
Abstract
Introduction
Hyperacusis, low sound-volume tolerance, can sometimes be a severe condition for patients, who may experience discomfort at 40 dB, or sometimes even at lower sound volumes. The disorder may be frequency specific. Not all sounds of the same loudness cause discomfort/pain – only sounds within a certain range; thus a small change of frequency may cause discomfort at low volume. 14 In a survey conducted by the American Tinnitus Association, 70% of hyperacusis patients reported some form of hearing loss. Among hyperacusis patients, 86% suffer from tinnitus, and in such cases it is often the hyperacusis that is considered the more severe of the two disorders. 15 A positive correlation has been found between hyperacusis and tinnitus. A classification system exists for hearing loss, and a similar system is suggested for hyperacusis. 16 The tolerance level for pure-tone sound is less than 90 dB HL. 17 Hyperacusis is caused by pathologic conditions of the peripheral auditory system, diseases of the central nervous system, and hormonal and infectious diseases. In some cases there is no known cause. The pathophysiology of hyperacusis probably involves a central mechanism rather than a peripheral one. 18 Hyperacusis and phonophobia represent disturbances of central auditory processing without peripheral pathology, often combined with psychosomatic reactions. 19 Free radicals and singlet state oxygen have been detected in laser-irradiated biological material and systems, 20,21 There are several medical and biological effects reported in medical studies of the influence of electric and magnetic fields, including dilation of capillaries and less blood-flow resistance, with research also suggesting magnetic field therapy as a new concept to treat tinnitus. 22 –25 The appearance of high levels of reactive oxygen species (ROS) and their negative influence on the organism have been verified. 26 It has been claimed that tinnitus treatment research projects have displayed a positive placebo effect among up to 40% of the patient population. 27 While searching the literature on MEDLINE and PubMed, no hyperacusis treatment studies were found where hyperacusis pain levels measured in dB HL have improved significantly.
The aim of this clinical trial was to find out whether or not hyperacusis pain-threshold levels improved after therapy compared to a placebo group, where 40% of the observations were expected to improve. The aim was also to determine how great the improvements in such cases would be. It is the combination of the three treatment modalities described in this article that is novel about this work, as well as the findings that pain thresholds improve for patients suffering from hyperacusis when treated simultaneously with these three therapies.
Materials and Methods
Subjects
From 1999 through 2001, patients with different kinds of inner-ear disorders, also suffering from both tinnitus and hyperacusis, came to the clinic for treatment of their tinnitus symptoms with laser therapy in combination with pulsed electromagnetic field therapy/repetitive transcranial magnetic stimulation (rTMS) and the control of ROS. The three therapies were administered simultaneously. Hyperacusis pain thresholds were not measured for the first 10 hyperacusis patients undergoing treatment, but they all claimed that their hyperacusis improved. Out of those first 10 patients treated, 8 claimed that the improvement was great, and 6 that the improvement was noticeably greater 3–4 mo after therapy finished than at the last session of the treatment period. After observing improvements based upon subjective assessment from the first 10 treated hyperacusis patients, an audiometric measurement method for hyperacusis pain thresholds was developed based upon recent scientific articles 16 to make measurement and evaluation more accurate than subjective assessment. A prospective clinical trial was planned and carried out in 2001.
From 2001 through 2006, 444 observations were measured both before and after therapy. An observation is the measurement before and after therapy of one frequency in one ear. Up to 11 observations per ear were measured, ranging from 125 Hz to 8 kHz. All were initially tested in each ear, but only those regarded as hyperacusis were tested after therapy. The number of observations in an ear depended on the number of frequencies where pain from sound levels lower than 87.5 dB HL occurred.
In this clinical study, 30 males and 18 females were treated and audiometrically tested. Patients ranged in age from 15 to 86 years, with an average age of 39.3 years and a median age of 39 years. All patients's hyperacusis was deemed to be chronic, as they claimed they had been suffering from hyperacusis for at least 6 mo and up to 20 years–but no pain or annoyance thresholds had ever been tested at any other clinic. All hyperacusis patients visiting the clinic were offered the treatment; there were no exclusion criteria in this study.
One patient claimed that his hyperacusis had slowly improved over a period of 5 years but that his yearly improvements were minimal. There was one dissident/dropout not audiometrically tested after therapy finished. All 48 patients and a total of 83 ears were audiometrically evaluated. Short-term follow-up (evaluation immediately after the last treatment session) was performed on 364 observations, 40 patients, and 69 ears. Long-term follow-up (evaluation 4–6 months after the last treatment session) was performed on 80 observations, 8 patients, and 14 ears.
