
Abstract
Introduction
Faced with this challenge, the scientific community began to focus research efforts on novel technologies and materials for the treatment of periapical disease, in an attempt to achieve better success rates for apicoectomy. Success rates >90% with modern periapical surgical techniques have been reported in the literature. 3
Periapical surgery shares the objective of traditional endodontic treatment—to clear bacteria from the apical delta and establish an effective barrier to prevent recontamination with microorganisms and/or microbial metabolites that would otherwise invade periapical bone and soft tissues. Obtaining a successful apical seal is dependent upon adequate apicoectomy, retrograde cavity preparation, and choice of a good retrofilling material. 4
Perfecting a method that enables improvement of root morphology after apicoectomy (increasing smoothness and decreasing porosity so as to minimize microbial deposition) is one of the goals of apical surgery.
The objective of this study was to test the null hypothesis that Nd:YAG laser does not induce morphological changes in the apical dentin after apicoectomy and retrofilling with gutta-percha and mineral trioxide aggregate (MTA). Toward this end, we conducted an in vitro, scanning electron microscopy (SEM), and energy-dispersive X-ray spectrometry (EDS)-based analysis of the effects of Nd:YAG laser irradiation on the morphology of the apical dentin after cross-section. We compared the marginal adaptation of irradiated and nonirradiated filling and retrofilling materials (gutta-percha and MTA, respectively), assessed morphological changes in apical dentin after Nd:YAG laser irradiation, and identified changes in the chemical composition of apicoectomized areas after irradiation.
Materials and Methods
The present study was approved by the Pontifícia Universidade Católica do Rio Grande do Sul (CEP/PUCRS) Research Ethics Committee.
Specimen preparation
The sample consisted of 40 human canines (maxillary or mandibular), with classic, single-root anatomy and complete root formation. For inclusion in the sample, teeth had to be free of root fracture, resorption or obliteration, or prior endodontic treatment, and had to be kept in 0.9% saline solution at 4°C. All teeth were surface cleaned, which involved scaling to remove any calculus and rubbing with saline-soaked gauze. Crowns were removed with a carborundum disc wheel (Moyco Precision Abrasives, Montgomeryville, PA), 16 mm from the apex, as measured with digital calipers (Digimatic®, Mitutoyo Sul Americana, Suzano, Brazil).
Endodontic treatment
The working length for endodontic instrumentation was established as the distance from the file tip to the foramen after placement into the root canal. Flex-R stainless steel files (Moyco® Union Broach, York, PA) were introduced into the canal after filling with 1% sodium hypochlorite (NaOCl). Canals were widened to size #35. Irrigation with 2 mL of 1% NaOCl was performed when switching files. Canals were filled with the lateral condensation technique, using #40 master gutta-percha cones (Endopoints®, Rio de Janeiro, Brazil) B7 accessory cones (Endopoints®, Rio de Janeiro, Brazil) and zinc oxide-eugenol sealer (Endofill®, Dentsply, Petrópolis, Brazil).
Teeth were randomly allocated into four groups as shown in Table 1.
Apicoectomy
In all four groups, apicoectomy was performed using a #4102 cylinder diamond bur (Microdont®, São Paulo, Brazil) mounted in a high-speed handpiece (Kavo®, Santa Catarina, Brazil), perpendicular to the long axis of the root, under constant saline solution cooling, 3 mm from the apex.
Retrograde cavity preparation and retrofilling
In groups C and D, retrograde cavity preparation was performed with a Jet Sonic Four Plus ultrasound unit (Gnatus®, Ribeirão Preto, Brazil), adjusted according to manufacturer recommendations for the S (scaling) setting, and a S 12/90D diamond-coated ultrasonic retro-tip (Gnatus®, Ribeirão Preto, Brazil), on power setting 8, under constant irrigation with saline solution (0.9% NaCl). Cavity width corresponded to the diameter of the retro-tip, and depth was standardized by marking the ultrasound tips at 3 mm. Specimens were then filled with MTA cement (Angelus®, Londrina, Brazil), manipulated according to manufacturer instructions. The cavity was filled to excess with an amalgam carrier and the cement was condensed with a #11 Paiva plugger (Erwin Guth, São Paulo, Brazil). Excess cement was removed with a #1/2 periodontal curette (Hu-Friedy Manufacturing Company, Inc.®, Chicago, IL).
