
Abstract
Introduction
LLLT has been reported to bring positive effects to muscle activity in different areas, 4 –6 especially in health treatments involving the rehabilitation process or muscle activity. The strong and prolonged contraction of a muscle usually causes fatigue, resulting in the incapacity of the metabolic and contractile processes of the muscle fibers. This is due to the reduction of energy supply of the mitochondria in the muscle fibers, which quickly leads to fatigue. The electromagnetic irradiation in the red region, absorbed by the biologic tissues, may cause variations in the muscle activity because of changes in the ionic gradient, 7 in the concentration of adenosine triphosphate (ATP), 8 and in the activity of the Na+K+-ATPase. 9,10
According to the authors, biomodulation promoted by laser phototherapy is related mainly to the local blood-flow increase (or input) 11 –13 and neuromuscular activity. Muscle fatigue is a process resulting from inadequate tissue blood perfusion. 14 –18 Recent studies in animals showed that LLLT could reduce the debilitating influence of local fatigue on muscle force and possibly reduce muscle damage after strenuous exercises in a dose-dependent manner. 19 Leal Jr. et al. 20 observed in clinical studies that LLLT can delay the perceived onset of muscle fatigue and exhaustion, probably by local mechanisms including minimization of oxidative stress or a decrease in the production of reactive oxygen species. This study indicates the effect of LLLT in the improvement of muscle performance and opens a clinical window to the treatment of musculoskeletal conditions in which muscle fatigue is a precursor to pain. Studies with infrared laser verified that LLLT applied before high-intensity exercises can increase the removal of blood lactate and reduce muscle damage, providing athletes with faster muscle recovery between exercise sessions. These clinical findings indicate that LLLT before exercise can protect muscles against minor damage and inflammatory reactions after heavy exercise. 21,22
Recently, some authors noticed that, in some cases, LED (light-emitting diode, noncoherent electromagnetic irradiation) therapy provided better results in the tissue metabolic process than those obtained with laser therapy. 23,24
The light in the visible region of the electromagnetic spectrum produces photochemical effects at the cellular level. Such effects are related to the selective action in the tissues by the deposited luminous intensity. 25 Phototherapy using LEDs has been investigated only in studies involving in vitro or animal skeletal musculature. Studies with the objective of observing the effects of LED irradiation on muscle activity in humans still have not been performed. The purpose of the present study is to analyze electromyography, 25 –27 the effect of the noncoherent electromagnetic irradiation generated by LED in the red region on the activity, force, and fatigue time of the masseter muscle.
Materials and Methods
Subjects
Thirty test subjects of both genders (seven men, 23 women) aged 23 ± 3 years, randomly divided into three groups of 10 subjects each, took part in the study. The inclusion criteria were that subjects should have complete dentition, healthy temporomandibular joints, and be in general good health. The control signals of all test subjects without treatment (placebo or LED) were recorded. LED irradiation at the right masseter muscle was applied to all subjects. The groups received different amounts of LED irradiation on the right masseter: 1.044 J per point (G 1), 2.088 J per point (G 2), and 3.132 J per point (G 3). Measurements were performed before the irradiation to generate control signals and minimize individual variations. The control-signals record was considered standard information of a normal EMG signal (individualized information): root mean square (RMS), maximal and mean force (kgf), and time before fatigue.
