
Abstract
Fractional exhaled nitric oxide (FENO) measurements are useful in monitoring airway inflammation. Online and offline sampling techniques are well standardized. However, young children are often unable to perform slow vital capacity maneuvers. The aim of this study was to compare a simplified mobile offline tidal breathing method with an online single breath measurement. We performed online and offline FENO measurements in children between 5 and 16 years with respiratory disease. Online measurements were performed by a slow vital capacity maneuver; offline measurements were performed by collecting exhaled air in Mylar balloons during tidal breathing. In 59 children (5.3–16.7 years) able to perform both techniques, a good correlation (0.9348) between offline tidal breathing and online single breath measurement was found over a wide range of values. Offline tidal breathing values correspond to online values. Online single breath FENO values can be predicted from offline tidal breathing FENO values. Offline tidal breathing measurements are highly correlated with online single breath values in children.
Introduction
Categorizing preschool wheezers by the presence and type of inflammation in the airway rather than by atopic status or wheezing pattern is a potential strategy to evaluate treatment response to, for example, inhaled corticosteroids. Although broncho-alveolar lavage studies have brought new insight about inflammation in preschool wheeze, 4 this technique is too invasive to be performed routinely. Fractional exhaled nitric oxide (FENO) is a widely studied marker of airway inflammation in adults and children known to differentiate between asthma and no asthma and in addition low FENO values reflect asthma symptom control during treatment.5–8 FENO measurements certainly have not completely fulfilled their promise of being a reliable, easy, and useful tool to improve outcome of asthma treatment. In older children, monitoring of clinical symptoms and lung function was as good as monitoring FENO during the follow-up of inhaled corticosteroid therapy. 5 Higher FENO values have been reported in infants and toddlers with recurrent wheeze versus single episodic wheeze using the offline tidal breathing method.9,10 Few data, however, relate values obtained with the offline tidal breathing method to the classic online slow exhalation technique. Therefore—in a first evaluation—we compared offline and online values in children able to perform both techniques.
Methods
Subjects
Children between the age of 5 and 16 years were recruited during a routine outpatient visit provided that they did not have a respiratory infection in the preceding 2 weeks. Subjects included patients attending the respiratory clinic for routine follow-up for asthma (n = 49) and other respiratory problems (n = 10) such as primary ciliary dyskinesia, humoral immune deficiency, bronchiolitis obliterans, and pulmonary malformations. Asthma was diagnosed according to GINA guidelines. Informed consent was obtained from parents and children, and the study was approved by the hospital's ethics committee.
Subjects were asked to perform an offline tidal breathing FENO collection first, and an online single exhaled FENO measurement 15 min later.
Offline and online measurements
Measurements were performed according to ATS and ERS guidelines.3,11
For the offline measurement, we used tidal breathing maneuvers and collected expired air via a well-fitted mouth mask, attached to a 1,250 L Mylar balloon. In these balloons, NO levels in expirates are stable for at least 6 h. To prevent nasal contamination, we used a 2-way positive expiratory pressure valve with a fixed expiratory resistance of 5 cm H2O, so that the velum was closed during expiration. Because we wanted to use a mobile, technically simple, and inexpensive construction, we did not use a flow restrictor. Expiratory flow was kept relatively constant by instructing the children to breathe in a relaxed way with a frequency of about 16 respirations/min. Every child was instructed to fill 3 balloons. Afterward (maximal time lag 2 h) the mixed expired FENO concentrations were determined with the NIOX chemiluminiscence analyzer (Aerocrine). The mean of the 3 values was denoted as offline tidal breathing FENO.
For the online measurements a slow vital capacity maneuver was performed through the NIOX mouthpiece to reach a plateau level of FENO. To prevent nasal contamination, children were asked to exhale immediately after inhalation without breath holding. A 2-way non-rebreathing valve maintained the expiratory flow constant at 50 mL/s. A biofeedback mechanism was used. Results were displayed and plateau levels, varying <10% (regression analysis performed by analyzer's software), were recorded. Three or, if necessary, more (but not >7) exhalation maneuvers were performed at 2 min intervals. The mean of 3 reproducible FENO measurements was used to calculate online single breath FENO.
ATS guidelines advise testing with ambient NO (aNO) levels below 5 parts per billion (ppb). Because on one-third of the days aNO exceeded 5 ppb in Belgium, we used a cut-off value of 10 ppb.
