
Abstract
Introduction
During cavity preparation, some active bacteria may be left, because of the lack of definitive and reliable criteria for detection of carious dentin and complete elimination of bacteria in the cavity. 3
During the preparation and fabrication procedures of an indirect restoration, there is a greater possibility of bacterial contamination of the cavity. Particularly, bacteria may remain in the smear layer when luting is done with self-etch resin cements. In this way, the adjunctive treatment with antibacterial agents during the luting of the indirect restorations would be advantageous if it did not adversely affect the bonding ability of resin cements. As a result, the potential occurrence of recurrent caries, pulpal inflammation, and postoperative sensitivity is decreased. 4 Chlorhexidine gluconate (CHX) is the most well-known and strong antibacterial material. Moreover, CHX possesses a matrix metalloproteinase (MMP) inhibition property that preserves the integrity of bonding interface over time. 4,5
For >10 years, erbium lasers have been widely employed in many fields of dentistry, as their emission is well adsorbed by hydroxyl groups in water and the biologic tissue containing hydroxyapatite. 6 The newer erbium laser, Er,Cr:YSGG with wavelength 2.78 μm, is more absorbed by hydroxyapatite than water in contrast to wavelength 2.94 μm emitted by Er:YAG. 7
The antibacterial effect of different lasers, 8,9 which was attributed to their capability of removing smear layer and debris, has been previously demonstrated. 10 The bactericidal efficacy of Er,Cr:YSGG has been well documented even at a lower power setting of 1W, 9 and a similar antimicrobial effect as that of CHX on Streptococcus mutans was reported at 0.75 and 1 W. 11
Based on the abovementioned documents regarding the excellent effectiveness of the two antibacterial procedures, it is important to verify whether each of these had no interfering effect on the bonding ability of adhesive resin cements. The objective of this in vitro study was to determine the impact of the laser disinfection on the dentin bond strength of two types of resin cements, self-etch and etch-and-rinse cements, compared with that of CHX application prior to adhesive cementation.
Materials and Methods
Eighty intact human premolars extracted for orthodontic treatment were stored in a 1% chloramine T solution at 37°C for 2 weeks, and then stored in distilled water at 4°C before use. After removing of the roots, the crowns were horizontally mounted in acrylic resin.
The midcoronal dentin surfaces were exposed by removing the occlusal enamel with a diamond saw under water spray. The flat dentin surfaces were polished with 600 grit silicon carbide abrasive paper to provide a standardized smear layer. The prepared teeth were randomly divided into eight groups of 10 teeth each. In the first four groups, ED primer II/Panavia F2.0 (ED/P, Kurary Medical, Tokyo, Japan) was used and Excite DSC/Variolink N (Ex/V, Ivoclar- Vivadent, Schaan, Liechtenstein) was employed in the other four groups for cementation of indirect composites. A total of 80 indirect composite (Gradia, GC, Tokyo, Japan) rods 2 mm in diameter and 3 mm in height were made and prepared for cementation (Table 1).
MDP, methacryloyloxydecyl dihydrogen phosphate;
Bis-GMA, bisphenol A-glycidyl methacrylate
In two control groups, ED/P and Ex/V were used, according to the manufacturers' instructions. In CHX+ED/P and CHX+Ex/V groups, 2% CHX gluconate solution (Consepsis, Ultradent, USA) was applied on the dentin surface for 60 sec before ED primer II in Panavia F2.0, or after acid etching in Ex/V.
In wet laser + ED/P and wet laser + Ex/V groups, an Er,Cr:YSGG laser (Waterlase, Biolase Co., CA) was used according to the following setting: wavelength 2.78 μm, G4 fiber tip with a diameter of 600 μm, focus mode at a focal distance of 1–2 mm, pulse frequency of 20 Hz, pulse duration of 140 μsec, an irradiation time of 5 sec for five times at intervals of 15 sec, scanning the bonding surface, perpendicular to the lased surface. A power of 0.75 W with air pressure of 15% and water pressure of 15% was used. 11 The energy per pulse of 37.5 mJ and energy density of 6.7 J/cm2 were calculated. The irradiated area on dentin surface was a circular area≈3 mm in diameter. Then, the luting was performed as in the respective control groups.
In dry laser+ED/P and dry laser+Ex/V groups, laser irradiation was applied on the dentin surface as described previously, except for lack of water or air cooling.