Instrumentation
Biologic signals were obtained by using a 16-channel module (EMG System, Brasil Ltd), consisting of a signal conditioner with a bandpass filter with cut-off frequencies at 20–1,000 Hz, an amplifier gain of 1,000, and a common mode-rejection ratio >120 dB. The data were processed by using specific software for acquisition and analysis (EMG Analysis V1.01), a converting plate for A/D 16-bits signal to convert analog into digital signals with a sampling frequency of antialiasing 1.0 kHz for each channel, and an input range of 5 mV. Active bipolar superficial electrodes consisted of two rectangular parallel bars of Ag/AgCl (1 cm long, 0.2 cm wide, and 1 cm apart). These bars are coupled to a rectangular acrylic resin capsule 2.2 cm long, 1.9 cm wide, and 0.6 cm high, with an internal amplifier to reduce the effects of electromagnetic interference and other noises. 28
Electrodes were fastened to the skin and guided by bone prominences and the direction of the muscle fibers. 29 The skin was shaved and vigorously scrubbed with alcohol to reduce skin impedance before the attachment of the electrodes. The electrodes were then coated with a thin film of conductive gel and fixed with micropore adhesive tape to the midline of the muscle belly with the detection surface perpendicular to the muscle fibers. 30 In all procedures, the capture and analysis of EMG signals were carried out as recommended by the International Society of Electrophysiology Kinesiology (ISEK). 31
Procedure and data acquisition
The electrodes were fixed to the prepared skin of each subject at the medium point of the masseter muscle, parallel to the direction of the fibers, following the anatomic references of Perotto and Delagi. 32 The subjects had two isometric contractions, over two overlaid occlusal platforms, coupled to a load cell and to a device for biologic signal acquisition, as shown in Fig. 1. This contraction time is long enough to cause muscle fatigue. 33 –36 The EMG evaluation occurred after maximal isometric voluntary contraction (MIVC). Each contraction lasted 60 s and was produced by biting a piece of chewing gum placed bilaterally. Chewing gum was used to eliminate the discomfort of tooth contact. Patients were sitting safely on a comfortable chair, staring at a computer screen that exhibited the electromyographic signs. A clear and precise verbal command was given to the patients related to the muscle contractions and acquired signals. A computer screen was used as biofeedback to control the intensity of maximal voluntary contraction to eliminate subjective muscle effort.
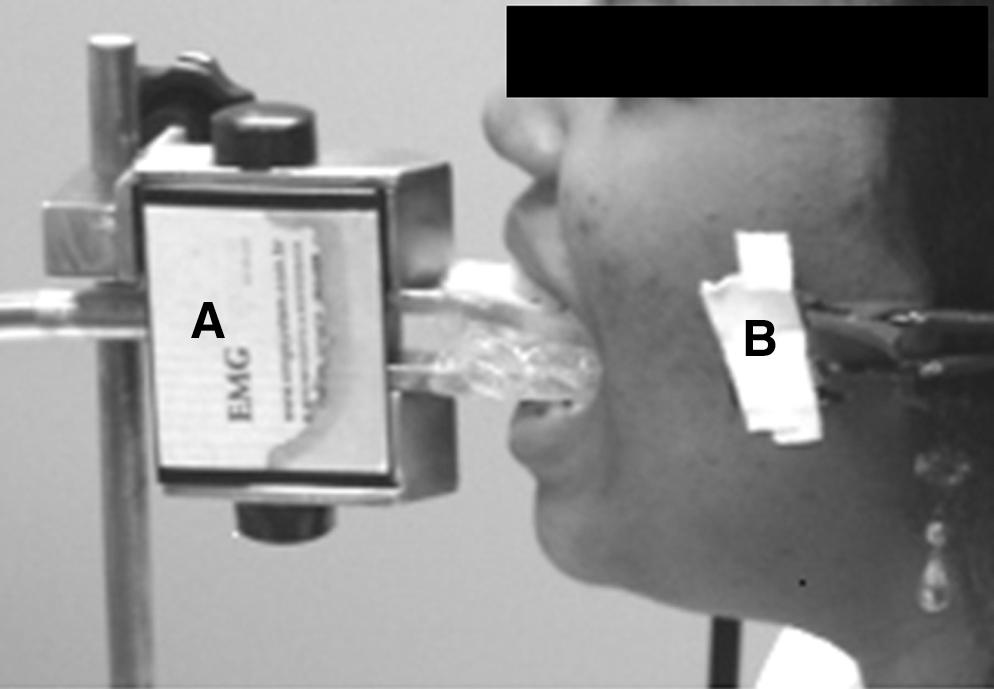
Volunteer during the acquisition of the electromyography signals.
The biologic signals of the first acquisition were considered control signals. After 5 min of muscle rest, 37 the right masseter muscle was irradiated. The left masseter muscle was maintained with placebo. The irradiation simulation on the left masseter was made with the equipment off (placebo procedure). A second signal acquisition (after irradiation or placebo procedure) was carried out 5 min after the irradiation.