Statistics
The correlation between online single breath and offline tidal breathing FENO values was assessed using Pearson correlation coefficients. Student's t-test was used for statistic analysis of differences in age between the groups, reporting mean values and standard deviations. Statistical analysis of nonparametric values was performed using Mann–Whitney U-test reporting median values and interquartile ranges (IQR). Bland and Altman statistics were used to compare the 2 methods of NO analysis.
Results
Of 66 children recruited, 59 with a mean age of 10.3 years (range 5.3–16.7 years) performed online and offline FENO measurements successfully. Seven children failed a successful online maneuver. Forty-nine children had a diagnosis of asthma: 39 of them were treated with inhaled corticosteroids, 5 with other asthma medication, and 5 had no maintenance therapy. Ten children had other pulmonary problems.
Median online single breath FENO value was 20.2 ppb (IQR 38.3 ppb): the highest value of 153.2 ppb was recorded in a boy with poor asthma control; the lowest of 2.9 ppb, in a boy who was in follow-up because of a pneumonia. Median offline tidal breathing FENO value was 8.7 ppb (IQR 8.3 ppb): the highest value of 35.4 ppb was recorded in the boy with the maximum online single breath FENO value; the lowest of 2.8 ppb was recorded in a girl with primary ciliary dyskinesia.
Online single breath FENO values (median of 23.7 versus 8.55 ppb; P = 0.002), as well as offline tidal breathing FENO values (median of 9.8 versus 6.5 ppb; P = 0.02) were significantly higher in asthmatic compared to nonasthmatic subjects (Table 1).
aNO, SD, and IQR, used because of non-normal distribution of single breath FENO and tidal breathing FENO values.
Analysis by t-test.
Analysis by Mann–Whitney U-test.
