
Abstract
Introduction:
The atopic march refers to the progression of allergic disorders from atopic dermatitis (AD) in early childhood to food allergies, eosinophilic esophagitis (EOE), and later respiratory allergies such as asthma and allergic rhinitis. Mutations in the filaggrin gene, which compromise skin barrier function, are strongly associated with this progression and contribute to allergic sensitization.
Case Presentation:
We introduce a 7-year-old boy with severe AD, food anaphylaxis, EOE, allergic rhinitis, and asthma associated with a filaggrin mutation (c.5152C>T). His clinical course illustrates the atopic march, with initial skin involvement progressing to gastrointestinal and respiratory allergic manifestations.
Conclusion:
Understanding the genetic factors that drive this progression may help identify targets for early intervention to prevent the further development of allergic disease.
Introduction
Atopic march is attributed to the consecutive progression of allergic conditions as a child grows from infancy into childhood. 1 The progression typically starts with atopic dermatitis (AD) and can lead to other allergic diseases, including allergic rhinitis, asthma, and eosinophilic esophagitis (EOE).2,3 Skin barrier dysfunction, often observed in AD, can facilitate transcutaneous sensitization to food allergens, further driving the progression of the atopic march and increasing the risk of IgE-mediated conditions. 4
EOE is an inflammatory allergic disease with eosinophil-rich inflammation of the esophagus 5 with a prevalence of 0.5–1 per 1,000. 6 Some variables, such as environmental and genetic factors and the immune system of the host, can contribute to EOE pathogenesis. 7 Moreover, the disruption of the epithelial barrier, in conjunction with the activation of eosinophils, mast cells, and some cytokines, such as interleukin 5 (IL-5) and IL-13, driven by polysensitization to food allergens, can trigger the development of EOE. 8
EOE is considered a late occurrence of the atopic progression process. 9 The association of EOE and AD suggests a shared genetic and immunological basis.2,10,11 A prevalence of 17.8% of AD was reported in children with EOE. 12
Filaggrin, an epidermal protein, contributes to the stability of the stratum corneum by forming a tight complex with keratin filaments, thereby supporting its strength and integrity. The breakdown products of filaggrin, which act as moisturizing factors, are crucial for maintaining the elasticity and proper function of the stratum corneum. This protein is expressed in the stratified epithelium of the epidermis, oral epithelia, and esophageal mucosa. 13 The defective filaggrin action results in an impaired skin barrier. Loss-of-function mutations in filaggrin are recognized not only as genetic risk factors for AD and allergic sensitization but may also contribute to an increased risk of EOE.8,13,14
We present here a case of a child with the evolution of an atopic march, likely initiated in part by a preexisting filaggrin deficiency that becomes apparent after the progression of his complete allergic progression.
Case presentation
We report a 7-year-old Caucasian boy with a history of severe AD from early infancy, followed by the development of multiple atopic diseases. He is the first and only child of unrelated parents, born of a normal pregnancy. He was exclusively breastfed until he was 4 months old. The first presentation of the patient was severe AD at 1 month of age.
At the age of 3 months, he developed severe gastroesophageal reflux, irritability, poor weight gain, and persisting eczema. A skin prick test was performed and confirmed cow’s milk protein allergy, prompting the mother to eliminate cow’s milk protein from the infant’s diet and introduce an amino acid-based infant formula (EleCare) due to inadequate weight gain. Moreover, Pantoprazole was prescribed for reflux symptoms; however, there was no significant improvement until baclofen was initiated as part of the treatment regimen.
Due to the taste of the amino acid-based infant formula, he stopped using it. At 6 months of age, he experienced anaphylactic shock, wheal, dyspnea, cyanosis, and vomiting shortly after ingesting porridge containing cow’s milk and rice, which the mother, unfortunately, had given to him. Before the age of 7 months, he experienced anaphylaxis after consuming regular formula, and subsequently, he also suffered from anaphylaxis after consuming an extensively hydrolyzed formula (Aptamil Pepti Junior). At 8 months of age, the patient experienced a fourth anaphylactic reaction after ingesting egg white protein. A specific IgE assay (Allergyscreen, MEDIWISS Analytic GmbH, Germany) and skin prick tests revealed sensitization to allergens such as nuts, peanut, dairy, egg, sesame, fish, wheat, and soybean, which led to their exclusion from the diet. Despite improvements in eczema with prescribed treatments and medications, symptoms such as restlessness, reflux, food aversion, and poor weight gain persisted.
