
Abstract
Introduction
Spasticity acts as a negative factor in the masticatory masseter and temporalis muscles, causing hypertonia and limiting the opening range of the oral cavity. Severe neuromuscular dysfunction associated with spasticity and tonic bite reflex, with interposition of soft tissues between the dental arcades, results in soft-tissue trauma owing to the lack of protective reflexes caused by the mandible movement disorders resulting from spasticity. 3
Several management methods for oral trauma have been suggested, depending on the severity, frequency, and cause of injury. These include medication, behavioral techniques, and the use of oral appliances or dental extractions. 2,4,5
Laser use opens up new dimensions in treatment in a variety of clinical procedures based on the ability of different types of lasers to cut, coagulate, ablate, and vaporize biological tissues. 6
The aim of this study was to report a clinical case of surgical lip lesion removal owing to self-injurious behavior in a 9 year-old male quadriplegic, spastic, CP patient using high and low lasers in association.
Case Report
A 9-year-old male quadriplegic, spastic CP patient was referred to the Odontological Unit of Lar Escola São Francisco-Rehabilitation Center at the Federal University of São Paulo, São Paulo, Brazil, for odontological care owing to the presence of an extensive lower lip lesion resulting from self-injury (Fig. 1).
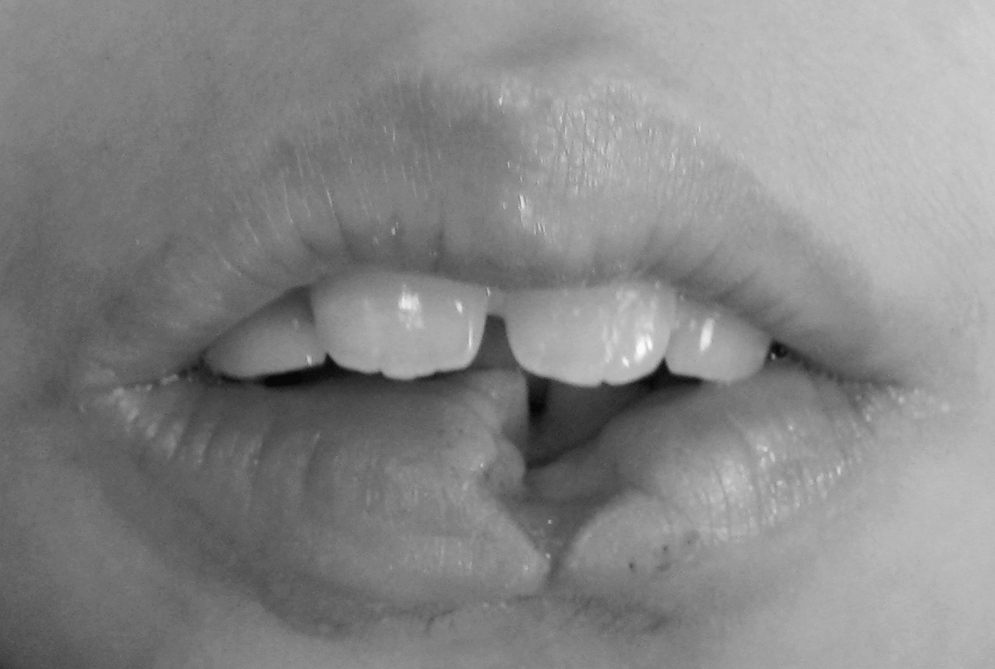
Aspects of the lower lip lesion resulting from self-injury.
According to the caregiver, the patient could not be fed due to oral pain resulting from traumatism in the lower lip caused by tooth 21. Clinically, extensive lower lip ulceration was observed, with loss of internal mucosa and lip vermillion tissues. Pale labial mucosa and a smooth depapillated tongue were also observed, suggesting the presence of anemia.
Besides severe motor impairment, the patient presented loss of vision and hearing. The patient was regularly administered baclofen (15 mg/day), clonazepam (1.5 mg/day), and phenothiazine (5 mg/day).
Preoperative laboratory exams, including a hemogram and a blood count coagulogram, were requested to investigate the patient's systemic conditions. The results showed low values for hemoglobin (Hb) concentration (6.5 g/dL) and hematocrit (Ht) (24.3%) and increased anisocytosis, moderate microcytosis, hypochromia poikilocytosis, and platelets (86,000/μL). Activated partial thromboplastin time (APTT) was 42.8 sec and international normalized ratio (INR) was 1.59.
