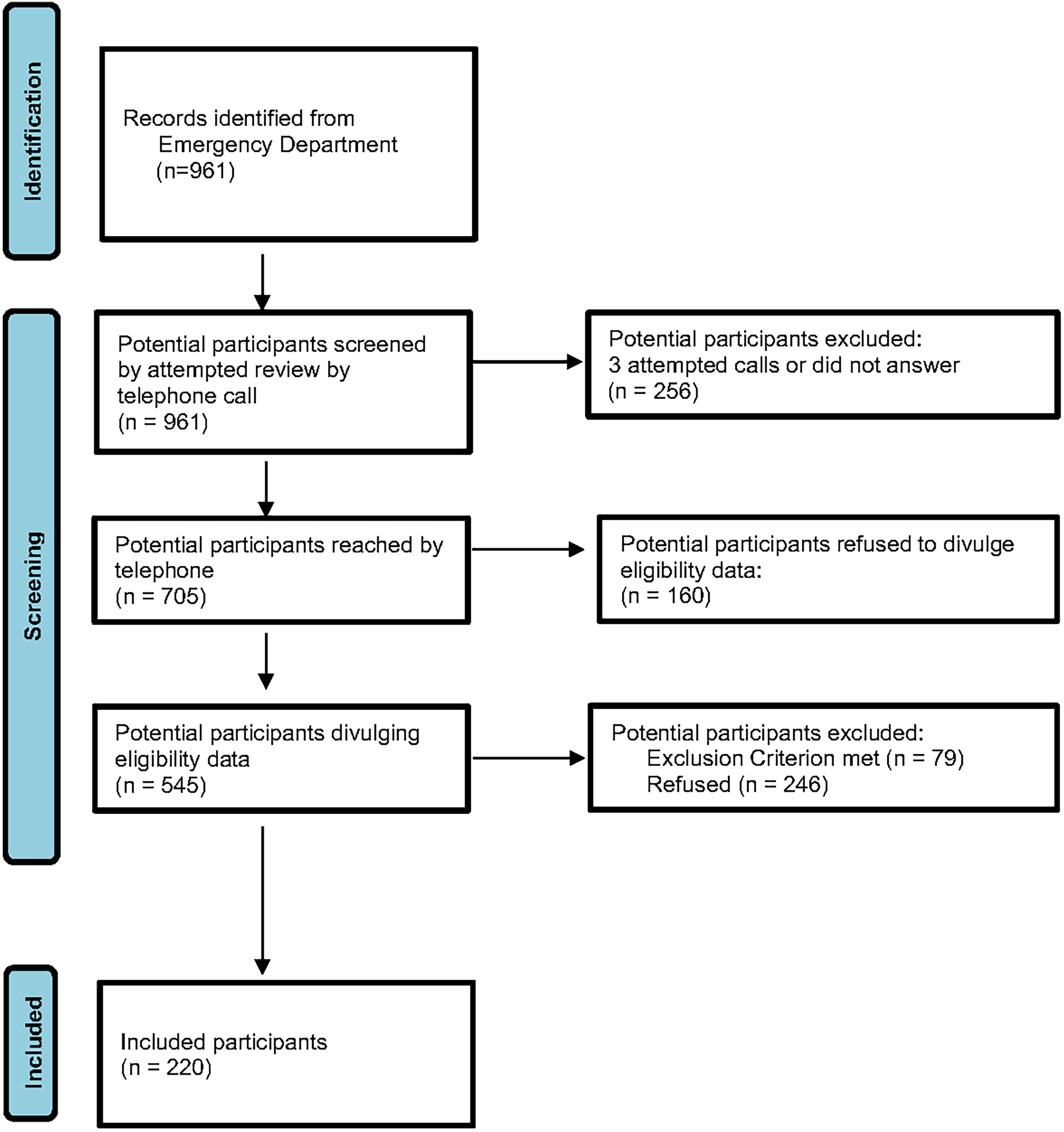
Identification of children with mild traumatic brain injury.