aNO, ambient nitric oxide; FENO, fractional exhaled nitric oxide; IQR, interquartile range; ppb, parts per billion; SD, standard deviation.
Online single breath FENO values were significantly higher than offline tidal breathing FENO values (median 20.2 versus 8.7 ppb; P = 0.0001). There was strong correlation between online single breath FENO and offline tidal breathing FENO in the total group (Pearson correlation r = 0.93, P < 0.0001; Table 1) as well as in the asthmatic (r = 0.93; P < 0.0001) and nonasthmatic subgroups (r = 0.92; P < 0.001).
As shown in Fig. 1 there is a systematic error: the online single breath FENO value is always higher than the offline tidal breathing FENO value and as the average FENO value increases, the difference between both measurements increases. Thus, offline tidal breathing FENO systematically underestimates online single breath FENO.
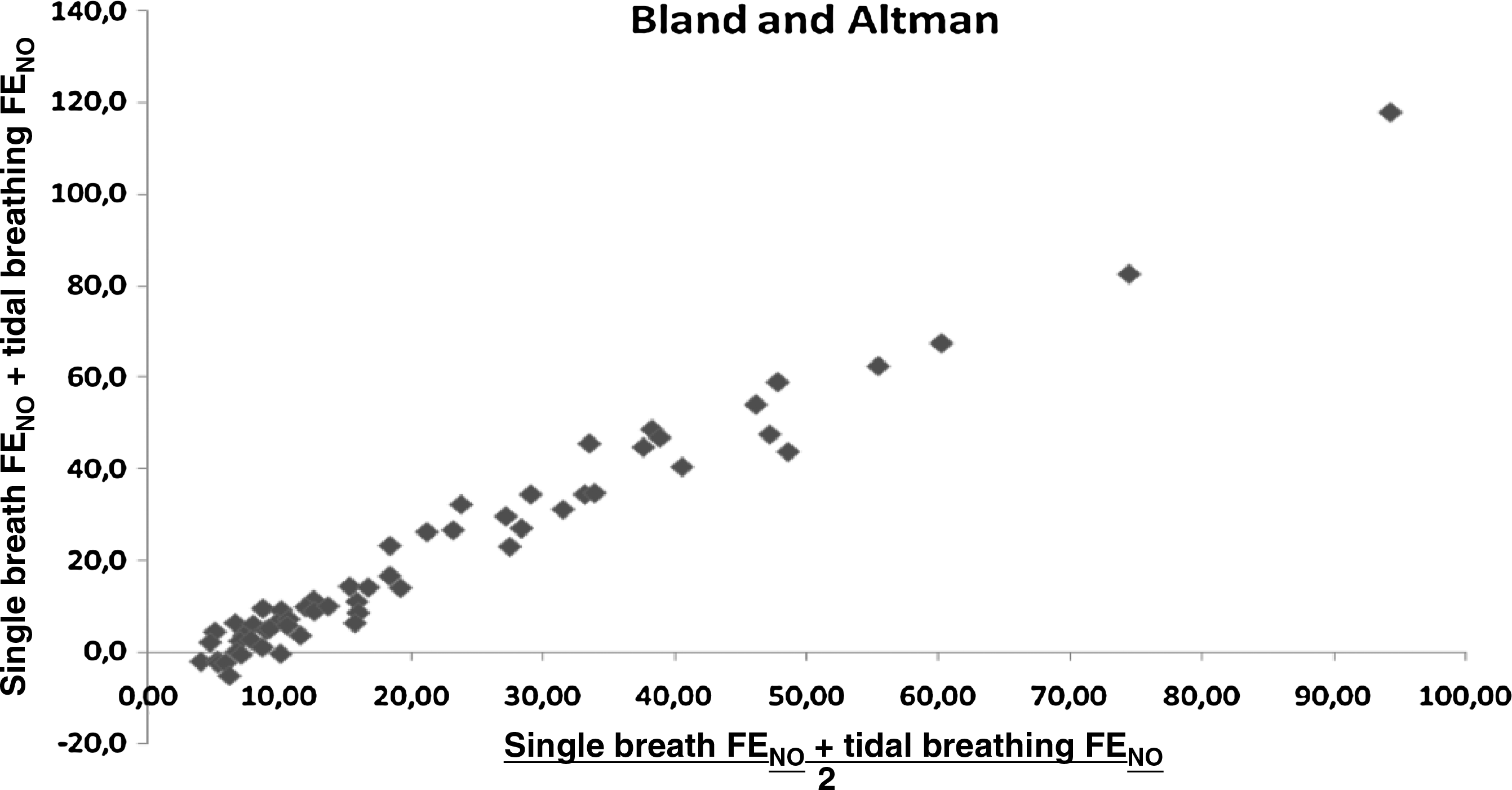
Bland and Altman plot. This plot shows a proportional error with increasing difference between the mean and the subtracted value with increasing values of fractional exhaled nitric oxide (FENO).
To predict online single breath FENO values from offline tidal breathing FENO values, we derived the following regression equation from our data: [online single breath FENO] = [4.0229 × offline tidal breathing FENO—12.932] (Fig. 2). Do note that this regression equation was derived from a sample with mild, well-controlled asthma. This equation may therefore well differ in a population with more severe asthma and/or with FENO measurements outside of the range observed in our sample. Also, the influence of age, sex, ethnicity, and other parameters on this equation was not able to be examined due to small sample size. To this purpose, studies in a larger sample should be performed.