The patients were treated twice a week with 10–20 sessions per patient. Each session lasted 32 min. Both ears were always treated simultaneously to avoid the unwanted side effect of vertigo, even when only one ear was afflicted with hyperacusis.
Contraindications for laser therapy are: cancer tumors on the N. acusticus or N. vestibularis; epilepsy; and strong pigmentation. With regard to pigmentation, dark or wheatish patients should be treated with laser probes not exceeding an output of 100–300 mW. Strong pigmentation absorbs the light. Dark tissue in the meatus acusticus can overheat, which can cause pain and/or damage due to heat-dependent reactions.
Restrictions for patients receiving laser therapy include: not exposing themselves to high doses of broadband white light during the period when therapy is performed and during the first 2 wk following therapy; protecting their ears from all kinds of sound traumas during the therapeutic period and during a period of 6 mo after the final treatment session. In addition, patients with abnormally high levels of ROS should not take any medication that will increase levels of ROS, and patients with abnormally low levels of ROS should not take antioxidants.
Equipment and treatment protocol
Irradia AB (Stockholm, Sweden) was the manufacturer of the laser equipment. Two different categories of laser probes were used. The inner ear was treated with both 808 and 650 nm lasers, both successfully used in several tinnitus studies. The 650 nm laser was also used for the treatment of the epidermis in the ear canal and in the middle-ear tissue, sometimes affected by inflammatory processes.
Trigger points and stiff chewing muscles in the jaws were additionally treated with a 904-nm laser on those patients suffering from tinnitus suspected to be correlated to temporomandibular causes.
At every treatment session, 177–504 J of laser light from the 808 and 650 nm laser probes was administered via meatus acusticus. The dose per session was not always the same for a patient throughout the whole treatment period. It was adapted for each patient, taking into consideration differences in anatomy, side effects, and detectable reactions and/or non-reactions.
Laser light was administered using three different probes: GaAs, 904 nm, 120 mW (8 diodes, 15 mW average output power/diode), 5 Hz pulse (this pulse frequency has successfully been used in tinnitus therapy by Prochazka and Hahn
6
), administered for 7 min (50 J) over a circle area of 50 cm2 over the temporal lobe, the M. masseter, Proc. coronoideus, and the Lig. stylomandibulare. GaAlAs, 808 nm, 490 mW, sun feather shaped 30° diverging beam, continuous light, administered via meatus for a minimum of 4 min (120 J) and a maximum of 16 min (480 J) at the beginning of the session. The laser probes were applied as close as possible to the tympanic membrane so that as much laser light as possible could be administered to the inner ear. Contact mode with the tympanic membrane was not possible. The probe tip was located at a depth of 1–2 cm in the ear canal. All patients had fair skin, and none experienced any discomfort from heat or thermal effects. InGaAlP, 650 nm, 35 mW, continuous light, unfocused collimated beam, administered via meatus for a minimum of 16 min (34 J) and maximum of 28 min (59 J), after the administration of 808 nm laser light. The laser-probe tips were placed in the ear canal, aiming toward the tympanic membrane.
Pulsed electromagnetic field used for rTMS
A Bemer 3000 (Triesen, Germany) pulsed electromagnetic field system was used for rTMS. The Bemer 3000 system is an approved device for the use in medical treatment in the EU, class 2A according to the ISO 9002 and DIN EN 46002. Further information about the Bemer 3000 system can be found on the Bemer 3000 homepage. 28 The system comprised a preprogrammed Bemer 3000 basic driver and a Bemer 3000 standard electromagnetic intensive applicator with a maximum output of 100 μT, used bilaterally for 16 min per ear. To begin with, the applicator was applied close to the mastoid bone, behind the most afflicted ear of each patient suffering from hyperacusis (Fig. 1). After treating the first ear, the applicator was moved to the same position on the other ear for 16 min. Program P3 was used for the intensive applicator.

The patients were treated lying down, here with an 808-nm laser-probe tip placed inside the ear canal. The Bemer 3000 pulsed electromagnetic field applicator is placed close to the mastoid bone, behind the ear.
