
Abstract
Pneumonia associated with parapneumonic effusion in children continues to be a common and, at times, a difficult problem to manage. While the majority of children can be treated with antibiotic therapy alone, once the effusion reaches the fibropurulent stage or later, the organizing stage treatment can become more complicated. In the past, once the empyema, these later stages, it was treated with antibiotics, prolonged chest tube drainage, and, if these failed, open thoracotomy for debridement. This was associated with long hospitalization and significant morbidity due to the delayed referral to a surgeon and to the surgical procedure itself. With the expanded use of endoscopic techniques, thoracoscopy has been increasingly used in the treatment of empyema and much earlier in the course of disease. The procedure can be performed quickly and efficiently through 2–5-mm incisions with minimal morbidity. Studies have shown that early thoracoscopic intervention can result in quicker recovery, a decreased length of hospital stay, and earlier return to normal activity, with minimal, if any, increased cost. These facts make this procedure ideal for the treatment of empyema in children.
Introduction
It is clear that empyema in some children is a difficult clinical problem with an often protracted course. Traditional conservative treatment has consisted of therapy with just antibiotics alone or pleural drainage via the chest tube. This is usually adequate for the early or parapneumonic effusion phase, but is often inadequate once the fibropurulent stage is reached. Conservative treatment in this stage has been associated with a high failure rate or a protracted course because of poor antibiotic penetrance to the pleural cavity and because of the inability to adequately drain loculated areas by blind tube thoracostomy. Surgical dogma dictates that the treatment of loculated abscesses is timely, and appropriate drainage and neither of these therapies meet this requirement. While the majority of patients treated this way may eventually get better, they can suffer through days or weeks of hospitalization, antibiotic therapy, and prolonged morbidity and recovery. Cases of treatment failure have resulted in the need for surgical debridement. This was traditionally done via a limited thoracotomy with mechanical debridement of all solid components (the inflammatory peel), a breakdown of all loculations, and drainage of all fluid pockets. This was a simple and an effective solution, although with the morbidity of a thoracic operation.
Over the last 2 decades, minimally invasive thoracoscopic surgery, or VATS, with a low operative morbidity, has become the gold standard for the operative management for fibropurulent pleural space disease. Early reports by these authors Kern and Rodgers 1 , Rothenberg and Chang 2 Gandhi and Stringel 3 , Klena et al. 4 , Merry et al. 5 , Kercher et al. 6 , and McGahren 7 showed the efficacy of thoracoscopic debridement and the improvement in patient outcomes. This included shorter hospital stays or length of stay (LOS), earlier return to normal activity, and decreased overall costs despite the operative intervention. The minimal morbidity associated with this procedure makes it ideal for the treatment of empyema in children. Others advocate the use of fibrinolytic therapy for stage 2 or 3 empyema, and this can be effective in many cases. However, a debate between the 2 therapies is beyond the scope of this article. What is clear is that when fibrinolytic therapy fails, VATS is the therapy of choice.
Technique
The patient is taken to the operating room, and the procedure is performed under a general anesthetic. Single-lung ventilation is generally not required, as the affected side already has a collapsed or compressed lung. The patient is placed in a lateral decubitus position with the involved side-up. The chest is then prepped and draped in the usual fashion.
The chest is first aspirated with a needle placed just anterior to the mid-axillary line at approximately the fourth or fifth interspace to insure that the trocar is placed in a safe area. After infiltrating the site with a local anesthetic and making a small transverse incision (5 mm), a 5-mm trocar is inserted. If fluid is not easily aspirated, an open approach may be used for placement of the first trocar, to assure there is no injury to the lung. If there is an identified site on ultrasound or computed tomography with a big fluid pocket close to one of the proposed port sites, this should be chosen as the point of entry. Once the initial trocar is placed, a suction device is placed through the trocar into the pleural space, and as much fluid as possible is removed. A 5-mm 30° scope is introduced via the trocar and the pleural space examined. In some cases, insufflation with low-flow CO2 to a pressure of 4–5 mmHg may help collapse the lung and improve visualization, as the fibrinous adhesions are taken down. The second trocar should then be placed under direct visualization with the endoscope. If no clear space is identified, the endoscope can be used gently to bluntly take down adhesions and breakup loculations, freeing the lung from the chest wall. Once an adequate space has been cleared, a second trocar can be safely placed. This 5-mm port is placed more posteriorly and inferiorly at approximately the sixth interspace along the posterior axillary line. Generally only 2–5-mm ports are required to perform the procedure.