After cementation according to the manufacturer's instructions for each resin cement (Table 1), the specimens were stored in distilled water at 37°C for 24 h. Shear bond strength was measured with a universal testing machine (Instron, Z020, Zwick Roell, Germany). A knife edge shearing rod at a crosshead speed of 1 mm/min was used to load the specimens until fracture. Shear bond strength in MPa was recorded. All data were analyzed with two way ANOVA, and multiple comparisons were performed using Tukey test at a 0.05 level of significance, using SPSS version 11.5 software (Chicago, IL). After debonding, the fracture modes were evaluated under a stereomicroscope (Zeiss, Germany) at 10×and classified according to the predominant mode of fracture as adhesive fracture at the resin cement–dentin interface, cohesive fracture in the resin cement, cohesive fracture in the dentin, or mixed adhesive and cohesive fracture in the resin cement.
Scanning electron microscopy (SEM) examination
Three additional dentin samples prepared in the same manner as for bond strength test were selected for SEM evaluation as follows: (1) nonirradiated dentin surface (control), (2) dentin surface irradiated by Er,Cr:YSGG, as described for wet laser groups, (3) dentin surface irradiated by the same laser as described for dry laser groups. The samples were prepared and examined under SEM (KYKY, EM 3200, China) at 500×magnification.
Results
The mean shear bond strengths (MPa) and standard deviation in the 8 groups are presented in Table 2. As detected by two way ANOVA, mean bond strength was significantly influenced by disinfectant pretreatment conditions (p<0.001), but not by the cement type (p>0.05). The interaction between the two variables was not statistically significant (p>0.05).
A different superscript indicates statistically significant different values.
CHX, chlorhexidine.
For two resin cements, the lowest bond strength was obtained in the dry laser group (ED/P:10.18±2.67 and Ex/V: 9.64±2.66); there was a significant difference between the dry laser group and the other groups (control, CHX, wet laser) (p<0.001). The other two-by-two comparisons (CHX×control, CHX×wet laser and control×wet laser) were not significant (p>0.05).
The results of fracture analysis indicated that most of the fracture modes in dry laser groups were adhesive fractures. In the six remaining groups, generally all four modes of fracture were observed (Table 3).