Evaluation of results
ROS–measurement and analysis device: ROS in blood were analyzed in order to be able to prescribe suitable doses of antioxidant tablets. A sample of 20 μl capillary blood was analyzed spectrophotometrically with a Callegari CR 2000 Free Oxygen Radicals Monitor (FORM). ROS were measured in Free Oxygen Radicals Test (FORT) Units (Callegari S.p.A.). The normal interval for FORT in blood is 230–310 FORT Units. If the test exceeded the upper limit of 310 FORT Units, antioxidants were prescribed in larger doses than the patient's actual intake, so that the FORT value would most likely reduce. If the FORT test displayed abnormally low levels of FORT Units, then
Audiometric test: Patients suffering from hyperacusis were measured with a calibrated manual audiometer with audiometric earphones in a sound-isolated room. In the hyperacusis pain-threshold hearing test, 11 standard frequencies, ranging from 125 Hz to 8 kHz, were tested. The sound length per beep was 0.2 s. Each frequency measurement started with a sound volume of 25 dB HL and then rose in 5-dB-HL steps until the patient experienced pain from the sound. The first frequency tested was always 8 kHz, then 6 kHz, 4 kHz, etc. If the patient experienced no pain below or at 85 dB HL, the audiometric test at that frequency was aborted and the test continued with the next frequency.
All patients were instructed to respond at the level they experienced sound as painful. Annoyance or discomfort was not accepted as a response level; sound pain thresholds seem to be more distinct than sound annoyance or discomfort thresholds. The audiometric tests were executed with a device that was unable to exceed volumes of 100 dB HL at frequencies from 500 Hz to 6 kHz. The maximum test level for 250 Hz and 8 kHz was 80 dB HL, and 60 dB HL for 125 Hz.
Pain experienced at any sound level lower than 90 dB HL was regarded as hyperacusis. Patients not experiencing pain at any sound level during the final evaluation were given an estimated value for their pain threshold, 5 dB HL higher than the maximum capacity of the audiometric device.
The patients decided whether they would return to the clinic for either a long-term follow-up evaluation after 4–6 mo, or a short-term follow-up immediately after the final therapeutic session.
Statistical analysis: Statistical analysis was based upon the whole population, the short-term follow-up group, and the long-term follow-up group. The average and median pain-threshold levels per frequency, per observation, and per ear were analyzed. Standard deviation and variance was also calculated. The chi square (χ2) test was used to compare verum groups in the study with a placebo group, where 40% of the observations were expected to improve. The significance, based upon the differences before and after therapy as well as the differences in improvements between the short-term and the long-term follow-up groups, were calculated using the Student's t-test.
Results
The hyperacusis pain thresholds improved for all treated patients. Out of a total of 83 ears, 69 had an average improvement of 10 dB HL or more. The largest average improvement in one ear was 40 dB HL, and the largest improvement for a single observation was 65 dB HL.
Table 1 shows that the average improvement in the long-term follow-up group was considerably better than the average improvement in the short-term follow-up group. A heteroscedastic, two-tailed distribution Student's t-test comparing all observations in the long-term and short-term follow-up groups showed a significant difference (p = 5.54× 10−10).
Table 2 shows that severe hyperacusis improved more than milder conditions. Patients experiencing pain at 40 dB HL before therapy received an average improvement of 47.5 dB HL and tolerated an average sound volume of 87.5 dB HL after therapy.
Table 3 shows the values used in the three chi square (χ2) tests and the significant improvements in all three groups compared with a placebo group, where 40% of the observations improved.
In the long-term follow-up group, 43 (54%) of the 80 observations reached the maximum sound-level capacity of the audiometric device at the final examination without the patients experiencing pain. In the short-term follow-up group, it was 128 observations (35%).
There was one unimproved observation (1%) in the long-term follow-up group, and 25 (7%) in the short-term follow-up group. The difference is significant (p = 2.64 × 10−50).
A total of 84.3% of ears and 79.2% of patients improved on all observations, and 64.6% of patients recovered completely from chronic hyperacusis.
Using the Student's t-test, the difference in improvement, measured in dB, between the two groups was found to be significant (p = 5.54 × 10−10). Before therapy, the difference was p = 2.27 × 10−7, which reveals a significant difference between the two groups before therapy but not after (p = 0.42).
The two poorest average improvements per ear were found in the same individual, where the average improvements per ear were 1 and 3.5 dB. The levels of ROS for this individual were 852 FORT Units (an extremely high value) at the start of therapy, and 460 FORT Units at the end of therapy, which is still much higher than normal levels, even after allowing for estrogen pills that were taken.