A tissue-sample biopsy was performed on the internal mucosa of the lip. The results were characterized by the presence of inflammatory cells, epithelial cell proliferation, and increased angiogenesis. These results have important consequences for clinical outcome and treatment management.
Initially, treatment involved the use of low-level laser lherapy (LLLT) to improve the labial tissue healing of the lesion, which measured 2.2 cm externally and 3.4 cm within the internal mucosal (Fig. 2). Treatment was performed with a low-potency diode indium–gallium–aluminun–phosphide (InGaAlP) laser, 685 nm (Quasar®, Dentoflex, São Paulo, Brazil), with a continuous output power of 100 mW and a tip diameter of 1 cm2, using an energtic power and deposition density of 190 J/cm2 in scanning mode. The time of application was established and predetermined by the laser apparatus based on energetic power. A 24-h interval was used between the first and second administrations and a 7-day interval between the two subsequent applications.
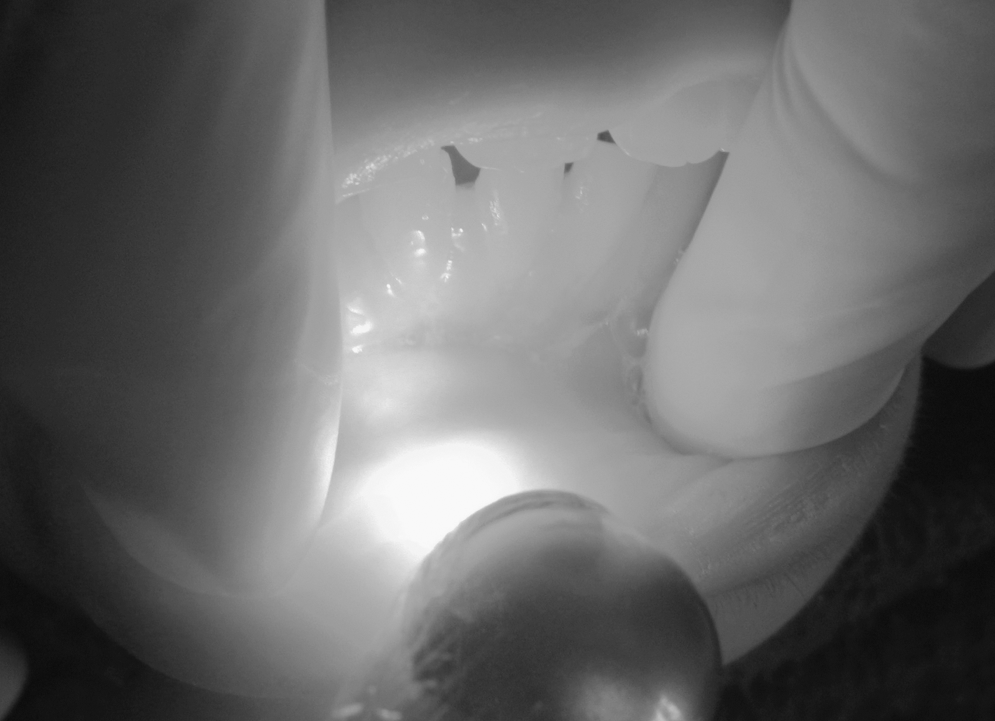
Low-level laser therapy application in the injured area.
Following this phase, because of the systemic conditions of the patient, a high- level laser was chosen to remove the remaining tissue. Antibiotic preoperative medication prophylaxis was used to avoid contamination and consisted of 250 mg of amoxicillin every 8 h initiated one day before surgery.
Intraoral antisepsis was performed with 0.12% gluconate chlorhexidine (Perioxidim®, Glaxo Welcome, São Paulo, Brazil) and extraoral antisepsis with 2% gluconate chlorhexidine (Methiolate®, Dm Pharmaceutical Industry Ltda, São Paulo, Brazil).
After local anesthesia with 4% Articaine® and epinephrine diluted at 1:100.000, the parameter of the lesion was outlined. The carbon dioxide (CO2) Laser Surgical System (Model: ML ϕ15-CD, ultra pulse, OptroniKa, Vienna, Austria) was used at a power setting of 5 W in continuous cutting mode. The hand piece was maintained at almost 5 cm perpendicular to the lesion, increasing the ablation power of the laser. Treatment was initiated in the medial area and proceeded to the labial commissure region. After removing the injured tissue, the base of the lesion was treated with an unfocused laser to promote homeostasis. The CO2 laser generates a lot of heat, which readily carbonizes tissue. Since this carbonized or charred layer is a biological dressing, it should not be removed (Fig. 3).