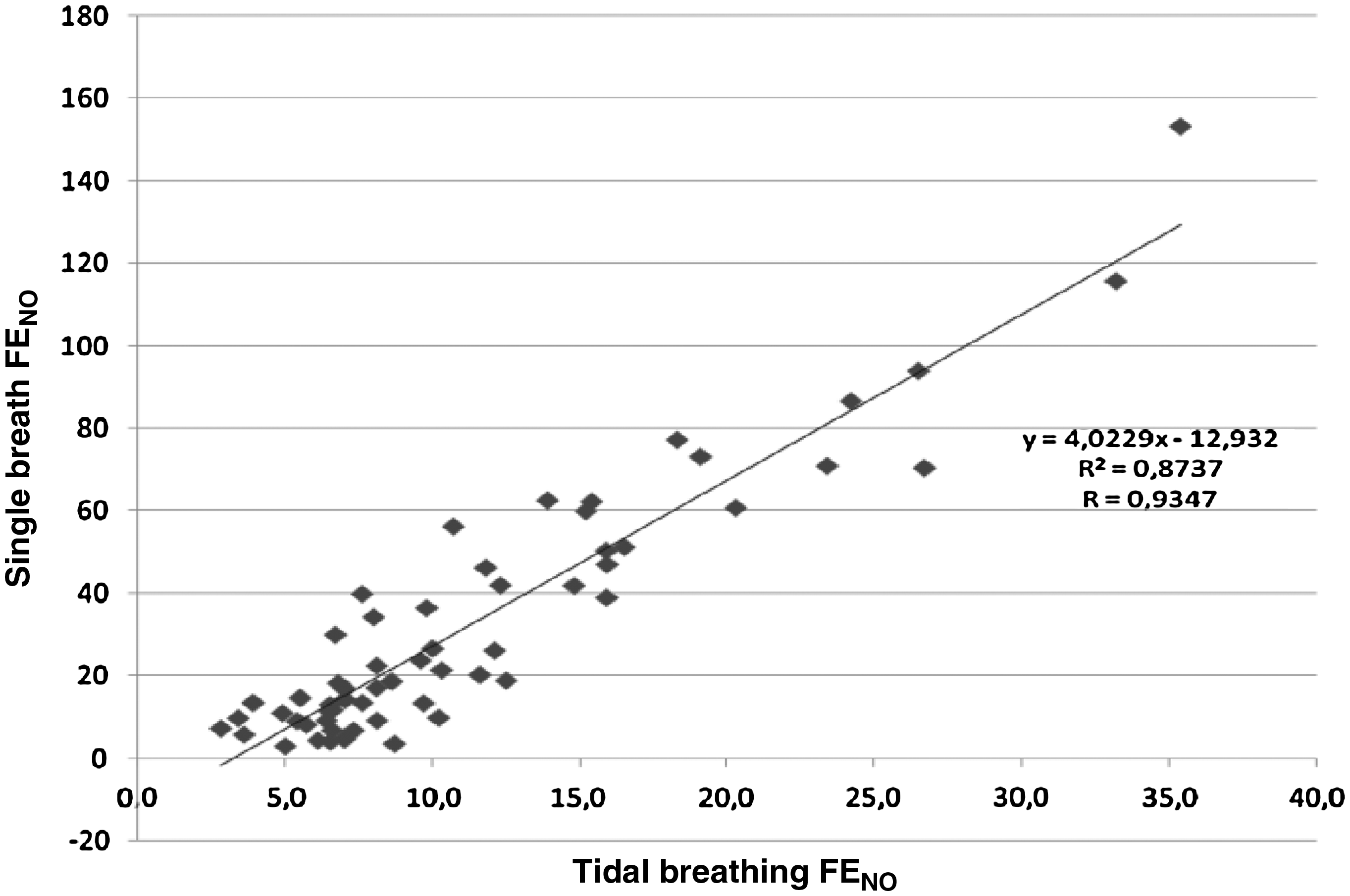
Correlation between single breath FENO and tidal breathing FENO. All FENO values are expressed in parts per billion. To predict online single breath FENO values from offline tidal breathing FENO values, the following equation was calculated: online single breath FENO = 4.0229 × offline tidal breathing FENO − 12.932. This equation has a correlation coefficient of 0.93.
Bland and Altman analysis of “measured” single breath FENO and “calculated” single breath FENO indicates that there is a moderate agreement between both, with a 95% confidence interval of −22 to +22 ppb for the difference between the measured and the calculated single breath FENO.
As for the influence of aNO, values obtained with aNO levels between 5 and 10 ppb were not different from values obtained with aNO levels below 5 ppb (median 10.8 versus 8.6 ppb; P = 0.286). The group with aNO >5 ppb contained 16 patients, the group of aNO <5 ppb, 43. For online measurements the median value was 18.6 ppb (IQR 10.35–46.1 ppb) with aNO <5 ppb versus 29.4 ppb (IQR 11.95–48.05 ppb) for aNO >5 ppb. For offline measurements the median value was 8.6 ppb (IQR 6.55–13.1 ppb) with aNO <5 ppb versus 10.8 ppb (IQR 7.45–15.9 ppb) with aNO >5. Moreover, aNO was not a plateau for the FENO measurements.
Discussion
We have shown an excellent correlation between online single breath and offline tidal breathing FENO measurements over a wide range of values in children able to perform both techniques. However, both methods yield different results because the offline values systematically underestimate the online values. This is probably caused by a much greater impact of air obtained from the large airways, including dead space, in offline values compared to online values.
