
Abstract
Introduction
OM is seen in 75–99% of patients receiving conditioning regimens for HSCT, particularly in those who combine TBI and chemotherapy. 1,2 OM occurs with very high frequency following the conditioning regimen of HSCT, which usually uses high-dose chemotherapy with or without TBI. 3,4
High-dose chemotherapy administered as part of the preparative regimen for HSCT does not merely have a direct cytotoxic effect on the oral epithelium but is also associated with a wide range of local tissue reactions, including damage from reactive oxygen species and inflammatory cytokines and damage to submucosal connective tissues and vasculature, leading to injury or disruption of the mucosal barrier. The clinical presentation of OM consists of mucosal burning, erythema, ulceration, bleeding, and edema along with pain, 5 –7 symptoms that most commonly develop on the nonkeratinized mucosa of the floor of the mouth, tongue, buccal mucosa, and soft palate. 7 The maximum severity of OM occurs between 7 and 11 days post-transplant (D+7 and D+11). 3 Many patients experience significant pain requiring narcotic analgesia, and they subsequently often experience substantial weight loss and nutritional deficits. 8 Because of the recipient's immunosuppression, OM can cause severe complications such as microbial, viral, and fungal infections that can lead to septicemia. 6,9 The development of an active therapeutic intervention that can reduce the morbidity of OM would improve quality of life. 8 –10 The impact of OM on the course of HSCT therapy can be considerable at many different levels. 7,11 Sonis 7 has shown that an increase in the severity of OM is associated with higher fever, risk of infection, dependency on total parenteral nutritional, use of intravenous narcotic analgesic drugs, and mortality within the first 100 d.
To date, OM management has primarily been palliative, and OM prevention and therapy have been mainly empiric, encompassing a broad variety of approaches such as basic oral care, bland oral rinses, analgesics, antibiotics, cryotherapy, growth factors and cytokines, biologic mucosal protectants, anti-inflammatory agents, and complementary and alternative medicines, to cite but a few examples. 12 Many of these approaches have been potentially helpful, but because of certain shortcomings, the clinical studies that evaluated them could not find sufficient levels of evidence to recommend or suggest their use. Currently, there is no existing intervention that is completely successful in preventing OM, and consequently standard treatment for this complication has been symptomatic. 13
Therapeutic laser treatment, also referred to as low-level laser therapy (LLLT), was introduced by Mester and colleagues. 14 Considerable basic research has been undertaken since the 1970s. There have been more recent investigations, in particular with animals, 15,16 and some well-controlled clinical studies in the field of dentistry. 17,18 LLLT is characterized by low-intensity red or near-infrared light used in such a way that the observed biologic effect is attributed to nonthermal events. 19 It is reported to produce basic effects such as analgesia, anti-inflammatory activity, and biomodulation. 20 –22 Previous reports showed its influence on protein synthesis and the number, growth, and differentiation of cells when applied to different tissues. 23 However, the biochemical response and the effects at a cellular level are not well understood. 22 Helium-neon (He-Ne) laser (632.8 nm) treatment is the most frequently studied form of LLLT for the prevention or reduction of OM and the oral pain associated with cancer therapy. Research is currently underway on the use of diode lasers with wavelengths ranging from 650 to 905 nm 24 ; however, findings are often contradictory in terms of the presumed benefits.
A number of clinical studies have reported the benefit of low-level lasers to prevent OM in HSCT 3,25 –28 and in head and neck radiotherapy patients. 29 –31 Unfortunately, the basic parameters of LLLT reported in these studies varied significantly with regard to types of laser sources (HeNe, GaAlAs, InGaAlP, and GaAs), wavelengths (632.3, 650, 660, 780, 810–820, and 901 nm), and energy densities. In this trial we investigated the clinical effects of the InGaAlP (660 nm) laser on the prevention of OM induced by conditioning regimens in HSCT patients.
