
Abstract
Introduction
Some therapies such as ultrasound (US) and low-level laser therapy (LLLT) are common modalities used for treating several skeletal muscle conditions. 6,7 Both therapies effectively reduce postinjury inflammatory processes, stimulate the formation of new blood vessels, and accelerate soft tissue healing. 8 –10 Therapeutic US is a type of mechanical energy that is transmitted through and into living tissues in the form of acoustic pressure waves. It has been theorized that micromechanical strains, produced in biological tissues by such pressure waves, may result in biochemical events that accelerate tissue healing. 11 That therapeutic modality is well established, approved by the U.S. Food and Drug Administration, and in frequent use. 7 In muscle tissues, US can stimulate proliferation of myogenic precursor cells, myogenic cells, and fibrillar collagen. 4,5 Piedade et al. 4 found that US could stimulate myoregeneration and collagen deposition, as well as accelerate tissue regeneration process in an experimental model of lacerative gastrocnemius muscle lesion.
The action of LLLT is based on absorption of light by tissues, which generates a series of modifications in cellular metabolism. When laser is applied to tissues, light is absorbed by photoreceptor chromophores located in the cells. Once absorbed, the light can modulate specific biochemical reactions inside the cell and stimulate a series of mitochondrial chain reactions resulting in ATP synthesis. 8,10
Such effects are known to increase the synthesis of DNA, RNA, and cell-cycle regulatory proteins, therefore promoting cell proliferation. 6 Some studies have demonstrated that LLLT promotes skeletal muscle regeneration in mammals 12 and amphibians. 13,14 In vitro studies evaluating the differentiation process in muscle tissues showed increased myoblast motility and muscle fiber formation delay resulting from low-energy laser irradiation. 15 Amaral et al. 12 observed that 632.8-nm HeNe laser at a 2.6 J/cm2 dose increased mitochondrial density and muscle fiber density of rats.
Despite the positive effects of US and LLLT on tissue regeneration, the mechanism by which such therapies act on injured muscle tissue is not fully understood, and their use as a treatment modality is still controversial. 16 Moreover, the use of a wide range of doses by different authors and the lack of standardized experimental conditions make it difficult to compare published results. Also, given that some inflammatory mediators such as prostaglandin and arachidonic acid products play an important role during tissue repair, it is essential to evaluate the effects of LLLT and US on cyclo-oxygenase-2 (COX-2) expression during the process of muscle repair. Cyclo-oxygenase is a key enzyme in the conversion of arachidonic acid to prostanoids. The expression of COX-2 is relevant to many pathological processes, including inflammation, tissue repair, and ultimately carcinogenesis. 17 Since US and LLLT are widely used for accelerating tissue healing process, the aim of this study was to compare their effects on injured skeletal muscle healing after cryolesion by means of histopathological analysis and immunohistochemistry for COX-2.
Methodology
Animals
Thirty-five Wistar male rats (weighing 300 ± 20 g) were maintained under controlled temperature (22 ± 2°C) and light–dark periods of 12 h, with free access to water and commercial diet. All animal handling and surgical procedures were strictly conducted according the Guiding Principles for the Care and Use of Laboratory Animals. This study was approved by the Committee of the Federal University of São Paulo. Animals were randomly distributed into four groups: control group (n = 5), uninjured and untreated animals; injured control animals (n = 10) with muscle injury and no treatment; LLLT treated (n = 10), animals with muscle injury treated with LLLT; and US treated (n = 10), animals with muscle injury treated with US.
Surgery
Animals were anesthetized with xylazine (Syntec, 20 mg/kg, intraperitoneal) and ketamine (Agener, 40 mg/kg, intraperitoneal) and exposed to cryolesion of the muscles. The cryolesion consisted of two freeze–thaw cycles of the muscle in situ. Freezing involved applying the flat end (0.4 by 0.4 cm) of a piece of iron, precooled in liquid nitrogen, to the surface of the proximal and distal third parts of the muscle and maintaining it in position for 10 sec (twice). Once the muscles thawed, the wounds were closed with polyamide threads (6-0), and thereafter, animals were kept for several hours on a warm plate (37°C) to prevent hypothermia.