Laser irradiation.
The 20 teeth in groups B and D were irradiated with an Nd:YAG laser (Fotona®, Twinlight Laser Dental, Brasília, Brazil, λ=1064 nm), in pulsed mode, at a pulse repetition rate of 10 Hz, with no refrigeration, at an energy setting of 150 mJ/pulse (power 1.5 W), for 60 sec, with the fiberoptic tip located 2 mm from the apex. 5 The laser beam was applied in a zigzag fashion, buccal to palatal/lingual and mesial to distal, to ensure irradiation of the entire cut surface. The fiberoptic tip was trimmed with a #11 scalpel blade before use in each group, so as to prevent changes in the distribution of laser irradiation across the apical surfaces.
Between all procedures of the experiment, specimens were kept at room temperature in 0.9% saline solution.
Preparation for SEM analysis
Teeth were kept in a desiccator for 2 weeks to ensure slow removal of water. Desiccated samples were then embedded in low-density epoxy resin (to enable lengthwise sectioning at the center of the apex), followed by thin film sputter coating with gold (to enable SEM imaging).
SEM analysis
Longitudinal and cross-sectional SEM images of the apicoectomized surfaces of all 40 teeth were obtained with an XL 30-model scanning electron microscope (Philips®, Eindhoven, the Netherlands), so as to ensure visualization of the entire resected surface and enable assessment of adaptation of the filling material to the root canal in each group.
Qualitative analysis of specimens was performed under 70× magnification for identification of any irregularities, debris, smear layer, fusion, recrystallization, and dentin sealing. Prior to assessment, examiners were calibrated using the surfaces shown in Fig. 1 as a reference.
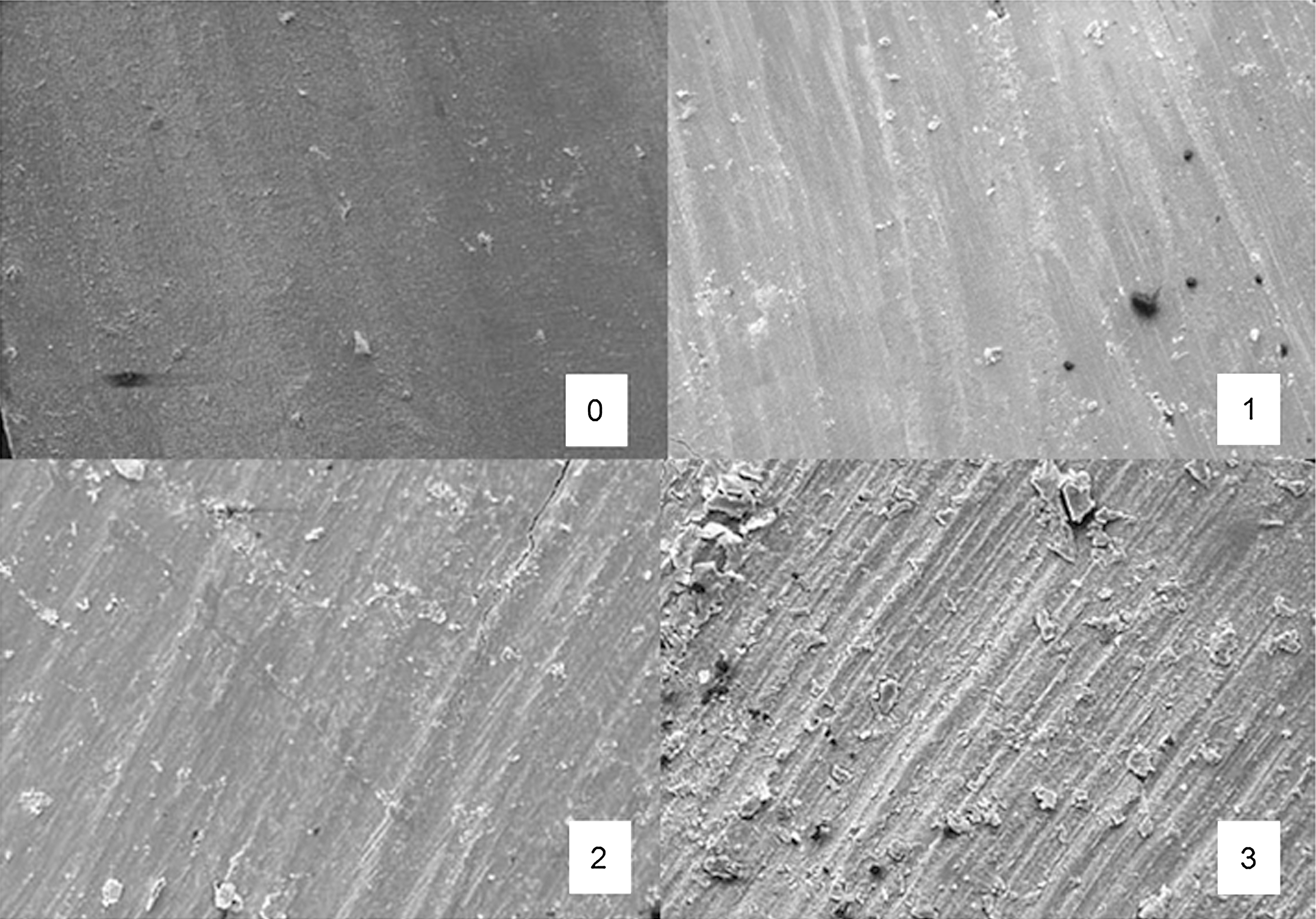
Root dentinal surface, with different smoothness scores for examiner calibration. (Source: Duarte et al. 6 )
Longitudinal images and cross-sections were analyzed under 1000× magnification for quantitative assessment of the gap between the filling (groups A and B) or retrofilling material (groups C and D) and the root canal walls. All images were assessed using the Image Tool® software package (Image Tool for Windows 3.0, UTHSCSA, San Antonio, TX,).