Patients and Methods
From September 2004 to October 2005, patients admitted to the Bone Marrow Transplantation Unit at the Araújo Jorge Cancer Hospital/Goiás Fight Cancer Association-Brazil (HAJ/ACCG) who were at risk of developing OM were approached to participate in this study.
The research was performed in compliance with the Research Ethics Committee of the HAJ/ACCG. On the day of admission for the transplantation, patients who consented to participate were divided into two groups, one that would receive laser therapy prophylactically (laser group) and one that would not (control group), based on computer-generated randomization. The study was also conducted in full accordance with the ethical principles of the World Medical Association Helsinki Declaration.
The study involved 42 patients undergoing HSCT. The laser group (n = 21) received the hospital oral hygiene protocol (instructions for brushing, flossing, and rinsing), and low-intensity 660 nm laser irradiation was performed prophylactically. The control group (n = 21) received the hospital oral hygiene protocol only.
Inclusion criteria
Patients scheduled to receive myeloablative conditioning regimens utilizing chemotherapy with and without TBI were included. Eligible subjects received a thorough explanation of the study design and its implications and signed informed consent documents. Subjects eligible for inclusion in this study were between 4 and 64 years of age and were able to cooperate with the treatment protocol. Their oral mucosa was intact on the first day of conditioning, and they were able to carry out acceptable routine oral care per standard protocol.
Exclusion criteria
Patients were excluded from the study if they had active oral, viral, bacterial, or fungal infections or had active oral bleeding that was uncontrollable during laser therapy. In addition, patients were excluded if they were receiving drugs for the treatment and/or prevention of mucositis.
Oral examination and protocol of oral hygiene
Before hospitalization
Before the preparative regimen, a dentist examined the oral cavity of all patients. Potential sources of infection were assessed and completely eliminated in all patients. Patients from both the control and laser groups received guidance on oral hygiene (instructions for brushing, flossing, and rinsing). They were given mouth rinses with an ethanol-free 0.12% chlorhexidine solution, toothpaste, a soft tooth brush, and dental floss.
During hospitalization
Patients were encouraged to brush their teeth after every meal, use dental floss once a day, and wash their mouth with an ethanol-free 0.12% chlorhexidine solution twice a day.
Conditioning regimens
The characteristics of the conditioning regimens are summarized in Table 1. Patients received 200 mg fluconazole intravenously every 12 h from 2 d prior to transplant (D-2) and 500 mg/m2 acyclovir intravenously every 8 h from D-2 until neutrophil recovery.
Samples for blood cultures were collected by central catheter and peripheral veins in case of febrile episodes, and this was followed by empiric therapy with broad-spectrum antibiotics.
Busulfan 12 mg/kg and cyclophosphamide 120 mg/kg (busulfan 3 mg/kg/d for 4 d and cyclophosphamide 60 mg/kg/d for 2 d).
Busulfan 16 mg/kg and cyclophosphamide 120 mg/kg (busulfan 4 mg/kg/d for 4 d and cyclophosphamide 60 mg/kg/d for 2 d).
Cyclophosphamide 120 mg/kg (60 mg/kg/d for 2 d) and TBI 12 Gy × 6, every 12 h for 3 d.
Carmustine 300 mg/m2/d for 1 d; cytarabine 400 mg/m2/d for 4 d; etoposide 200 mg/m2/d for 4 d, and melphalan 120 mg/m2/d for 1 d.
TBI, total body irradiation.
Oral mucositis evaluation
The same investigator scored the degree of OM. The mucositis examinations were carried out by a trained clinical medical doctor (an oncologist) who was blind to the randomization allocation, using the World Health Organization (WHO) scale 32 : grade 0 = no mucositis; grade 1 = erythema without lesions; grade 2 = ulcers, but able to eat; grade 3 = painful ulcers but able to eat liquid food (nutrition), with analgesia for support; grade 4 = requires parenteral or enteral support and continuous analgesia. An oral examination was performed daily, after laser treatment, from D-2 until the wounds healed or until neutrophil recovery (granulocytes = 500/mm3).
