
Abstract
Introduction
The tendinous tissue is a dense connective tissue, whose function is to transmit the force of a muscle to a bone, to produce movement. 6,7 Tendons consist of fibroblasts and an extracellular matrix in which fibrous proteins of collagen, elastine, proteoglycans, glycoproteins, and multiple saccharides are immersed. 8 Collagen is the main structural protein and major component of the extracellular matrix (86–95% wet weight). Collagen fibrils are long, highly aligned, and have a crystalline structure, which gives them high mechanical resistance to tension. 9 –12
The healing of a calcaneal tendon may take weeks or even months to complete, making adherence to the treatment regimen difficult. 13 –16 Because of the high incidence of these injuries, there is a need for studies focusing on the improvement of tendon repair, reducing recovery time and the time to return to normal activities.
Satisfactory results have been obtained in studies conducted with the purpose of finding the means to accelerate the healing of the calcaneal tendon 17 using physical agents such as ultrasound, 3,18 electrical stimulation, 19 and low-level laser therapy (LLLT). 20,21
LLLT has provided relevant results such as an increase in fibroblast proliferation and collagen synthesis, 22 cutaneous neovascularization, 23,24 and tendon repair. 21,25 However, there are variations in the parameters used (e.g., wavelength, energy density, output power) by different investigators. Because only a few studies on LLLT have investigated the effect of different output powers, there is no consensus on which is the optimal output power for use in tendon repair. Therefore, the aim of the present study was to evaluate the effect of output powers of 40, 60, 80, and 100 mW on the repair of partial calcaneal tendon rupture in rats.
Methods
All animal experiments were approved by the Animal Care and Use Committee at the Federal University of São Paulo (UNIFESP-EPM). All animals received humane care in strict compliance with the Guide for the Care and Use of Laboratory Animals (National Research Council, 1996).
The sample consisted of 50 adult male Wistar rats (Rattus norvegicus), weighing 260–320 g. The animals were obtained from the Central Laboratory Animal Facility of the Federal University of São Paulo (UNIFESP), São Paulo, Brazil. The rats were housed in individual polypropylene cages, on a 12:12 h light–dark cycle, and fed standard rat chow and water ad libitum.
The animals were randomly divided into 5 groups of 10 rats each using the Statistical Software Biostat 5.0 (Brazil-Pará-Belém). A partial tendon rupture was induced by direct trauma in all animals. After, each group was subjected to the following procedures: the control group received sham stimulation, and the experimental groups received laser treatment for 5 consecutive days. Six days after trauma-induced injury, the animals were killed, and the calcaneal tendons were removed and examined by polarized light microscopy.
Procedure to induce partial calcaneal tendon rupture
The animals were weighed and anesthetized with an intraperitoneal injection of ketamine hydrochloride (100 mg/kg) and xylazine hydrochloride (50 mg/kg). The skin over and around both the right and left calcaneal tendons was shaved; the paw subjected to trauma-induced injury was selected by lottery (Statistical Software BioStat 5.0). An injury device was developed at the machine shop of the Federal University of São Carlos (UFSCar).
The selected paw was positioned on the injury device and a light tensile force was applied to the calcaneal region in such way that the ankle was maintained in dorsiflexion and the dorsal surface of the paw was in contact with the injury device. Following, a 186 g weight was dropped on the tendon of the animal from a height of 20 cm (potential energy, 364.9 mJ), (Fig. 1).