Statistical analysis
Inter-rater agreement of qualitative analysis was measured by assessment of a scale consisting of 10 photomicrographs. The κ test was used for comparison of results and revealed significant (p<0.001) inter-rater agreement.
The Kruskal–Wallis test was applied to nonparametric qualitative assessment data, after use of descriptive statistics for identification of means and standard deviations. Analysis of variance (ANOVA) was performed on quantitative assessment and EDS variables with normal distribution, followed by Tukey's multiple comparison test. The Shapiro–Wilk test was used to test for normal distribution of the percentage carbon, oxygen, phosphorus, and calcium content of dental apices in all four groups. The significance level was set at 5%.
Results
On qualitative assessment of the homogeneity of apicoectomized surfaces, mean scores showed that the Nd:YAG laser-treated groups had more regular, homogeneous surfaces. Comparison of mean scores showed significant differences (p<0.01) between the irradiated groups (B and D) and the nonirradiated groups (A and C) (Table 2).
SD, standard deviation.
p Values calculated from Kruskal–Wallis test.
Statistically significant difference (for α=0.05).
There were no significant differences between the two nonirradiated groups (A and B), or between the two laser-irradiated groups (C and D). Surfaces in groups A and C were rated as being more irregular, with more debris and smear layer reported, whereas in the Nd:YAG-treated groups (B and D), the surface had a glazed, vitrified appearance, with areas of fused dentin. No craters were observed in groups B and D. Canaliculi were visible only in groups A and C; none were identifiable in groups B and D, which confirmed dentin sealing. No accessory canals were detected in any study specimens. There was no evidence of spreading or displacement of the filling materials on any cut surfaces. Imaging findings suggested that adaptation of gutta-percha was inferior to that of MTA (Fig. 2).