Baseline characteristics
Table 1 shows that our efforts to match the OI group (n = 110) to the mTBI group (n = 220) by sex and age were effective. Furthermore, there were no significant group differences in preinjury child variables (ethnicity, adaptive function, lifetime and current psychiatric disorder, academic function, IQ) and preinjury family variables (family function, family psychiatric history, socioeconomic status). In comparison with the OI group, the mTBI group had a significantly lower percentage of enrolled White (65.0% vs. 79.1%) versus minority (35.0% vs. 20.9%) race participants (Pearson’s chi-squared test p value = 0.011). The ISS was significantly greater in the enrolled OI group versus the enrolled mTBI group (3.98 ± 1.00 vs. 2.70 ± 2.46, respectively; df = 328; p < 0.001). A significant difference in the cause of injury between the OI and mTBI enrolled groups (Fisher’s exact test p < 0.001) was evident. Inspection of the data found that this was related to falls in 85% of OI cases versus 55% of mTBI cases, and more mTBI cases were injured by accidentally striking or being struck by an object, accidentally striking or being struck by a person, and having a transportation-related injury. Hospitalization occurred in 25/220 (11.4%) mTBI cases and 5/110 (4.5%) OI cases. Definite trauma-related abnormal research MRI scans were noted in 6/174 (3.4%) mTBI cases and none of the OI cases. The abnormalities included one participant with encephalomalacia plus evidence of previous hemorrhage, two others with encephalomalacia alone, and three others with evidence of previous hemorrhage alone. The rates of specific preinjury lifetime psychiatric disorders in the OI and mTBI groups were similar (Table 2). The rates of all the disorders are within the ranges of epidemiological studies, except for a higher rate of ADHD. This exception is typical of cohorts of injured children. 46 Teachers’ input from the TRF was available for only 116/330 (35.2%) participants for reaching baseline “best-estimate” psychiatric diagnoses.
Baseline Demographics, Psychiatric, Adaptive, Family, Academic, Intellectual Status, Injury Severity, Cause of Injury, Hospitalization, and Abnormal Research Magnetic Resonance Imaging Scan
Specific Lifetime Preinjury Psychiatric Disorders
There were no cases of the following preinjury psychiatric disorders: panic disorder, obsessive-compulsive disorder, cyclothymia, bipolar disorder, alcohol use disorder, and drug use disorder.
Follow-up and attrition
Participation at the 3-month follow-up visit was 189/220 (85.9%) and 94/110 (85.5%) of the enrolled participants with mTBI and OI, respectively. Corresponding participation at the 6-month follow-up visit was 189/220 (85.9%) and 89/110 (80.9%), and at the 12-month follow-up visit was 172/220 (78.2%) and 85/110 (77.3%).
Novel psychiatric disorders
Table 3, subdivided into mTBI and OI sections, shows the course of every participant who developed an NPD documented at specific follow-up assessments during the first postinjury year and includes the preinjury psychiatric status of each of those children.
Novel Psychiatric Disorders in the First Postinjury Year
Provided psychotherapy alone for the adjacent diagnosis.
Provided combined psychotherapy and psychopharmacotherapy for the adjacent diagnosis; + = provided psychopharmacotherapy alone for the adjacent diagnosis. H = child was admitted to the hospital for the index injury. A = abnormal research MRI.
ADHD, attention/deficit/hyperactivity disorder; H/I, hyperactive/impulsive; MDD, major depressive disorder; NPD, novel psychiatric disorder; PC, personality change due to a general medical condition; PTSD, post-traumatic stress disorder.