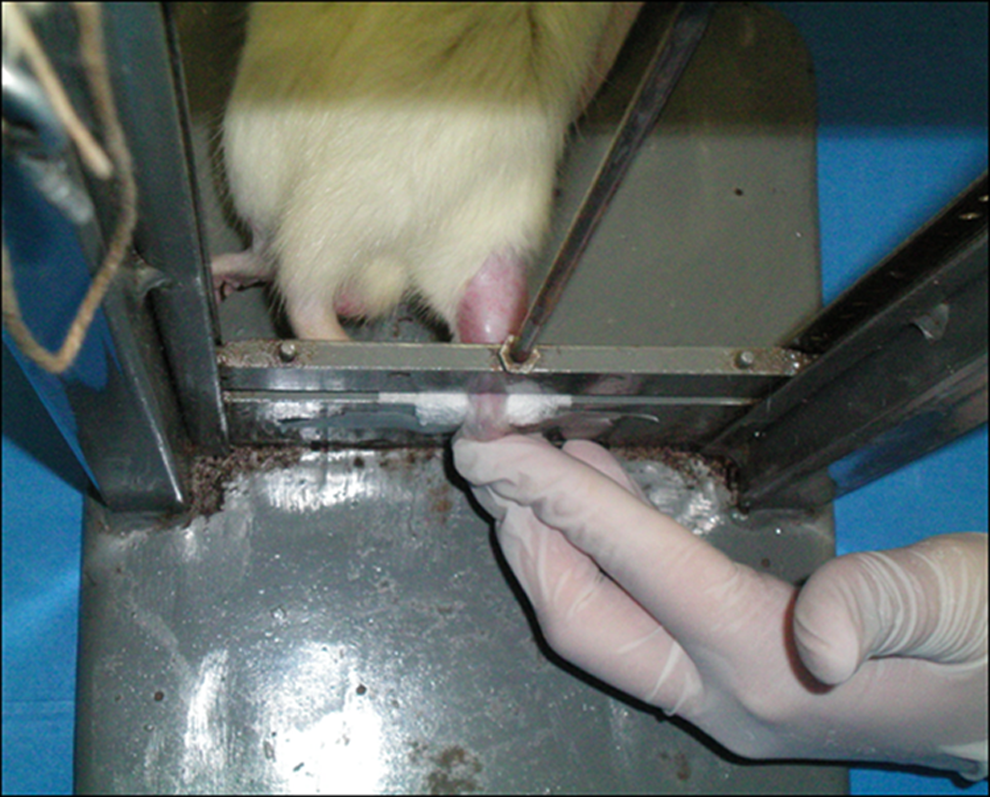
Injury device for partial calcaneal tendon rupture. Overall view of the weight over the tendon at the moment of the injury after the weight was dropped.
Immediately after this procedure, the weight was removed and the injury site was marked with a circle using a skin pen for the laser treatment. Next, the animals were returned to their cages and were observed until the anesthesia wore off.
Laser treatment
The laser treatment was started after trauma-induced injury, and all animals were subjected to the treatment for 5 consecutive days. Treatment sessions were conducted on each animal at the same time of day as the first laser application. The laser probe was placed in direct contact with the animal on only one treatment point at the injury site and positioned perpendicularly to the calcaneal tendon.
Laser treatment was delivered using a GaAlAs diode laser (DMC®, Sao Carlos, Sao Paulo, Brazil) emitting at a wavelength of 830 nm (infrared), with output powers of 40, 60, 80, and 100 mW, energy density of 30 J/cm2, total energy dose of 0.84 J, beam cross-sectional area of 0.028 cm2, and operating in a continuous mode.
The animals were randomized into five groups and each group was subjected to laser treatment and irradiated as follows: • Control group – sham stimulation • 40 mW group – output power of 40 mW and power density of 1.4 W/cm2 for 21 sec • 60 mW group – output power of 60 mW and power density of 2.14 W/cm2 for 14 sec • 80 mW group – output power of 80 mW and power density of 2.8 W/cm2 for 10.5 sec • 100 mW group – output power of 100 mW and power density of 3.5 W/cm2 for 8.4 sec
Tendon excision and sample preparation
Six days after trauma-induced injury, the animals were killed by anesthesia overdose. For removal of the calcaneal tendon, two incisions were made in each animal: one in the musculotendinous junction, and another proximal to the calcaneal insertion. Five seconds after removal, the calcaneal tendon was affixed to a paraffin surface, which had been previously molded in a Petri dish. Two pins were used to affix the tendon to the paraffin; the first pin was placed in the base of the tendon (osteotendinous junction), and the second pin was placed in the gastrocnemius muscle. Following, 10% buffered formaldehyde was poured into the Petri dish until the sample was covered by liquid. The sample was maintained immersed for 40 min, after which the formaldehyde was removed, an incision was made 2 mm below the musculotendinous junction, and another incision was made 2 mm above the osteotendinous junction using a shaving blade.
All samples were cut to the same length of 0.8 cm. Next, each sample was wrapped in paper filter (3×2 cm) and placed inside a small box, which was immersed in 10% buffered formaldehyde for 24 h, and then in 70% alcohol for 48 h, initiating the preparation of histological slides for polarized light microscopy.
Following this, the organization, state of aggregation and molecular arrangement of collagen fibers were evaluated by birefringence measurements and the collagen content was determined by Picrosirius Red staining.