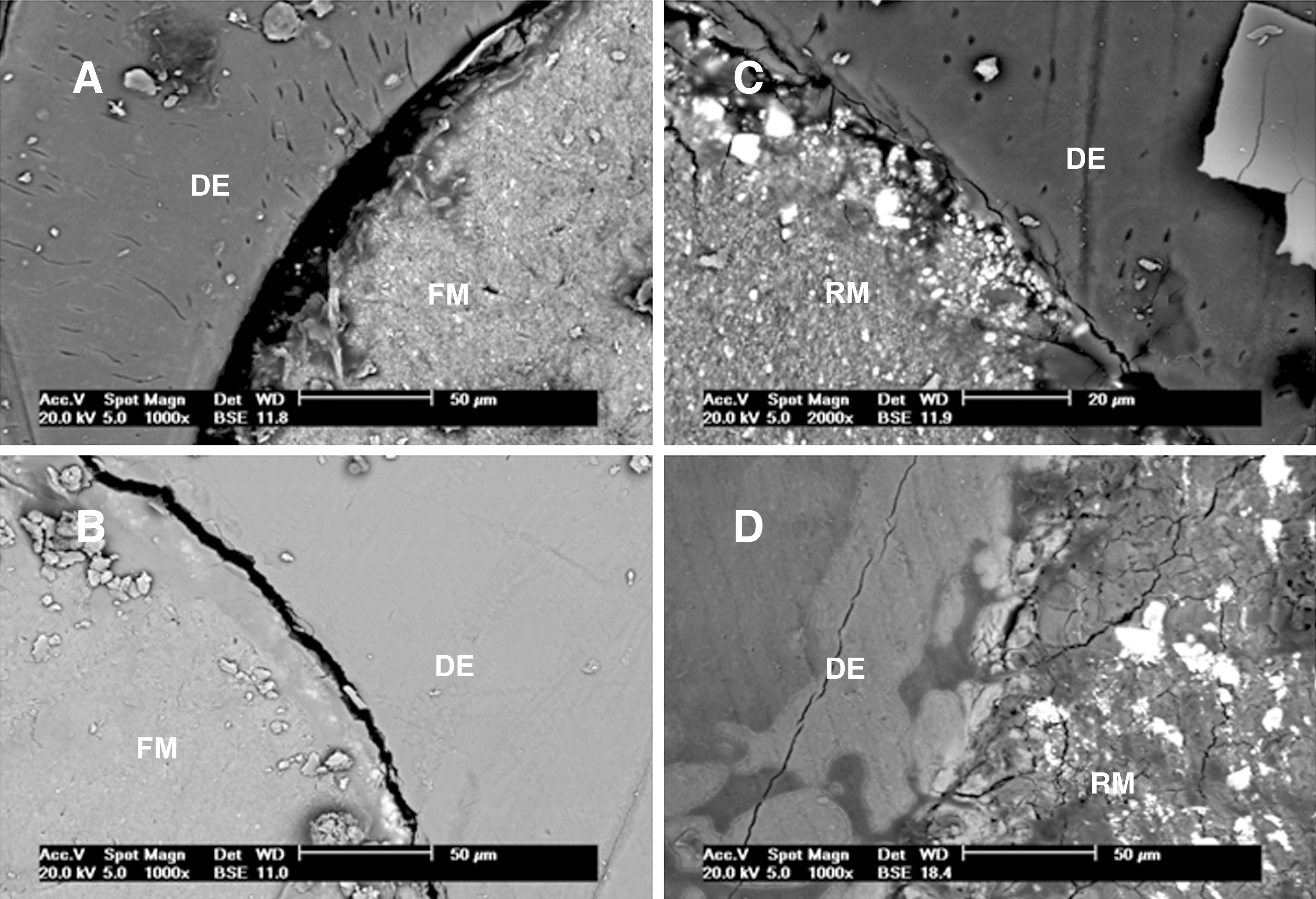
Measurement of gaps on cross-sectional images showed superior marginal adaptation in groups C and D (MTA retrofilling), with mean gaps of 2.6685 μm and 12.0755 μm respectively. The largest gaps were found in groups A and B (20.363 and 74.982 μm, respectively); both used gutta-percha as the filling material (Table 3). Comparison of mean gap sizes on cross-sectional and longitudinal images showed significant differences between groups A and B (p<0.01) and between groups C and D (p<0.01), which is indicative of a change in the dimensions of materials present in the root canal after Nd:YAG irradiation. The statistically significant difference in gap sizes between groups A and C reveals that MTA was associated with the best marginal adaptation. Likewise, the difference between groups B and D shows that MTA was more resistant to the size changes induced by Nd:YAG laser irradiation.