The signals were sampled at a rate of 2,000 Hz per channel. To reduce possible interferences in the stimulus induction, the skin in the region of the masseter muscle was shaved and cleaned with alcohol. All subjects underwent the same procedure.
The electrical activity of the left (placebo side) and right (treated side) masseter muscles was monitored during 1 min, while the subject had an MIVC by closing the mouth with the platform of pressure on occlusion as antagonist (Fig. 1). The subjects were instructed to use maximal force during MIVC, with only one verbal command. After the first data acquisition, the subjects rested for 5 min. After that period, the LED was applied with the specific dose corresponding to the group (Table 1).
Wavelength: 640 nm with 40 nm full bandwidth at half maximum. G, group; CW, continuous wave.
The irradiation was made with LED equipment (FisoLED®, MM Optics, São Carlos, Brazil) at a 90-degree angle with the skin and slight pressure (Table 1). The irradiation was applied at eight points (distance of 1 cm between points) on the masseter muscle (transcutaneous). The irradiation started at the origin point (zygomatic process of the maxilla and zygomatic arch) of the masseter muscle and finished near its insertion (lower border and angle of the mandible). The mouth remained closed during the whole irradiation procedure.
Five minutes after irradiation, a new EMG record was carried out, by using the same acquisition protocol as the first register (Fig. 1). The signal treatment was performed by complete wave rectification, linear cover by Butterworth of the fourth level, with 5-Hz frequency, normalized in time base and amplitude. The amplitude was normalized by the mean. The RMS was calculated by using data recorded from the isometric activity during 60 s. The RMS (μV) values were considered the activity of the right masseter muscle (ARMM) and activity of the left masseter muscle (ALMM) to explain the results. The time before fatigue was measured when the signal was reduced to 20% below the initial intensity (μV), during experimental time acquisition (60 s). The maximal force (kgf max) was obtained 10 s after the MIVC was started. The mean force was calculated by using the values of intensity during 60 s.
One researcher applied the treatment (placebo or LED irradiation), and two others performed the electromyography examination. Two different groups of researchers were used so that no bias would exist in the analysis of the electromyography signals.
Ethical considerations
This research was approved by the Committee of Ethics in Research of UNIVAP (Universidade do Vale do Paraíba), under the protocol L189/2005/CEP, according to the resolution number 196/96 of the Brazilian National Health Council.
Statistical analysis
The data were analyzed with the GraphPad Prism Version 2.0 software, by using the Mann–Whitney test and the Wilcoxon test based on the rectified signal of paired samples (before versus after irradiation or the placebo condition). The level of significance adopted was 5% (p < 0.05). The Wilcoxon test is used to determine the magnitude of difference between matched groups.
Results
The activity of the right masseter muscle (ARMM) was analyzed before and after LED irradiation in the three different groups. The activity of the left masseter muscle (ALMM) was simultaneously analyzed; this side was considered not irradiated. A significant difference (p < 0.05) in the ARMM was observed after irradiation with 1.044 J per point. The same was observed for the left side (placebo). This result was not observed after the 2.088 J per point and 3.132 J per point irradiations, in which no significant change was noted in the root mean square (RMS) value.