Aspects of the tissue after surgical removal with the CO2 laser.
Over the next 3 weeks, the patient received two applications of LLLT with a 24-h interval between the two administrations after the surgical laser application and a 7-day interval between two subsequent applications.
Two days later during postoperative follow-up, the caregiver did not report any bleeding episodes, and clinical observation verified that the surgical site presented normal characteristics.
An acrylic plate of autopolymerizing acrylic resin (JET, Classico Ltda,) was made that covered teeth 12, 11, 21, and 22 and was installed 4 days postsurgery. The plate was fixed with a photopolymerized resin system to decrease the risk of insufficient retention. A perforation was made in the plate that allowed a limited amount of dental floss to pass through to permit the caregiver access in case of displacement. This plate was used for 4 weeks.
After 30 days a significant reduction in injury to the oral tissues was observed; the region presented normal color and good healing conditions, so the plate was removed (Fig. 4).

Aspects of the lip 30 days after treatment.
Discussion
Self-inflicted oral trauma in individuals presenting neurological damage 1 with spastic 4 CP 7 is commonly observed in the form of lip chewing, 2,8 a behavior that causes painful lesions and interferes with proper sucking and feeding, thus putting the patient at risk of nutritional deficiency. This situation can also be a negative factor in self-esteem. 9
Currently, the therapeutic use of lasers (LLLT) on various types of buccal and oral lesions is considered one of the greatest technological advances in dentistry. 6 An improvement in the lesion area was observed after the laser therapy protocol at the beginning of the treatment.
The use of LLLT in animal models has suggested that it may have potential as an alternative therapy to anti-inflammatory drugs. 10,11 In a previous experiment, Albertini and colleagues 11 reported that red LLLT with a wavelength of 650 nm reduced rat paw edema similarly to a 1-mg/kg dose of diclofenac sodium, a nonsteroidal anti-inflammatory drug (NSAID), and a nonselective cyclooxygenase (COX) inhibitor. They also showed that wavelengths of 660 and 684 nm from red diode lasers are similarly effective at reducing edema formation during the first 4 h of inflammation. 12 A reduction in the density of inflammatory cells in injured tissue has previously been reported after LLLT in the wound healing of diabetic rats 13 and mouse pleurisy. 14 For the patient in this case, who presented severe motor impairment and was regularly administered three drugs daily, the use of LLLT was beneficial, since an improvement was observed in the lesion site without the use of NSAID or analgesic drugs.
Compared to conventional surgery, high-power lasers promote homogeneous tissue ablation and excellent homeostasis, thus facilitating visualization of the surgical site, providing greater surgical precision, and leading to a faster and safer procedure. Owing to their tissue vaporization properties, high-power lasers reduce the possibility of bacteremia, making postsurgery more comfortable and safer. 15
Carbon dioxide (CO2) laser energy has a very high water absorption coefficient, functions independently of tissue color, and is well absorbed by all soft tissue that is high in water content, with minimal effects on adjacent nontarget tissue. These properties make the CO2 laser ideal for surgical use on oral soft tissue. 16 Coagulation of small vessels is excellent, and postoperative bleeding is thus decreased. Sterilization of the operation site is virtually instantaneous, and acute inflammatory reaction is delayed and minimal. Trauma to the tissue is diminished, and scar formation is reduced to a minimum. Further, the use of the unfocused laser at the base of the lesion allows for immediate contraction of the surgical site. 17,18
Based on the properties described above, a CO2 laser was chosen to perform the surgery, a decision that also considered the patient's systemic conditions, leading to reduced bleeding, lower risk of bacteremia, and lower local trauma injury. To improve the process of wound healing (re-epithelization), an oral appliance was manufactured and installed. 2,4,5 When an appliance is indicated to prevent oral trauma, it must deflect traumatized tissues away from the occlusal table, permit mandibular movement, enable daily oral care, and permit healing of the injured tissues. It should also be easily fabricated, be comfortable, and pose no risk to the patient. 19
Conclusions
The association of high and low lasers to remove and heal a lip lesion owing to self-injurious behavior was effective and promoted an improvement in the patient's quality of life by establishing painless mastication.
Footnotes
Author Disclosure Statement
No competing financial interests exist.