A suction irrigator is introduced to aspirate the free pleural fluid and to further breakdown loculations with blunt dissection. A sample of the fluid can be collected at this time with a trap. A pair of grasping forceps can then be used to peel off and remove the fibrinous debris through the trocar (Fig. 1). A bowel clamp works well for this purpose. The scope and operating instrument can be interchanged from one port site to another to ensure that all of the pleural surfaces are reached. A systematic approach within the chest also helps ensure that no surface is left untouched. Once the lung has been completely freed, all of the pleural fluid drained, and most of the fibrinous peel are removed, and the thoracic cavity is irrigated with warm normal saline that is subsequently aspirated out. The suction irrigator is removed and the pneumothorax dissipated. The lung is allowed to expand fully with the help of positive pressure breaths from the anesthetist. Once full expansion is confirmed, the lower trocar is removed, and a chest tube, appropriate to the child's size, is placed and positioned posteroinferiorly under thoracoscopic vision and secured in place. The scope and remaining trocar are removed. This site is sutured closed. The chest tube is attached to a pleurovac, and appropriate dressings are placed. It is important that the procedure be performed quickly and efficiently and, in general, should last well under an hour. The principle should be to remove all loculations, fluid, and the majority of the inflammatory peel. Lung expansion after the procedure should be relatively immediate. One side benefit of the thoracoscopic approach is that the lung surface can be examined thoroughly. This has become more important with an increasing incidence of severe necrotizing pneumonia now being seen. If a necrotic or an ischemic lung is visualized, and if the child fails to respond appropriately to therapy, this information may help in the decision tree to proceed with further studies or even surgical resection of the affected lobe.

Inflammatory peel as seen at thoracoscopic debridement.
Postoperative Care
The chest tube is initially left to suction at −10- to −20-cm H2O pressure. Once drainage becomes minimal, there is no evidence of an air leak, and the child is improving, and the chest tube can be removed, usually after a trial of underwater seal. This is usually by the third or fourth postoperative day. Antibiotics are continued and, if cultures are positive, adjusted accordingly. Chest X-rays are obtained at intervals to follow progress (Figs. 2 and 3). Analgesia is necessary and most often given as intravenous morphine boluses in the first 24–48 h postoperatively. Oral analgesia is usually adequate thereafter. The patient is usually discharged to home on antibiotics after s/he has been a febrile for 48 h. Follow-up chest X-rays are obtained as an outpatient to insure complete resolution.

Chest X-ray 2 h after video-assisted thoracoscopic surgery.

Chest X-ray postoperative day 3 before removal of chest drain.
Discussion
Thoracoscopic debridement has significantly changed the algorithm for the treatment of empyema in children (Fig. 4). The ability to quickly clean out infected fluid and debris through minimal incisions and with minimal morbidity has lowered our threshold for intervention. In general, any child thought to need a chest tube for adequate drainage of an empyema is taken to the operating room for a thoracoscopic debridement. Earlier intervention has resulted in quicker recovery with minimal complications. The procedure is relatively straightforward and does not require advanced endoscopic skills. Also, excessive time should not be taken in debriding the chest, as the goal should just be to break down all loculations and remove the majority of the inflammatory peel. Excessive operative times will add to the morbidity of the procedure. A small amount of bleeding or even small air leaks may result from the blunt dissection, as the inflamed fibrinous adhesions are taken down, and the peel is removed. However, these complications, if present, are usually minor and self-limited, and the chest tube drainage is an adequate treatment.