Treatments
Treatments started 24 h postsurgery and were repeated every 48 h, for a total of 6 sessions. Low-intensity pulsed US [Exogen; 1.5 MHz, 1:4 duty cycles, intensity spatial average, temporal average (SATA) 30 mW/cm2, 20 min/session, stationary mode application] was used. 7 Also, a low-energy GaAlAs laser (Tera laser, DMC®, São Carlos Equipment) was used at 830 nm (continuous wave, 0.028-cm2 beam diameter, 1.07 W/cm2, 50 J/cm2, 30 mW) with an irradiation time of 47 sec (total energy per point 1.41 J). The irradiation was performed in one point, above the area of the injury, through the punctual contact technique. On day 13 postinjury, animals were sacrificed (with profound sedation and overdose of ketamine and xylazine, 0.5 mL each) in order to extract their tibialis anterior muscles.
Histopathological analysis
Muscles obtained from all experimental and control groups were washed immediately with saline and then fixed in 10% buffered neutral formalin solution. After fixation, the muscle tissue was embedded in paraffin, sectioned, and stained with hematoxylin and eosin. Histopathological evaluation was carried out under a light microscope. The analysis was performed by two independent reviewers (DAR and ACMR) who were blinded to the treatment. The qualitative analysis considered any changes at the injury site, such as presence of inflammatory process, granulation tissue, necrosis, or tissues undergoing hyperplasia, metaplasia, and/or dysplasia. Semiquantitative analyses of muscle sections were done as described elsewhere with minor modifications. 18 Briefly, the findings were graded as follows: no changes;+, mild (focal myocyte damage or small multifocal degeneration with slight degree of inflammatory process); ++, moderate (extensive myofibrillary degeneration and/or diffuse inflammatory process); or +++, marked (necrosis with diffuse inflammatory process). Based on histopathological changes in muscle tissue, rats were divided into three groups: group A (no changes); group B (mild changes); and group C (moderate and/or severe changes).
Immunohistochemistry
Serial longitudinal muscle sections of 4 μm were deparaffinized in xylene and rehydrated in graded ethanol, then pretreated by microwave (Brastemp) with 10 mM citric acid buffer (pH = 6) for three cycles of 5 min each at 850 W for antigen retrieval. The material was pre-incubated with 0.3% hydrogen peroxide in phosphate-buffed saline (PBS) for 5 min for inactivation of endogenous peroxidase, and then blocked with 5% normal goat serum in PBS for 10 min. The specimens were then incubated with anti-COX-2 antibody (Santa Cruz Biotechnology) at a concentration of 1:400. Incubation was carried out overnight at 4°C and was followed by two washes in PBS for 10 min. The sections were then incubated with biotin-conjugated secondary antibody (anti-rabbit IgG) (Vector Laboratories) at a concentration of 1:200 in PBS for 1 h. The sections were washed twice with PBS before application of preformed avidin biotin complex conjugated to peroxidase (Vector Laboratories) for 45 min. The bound complexes were visualized by the application of a 0.05% solution of 3-3′-diaminobenzidine and counterstained with Harris hematoxylin. For control studies of antibodies, the serial sections were treated with rabbit IgG (Vector Laboratories) at a concentration of 1:200 in place of the primary antibody. Additionally, internal positive controls were performed with each staining bath.
Immunohistochemical data were evaluated by two experienced pathologists (DAR and CCM) under subjective morphologic analysis as established in previous studies conducted by our group. 19,20 Briefly, the analysis was performed under subjective morphological analysis considering the presence of immunopositive cells in the tissue.
Statistical analysis
Data from semiquantitative histopathological analysis were evaluated using one-way ANOVA, followed by the post hoc Student–Newman–Keuls method. Numbers were attributed to the different classifications: no changes were classified as 0; mild was classified as 1; moderate was classified as 2; and marked was classified as 3. The level of statistical significance was defined as p < 0.05. Statistical evaluation was carried out using GraphPad Prism 4 (GraphPad Software).
Results
Histopathological findings
Figure 1A shows the muscle tissue without any injury. Histopathological findings from injured control rats showed destroyed zones with interstitial edema and neutrophil granulocytes, characterizing acute extensive myofibrillary degeneration (Fig. 1B). Nevertheless, injured animals irradiated with LLLT presented mild to minor degenerative changes of muscle tissue (Fig. 1C). Moreover, a high cell concentration was noticed. In the same way, US was able to reduce tissue injuries (Fig. 1D); however, the effects were less pronounced when compared with the effects of LLLT.