At 15 months of age, in light of poor weight gain, unresponsiveness to antireflux treatment, and accompanying gastroesophageal symptoms, a referral to a gastroenterology specialist was made. The patient underwent an endoscopy, which confirmed a diagnosis of EOE based on both endoscopic (Fig. 1) and pathological findings. The esophageal mucosal biopsy demonstrated severe esophagitis, compatible with EOE (eosinophils >50/HPF). The gastroenterologist prescribed a treatment plan that included swallowed budesonide respules, pantoprazole, and baclofen, along with an eight-food elimination diet recommended by an allergist. This diet excluded wheat, dairy products, eggs, soybeans, seafood, nuts, peanuts, and sesame.
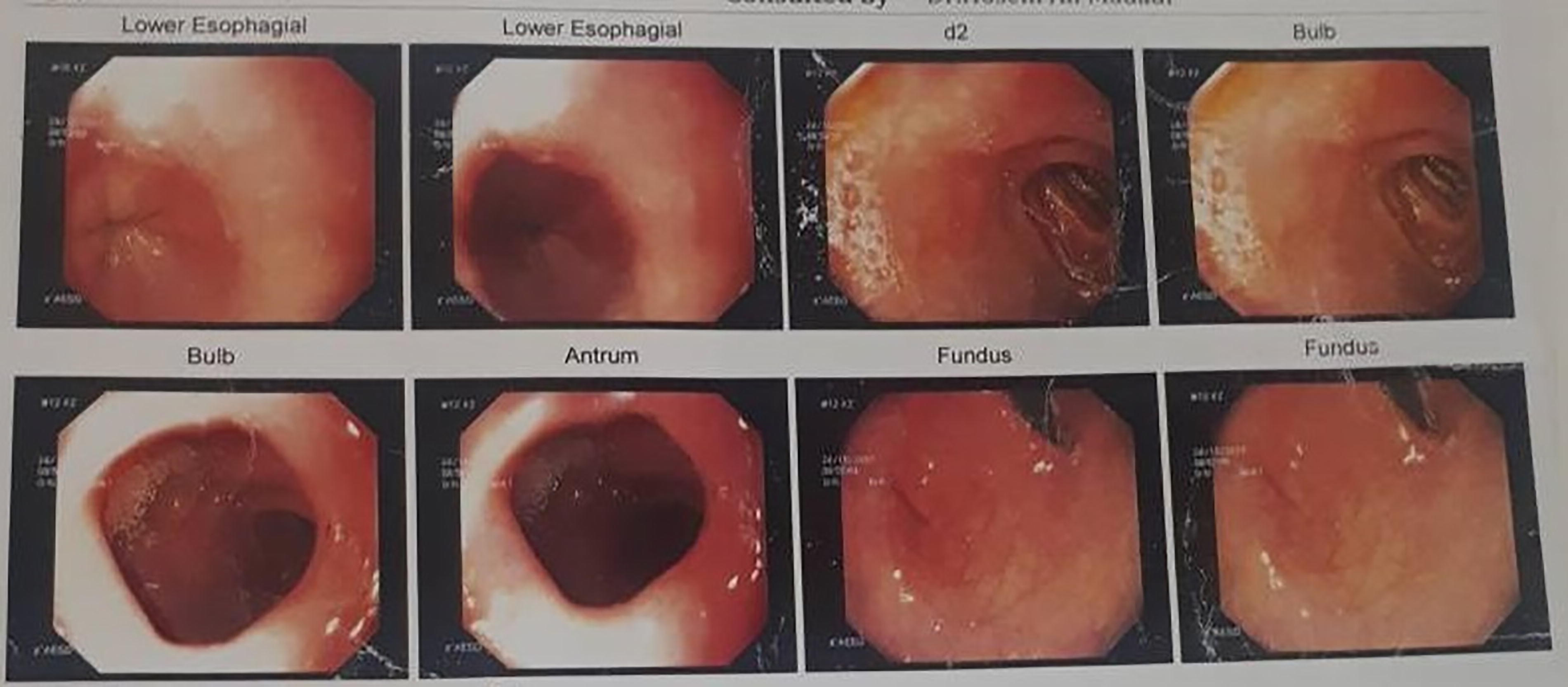
The picture of the upper GI endoscopy of the patient. GI, gastrointestinal.