SD, standard deviation.
p Values calculated from ANOVA.
Statistically significant difference (for α=0.05).
Assessment of gaps on longitudinal SEM images again showed poorer adaptation between the filling material and dentin surface in groups A and B (15.1155 and 33.232 μm, respectively), and, consequently, smaller gaps in groups C and D (4.203 and 4.9765 μm, respectively) (Table 3). This statistically significant between-group difference once again shows the causal relation implied by analysis of cross-sectional SEM image findings. Therefore, one may infer that both MTA (groups C and D) and gutta-percha (groups A and B) underwent dimensional changes, which would account for the between-group differences. Furthermore, the marginal adaptation of MTA was again superior to that of gutta-percha.
Regarding EDS analysis of chemical composition, ANOVA was used to ascertain whether there were any significant between-group differences in carbon, oxygen, phosphorus, and calcium content of samples. There were no significant between-group differences in carbon or oxygen content. Mean phosphorus content was higher in the Nd:YAG laser-treated groups, whereas mean calcium concentrations were higher in the nonirradiated groups (Table 4).
C, carbon (p-value); O, oxygen; P, phosphorus; Ca, calcium; SD, standard deviation.
p Values calculated from ANOVA.
Statistically significant difference (for α=0.05).
Because of the between-group differences in phosphorus and calcium content, Tukey's multiple comparison test was used for pairwise comparison of the study groups. The test showed significant differences between the calcium content of specimens in the Nd:YAG laser-treated groups (B and D) and that of specimens in the nonirradiated groups (A and C). A versus C and B vesus D comparisons showed no significant differences. These findings strengthen the association between Nd:YAG use and modification of the chemical composition of the dentin surface.
Comparison of the percentage calcium content of samples showed significant differences between groups A and B, A and D, and C and D. These findings suggest that Nd:YAG laser irradiation is associated with a decline in calcium levels.
Analysis of the EDS spectra of these three groups showed that phosphorus content was highest in group D (apicoectomy+retrofilling+Nd:YAG laser), followed by group B (apicoectomy+Nd:YAG laser). Calcium levels were similar in group A (apicoectomy alone) and in the remaining groups. EDS spectra show peaks that represent certain elements associated with metal treatment of specimens (gold, silver, palladium, zinc) or the saline solution in which specimens were cleaned and stored (sodium); these are unrelated to the dentin structure (Fig. 3).