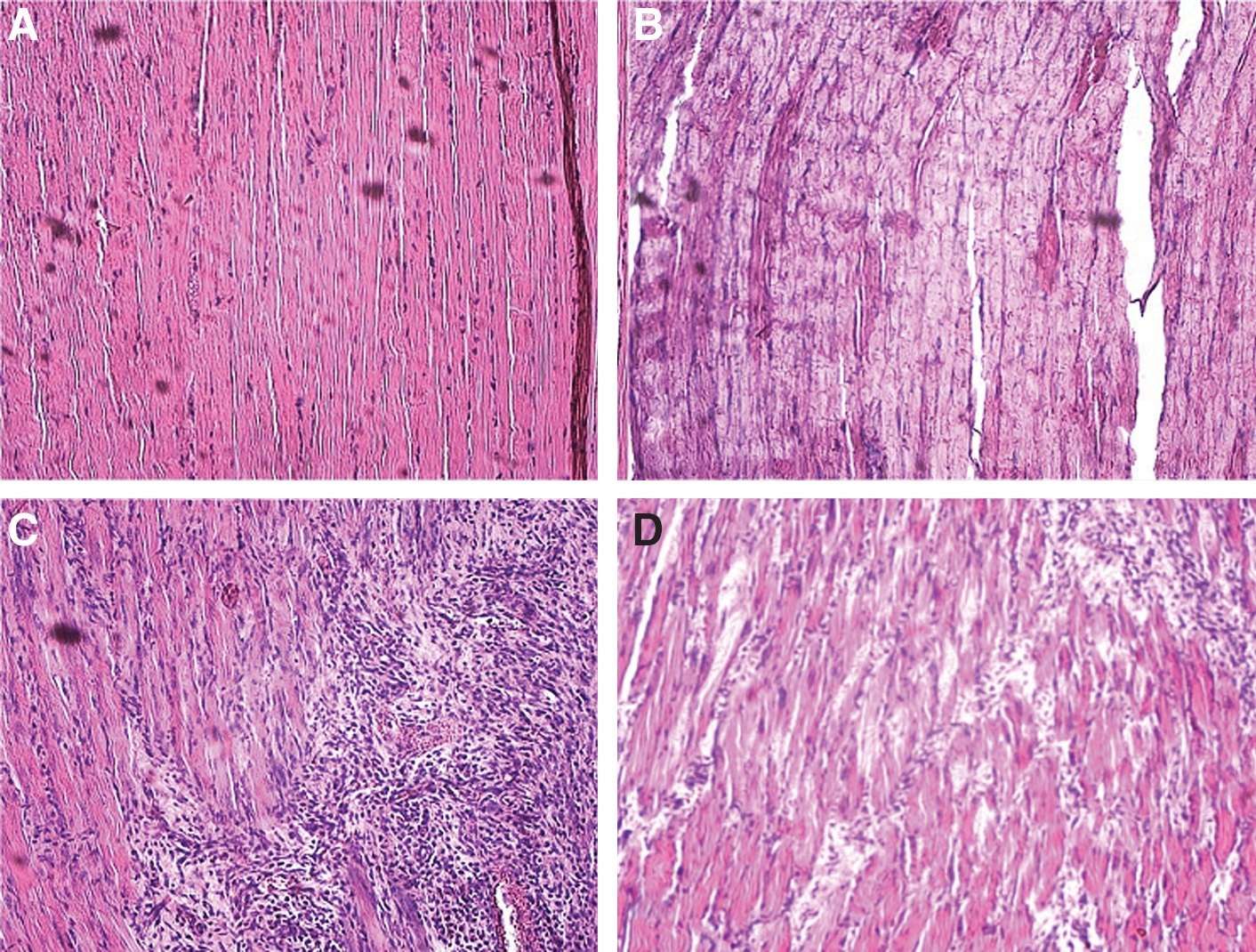
Photomicrographs of
Table 1 shows the semiquantitative analysis of the effects of LLLT and US treatments on the degree of histopathological changes produced in the injured muscle tissue. All injured control animals showed severe histopathological modifications. In the LLLT group, two animals were classified as C, with severe histopathological modifications and eight as B (mild). Interestingly, four animals of the US group were classified as C and six as B.