During the 3-month postinjury follow-up, NPD developed in 18 children with mTBI, including four children with two NPDs and 14 children with one NPD. NPD occurred in three of the children with OI, and each of these children had a single NPD. The specific NPDs and categories of NPD are shown in Table 4. Within the mTBI group, the NPDs were ADHD (n = 7); adjustment disorder (n = 4); anxiety disorder (n = 4) that included generalized anxiety disorder, specific phobia, separation anxiety disorder, and other specified anxiety disorder; oppositional defiant disorder (n = 3); personality change due to a general medical condition (n = 3); and a tic disorder (n = 1). The NPDs in the OI group consisted of oppositional defiant disorder, adjustment disorder, and specific phobia. Teachers’ input using the TRF was available for only 100/283 (35.3%) participants for guiding “best-estimate” psychiatric diagnoses at the 3-month assessment.
Specific Novel Psychiatric Disorders at 3-, 6-, and 12-Month Postinjury
Bolded numbers indicate details of the specific novel psychiatric disorders that developed in each group. Denominators vary for novel psychiatric disorders due to the ineligibility of certain individuals for a particular novel psychiatric disorder if they already manifested that disorder before the injury.
ADHD, attention/deficit/hyperactivity disorder; GAD, generalized anxiety disorder; TBI, traumatic brain injury.
NPD at the 6-month follow-up (reflecting evidence of NPD in the 3- to 6-month postinjury interval) was evident in 13/189 (6.9%) children with mTBI, including two children with two NPDs, and 8/89 (9.0%) children with OI, and each of these children had one NPD. The specific NPDs and categories of NPD are shown in Table 4. Within the mTBI group, the specific NPDs were ADHD (n = 4), oppositional defiant disorder (n = 3), specific phobia (n = 2), generalized anxiety disorder (n = 1), other specified anxiety disorder (n = 1), other specified depressive disorder (n = 1), other specified trauma- and stressor-related disorder (n = 1), personality change due to TBI, apathetic subtype (n = 1), and adjustment disorder (n = 1). Within the OI group, the specific NPDs were adjustment disorder (n = 2), ADHD (n = 1), major depressive disorder (n = 1), specific phobia (n = 1), oppositional defiant disorder (n = 1), other specified disruptive, impulse-control, and conduct disorder (n = 1), and cannabis use disorder (n = 1). Teachers’ input using the TRF was available for only 91/278 (32.7%) participants for guiding “best-estimate” psychiatric diagnoses at the 6-month assessment.
NPD at the 12-month follow-up (reflecting evidence of NPD in the 6- to 12-month postinjury interval) was evident in 15/172 (8.7%) children with mTBI, including four children with two NPDs, and 9/85 (10.6%) children with OI, and each of these children had one NPD. The specific NPDs and categories of NPD are shown in Table 4. Within the mTBI group, the specific NPDs were ADHD (n = 3), oppositional defiant disorder (n = 2), specific phobia (n = 2), major depressive disorder (n = 2), and one each of other specified depressive disorder, other specified bipolar and related disorder, other specified anxiety disorder, generalized anxiety disorder, other specified trauma- and stressor-related disorder, adjustment disorder, conversion disorder, personality change due to TBI, affective lability subtype, Tourette’s disorder, and provisional tic disorder. Within the OI group, the specific NPDs were ADHD (n = 2), and one each of oppositional defiant disorder, other specified disruptive, impulse-control, and conduct disorder, major depressive disorder, panic disorder, specific phobia, adjustment disorder, and cannabis use disorder. Teachers’ input using the TRF was available for only 55/257 (21.4%) participants for guiding “best-estimate” psychiatric diagnoses at the 12-month assessment.
Examination of the persistence of NPD that developed within the first 3-month postinjury revealed the following (Table 3). Four of the 15 (27%) children with NPD evident in the first 3 months and who also had no missing psychiatric assessments over the first postinjury year experienced persistence of their NPD to 12-month postinjury. The corresponding phenomenon within the OI group was 2/3 (67%). The persisting NPDs were specific phobia (1 in each group), oppositional defiant disorder (1 in each group), and one each of anxiety disorder other specified and tic disorder in the mTBI group. Of particular interest is that ADHD (n = 7), the most frequent NPD in the mTBI group at the 3-month assessment, resolved in 5/5 cases with data through 12-month postinjury. There were two instances of novel ADHD that developed in each of the mTBI (2/142; 1.4%) and OI (2/74; 2.7%) groups only after the 3-month follow-up.