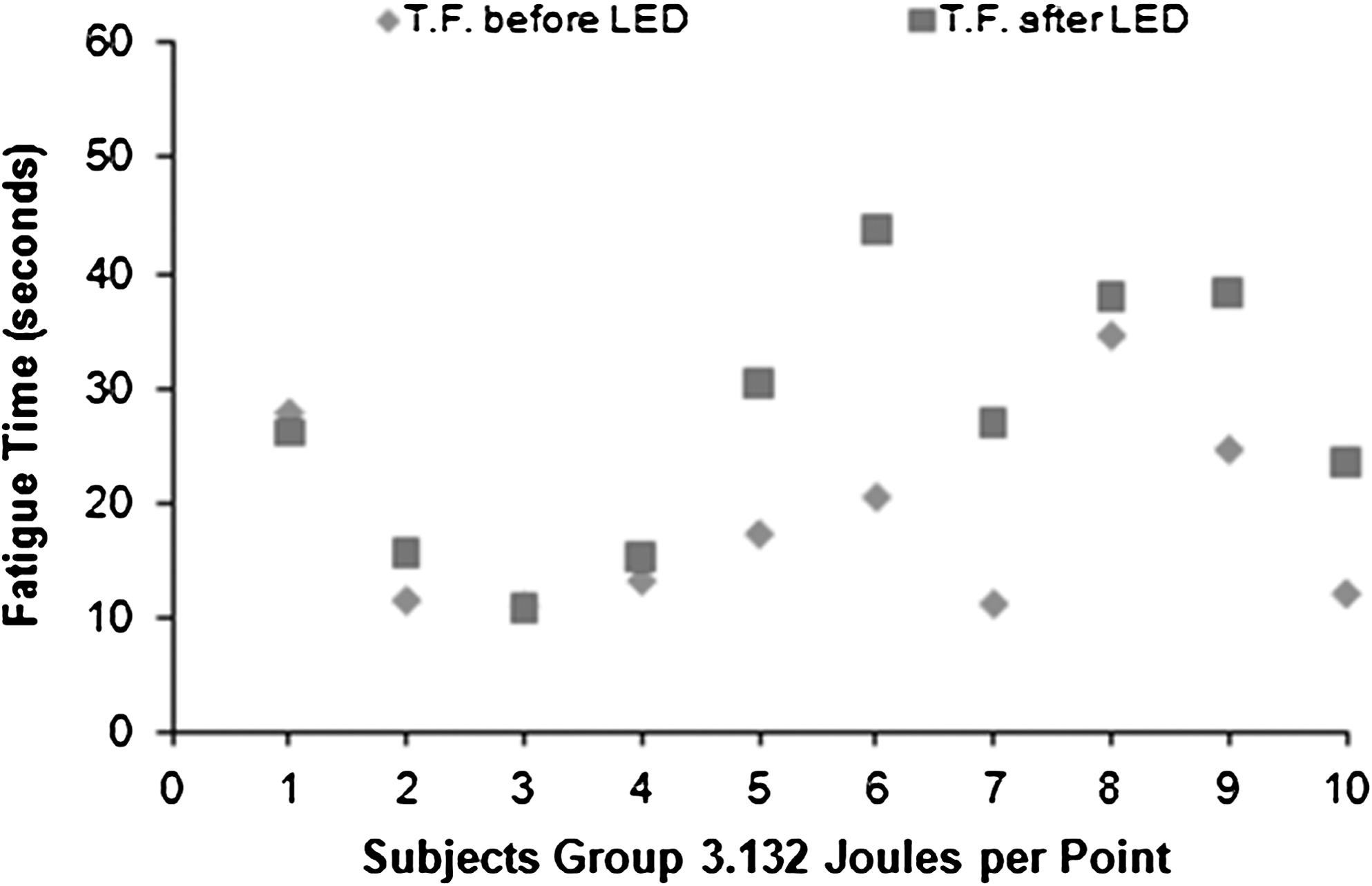
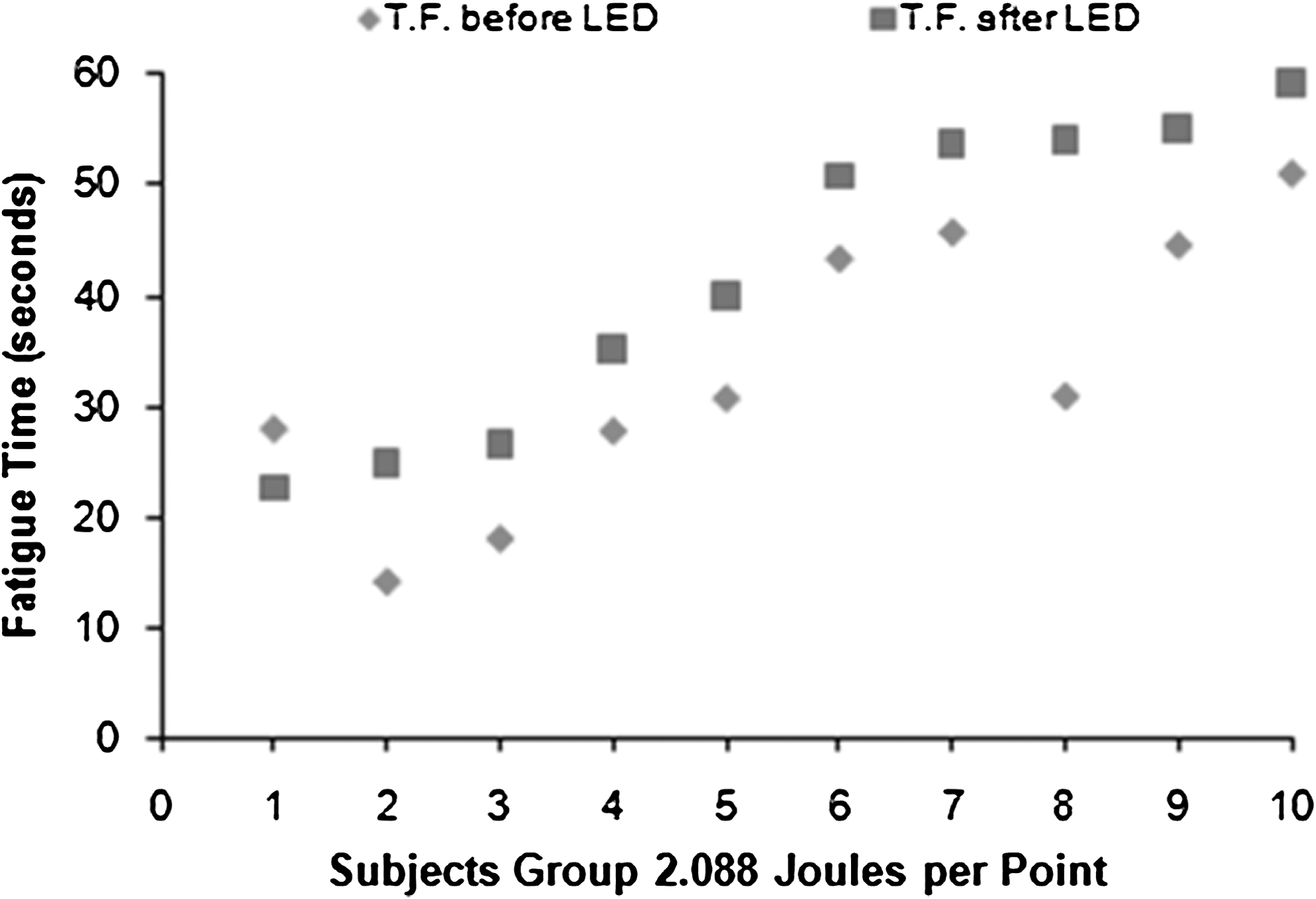
The resistance against fatigue increased significantly (p < 0.01) after the irradiation of the LED with 2.088 J per point. However, no significant difference was found between therapy with 1.044 J per point (Fig. 2) and 3.132 J per point (Fig. 3). No significant changes were observed in the maximal and mean force of the masseter muscle after the application of the LED with any of the three intensities.