Birefringence measurements
Birefringence optical retardation (OR) measurements were made in monochromatic light (546 nm) using a light microscope (Leica, Ernst-Leitz, Strabe, Wetzlar, Germany) with a POL 10 ×/0.22 eyepiece, a 0.9 condenser, and a compensator (λ/4, Senarmont).
Prior to the birefringence analysis, all histological slides were immersed in distilled water for 30 min. During the measurements, the longitudinal axis of the tendon was positioned at the angle of 45° with respect to the microscope polarizer; at this position, the optimum value of optical retardation for collagen fibers was obtained (OR=brightness).
Picrosirius Red staining
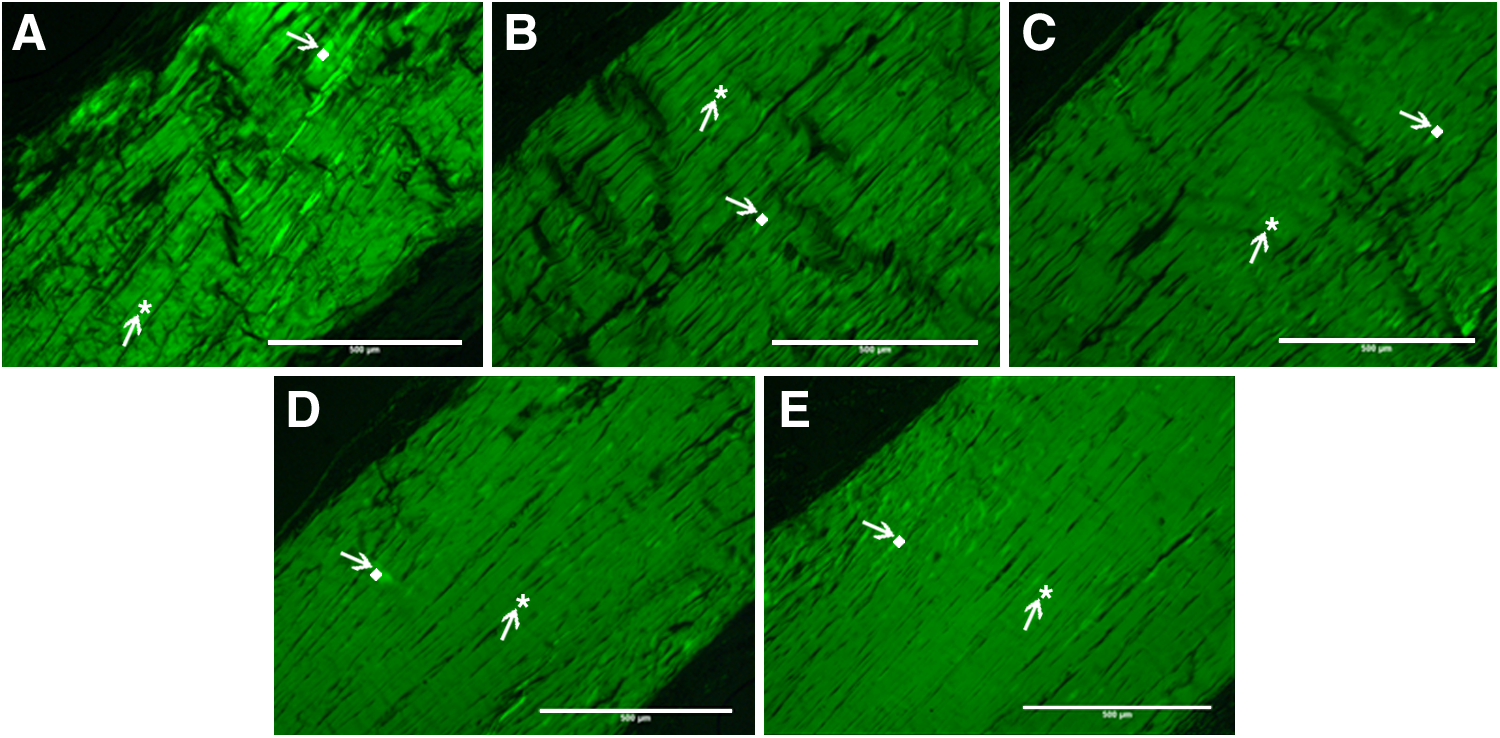
The tissue stained with Picrosirius Red was examined by polarized light microscopy (Nikon E-800 microscope, London, UK) for the presence of thin type III collagen fibers (green) and thick type I collagen fibers (red and yellow). Ten microscopic fields (field area, 303598.2 μm2; total area, 3035982 μm2) were analyzed per slide. Images were imported to the Image-Pro Plus 4.5 software (Bethesda, MD) for quantitative analysis; results are expressed as mean percentages of the total area occupied by each type of collagen fiber.