Parameters such as pain, use of opioids, and parenteral support were not evaluated.
Laser parameters
In the laser group, oral mucosa was irradiated with an InGaAlP diode laser. The parameters used were 660-nm wavelength, output power of 40 mW, and an energy density of 4 J/cm2 measured at the fiber optic end with 0.04 cm2 of section area. Irradiations were done in contact using punctual irradiation. A dentist trained in laser irradiation procedures provided the laser treatment regimen and was the only member of the team who knew the group to which the patient had been randomized. The laser was applied in contact using punctual irradiation, for 4.0 sec per point, using 0.16 J of energy per point, with evenly distributed exposure to sites (upper lip, lower lip/lip mucosa, buccal mucosa right and left, lateral tongue right and left, ventral tongue, and mouth floor), side by side, touching the mucosa, totaling 10 points per region. The total energy applied per day was 12.8 J. Daily sessions began on D-4 and continued through to D+4. There was a total of nine treatment days, and laser therapy was administered at approximately the same time each day. Before application of the laser, the tip was wrapped in polyvinyl chloride film and then disinfected with a 70% alcoholic solution. For eye protection all patients wore eyeglasses to totally block out the light during application of the laser. When patients of control group presented OM grade 3, they all received laser treatment with 4 J/cm2.
Statistical analysis
Patient characteristics were compared across both groups (control and laser) using the chi-square test for continuous variables (age, sex, and stem cell source). The mucositis scores obtained for patients were compared using the WHO mucositis scale. A Mann–Whitney test was used to compare the OM grade across both groups (control and laser). The occurrence (grade 0/grade > 0) and the intensity (grade 3/grade >3) of OM in both groups were compared, using the chi-square test. All p values <0.05 were considered statistically significant.
Results
From September 2004 to October 2005, 56 patients were admitted to the Bone Marrow Transplantation Unit of HAJ/ACCG. Fourteen patients were excluded from the study; 12 had autologous and not myeloablative transplantation, one had oral mucosa that was not intact on the first day of conditioning, and one required oral tracheal intubation on D-2.
The remaining 42 patients all completed the study. The laser application was well tolerated and no side effects occurred. Table 1 summarizes the patient characteristics.
Mucositis evaluation using WHO criteria
Based on the WHO scale, laser group patients presented less OM. Results showed that 66.7% of patients were free of ulcers (grades 0 and 1), 33.3% developed mucositis grade 2 when treated with laser therapy, and none showed mucositis grades 3 and 4. In the control group, 95.2% (20 out of 21) developed mucositis and 4.8% of patients were free of ulcers (grade 0). It is important to note that 14 of 21 patients (66.7%) in the control group had small ulcers (grade 2) and that in the laser group, 7 of 21 (33.3%) had grade 2 mucositis. In the control group, 6 of 21 (28.5%) presented OM grade 3, and in the laser group grade 3 mucositis did not occur (0%). The difference between the two groups in relation to the OM grade was statistically meaningful (p < 0.001) (Fig. 1).