A, no histopathological changes; B, mild histopathological changes; C, moderate or severe histopathological changes.
p < 0.05 vs. control.
Immunohistochemistry
COX-2 expression was detected either in the cytoplasm or in the nucleus of the muscle cells. A larger number of COX-2 positive cells were found in rats exposed to cryolesion only (Fig. 2A). By contrast, COX-2 immunoexpression was less intense in the LLLT group when compared to the control (Fig. 2B). The same scenario occurred in the group exposed to US, i.e., fewer cells presented COX-2 immunoreactivity compared with the control (Fig. 2C). Figure 3 shows the high magnification of COX-2 immunoexpression, denoting positive expression in myofibrillar cells in the laser-irradiated group.
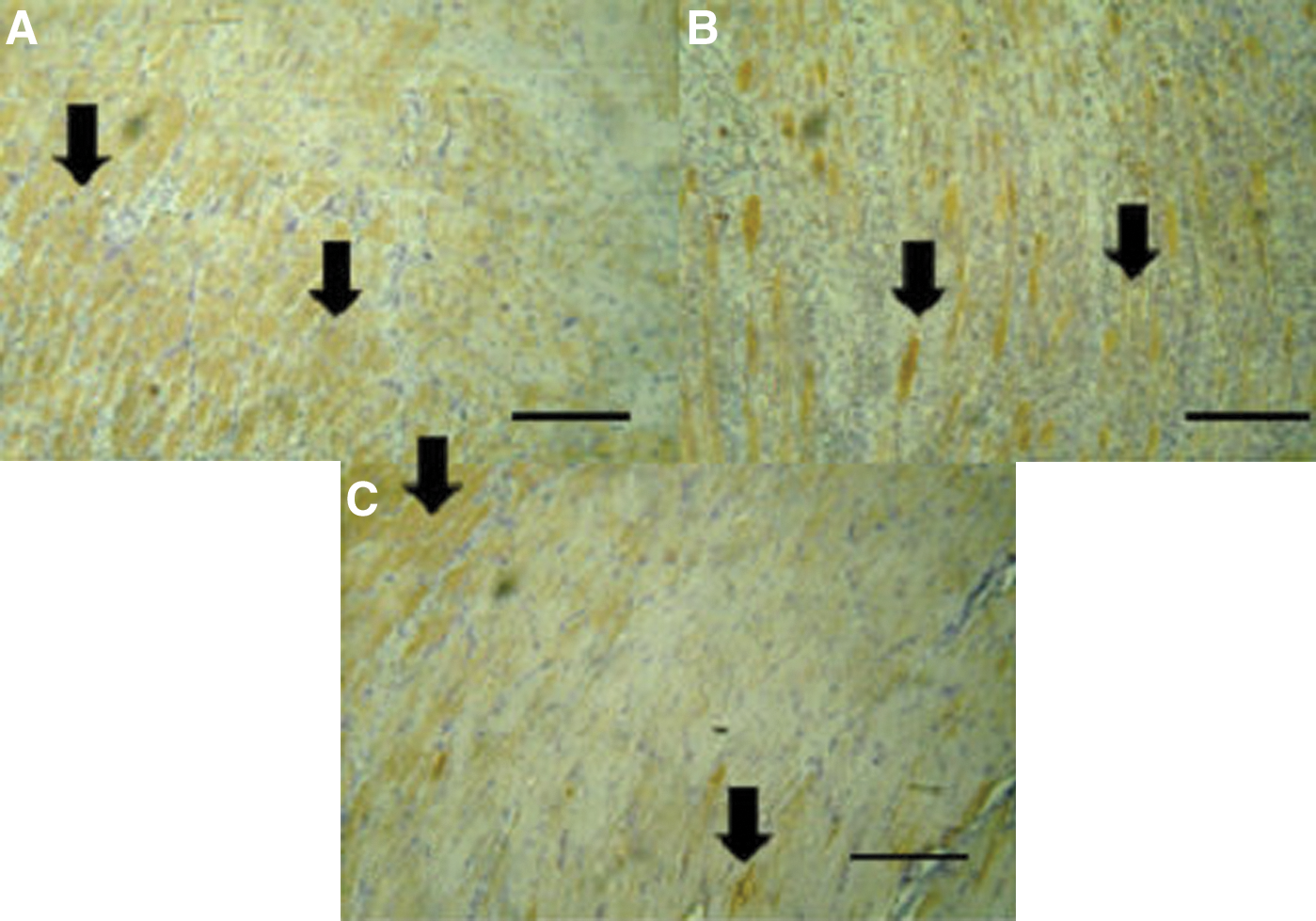
Immunohistochemistry for cyclo-oxygenase-2 (COX-2)
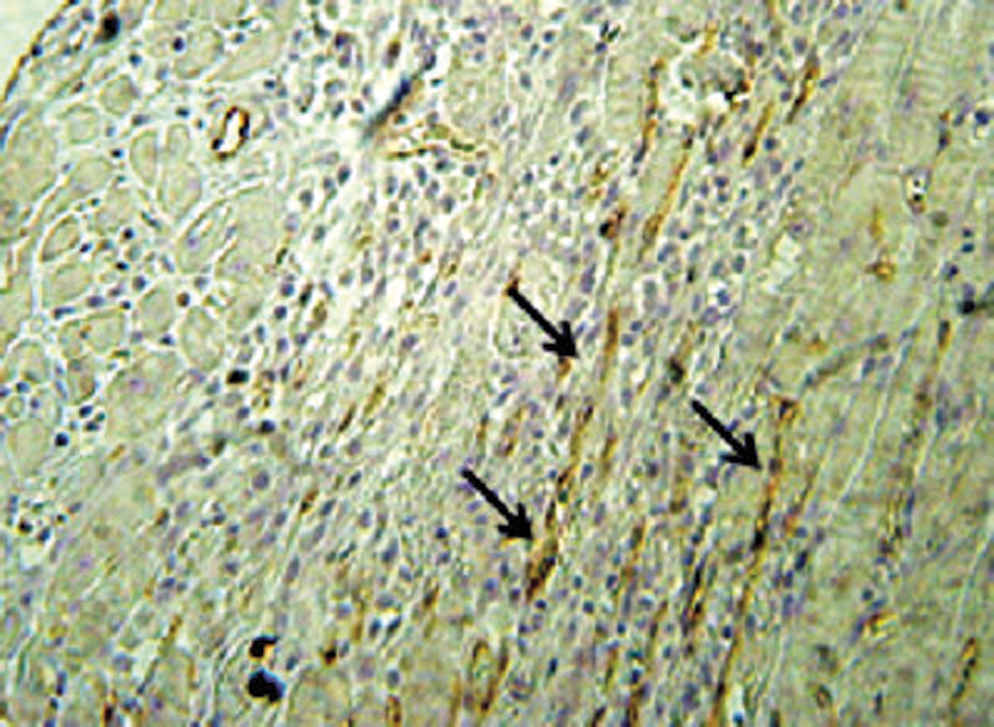
High magnification of COX-2 immunoexpression denoting positive expression in myofibrillar cells (immunohistochemistry stain).
Discussion
The goal of this study was to investigate the histopathological changes and the expression of COX-2 after LLLT or US application on muscle injured through cryolesion. To the best of our knowledge, this approach has not been used so far.
Regarding the histopathological examination, rats with cryolesion had acute extensive myofibrillary degeneration, which was related to infiltration with neutrophil granulocytes and interstitial edema. Moreover, LLLT attenuated the pathological features induced by cryolesion as demonstrated by the histopathological findings. When US therapy was evaluated, similar outcomes were detected by the diminished inflammatory response, but the response was less significant than with LLLT.