NPD occurred in 29/198 (14.7%) children with mTBI and 11/96 (11.5%) of children with OI who had at least one postinjury follow-up assessment. Table 3 shows that hospitalization for the index injury in the mTBI group occurred in 2/29 children with NPD and 1/11 children with OI. Only 1/29 (3.4%) of children with NPD in the mTBI group had a definite trauma-related MRI abnormality. Table 3 also shows timing and other details of participation in psychotherapy and psychopharmacotherapy in children with NPD. Of the 29 children with mTBI who developed an NPD, 7 (24%) participated in either psychotherapy alone (n = 3) or combined psychotherapy and psychopharmacotherapy (n = 4). Of the 11 children with OI who developed an NPD, 5 (45%) participated in either psychotherapy alone (n = 2), psychopharmacotherapy alone (n = 1), or combined psychotherapy and psychopharmacotherapy (n = 2).
Time effect of mTBI on novel psychiatric disorders
In multipredictor analyses adjusted for potential confounders (Table 5), mTBI had a nonsignificantly higher NPD risk than OI at the 3-month follow-up (adjusted OR [aOR]=14.347, CI95 [0.614, 334.398], p = 0.129). NPD risk increased over time in children with OI: 6 months vs. 3 months aOR = 17.766, CI95 [1.712, 184.376], p = 0.020); 12 month versus 3 months aOR = 21.165, CI95 [1.481, 302.473], p = 0.020), but not in the mTBI arm, corresponding to a significant group-by-time interaction: adjusted ratio of ORs for mTBI versus OI at 6-month versus 3-month aROR = 0.029, CI95 (0.002, 0.411), p = 0.012, and at 12-month versus 3-month aROR = 0.024, CI95 (0.001, 0.496), p = 0.012. Figure 2 suggests that at 3 months the mTBI group has a higher probability of NPD than the OI group, but not at 6 or 12 months. Longitudinal mixed-effects logistic regression, not adjusted for potential confounders, shows an overall difference between the two groups (mTBI vs. OI) over time (main effect + interaction p = 0.0289 and a significant time-by-group interaction (p = 0.0131).