Statistical analysis
The reproducibility of the measurements made by two observers was assessed using the intraclass correlation coefficient (ICC) and the Bland-Altman graphs.
The one-way analysis of variance (ANOVA) was used for group comparison. Variance equality hypothesis was verified by the Levene's test. When the variances were different, the Brown-Forsythe correction and the Dunnett's multiple comparison methods were used. Significance was set at p<0.05 for all analyses
Results
Birefringence results indicated that groups treated with LLLT showed a non-statistically significant improvement (p>0.05) in the realignment of collagen fibers associated with an increase in the output power (Figs. 2 and 3).
Quantitative birefringence measurements showing the organization of collagen fibers in the different groups:
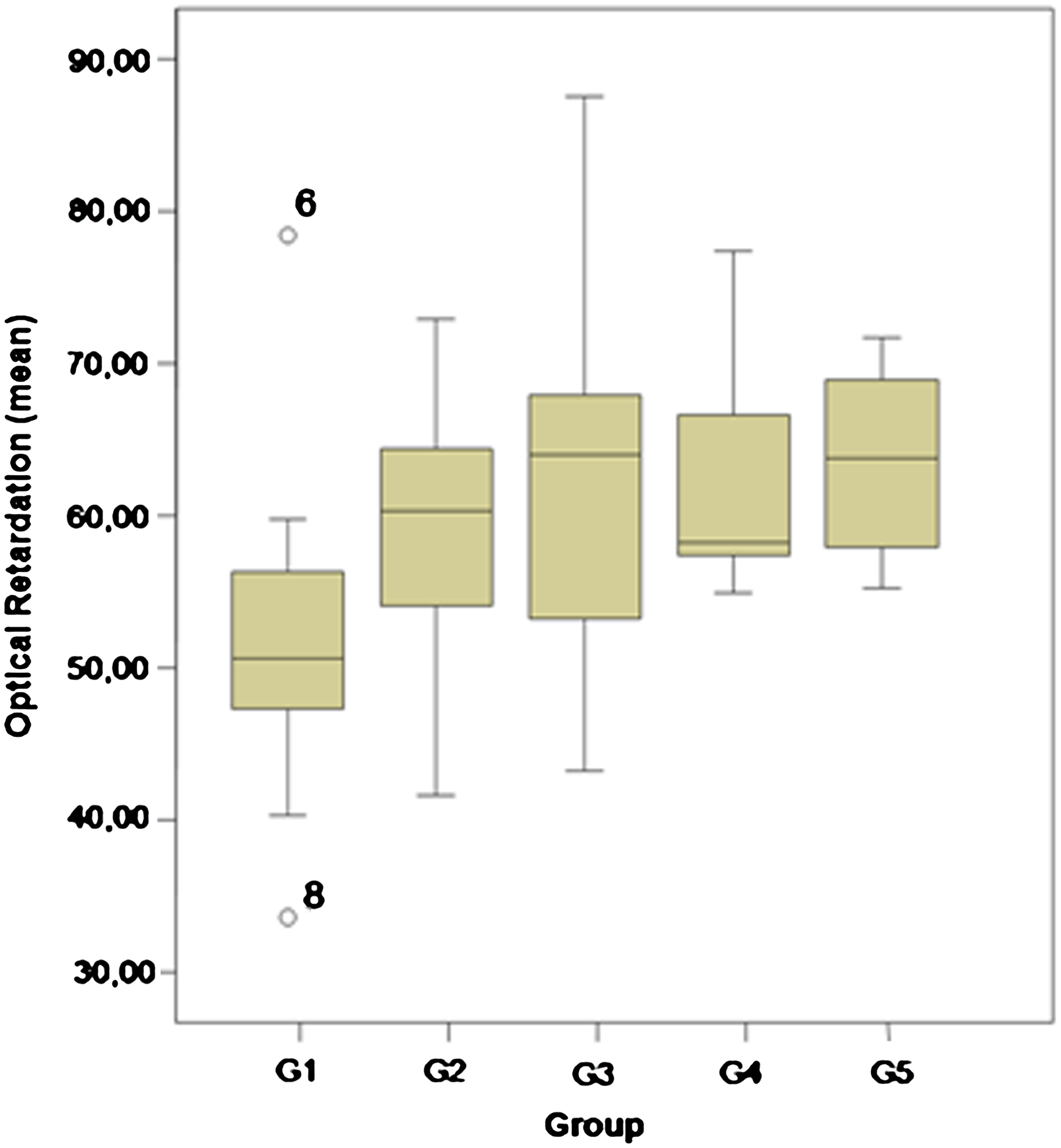
Box plot showing mean optical retardation (OR) values for the different groups. Mean OR values were non-statistically significant higher in the 40-, 60-, 80- and 100-mW groups than in the control group (p>0.05).