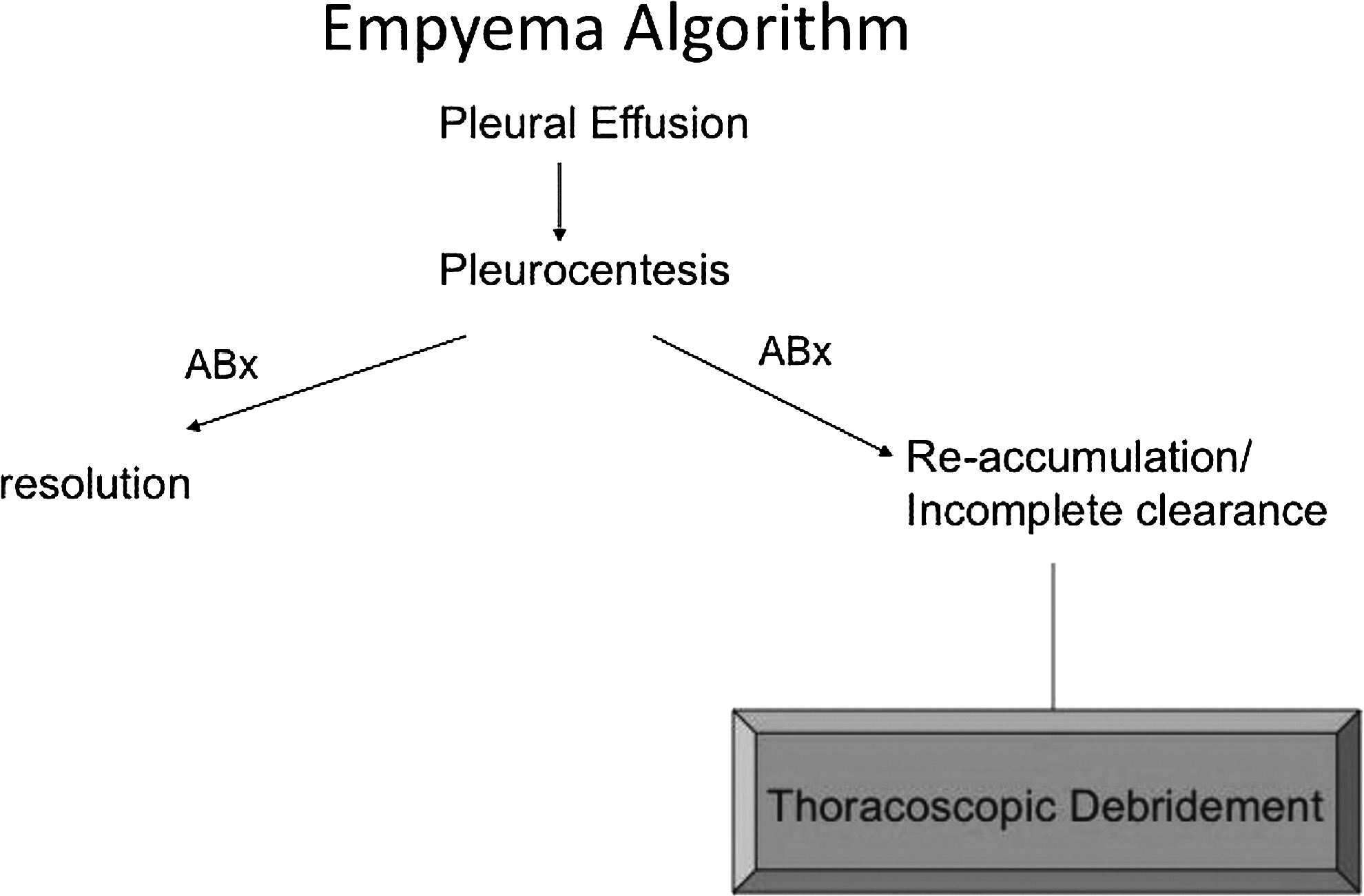
Empyema algorithm.