Several groups have studied the correlation between online and offline techniques for sampling FENO7,12–20 (Table 2). Most of the studies used offline techniques based on a slow vital capacity maneuver with or without flow restriction.7,12,14,17–19 In adults, the correlation between online single breath FENO and offline tidal breathing FENO values is already widely studied, and shows correlation coefficients between 0.63 and 0.99.14,17–19 In this population it is easy to instruct the patients how to perform all the maneuvers correctly.
FR, flow restriction; 95% CI, 95% confidence interval.
In children, 4 studies report a correlation between online single breath and offline single breath FENO. Jöbsis et al. 7 performed online and offline single breath maneuvers in a cohort of 100 children with a mean age of 14.1 years. He found a good agreement between both values when using a flow restrictor. Barreto et al. 12 also found an excellent correlation (r = 0.996) and a good agreement between online and offline single breath techniques in a group of 87 children with a mean age of 11.1 years. The range of the obtained values is not reported. Tadaki et al. 20 found an excellent correlation (r = 0.97) between online single breath FENO measurements and a modified offline single breath FENO measurement using flow restriction in a population of 32 children and 41 adults. A mean difference of 10% between both methods was found. Kissoon et al. 16 report a good correlation (r = 0.88) between online single breath FENO and offline single breath FENO measurement using different flow restrictions in a population of 112 children. The close correlation between both techniques is logical since the breathing maneuver used to collect the sample is similar. The disadvantage of using vital capacity maneuvers for offline measurements is that this technique cannot be easily applied in young children.
Until now, few studies examined offline tidal breathing FENO techniques in children. Buchvald et al. 13 showed a moderate correlation between offline tidal breathing FENO and online single breath FENO (r = 0.70) in a population of 16 school aged asthmatic children. The range of the obtained values is not reported. Jöbsis et al., 15 as well, showed a weak correlation between online single breath FENO and offline tidal breathing FENO (r = 0.53) in a population of 72 asthmatic children. In a study performed by Daniel et al., 21 offline tidal breathing FENO was compared to online single breath FENO in only 11 patients. They surprisingly showed no significant difference between both values, but a correlation was not calculated. Franklin et al. 22 compared offline single breath FENO (raised volume rapid thoraco-abdominal compression technique) with offline tidal breathing FENO in a group of 71 children and found poor agreement between both methods and a moderate correlation (r = 0.60). The range of the obtained values is rather small.
A poorer correlation between offline and online tidal breathing measurement compared to the offline and online single breath methods is not surprising because of the admixture of dead space expirate during the offline tidal breathing method.
In our study, we simplified the previously reported offline tidal breathing method by omitting the use of a flow restrictor. Children were, however, coached to breathe slowly during the collection to avoid that they would take big breaths to quickly fill the whole balloon. We anticipated that in future studies in younger children, collection of tidal expirate during sleep would mimic this slow breathing pattern. A straightforward comparison between offline and online method in toddlers is not possible, as toddlers cannot perform the online maneuver.
Out of practical considerations we included measurements obtained during days of aNO concentrations of 5–10 ppb. We understand the importance of the guideline, but still, if on 1/3 days aNO does indeed exceed the 5 ppb limit, the practicality of this guideline becomes an issue. The fact that the measurements obtained on days with aNO concentrations between 5 and 10 ppb were not significantly higher is reassuring. As shown in Table 2, our data explore the correlation between offline tidal breathing FENO measurements and online single breath FENO measurements over a wide range of values in a pediatric population. Although we found a better correlation than in previous reports, we clearly document the important systematic error as well. The better correlation is potentially due to the larger sample size and the wider range FENO. Because of the close correlation between the obtained values, the proposed equation can be used to calculate online values corresponding to measured offline values, at least in a population of patients with mild well-controlled asthma. In spite of all the methodological efforts made with regard to FENO measurements, the value of FENO in clinical pediatric practice is still a matter of debate.23–25
In conclusion, we here present data showing that offline tidal breathing measurements are feasible in children 5–16 years and that the results correlate well with the FENO obtained in online single breath maneuvers.
Footnotes
Acknowledgments
M.B., I.M., G.W., and K.D.B. have contributed to the study design and acquisition and analysis of data, have drafted the article, and have provided final approval of the final version. I.M. is supported by a Klinisch Onderzoeks Fonds (KOF grant) of the Katholieke Universiteit Leuven.
Author Disclosure Statement
No competing financial interests exist.
The work was performed at University Hospitals Leuven, Belgium.