It was observed that the higher the output powers (60–100 mW) the greater was the amount of type III collagen. Significant differences in the amount of type III collagen were found between the control group and the 60 mW (p<0.01), 80 mW (p<0.01), and 100 mW (p=0.02) groups (Table 1).
Significantly greater amounts of type I collage fibers were found in 80 mW group than in the control group (p=0.05). No significant differences in the amounts of type I collagen were found between the control group and the other experimental groups (p>0.05) (Figs. 4 and 5).
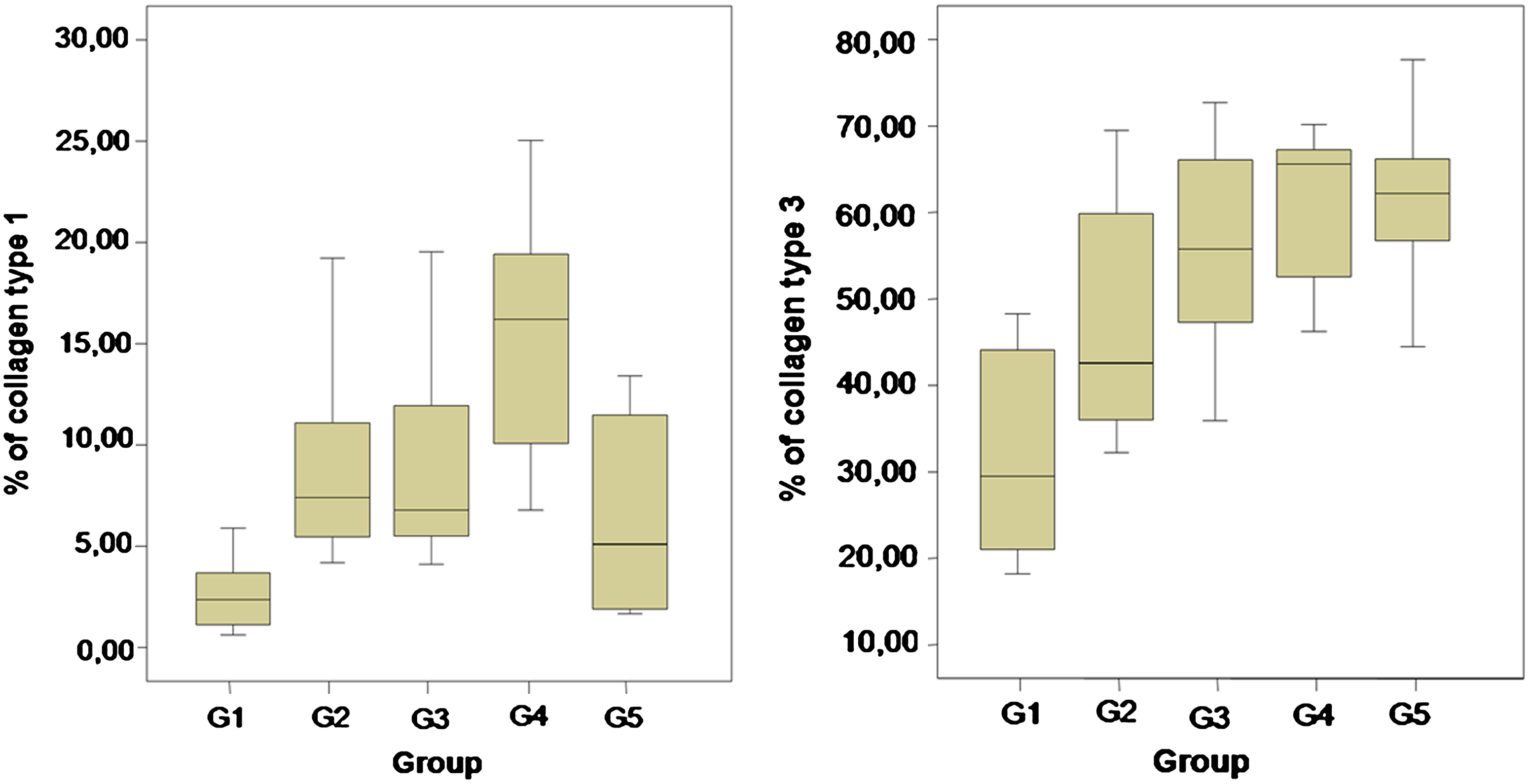
Box plot showing the percentage of type I and III collagen for the different groups. The percentage of type I collagen was significantly higher in the 80-mW group than in the control group (p=0.05). The percentage of type III collagen was significantly higher in the 60-, 80- and 100-mW groups than in the control group (p<0.05).