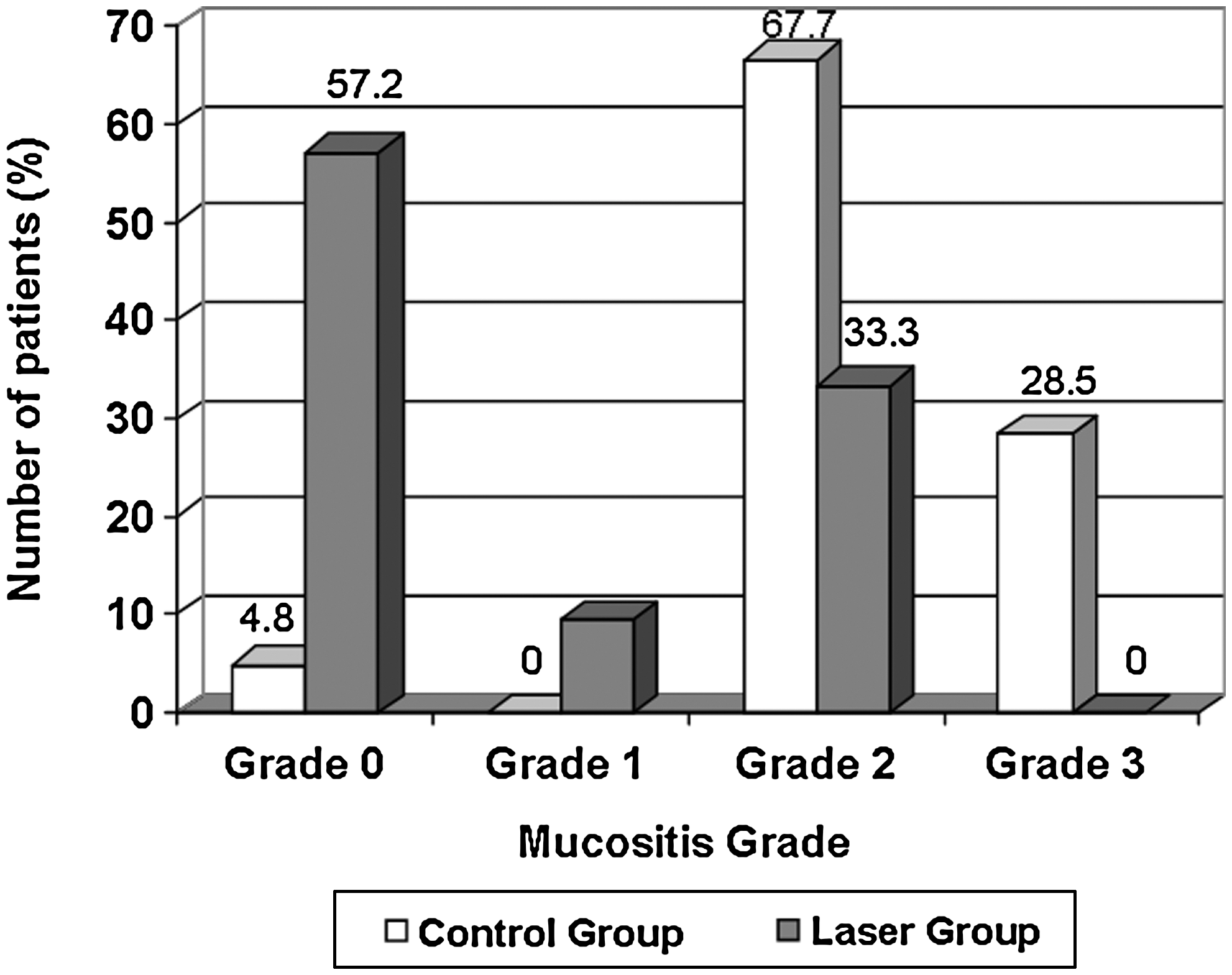
Differences between both groups in relation to the oral mucositis grade.
Discussion
OM is a common complication of the HSCT conditioning regimen. The complete pathophysiology of OM has still not been well defined. Prevention and treatment of OM remain as challenges for health-care providers. 7,9
In this study, patients underwent allogeneic and autologous transplantation, as did those in the studies of Antunes et al. 26 and Schubert et al., 27 whereas in the study of Cowen et al. 3 all patients underwent autologous HSCT. In the study of Barasch et al., 25 21 patients were submitted to autologous HSCT and one patient to allogeneic HSCT. Since allogeneic transplantation leads to more severe OM than does autologous bone marrow transplantation, our population may be considered more vulnerable and the results more remarkable. However, TBI being applied to all patients in the study by Cowen et al. 3 may counterbalance the difference.