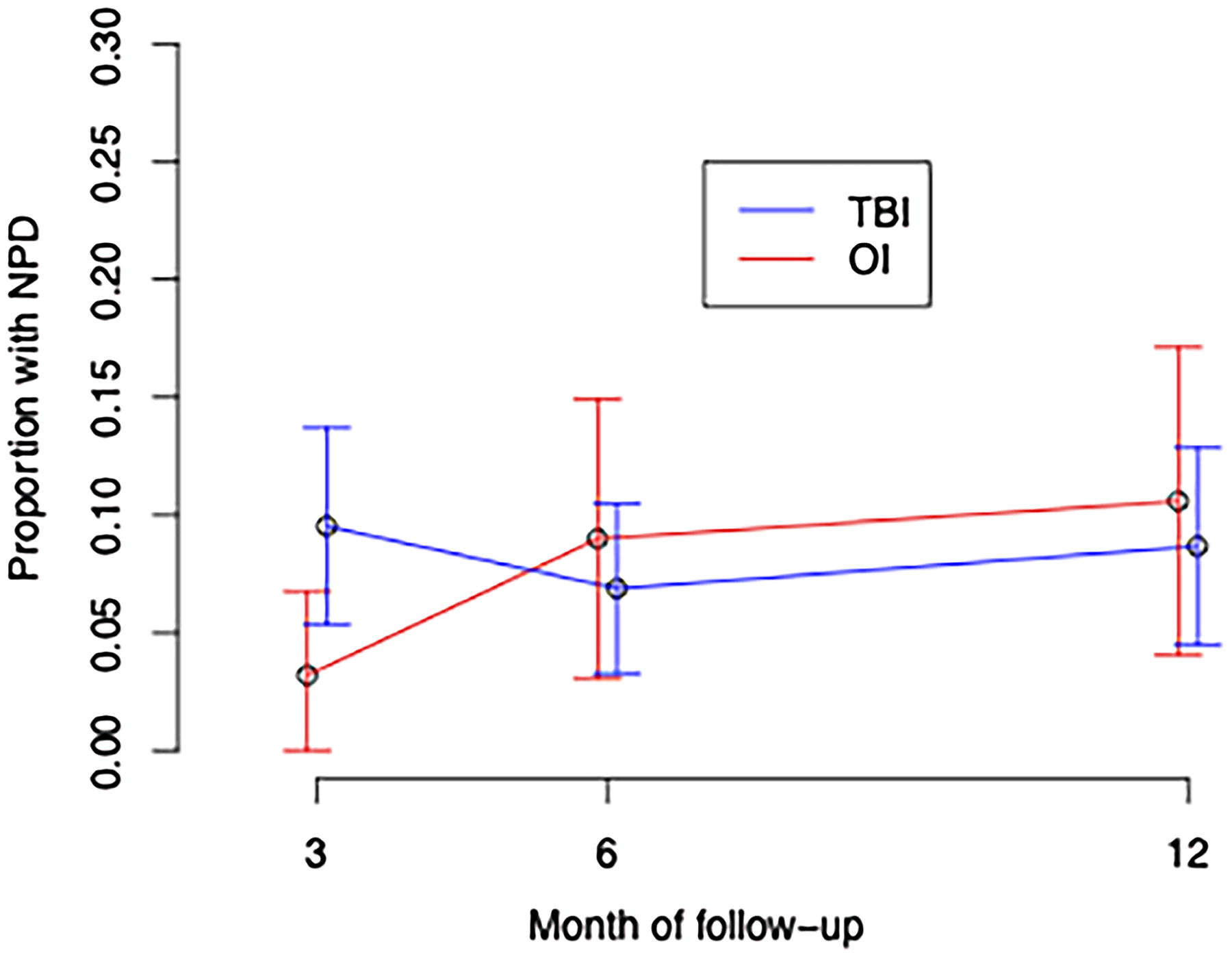
Proportion of children with novel psychiatric disorder over time.
Unadjusted and Adjusted Comparison of NPD over Time Between mTBI and OI Groups, Using Longitudinal Mixed-Effects Logistic Regression
Bolded numbers indicate p value <0.05.
mo, months; mTBI, mild traumatic brain injury; OI, orthopedic injury; vs, versus.
Effect of child and family characteristics on novel psychiatric disorders
In individual-covariate analyses (Table 6), the following factors were significantly associated with NPD occurrence at any point in the first postinjury year: Preinjury lifetime psychiatric disorder, OR = 8.995, CI95 (1.935, 41.802), p = 0.003; and preinjury family function measured with the McSIFF CRS score, OR = 0.383 per point, CI95 (0.171, 0.861), p = 0.014. Worse socioeconomic status showed a trend-level association, OR = 0.466, CI95 (0.205, 1.059), p = 0.056. The only other variable with a screening p value <0.15 was family psychiatric history (high vs. low intensity), OR = 3.184, CI95 (0.686, 14.777), p = 0.142.
Predictors of Novel Psychiatric Disorder in the First Year After Injury: Unadjusted Single-Predictor Regression Analysis and Adjusted Multipredictor Regression Analysis
The results for the prediction of Novel Psychiatric Disorder using a longitudinal mixed-effects logistic regression model are reported as odds ratios and 95% confidence intervals. Bolded numbers represent variables with p < 0.15 values in unadjusted analyses, which were included in the starting model for multipredictor analyses and variables with p < 0.05 in adjusted analyses.