During treatment, he experienced flares of AD and EOE. Higher doses of topical corticosteroids and pimecrolimus were needed to control the AD.
At 16 months of age, he had a wheeze and dry cough, along with nasal blockage, coryza, and sneezing. The diagnosis was asthma and allergic rhinitis, both of which are managed properly with inhaled and intranasal corticosteroids.
Despite many recommendations for a follow-up endoscopy, the parents refused due to fear of COVID-19. Finally, at the age of 4.5 years, an endoscopy was performed, revealing that the EOE had improved. Meanwhile, the eliminated foods were reintroduced with close monitoring for potential disease recurrence without endoscopy. Wheat, soybeans, fish, peanuts, and tree nuts were returned to the patient’s diet. However, IgE-dependent food allergies to milk and eggs persisted, and the patient experienced anaphylactic reactions after accidentally consuming dairy products and eggs during these times.
The ALEX test (Macroarray Diagnostics, Vienna, Austria) was performed. The results demonstrated a widespread multi-sensitization to pollens (grasses, weeds, and trees), mites, plant-based foods (legumes, grains, spices, fruits, vegetables, and nuts), cockroaches, animal foods (milk, egg, and meat), and animals (pets and farm animals). Among the food allergens, the highest IgE concentration in food extracts was found for cow’s milk (Bos d_milk = 35), goat milk (Cap h_milk = 23.30), and egg allergenic molecules such as ovomucoid (Gal d 1 = 33.80), ovalbumin (Gal d 2 = 32.61), and casein (Bos d 8 = 21.58). Additionally, the highest levels of IgE to aeroallergen extracts were observed against mugwort (Art v = 2.83), Russian thistle (Sal k = 2.71), and goat epithel (Cap h_epithelia = 26.90) and allergenic molecules including Sal k 1 (29.96) and Art v 1 (9.01). Moreover, a positive specific IgE reactivity was observed in protein families such as nonspecific lipid transfer proteins, storage proteins, lipocalins, serum albumin, and NPC2.
A genetic study was conducted for the patient due to the severe course and multiple atopic diseases. Whole-exome sequencing identified two novel variants in the filaggrin (FLG) gene. Based on American College of Medical Genetics and Genomics (ACMG) classification, 15 the Sanger sequencing results showed two heterozygous novel variants in close proximity: c.5151C>T (considered likely benign based on ACMG criteria) and c.5152C>T, which results in an early termination codon in the FLG gene (p.Gln1718Ter). This latter variant has been classified as Likely Pathogenic, according to the ACMG classification. Furthermore, the patient’s mother carries the same variants in this gene, although she reported no history of allergic manifestations. The father carries the likely benign variant and is also asymptomatic (Fig. 2).