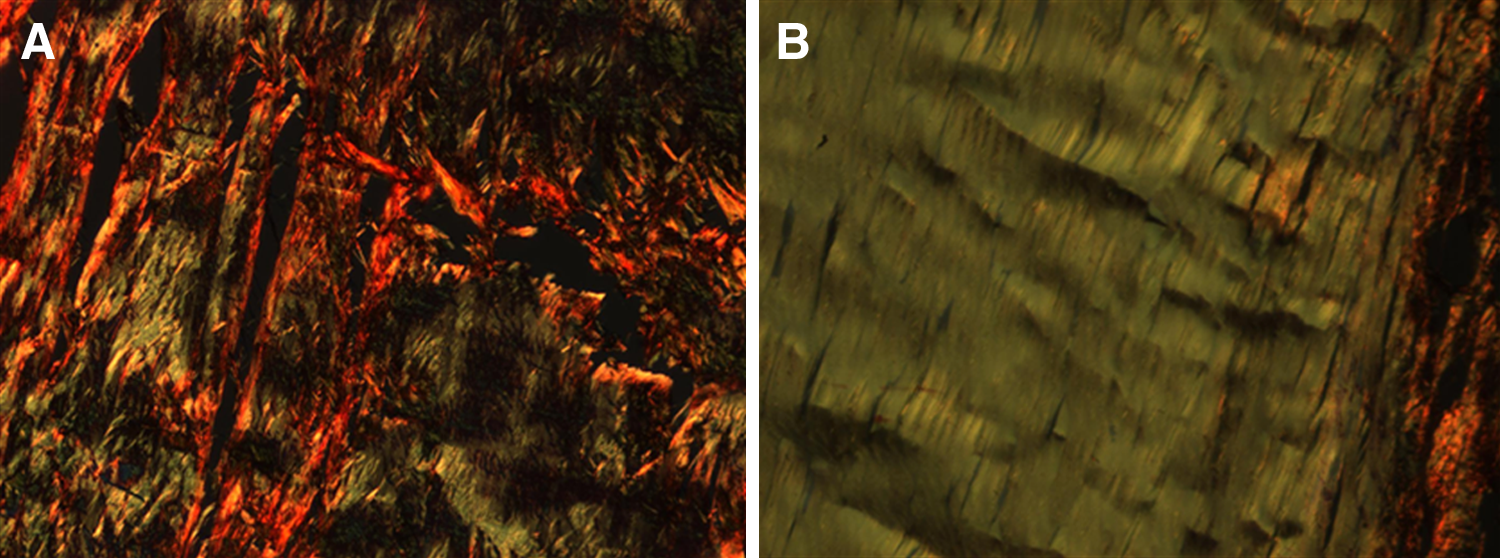
Tissue stained with Picrosirius Red examined by polarized light microscopy.
Discussion
Van Breugel and Bar 26 reported that most studies have considered energy density as the most important variable with respect to the therapeutic effects of laser irradiation. Few studies have been conducted to evaluate the effect of output power on the results of laser therapy.