CI, confidence interval; WASI-II, Wechsler Abbreviated Scale of Intelligence Second Edition; WRAT-4, Wide Range Achievement Test–4th Edition.
In multipredictor analyses adjusted for potential confounders (Table 5), NPD occurred at a significantly higher frequency in children with poorer preinjury family function, OR = 0.491, CI95 (0.243, 0.989), p = 0.047. Preinjury lifetime psychiatric disorder was associated with a higher frequency of NPD, OR = 5.08, CI95 (0.996, 25.898), p = 0.050.
Discussion
There were two main findings in our study that examined the occurrence of NPD in the first 12 months after mTBI versus OI. Our first hypothesis that NPD in children will occur with significantly higher frequency in children with mTBI versus comparable OI controls in the first 3-month postinjury, but not thereafter, was not supported. However, we did find an effect of time on the increased risk for development of NPD in children with OI at 6 months versus 3 months and at 12 months versus 3 months, but not in children with mTBI corresponding to a significant group-by-time interaction in terms of adjusted ratio of ORs for mTBI versus OI at 6 months versus 3 months and at 12 months versus 3 months. The second hypothesis was partially supported in that NPD in the first year postinjury was significantly predicted by preinjury family variables (lower preinjury family function) in both single-predictor (p = 0.014) and multipredictor (p = 0.047) analyses but by preinjury child variables (preinjury lifetime psychiatric disorder) only in single-predictor analyses (p = 0.003) and trending in multipredictor analyses (p = 0.05).
The finding that NPD, as a categorical diagnosis, is not significantly more common in the first 3 months after mTBI versus OI differs from our previous analyses of NPD counts (number of NPDs) in each participant from this same cohort in the first 3 months postinjury 7 as well as findings from behavioral studies with categorical and continuous measures of PCS. 19,47 The discrepancy in these findings is related to the differences in analytic approach. Specifically, the current analyses examined the overall pattern of the development of NPD in the first 12 months after injury and required statistical correction for multiple time points. Evidence in support of this postulation is that the OR of NPD in mTBI versus OI at 3 months was 14.327. In contrast, the previous analyses examined only NPD at a snapshot at 3-month postinjury. 7 We interpret this pattern of development of NPD as follows. Children, particularly those with lower preinjury family function and those with a preinjury lifetime psychiatric disorder, may develop NPD by natural history or as a consequence of injury, for example, mTBI or OI. We may understand this phenomenon by considering an injury as precipitating a disruption of the psychiatric and behavioral homeostasis established by the child and family before the injury and that mTBI results in an earlier, albeit transient, destabilization compared with OI because of direct and proximate perturbation of brain function. The transient destabilization among children with mTBI is followed by a return to a natural history trajectory of development of NPD that occurs in any population of children, disproportionately affecting those with lower preinjury family function 48 and those with preinjury lifetime psychiatric disorder. 49 The overall finding that over the first postinjury year, there was no significant difference in the presence of NPD in participants with mTBI versus OI, but a difference in timing of onset of NPD, is somewhat reassuring because it suggests that with an appropriate pediatric injury control group (OI), being a member of an mTBI group is associated with only a short-term psychiatric disturbance. However, it does not follow that for any particular individual with mTBI, their earlier-onset NPD will always resolve before 12-month postinjury (Table 2).