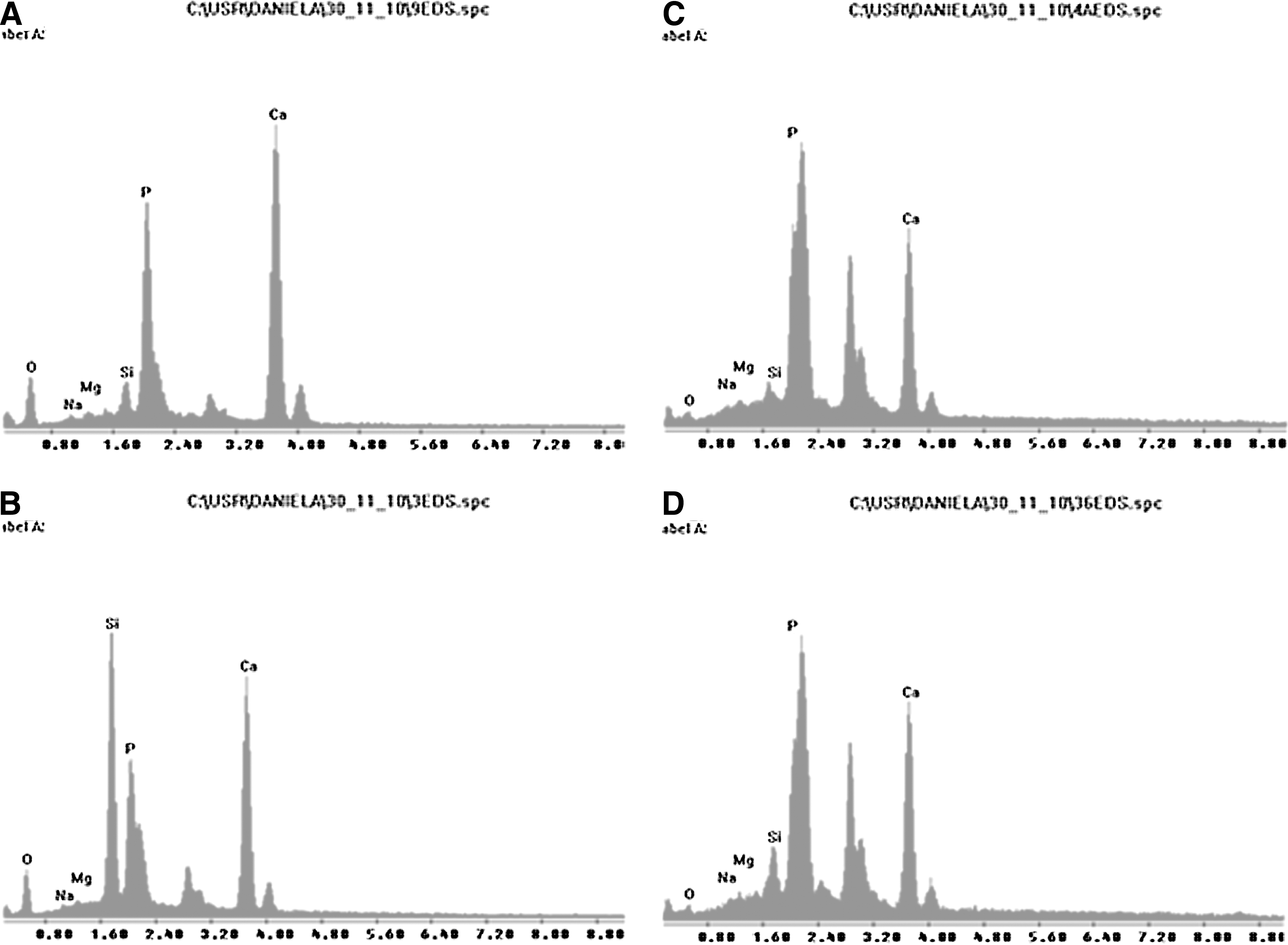
Energy-dispersive x-ray spectrometry spectra showing differences in phosphorus and calcium content of specimens in groups A, B, C, and D.