As already mentioned, an added advantage of the procedure is that the lung parenchyma may itself be easily evaluated. In our last review of our experience over the last 5 years, there were 7 cases of severe necrotizing pneumonia requiring later lobectomy. In each case, the direct visualization of necrotic lung at the time of thoracoscopy helped in the decision to resect the lung.
If surgical consultation is delayed and the patient has been symptomatic for a prolonged period of time, thoracoscopic drainage and debridement may not be possible, and an open decortication may be the patient's only option. This can, however, be assessed by the thoracoscope. With increased awareness of the success of thoracoscopic debridement, surgeons are now generally consulted early on in the course of disease, and the need for open decortication is rarely seen.
Over the last 15 years, these early experiences and results have now been reproduced at numerous institutions and often in prospective studies. Aziz et al. 8 compared patients undergoing chest tube drainage alone, chest tube drainage followed by VATS, and VATS alone. VATS patients had a significantly shorter hospital stay and overall lower hospital charges, whereas 40% of patients undergoing chest tube drainage alone failed therapy and required subsequent VATS. 8 A multi-institutional study by Shah et al. 9 in over 800 children showed that VATS was not associated with higher total hospital costs as those treated with drainage alone.9,11 This was primarily due to the significant cost savings associated with a decreased LOS, and the need for only 1 procedure in the majority of cases.
Some advocate for chest tube drainage and fibrinolytic therapy. Gates et al. 10 advocated for this stating a 50% success-rate associate with nonoperative therapy and higher LOS and costs associated with the surgical intervention. However, this was a retrospective study, and the sickest patients were the ones to receive VATS as a primary mode of therapy. However, 20% of the patients treated with fibrinolysis alone failed therapy and required eventual surgery. These patients had a significantly greater LOS, overall hospital costs, and likely increased morbidity because of their prolonged treatment cost. Primary and early intervention by VATS would likely have shortened their overall treatment course.
It is clear in all the studies that VATS is far superior to conventional thoracotomy and decortication. It is also clear in many studies that VATS is superior to tube thoracostomy alone, except in cases of uncomplicated and nonloculated parapneumonic effusions. Those with simple effusions could probably be treated with antibiotics and pleurocentesis alone with the same results.
The gray area appears to be in the area of fibrinolysis therapy versus VATS. 12 Most studies suggest that these therapies are relatively comparable for the less severe or uncomplicated cases.13,14 However, fibrinolytic therapy still requires placement of a chest drain, usually under heavy sedation, and then repeated applications of the lytic agent. This can be relatively manpower and resource demanding. In addition, there is a certain percentage (10%–40%) of cases that will fail this therapy and requires a VATS, which can be a more difficult procedure when the therapy is delayed.
We prefer a primary VATS approach in any patient with a complicated (loculated) effusion requiring chest tube treatment. The reasons are 3-fold. First, since placement of a chest drain in a child requires heavy sedation in a controlled and monitored environment, we prefer to do this in the operating room with a trained pediatric anesthesiologist, to maximize safety and patient comfort. The second is because of our minimal approach (2–5-mm ports) and the limited time we take to perform the procedure, the morbidity of this procedure is no greater than a tube thoracostomy alone. The ability to debried and drain the pleural space under direct vision also allows a quick and efficient way to evacuate the inflammatory peel and loculated fluid collections.15,16 This results in an immediate ability of the lung to re-expand and hopefully improve antibiotic penetration. It also decreases the likelihood of recurrent loculations requiring further intervention. This is opposed to the lytic therapy where failure of therapy often results in a secondary procedure and a longer hospital stay. The last reason is that thoracoscopy gives the surgeon a chance to visualize the lung, and this may help with future therapeutic decisions.
Treatment of parapneumonic effusions and empyema remains can be varied and remains somewhat controversial, but it appears clear that the most definitive therapy with the lowest complication rate appears to be thoracoscopic debridement and drainage.
Footnotes
Author Disclosure Statement
No competing financial interests exist.