In contrast to the similar influence of mTBI and OI on the occurrence of NPD when considering the entire first postinjury year, preinjury family function (in unadjusted and adjusted analyses) and preinjury lifetime psychiatric disorder (in unadjusted analyses) were enduring predictors of NPD present at any point in the first postinjury year. These findings underscore the importance of noninjury variables that influence psychiatric outcomes in injured children. While these findings are presented for the first time in an ED-treated population of children with mTBI and OI, they are consistent with repeated psychiatric findings in longitudinal cohorts of children hospitalized for mild to severe TBI, 2,22,23,50,51 analyses limited to hospitalized children with mTBI, 24 –26 as well as a large body of literature examining behavioral measures rather than psychiatric diagnostic outcomes. 15 –21,52 –57
The family function finding was expected because preinjury family dysfunction can be considered a suboptimal adaptation to life circumstances, and this dysfunction is a risk factor for future family problems by natural history 58 and in the context of TBI. 39,59 The children of families with greater preinjury dysfunction are at greater risk of adverse outcomes because their families may not have sufficient problem-solving skills to prevent, recognize, and communicate the problem and pursue viable interventions. 38
The child factor result was also anticipated because preinjury adverse child factors (psychiatric, adaptive function, neurocognitive) can be considered less than successful adaptations to daily life that, by natural history, tend to increase the risk of future corresponding adverse outcomes. 49 The findings that NPD was significantly predicted by greater preinjury psychiatric disorder in unadjusted analyses and at a trend level in adjusted analyses are consistent with results from short-term (3–24 months) 2 and long-term (24-year follow-up) 60 prospective longitudinal uncontrolled psychiatric investigations. This risk is a robust finding in natural history studies of childhood psychopathology, even in the absence of mTBI. 49 The results did not implicate lower presumed preinjury academic function and intellectual function as risk factors for NPD. This finding differs from those of a 6-month follow-up assessment of consecutively hospitalized children with mTBI, which found lower IQ, lower processing speed, and lower expressive language function significantly related to NPD. 26 These discrepant findings are most likely related to mTBI sample differences with regard to injury severity, that is, children consecutively treated primarily in the ED compared with consecutively hospitalized children. Thus, it appears that with milder forms of mTBI, preinjury psychopathology is a more important risk factor for postinjury domain-convergent psychopathology (NPD) than are preinjury neurocognitive domain-divergent variables.
Several study limitations are worth noting. First, NPDs at any point in the first year postinjury occurred in a minority of children with mTBI (14.7%) and OI (11.5%). Therefore, although the sample was relatively large, a greater sample would be desirable for studying NPD as a consolidated heterogeneous composite of diagnoses and specific NPDs. Second, attrition at 3, 6, and 12 months, respectively, was 14%, 16%, and 22%. However, our use of mixed-effects longitudinal models provided unbiased inference in the presence of dropout, even with dropout that depends on treatment arm or other individual characteristics that are included in the model (missing at random). Third, teachers’ behavioral questionnaires were missing in 65–79% of cases across assessment points. Fourth, the mTBI enrollees were significantly older than the non-enrollees. Still, the difference was merely 0.6 years, which is not likely to be clinically significant, and age did not predict NPD outcome. Fifth, there is a risk of a “good old days bias” when preinjury function is assessed postinjury. However, this risk applicable to both injured groups was mitigated with a timely postinjury initial assessment (mean = 17.7 ± SD = 5.8 days). This study and other similarly structured studies’ finding that the presence of preinjury lifetime psychiatric disorder predicted NPD suggests that the bias is minor. 2,3,22,23