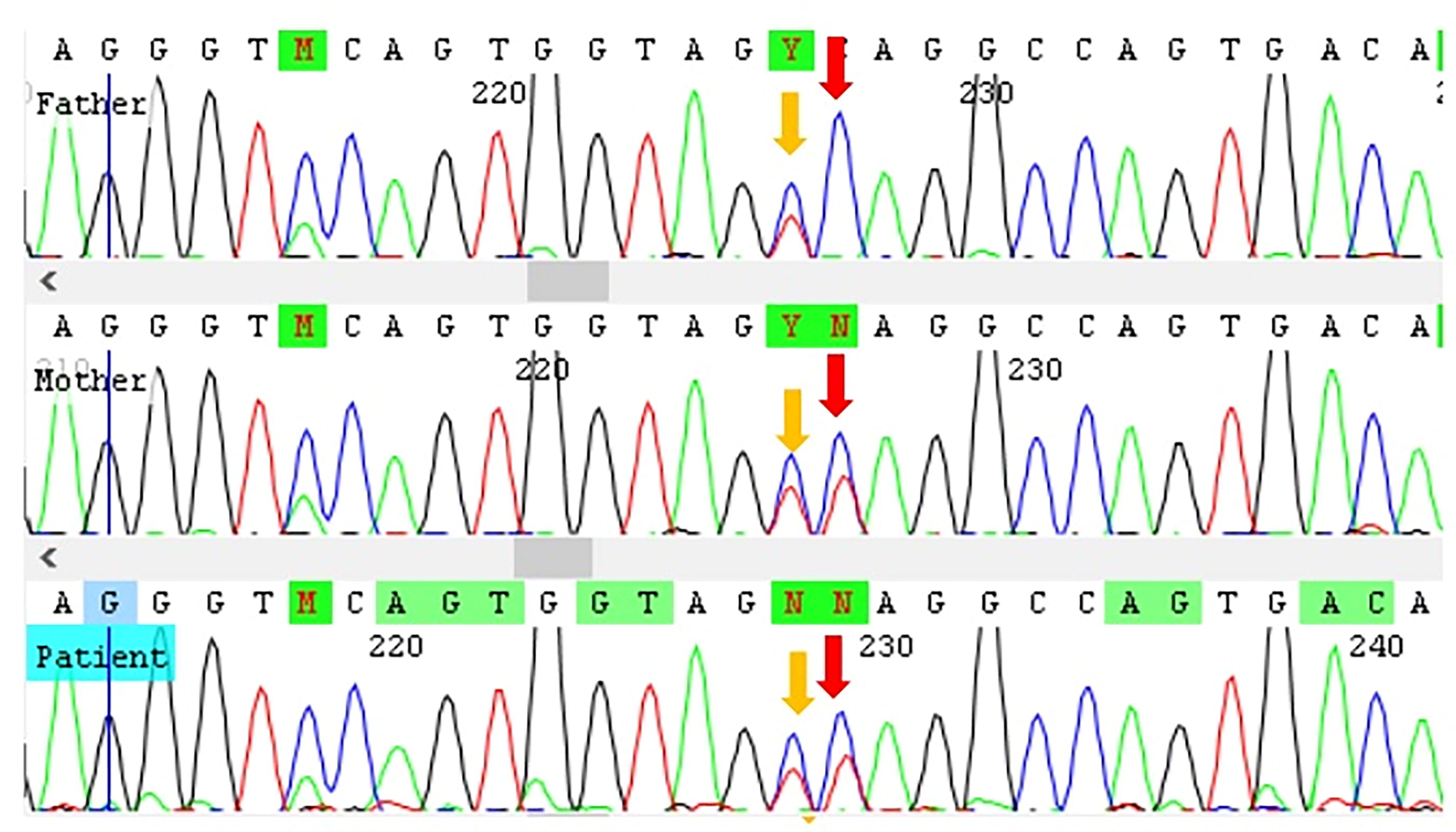
Illustration of the genetic results of the patient and his family: The Sanger sequencing results for the patient revealed two adjacent heterozygous novel variants: c.5151C>T (likely benign variant) and c.5152C>T, which results in an early termination codon in the FLG gene (p.Gln1718Ter). The father carries the likely benign variant, while the mother has both variants.
Discussion
The presented case had severe AD since infancy, which progressed to IgE-mediated food allergy, EOE, and subsequently to allergic rhinitis and asthma. This case underscores the complexity and challenges associated with AD and the potential coexistence of other atopic conditions.