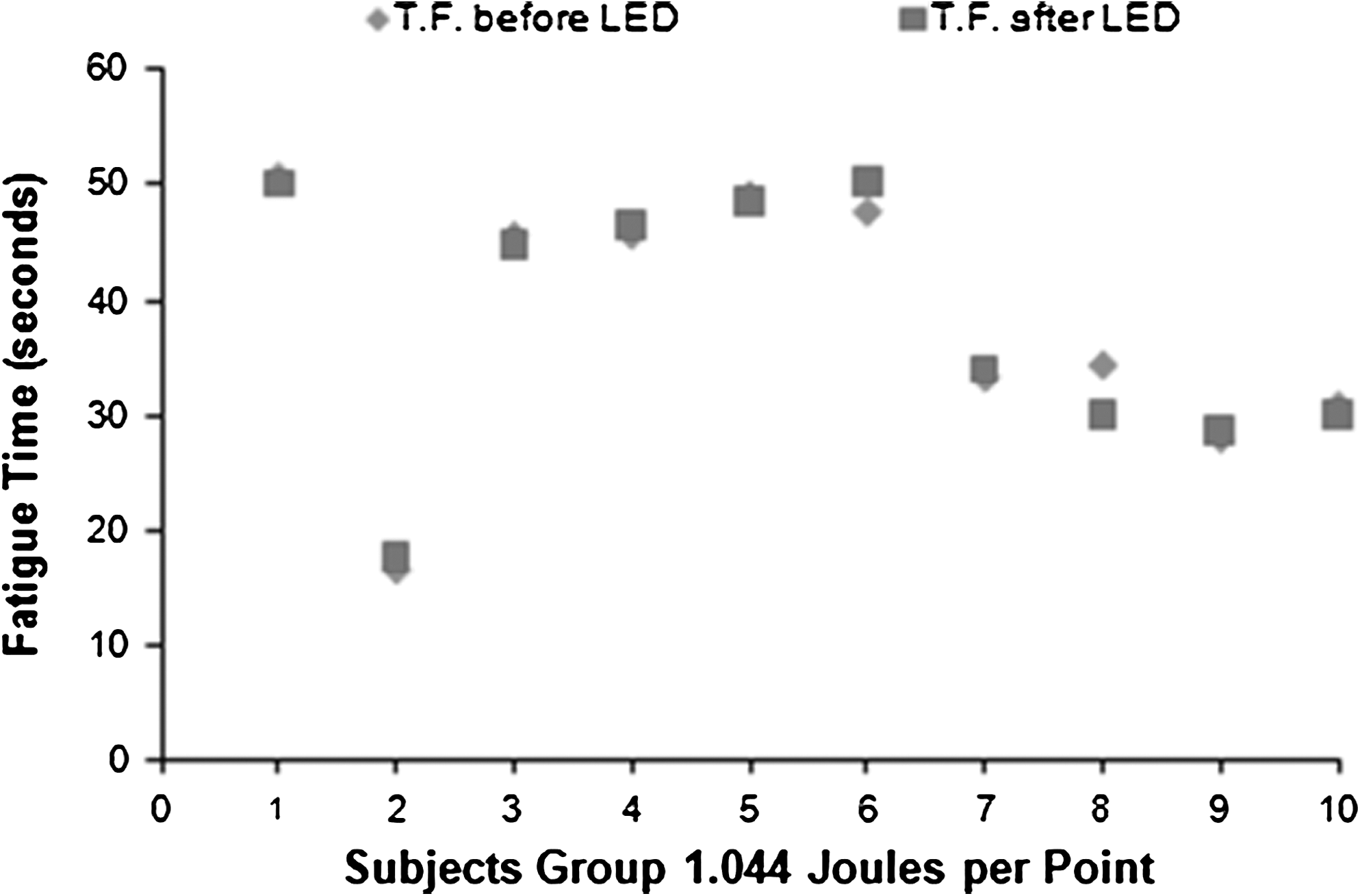
Comportment of the fatigue muscle during the date records (60 s, MIVC), before radiation (♦) and after radiation (▪) with LED. A small increase in the time before fatigue occurs in 50% of volunteers.
Comportment of the fatigue muscle during the date records (60 s, MIVC) before radiation (♦) and after radiation (▪) with LED. The increase in the time before fatigue occurs in 50% of volunteers. The other 50% did not have a significant increase.
Comportment of the fatigue muscle during the date records (60 s, MIVC), before radiation (♦) and after radiation (▪) with LED. The increase of the time before muscle fatigue occurs in 90% of the volunteers.
Table 2 summarizes the results of this study. The values of resistance to fatigue are also presented in Fig. 3, in which the tendency of the data before and after the therapy with LED at the intensity of 2.088 J per point is observed.