Discussion
For 171 (39%) of the observations tested, the maximum sound-level capacity of the audiometric device was reached without any experience of pain, as post-treatment pain thresholds could not be reached with the audiometric device. If the audiometric device had been able to generate louder sound volumes, the results might have been greater than displayed. However, measuring louder sound volumes also poses a greater risk of sound trauma.
Almost all patients in this study were evaluated for their hyperacusis for the first time in their lives. The fact that there is as yet no widespread standard procedure for measuring hyperacusis is a problem in determining how long a patient has been suffering from hyperacusis, how severe the condition has been, and if there have been changes over time.
A majority of the patients were assumed to have hyperacusis, depending on inner-ear damage inside the cochlea. The doses were therefore calculated with regard to light penetration of the cochlea, according to Tauber's penetration study, 10 after an ocular examination of the ear canal and of the tympanic membrane, and after an estimation of light absorption in the tissue surrounding the ear canal. The sun feather shaped 808-nm laser diode spreads the laser light more than a collimated laser diode. Therefore the use of collimated diodes could reduce the total dose of light administered.
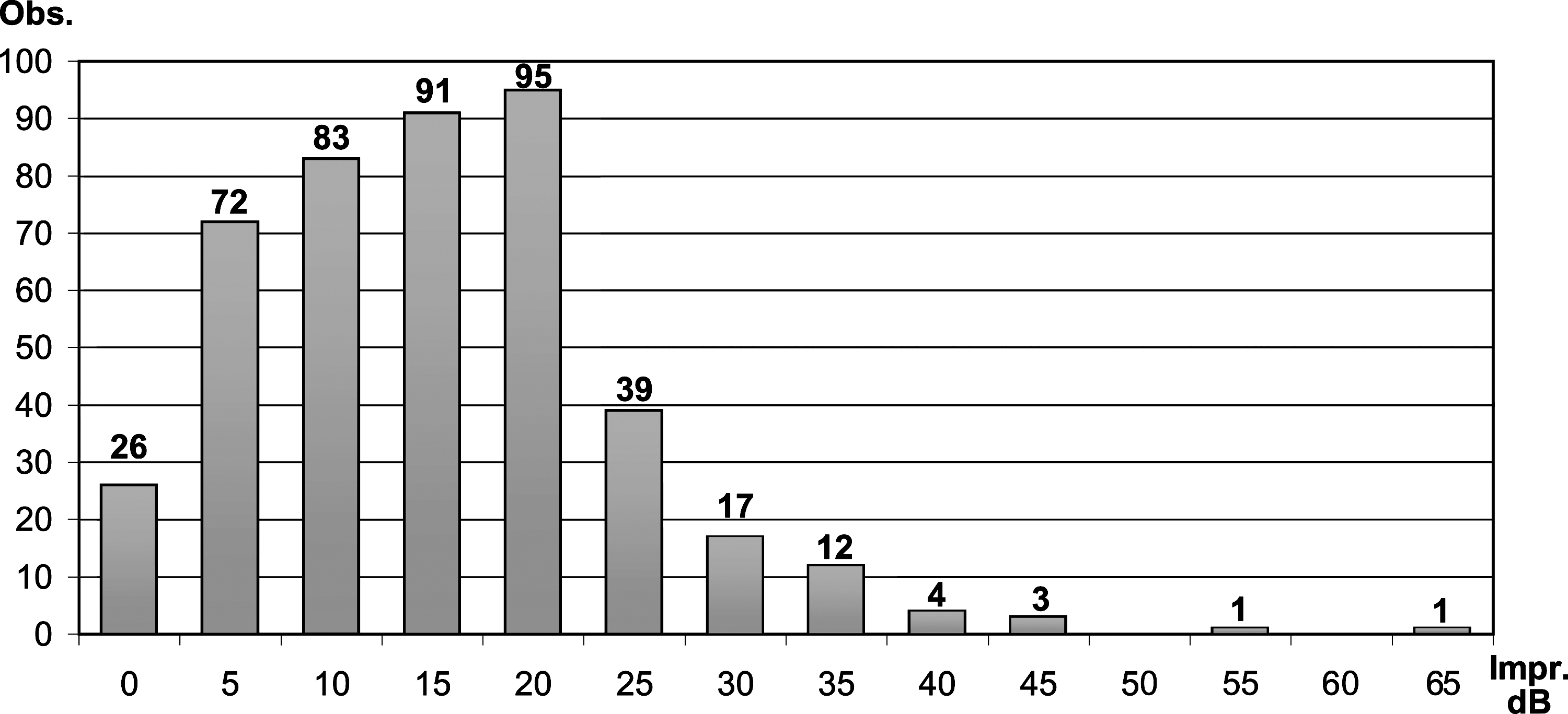
The most common result (21%) was an improvement of 20 dB HL. There were 26 unimproved pain threshold observations (6%). The largest improvement for a single observation was 65 dB HL. No observations worsened. The standard deviation is 9.42 based upon all observations.