Defects in filaggrin protein are among the most known causes of AD and various allergic conditions. Loss-of-function mutations in the filaggrin gene lead to defective skin barrier integrity.13,16
The cohort study findings by Kalb et al. revealed that loss-of-function mutations in the FLG gene increase the risk of developing multiple food allergies, independent of the AD presence. Moreover, they identified significant relationships between FLG mutations and sensitization to several food allergens such as egg, cow’s milk, peanut, and others. In addition, they found that FLG gene mutations are associated with a higher risk of developing persistent egg and cow’s milk allergies. 13 Similar to the Kalb cohort, our presentation describes a child with multiple food allergies with recurrent episodes of anaphylaxis due to egg and cow’s milk protein 13 continued to recur. Our patient also experienced severe food allergies in addition to persistent cow’s milk and egg allergies. Another study conducted in Italy on pediatric patients with FLG LOF mutations represented a severe form of food allergy. Their analysis for comparing specific food allergies in wild-type and FLG LOF mutation patients showed that FLG mutations only increased the risk of peanut and hazelnut allergies. 16 Our patient was also sensitized to these two food allergens.
According to the literature, the risk of sensitization to food or inhalant aeroallergens is not elevated as a result of the LOF mutation in the FLG gene and is not associated with the presence of AD. 1 Another finding from an Italian cohort study was that FLG mutations were not associated with allergic rhinitis and asthma. 16 However, our patient experienced allergic rhinitis and asthma with multiple aeroallergen sensitizations. These differences may be explained if they had followed their patient for a longer time. Further, it may be due to different epigenetic and environmental factors. Moreover, the presence of a filaggrin gene mutation may increase the likelihood of anaphylactic reactions to food allergens, as the compromised skin barrier promotes sensitization to these allergens. Within this complex network of relationships, the filaggrin gene mutation emerges as a crucial factor, highlighting its significance in the development of AD, 16 EOE, 17 and severe food allergies. 16
It is noteworthy to mention that our patient’s mother has the same mutation in the FLG gene without any allergic complications. Previous studies have indicated that a fraction of healthy individuals can be carriers of FLG mutations. It has been suggested that epigenetic regulation and environmental factors play a potential role in the pathogenesis of AD, along with pathogenic variants. These regulatory mechanisms affect immune responses, particularly the balance between Th1 and Th2 cells and are related to innate immunity and the structural proteins of the epidermis. 18
Furthermore, Hill et al. considered EOE the fifth member or late occurrence of the atopic march progression.9,19 Their 17-year cohort study found that the peak incidence of EOE follows the onset of AD, IgE-mediated food allergies, and asthma, occurring closely alongside the development of allergic rhinitis. Their peak ages for the diagnosis of EOE and allergic rhinitis were 2.6 and 2.1 years, respectively. 9 The sequence of allergic diseases in patients can vary. Contrary to their study, EOE occurred earlier than the respiratory allergy in our case. Perhaps if the endoscopy had been done earlier, the diagnosis of EOE could have been made sooner. 1
Conclusion
Understanding the pathogenesis of atopic march, particularly the progression from AD and food allergy to asthma and allergic rhinitis, is essential for identifying the genetic factors that drive these processes. This knowledge can inform strategies for early intervention and the development of new treatments aimed at preventing the progression to allergic airway diseases.
Footnotes
Acknowledgment
The authors acknowledge Mrs. Maryam Teimouri for her outstanding cooperation.
Consent for Publication
Informed consent was obtained from the patients’ parents.
Generative AI and AI-Assisted Technologies
Authors’ Contributions
A.R.: Conceptualization, validation, resources, writing—original draft, and writing—review and editing. L.M.: Resources and writing—review and editing. B.A.: Resources and writing—review and editing. M.K.A.: Investigation, resources, and writing—review and editing. Z.A.: Investigation, writing—original draft, and writing—review and editing. R.S.S.: Investigation, resources, and writing—review and editing. M.F.: Conceptualization, validation, resources, and writing—review and editing.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funding was received for this article.