In our study, both groups were similar in terms of the conditioning regimens. Even the two laser group patients who had received a conditioning regimen with TBI were free of OM.
The results of our study show that laser application reduced the occurrence and intensity of OM (Fig. 1), with 66.7% of patients in the laser group being free of ulcers when LLLT was performed preventively. No patients in the laser group developed OM grades 3 or 4, which shows a significant reduction in the intensity of OM. Additionally, no patients presented OM until D+4, while the laser treatment was applied. This shows the possible beneficial effect of laser as a preventive tool in HSCT patients.
The efficacy of this method for the prevention of radiation-induced OM has also been confirmed in studies by Bensadoun et al., 29 Maiya et al., 30 and Arora et al. 31 In these studies, the mucositis grades were significantly lower in the study group than in the control group, showing decreases in grades 2 and 3. Although the study was not carried out on HSCT patients, the results were in keeping with previous observations. In these trials, mucositis was evaluated by WHO criteria.
In the Cowen et al. 3 study, 30 patients received continuous laser illumination with a 632.8-nm wavelength, 25-mW output power, and 1.5 J/cm2 energy density, from D-5 to D-1. In their study, Barasch et al. 25 applied the same wavelength and power, and 1 J/cm2 of energy density from D-1 to D+3. In our trial both a higher energy density (4 J/cm2) and a longer period of administration (from D-4 to D+4) were applied. In marked contrast to previous data, this strategy proved to be highly effective: 57% of patients did not present any ulcers after HSCT compared with 100% of patients in the studies by Cowen et al. 3 and Barasch et al. 25 In a study by Schubert et al. 27 that used a prophylactic model for laser therapy, 70 subjects were randomized into one of two laser treatment arms (InGaAlP, 650 nm, 40 mW, and GaAlAs, 780 nm, 60 mW) from D-7 to D+2 or a placebo therapy group. Prophylactic LLLT with a 650-nm diode laser was more effective for decreasing mucositis severity than therapy with a 780-nm laser. Jaguar et al. 28 compared two groups of patients submitted to HSCT: group L+(n = 21 autologous + 3 allogenic) received irradiation with a diode InGaAlP (660 nm, 10 mW, 2.5 J/cm2) from the start of conditioning to D+2 while group L− (n = 23 autologous + 2 allogenic) received no laser therapy. All patients of L+ used intraoral cryotherapy which started 5 min before chemotherapy and continued for 30 min. In groups L+ and L− the authors observed that 50% and 84% of patients, respectively, had OM grade 3/4. Antunes et al., 26 with results similar to ours, used continuous laser illumination with a 660-nm wavelength, 50 mW of power, and 4 J/cm2 of energy density from D-7 until neutrophil recovery and reported that 63.2% of patients did not experience OM, 31.5% presented with OM grade 2, and 5.3% presented with OM grade 4. Our data suggest that both high laser energy density and the duration of the application may be pivotal for the outcomes of LLLT preventive treatment.
The findings from this study are consistent with Cowen et al., 3 Barasch et al., 25 Antunes et al., 26 and Schubert et al. 27 and are supportive of the studies by Bensadoun et al., 29 Maiya et al., 30 and Arora et al., 31 and they generally support the efficacy of LLLT in preventing cancer therapy–induced OM in patients undergoing HSCT. Our data confirm the efficacy of LLLT in preventing OM induced by conditioning regimens in HSCT patients.
Considerably more research is needed to define the ideal LLLT wavelength, fluence, intensity, and other treatment variables. In particular, laboratory studies need to be undertaken to explore where the energy is deposited in the tissue; how the laser energy interacts with intracellular organelles, structures, and metabolic processes; and what the ultimate tissue responses are to laser light exposure.
Conclusion
This study concluded that preventive laser therapy is beneficial in reducing the occurrence and intensity of OM in HSCT patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.