Tunér and Hode 27 suggested that a high output power may lead to a high energy density. Many studies on laser therapy 25,27,28 were conducted with lasers with output powers ranging from 10 to 40 mW, but there are few studies in the literature using lasers with output powers ranging from 40 to 100 mW. 29 Based on this fact, four different power settings were used in the present study (an intermediate value of 40 mW, and three higher values of 60, 80, and 100 mW) in order to determine which power setting would deliver the best results.
According to Chan et al. (2007), 19 the tendon repair process is similar to other repair processes that occur in biological tissues. The repair process is associated with the proliferation and migration of different types of cells, collagen synthesis, angiogenesis, and granulation tissue formation, and with the orientation of tendon cells and collagen fibers in a highly organized manner as an effort to restore the structure and function of the injured tendon.
In our study, the degree of orientation of collagen fibers and the type of collagen present in the initial phase of the inflammatory process were assessed by Picrosirius Red staining.
Birefringence analysis was conducted to assess the alignment of collagen fibers, as suggested by Vidal, 7 who considered this method ideal to detect and describe the orientation of collagen fibers of the tendon.
Birefringence results indicated a non-statistically significant trend (p>0.05) toward a gradual increase in mean OR values associated with an increase in the output power as follows: control group (52.1 nm), 40 mW group (59.42 nm), 60 mW group (61.82 nm), 80 mW group (61.59 nm), and 100 mW group (63.52 nm). These results disagree with the Oliveira et al. 21 results about treatment days, which reported a better organization of collagen fibers using an LLLT 850 nm with 1.4 W/cm2 and 4 J/cm2 on the 5th day, whereas our study showed better results on the 6th day after injury. In the present study, the tendon repair probably began to occur prematurely (from about the 3rd to the 5th day after injury) showed by assessment of OR values, for high output powers, should be made in a shorter period of time after injury. We believe that the nonsignificant results may be attributed to the small size of the sample and due evaluation period, like 7th day post lesion. However, we observed a gradual increase in the organization of collagen fibers associated with increase in the output power.
Significant differences in the amount of type III collagen were found between the control group and the 60, 80, and 100 mW groups (p<0.01), with the 100 mW group showing the best results. On the other hand, significant differences in the amount of type I collagen fibers were found only between the 80 mW group and the control group; this is an isolated case, as there is no study in the literature reporting similar results. Maffulli et al., 30 in a previous study on an in vitro model of human tendon healing, reported greater amounts of type III collagen in ruptured and tendinopathic Achilles tendons than in normal Achilles tendons. The amount of type III collagen in injured calcaneal tendons may be related to the phase of lesion development. Many studies in the literature reported a reduced amount of type I collagen and an increased amount of type III collagen in injured calcaneal tendons. 30,31
The greater amounts of type III collagen found in the 60, 80, and 100 mW groups may be explained by the fact that LLLT with high output powers may deliver a signal to the extracellular matrix that induces changes in fibril structures. These changes may occur because of the interaction between electromagnetic energy and collagen molecules. The azimuthal orientation of the collagen along the longitudinal axis of the tendon is a good evidence of structural changes in collagen fibers after irradiation. 18,32 The results from the present study suggest that LLLT using infrared lasers operating at output powers of 40, 60, 80, and 100 mW has a positive effect on the treatment of partial calcaneal tendon rupture. Our results are consistent with the findings of other studies reporting on the use of LLLT with longer time periods as a treatment for tissue repair, in which the response of fibroblasts and collagen molecules to laser irradiation were evaluated. 33 –35
The results of this study raise an important question regarding the parameters. Is power or power density the important factor to improve the tissue repair? In 2005 the World Association for Laser Therapy (WALT) published the dosage guidelines showing the importance of the energy (joules) and power density. The maximum power density recommended to treat the Achilles tendon is 100 mW/cm2, but this study used power densities of 1.4–3.5W/cm2 and still produced positive effects. Further studies are necessary to clarify the validity of the 100 mW/cm2 limit stated in the WALT guidelines.
Further studies are necessary to study the power densities such as 80, 90, or 100 mW/cm2.
Conclusions
The results also revealed that the laser output power affects tissue repair. However, it is still premature to state that output power is a fundamental factor in accelerating tendon repair. Further studies on LLLT using infrared lasers are necessary to better understand the effect of output power on tissue repair.
Footnotes
Acknowledgments
We thank the Division of Plastic Surgery of the UNIFESP, Lamav-UFSCar and the Coordination for the Improvement of Higher Education Personnel (CAPES) for supporting this study.
Author Disclosure Statement
No conflicting financial interests exist.