G1, 1.044 J/point group; G2, 2.088 J/point group; G3, 3.132 J/point group; ARMM, activity of the right masseter muscle (μV); ALMM, activity of the left masseter muscle (μV); FT: time before fatigue (seconds); kgf (max): maximum force (kgf); kgf (mean), mean force (kgf); *p < 0.05); control signal, without placebo or LED treatment.
Discussion
The influence of the electromagnetic irradiation in the red region over muscle activity has been demonstrated in animals 19,38 and clinical experiments. 20,38 This effect is characterized by increase of force and resistance to fatigue. 34 The introduction of LEDs in phototherapy has generated much controversy about its differences from and similarities to lasers. 39,40 Authors affirm that the photochemical effects are not related to light coherence, because coherence is lost in the first layer of skin, before light absorption by chromophores occurs. 41,42 Thus, few clinical studies used noncoherent light (LED) for muscle activity, 43 which motivated the current study.
In this study, the activity and process of fatigue of the masseter muscle after LED irradiation were analyzed. This muscle was chosen because of its significant role in the stomatognathic system.
The doses and numbers of points of irradiation, correlated with the concepts of spatial average energy fluence (SAEF), were established based on previous reports. 38,44
A significant difference in muscle activity was observed in the measurements of the left muscle activity after irradiation of 1.044 J per point of the masseter in the right side. This difference points to a possible systemic or placebo effect of the LED, but further studies are necessary to elucidate these findings.
The results presented show a significant difference in the right muscle activity before and after the irradiation with 1.044 J per point. These results indicate an activity of the noncoherent electromagnetic irradiation in the red region on the muscle recruiting and electrical activity. Neurotransmission is known to be directly influenced by the elevation of local temperature, which usually occurs with the increase of peripheral microcirculation. The superior RMS value, in the musculature irradiated with 1.044 J per point, may have been caused by the increase in the neurotransmission, elevation of ionic gradient, and increase in the intracellular energy increase (or input). 45,46
It is possible that increased blood perfusion on the masseter muscle after irradiation further improves muscle activity. This may be due to the increase in the local microcirculation when using LED irradiation. This suggestion about the LED irradiation effect was contributed by Queiroz et al., 47 using the same source of light and a similar dose. With a noncoherent light in vivo study with microscopy in real time, the authors observed an increase in the size of vessels 5 min after irradiation with red LED. According to the authors, these effects are overcome after 10 min. These results are similar to those of previous studies about the effects of laser irradiation on microcirculation. 38,48 –52
Even when an increase in muscle activity was observed with 1.044 J per point, no change was observed in force or time of fatigue. The results obtained with LED irradiation were not corroborated by previous studies using higher doses (5 J per point) of laser irradiation. 20 This response of the human muscle to LED irradiation enables the correlation between coherent red light (laser) and non-coherent red light (LED). The results presented in Fig. 2 show that 90% of the subjects had an increase in the time of postirradiation fatigue with 2.088 J per point, which was not observed after irradiation with 1.044 or 3.132 J per point. Such an increase suggests dose dependence. This finding suggests increased resistance to fatigue because of higher doses of irradiation energy per point with noncoherent red light. This fact confirms previous findings on the importance of the phototherapy dosimetry intended for positive biomodulation 38,53,54 by using coherent or noncoherent light on skeletal-muscle activity or fatigue prevention. The muscle force was not modified after irradiation. These effects show that this therapeutic modality has no negative collateral effect nor does it cause muscle lesion. 55
Conclusion
It can be concluded that the LED with emission of electromagnetic irradiation in the region of the red (640 nm) increases muscle activity without changing the time of fatigue and force with 1.044 J per point (total energy of the muscle, 8.32 J). The resistance to fatigue increased with 2.088 J per point (total energy of the muscle, 16.72 J). In short, LED can be used as a clinical tool to increase muscle activity (1.044 J per point) or prevent fatigue (2.088 J per point).
Footnotes
Acknowledgments
We thank DDSs Carolina Figueiredo and Flávia Bueno Gomes Moreira. We wish to thank the Foundation for the Improvement of Higher Education Personnel–CAPES for the financial support given through the PROSUP program.
Author Disclosure Statement
No competing financial interests exist.