There is a significant difference between the improvements of the long-term and short-term follow-up groups (p = 5.54 × 10−10). However, the difference before therapy was also significant (p = 2.27 × 10−7). After therapy, the difference between the groups was not significant, p = 0.42, which may be attributed either to greater improvements for long-term follow-up patients or to the fact that the 14 ears in the long-term follow-up group had more severe conditions at the start of therapy than those in the other group. On the other hand, several patients in the long-term follow-up group insisted that their ears definitely improved during the first 6 mo after the end of the treatment period, which may account for increased long-term effects.
All but three patients in this study were diagnosed as suffering from hyperacusis due to sound trauma. One person was suffering from hyperacusis after a bilateral sudden-deafness trauma; another after intravenous streptomycin therapy; and a third patient was exposed to sound trauma in combination with an intake of streptomycin. Damage to the inner-ear cells are therefore possible in all ears included in this study and could be the most frequent cause of hyperacusis here.
Systemic treatment effects cannot be excluded, but it is possible that the combined therapy in this clinical study was responsible for the positive results. Regarding the cause of hyperacusis and the positive treatment results for hyperacusis pain thresholds, it is very likely that among the majority of patients, hyperacusis depended on peripheral inner-ear damage and not that of central mechanisms.
High levels of ROS could be a reason for the poor improvements obtained in the described case where ROS levels were 852 FORT Units before therapy. All other hyperacusis patients were found to have ROS levels below 360 FORT Units at the start of therapy. ROS levels could play an important role in inner-ear therapy, and a future research project could be in the analysis of improvements for patients with inner-ear disorders. Concentrations of ROS within the normal interval (230–310 FORT Units) seem to be a selective tool for finding good candidates for the treatment. Poor candidates seem to be patients with extremely high levels of ROS and possibly also patients with very low levels of ROS.
This study did not include any control or placebo group, but an expectation, for spontaneous changes among chronic patients suffering from hyperacusis due to sound trauma, could be based upon placebo-group results from previous tinnitus studies. It is assumed by Borg 27 that up to 40% of patients in a tinnitus-treatment placebo group can sense an improvement. That is, however, when subjective assessment is used for evaluation and not, as here, using audiometrically measured results. However, audiometric evaluation has its difficulties. The position of the earphones can vary from one test to another, no matter how carefully and accurately the test is performed. For a large number of observations, the risk of a decisive error is, however, smaller than for fewer observations. In this study, there were 444 observations, making the risk of errors resulting in a positive rather than a negative outcome quite small.