Discussion
The primary objective of treating periapical inflammation is removal of the cause—usually an infection—and sealing of the affected area, which is served by a vast array of accessory canals that hinder periapical healing and health. Periapical surgery is still the best therapeutic alternative to meet the need for preservation of the tooth. 6 –8 High success rates of periapical surgery have been reported in recent years, with the advent of new surgical techniques, ultrasonic tips, and novel retrofilling materials. 9 –11
The anatomy of the apical region, with its canal system forming the complex apical delta, requires that root end resection be performed perpendicular to the long axis of the tooth. In the present study, cutting 3 mm from the apex removed all visible accessory canals and provided a seemingly constant diameter of dentinal tubules in the area. From a clinical standpoint, this method has been associated with superior outcomes in terms of removing necrotic tissue and clearing bacterial infection from the root end. 12,13
The choice of diamond-coated retro-tips for retrograde cavity preparation prior to MTA retrofilling was based on the current literature; specifically, on the lower risk of dentin fractures, which can jeopardize adaptation of the filling material. 14,15
MTA has achieved excellent reliability as a filling material in periapical surgery. According to the current literature and the results of the present study, we may state that apical placement of MTA is an effective strategy for reducing maladaptation of the filling material and, consequently, marginal leakage, which can adversely affect the clinical success rate of apicoectomy. 16 –20 One may suggest that the smaller gap sizes found in MTA-retrofilled teeth in our sample were also the result of the chemical composition of this material. In some specimens, adaptation was perfect, with the boundary between the filling material and the dentin walls being practically undetectable. 18
The dental canaliculi are structures that provide a permeability component to the root dentin. Reducing this permeability is the main objective of using novel laser-based technologies in apicoectomy. 21 As the 1064-nm Nd:YAG laser exhibits an affinity for certain mineral structures present in dentin, its heating and tissue fusion effects are particularly potent in this tissue. Descriptive assessment of SEM images showed vitrified surfaces with fused dentin in the Nd:YAG laser-irradiated groups, with negligible porosity and cracks. As well as demonstrating changes in the dentin surface, qualitative analysis of apical surface smoothness confirmed that Nd:YAG effectively fused the dental canaliculi, giving the dentin surface a glazed, homogeneous appearance. These findings are consistent with those reported by most authors in the current literature. 22 –25 It was also clear that laser penetration occurred in the region analyzed on cross-sections (3 μm), as shown by the obliteration of canaliculi to this depth in the irradiated groups. 23,25,26 Among the various lasers available, used for the sole purpose of reducing dentin infiltration and aiding apical decontamination, the Nd:YAG laser has proved most effective. 27 –30
Assessment of filling material adaptation on apical and longitudinal images showed a negative association between laser irradiation and gap size. In other words, laser irradiation induced dimensional changes in gutta-percha and MTA fillings alike. Melting of gutta-percha, a naturally thermoplastic material, was expected. However, similar changes in MTA were not foreseen in studies of the association between MTA filling and laser irradiation. We suggest this effect is caused by ablation and, possibly, recrystallization of the mineral aggregate, as occurs in the hard tissues of the tooth.
Changes in phosphorus content after Nd:YAG irradiation suggest an effect of decreasing the solubility of the irradiated surface at the ultrastructural level. 31 However, the reduction of calcium levels also identified after irradiation, which is not consistent with the current literature, suggests that further studies performed under systematically similar methods are required before any questions as to these potential effects of laser on dentin ultrastructure can be elucidated.
Conclusions
From the results of this study, we conclude that: root end resection at 90 degrees effectively reduces the presence of accessory canals; Nd:YAG laser induces changes in dentin morphology and seals canaliculi in the apical region after apicoectomy; marginal adaptation of MTA is good, and, more specifically, marginal adaptation was best in teeth treated with ultrasonic retrograde cavity preparation, MTA retrofilling, and no Nd:YAG laser irradiation; the association of MTA retrofilling and Nd:YAG laser produced dimensional changes in the retrofilling material; and analysis of the chemical composition of the dentin surface showed that phosphor content was increased and calcium content decreased in the Nd:YAG laser-treated groups.
Footnotes
Acknowledgments
This work is partially supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq). Additional support is provided by União Metropolitana de Educação e Cultura (UNIME). We give special thanks to Luis Cardoso Rasquim for many useful insights and suggestions.
Author Disclosure Statement
No conflicting financial interests exist.