Some studies have revealed that LLLT is capable of decreasing the inflammatory response and optimizing tissue repair in rats. 21,22 Tomasek et al. 23 stated that LLLT decreases the extent of edema and the number of inflammatory cells and increases the amount of collagen and elastic fibers in the wound-healing process, which might explain the positive effect of laser on tissue repair acceleration. Our results corroborate those of Amaral et al. 12 who found that the HeNe laser, at a dosage of 2.6 J/cm2, resulted in increased mitochondrial density and muscle fiber density in TA muscles as compared to a control group. Also, Cressoni et al. 24 showed that the AlGaInP laser treatment (785 nm), at 9 J/point, produced a decrease in the number of leukocytes in the inflammatory infiltrate at the injury site. Such results suggested that the AlGaInP laser treatment had anti-inflammatory effects and reduced the number of leukocytes at the injury site by accelerating the regeneration of connective tissue. By contrast, it seems that LLLT failed to show any beneficial treatment effect on delayed onset muscle soreness in humans. 25 Such discrepancies could probably be explained by the differences in the study designs because the present study was performed in rodents. Comparing LLLT responses in human and rat may help elucidate how well rodent models reflect the human situation as well as identify possible strategies for targeting muscle repair. Also, the different results may be explained by the wide range of parameters and treatment protocols used by the different authors. However, is still very difficult to explain these divergences, and further studies are required.
Moreover, it has been postulated that pulsed US enhances both myogenic precursor cells and fibroblast proliferation in an experimental muscle contusion injury. 26 Also, US seems to improve muscle extensibility 27 and force production after contraction-induced muscle injury. 28,29 In an earlier study conducted by Piedade et al., 4 pulsed US radiation induced collagen fiber deposition and a statistically significant larger amount of myotubes was observed 14 d after the surgery, which suggests a stimulatory effect of US in the early postinjury treatment of muscle lacerations.
When the expression of COX-2 was investigated, our results showed that both LLLT and US promoted a down-regulation for the inflammatory mediator. In a recent study conducted by Albertini et al., 30 the expression of COX-2 mRNA decreased in animals receiving LLLT 1 h after the administration of carrageenan, in inducer of inflammation. Our results also agree with those obtained by Herman and Khosla, 31 who analyzed the therapeutic effect of GaAlAs on inflammation by using 2.3 J/cm2 in three applications. Yet others have demonstrated that LLLT using GaAlAs radiation exerts a time-dependent anti-inflammatory effect at an energy density of 2.5 J/cm2 with as little as one application. 32 Taken together, such results support the notion that LLLT and US improve muscle repair as a result of down-regulation of COX-2 after induced muscle injury in rats.
We considered the methodology used in this study to be highly adequate to investigate the effects of LLLT and US on injured muscle. The cryolesion is a common experimental model of injuries in muscle tissue. 33 We also observed that both therapies with the parameters used had positive effects on injured muscles. Because a large suite of parameters and wavelengths of laser irradiation have been used by different authors, it is not possible to determine an ideal protocol of treatment. 12 The same point could be made for the US therapy. There is no definitive protocol and the effect of this therapy on muscle regeneration is still controversial. 4 In this study, we used a low-intensity pulsed US, which prevented the increase of tissue temperature. As far we know, our study is the first to investigate the effects of low-intensity US on muscle healing after an injury. The mechanism through which US helps tissue repair is more likely related to its mechanical effects (ultrasonication) than thermal effects. 34 Ultrasonication, or “micromassage” of the muscle tissue, produces a change in membrane permeability and stimulates the transport of second messenger substances such as calcium across the cell membrane. 33 These second messengers may then stimulate the proliferation of myogenic cells, the satellite cells, activating them and helping in the healing process. 34
Some limitations of our work should be pointed out. We investigated only one period after the muscle injury. It would be very interesting to investigate the early and late tissue response to the laser and US application in different periods postinjury. Also, more quantitative analysis should be included in future research such as the quantification of inflammatory cells or newly formed tissue at the site of the injury and an evaluation of muscle mechanical properties.
In spite of these limitations, the results of this work highlight the stimulatory effects of both laser therapy and US on muscle healing. Such findings would furnish preliminary data on the potential safety and efficacy of both therapies as treatments for muscle injuries, especially in athletes and workers, in order to lead to an earlier return to daily activities and the previous level of function. Our study exploring the effects of LLLT and US on injured muscles in rats also should allow us to design future research strategies using human experiments.
In summary, this study reveals that therapies with either LLLT or US have positive effects on injured skeletal muscle in rats. Although further long-term studies and clinical trials are required, the findings of our study point to a promising utilization of such therapeutic modalities for muscle tissue healing.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.