Another limitation of measuring pain is that patients can experience pain in a different way several months after the first measurement occasion. In this study, the time elapsing from the first measurement to the follow-up measurement was 1–8 mo.
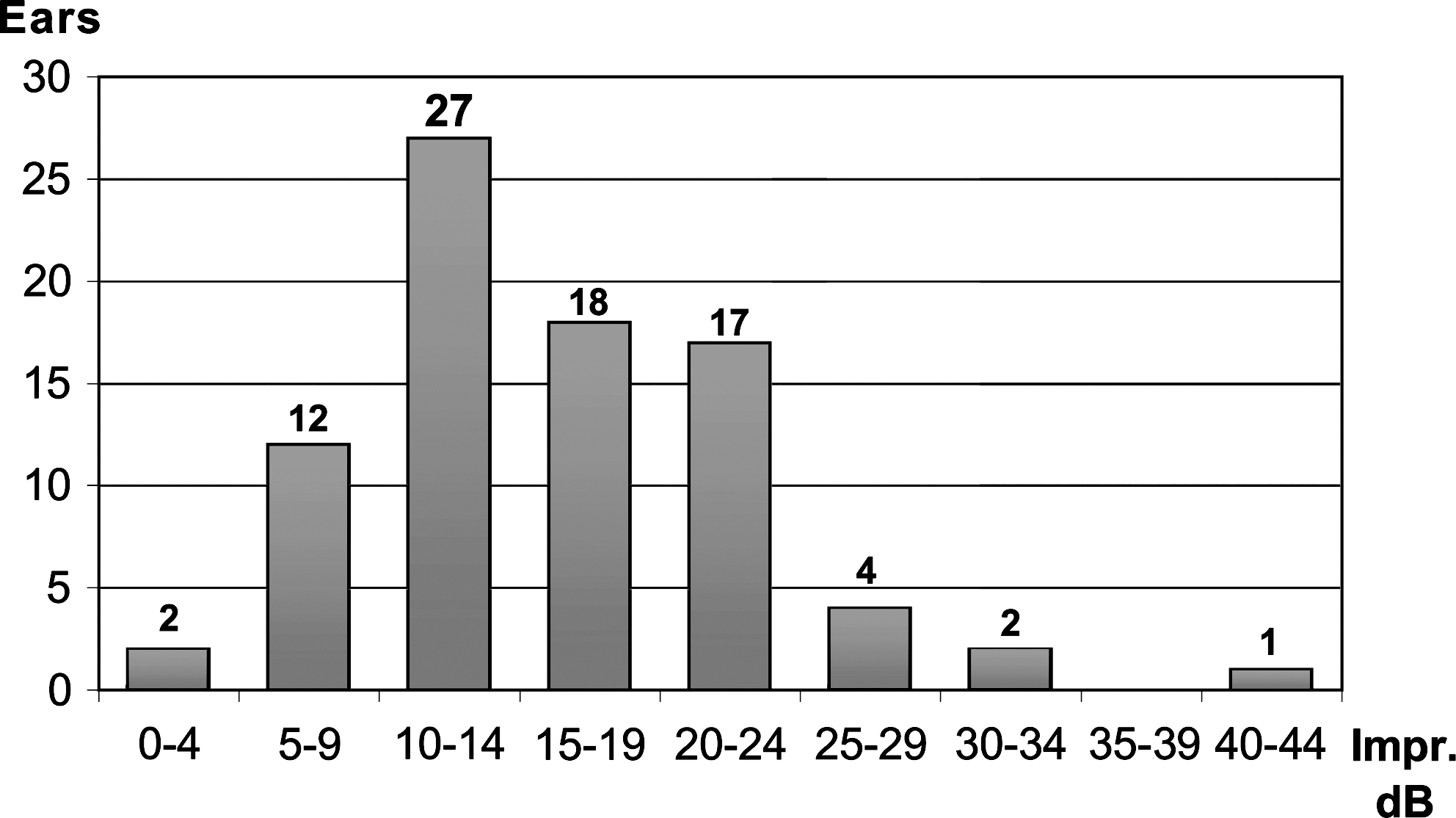
The most common average improvement per ear was found in the range 10–14.99 dB HL. An improvement of 10 dB HL or more on average was found in 69 ears (83%). The standard deviation is 7.14 based upon the average improvement per ear.
A positive correlation has been found between hyperacusis and tinnitus, suggesting a close relationship between the two disorders concerning mutual causes. 16 Assuming that 40% of hyperacusis patients receive a positive treatment effect (based upon Borg's statement about tinnitus patients 25 ), a comparison of results is possible, calculating whether the improvements are significant or not, and if they are, at what level. Based upon that, chi square (χ2) tests were calculated as p = 5.83 × 10−120 for all observations, p = 4.1 ×10−95 for short-term follow-up observations, and p = 7.67 ×10−27 for long-term follow-up observations. The differences are extremely significant. Based upon calculations where 80% of the observations in a placebo group would be improved, the results are p = 9.27 × 10−14 for all observations, p = 3.76 × 10−10 for short-term follow-up observations, and p = 2.76 × 10−5 for long-term follow-up observations. These differences are also significant, and they all support the positive treatment results.
All three therapies included in this multitherapy could positively affect the results. However, regarding recent research material, laser therapy could possibly be the dominant therapeutic factor for the improvements. It is for future research to determine what effects each of these single therapies have and what the best combinations and doses are in the treatment of hyperacusis, as well as of other inner-ear disorders.
Conclusions
The combined therapy in this study resulted in a positive effect on pain thresholds for all hyperacusis patients. The long-term follow-up group was found to have significantly greater improvements in hyperacusis thresholds than the short-term follow-up group. Hyperacusis seems to be dependent on peripheral causes in the majority of cases treated in this study. No major complications were observed and there were neither severe nor permanent side effects from laser therapy, rTMS, or the use of antioxidants for ROS control.
Footnotes
Author Disclosure Statement
No competing financial interests exist.