The study had several prominent strengths. This was the first controlled prospective psychiatric interview investigation of a sample of children consecutively treated for mTBI in the ED. The sample size was large, and by design, the injured control group matched the mTBI probands in terms of sex and age, and all were recruited from a single site. In addition, the groups were not significantly different with regard to most predictive variables, including preinjury psychiatric diagnosis, SES, preinjury family function, family psychiatric history, academic function, and IQ. NPD, the primary outcome, was generated from psychiatric assessments at 3-, 6-, and 12-month points by interviewers who were blind to group affiliation. The diagnoses were clinically relevant as they were made only when significant impairment occurred. Excellent interrater reliability for psychiatric diagnoses was demonstrated with a second rater, blind to the injury group. The assessment measures were clinically meaningful and included self-reported data and also interview-rated data on psychiatric diagnosis, family psychiatric history, and family function. The interviewers’ “best-estimate” psychiatric assessment is the gold standard and depends on multiple informants, including the child, primary caretaker, teacher when available, and the mental status adjudged by the interviewer. The first author, who is a board-certified child and adolescent psychiatrist and who was blind to the injury group, reviewed all assessments. The extension of previous findings at the 3-month postinjury follow-up to the 12-month assessment permitted an appreciation of the transient versus more persistent phenomenology of NPD after mTBI and OI. 7
The findings have several clinical implications. First, NPD is no more common after a single mTBI versus OI overall in the first 12-month postinjury, but the timing of onset of NPD is earlier in the mTBI group. This is relatively reassuring in view of the scope of mTBI as a public health concern. However, it does not mean that some individuals with mTBI will not have prolonged psychiatric complications. Second, the enduring risk factors for NPD through the first 12-month postinjury were significantly lower preinjury family function (unadjusted and adjusted analyses) and preinjury lifetime psychiatric disorder (unadjusted analyses) in the injured child. These findings support calls for public health measures to improve family function through education and family therapy because family function is presumed to be modifiable. Furthermore, while preinjury lifetime psychiatric disorder may be only partially preventable, secondary prevention using early diagnosis and treatment of NPD could mitigate psychiatric morbidity in injured children. Third, identification of higher-risk injured individuals with family dysfunction and personal history of psychiatric disorder could focus limited resources on the prevention and treatment of NPD. This could take the form of a public health debate that focuses on the development of a best-practice protocol whereby ED administrative personnel routinely request permission to share injury information with the child’s primary care physician and school counselor who, in turn, could receive continuing education regarding identification and surveillance of their patients/students who are at greatest risk for psychiatric complications.
In conclusion, children who suffered mTBI were no more likely than children who incurred extracranial injuries to exhibit an NPD in the first year postinjury but had an earlier onset of their NPD. Noninjury factors, particularly lower preinjury family function, which may be a modifiable variable, and preinjury lifetime psychiatric disorder, represent risk factors for NPDs over the first postinjury year.
Transparency, Rigor, and Reproducibility Summary
These analyses are derived from data collected systematically at a single site, the University of California, San Diego. The University of California, San Diego institutional review board approved the study. Written informed consent was obtained from parents, and children provided written consent or assent, depending on their age. The study involved an enrolled cohort (N = 330) of injured children aged 8–15 years. Participants were assessed at the time of enrollment and at 3-, 6-, and 12-month postinjury. Assessments included psychiatric, behavioral, and family assessment; neuroimaging; and neurocognitive testing.
Footnotes
Authors’ Contributions
J.E.M.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, resources, supervision, visualization, writing original draft, and writing—review and editing. N.J. and A.A.Q.: Data curation and writing—review and editing. E.D.B. and E.A.W.: Conceptualization, funding acquisition, methodology, and writing—review and editing. J.E.P. and T.M.E.: Methodology, supervision, and writing—review and editing. A.C. and E.Z.: Data curation, methodology, and writing—review and editing. J.R.H.: Conceptualization, funding acquisition, methodology, analysis of MRI scans, and writing—review and editing. M.H., T.T.Y., E.A.T., W.M., and E.L.D.: Writing—review and editing. F.V.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, visualization, writing original draft, and writing—review and editing.
Author Disclosure Statement
J.E.M. provides expert testimony in cases of traumatic brain injury on an ad hoc basis for plaintiffs and defendants on a more or less equal ratio. This activity constitutes approximately 5% of his professional activities. No competing financial interests exist for other authors.
Funding Information
This research was supported by a National Institute of Child Health and Development Grant HD088438 (J.E.M.: principal investigator; E.A.W. and F.V.).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.