ED/P, ED primer II/Panavia F2.0; CHX, chlorhexidine; Ex/V, Excite DSC/Variolink N.
The results of SEM observations are presented in Figs. 1 –3. The unlased sample showed that the dentin surface was covered by uniform and compact smear layer (Fig. 1). The dentin treated by the laser with water/air cooling showed a rough, rugged and clean surface with open tubules (Fig. 2). The dentin surface treated with the laser without water/air cooling showed a damaged surface with micocrack (Fig. 3).
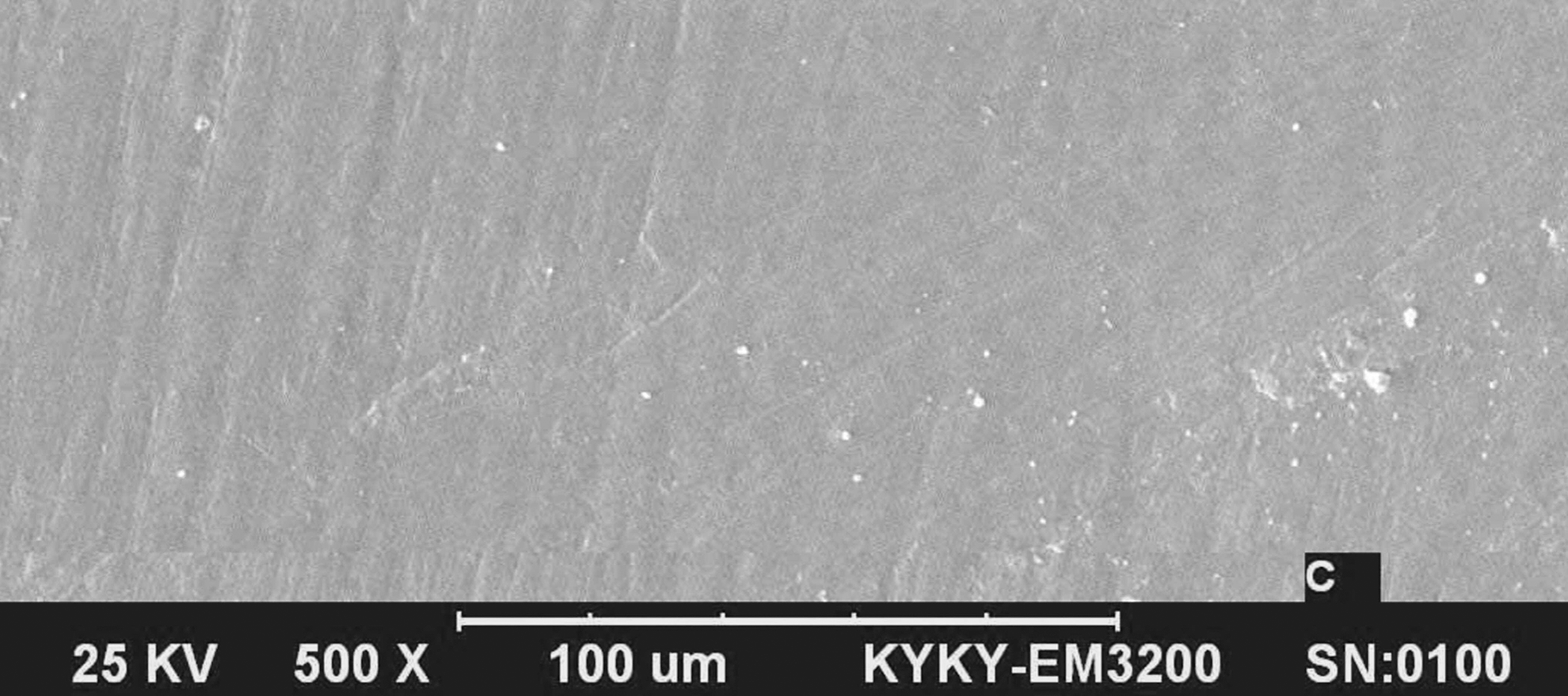
Scanning electron microscopic (SEM) view of the unlased dentin surface (500×)
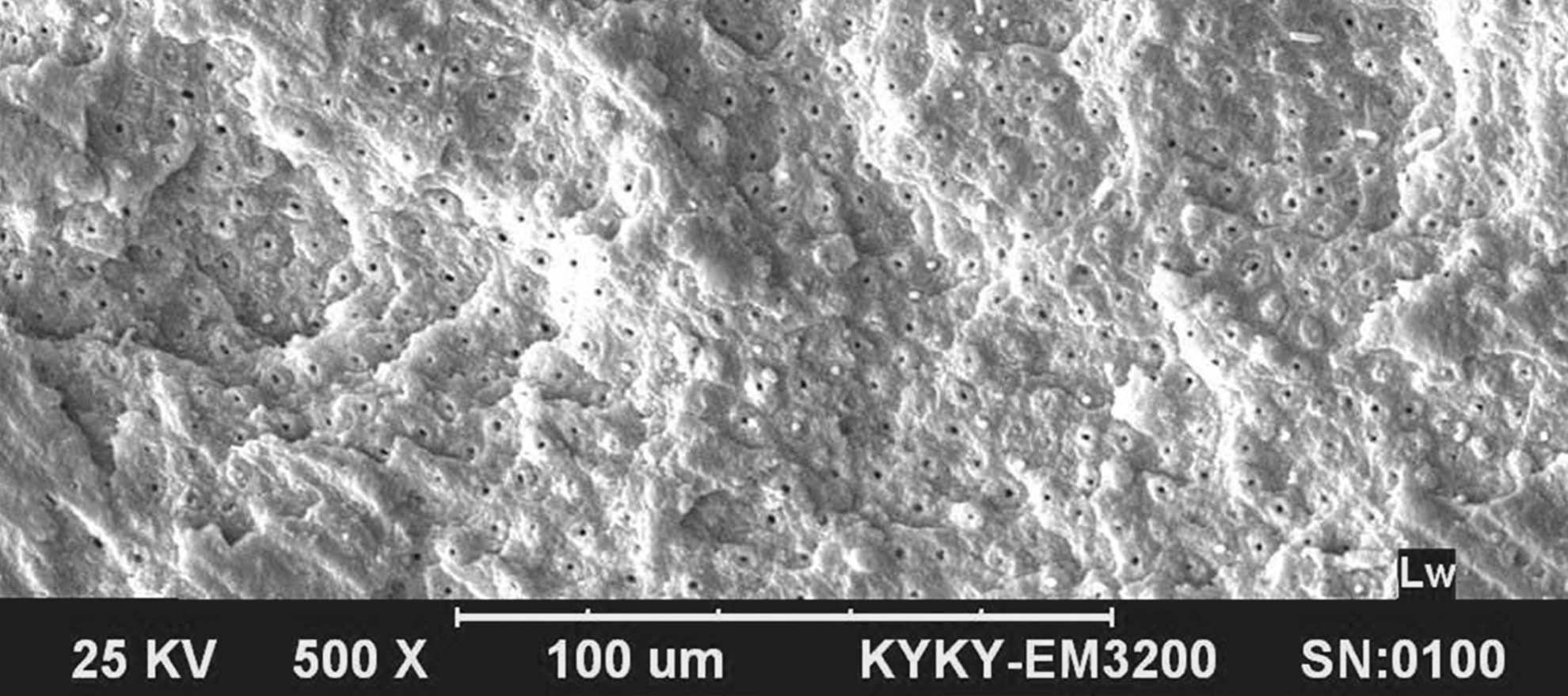
Scanning electron microscopic (SEM) view of the wet laser (0.75 W with water/air cooling, 20 Hz, focus mode, pulse duration of 140 μsec, 6.7 J/cm2) treatment on a dentin surface≈3 mm in diameter (500×)
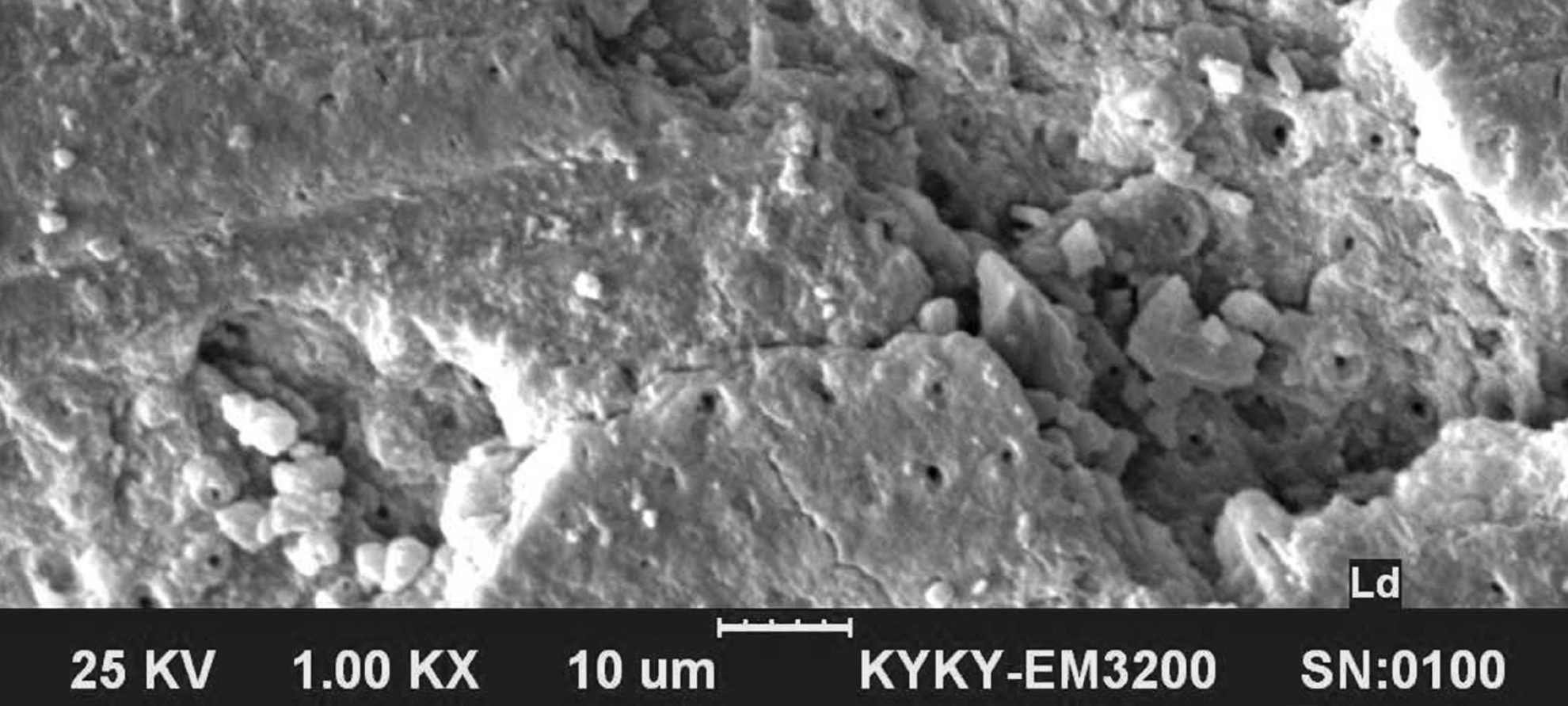
Scanning electron microscopic (SEM) view of the dry laser (0.75 W without water/air cooling, 20 Hz, focus mode, pulse duration of 140 μsec, 6.7 J/cm2) treatment on a dentin surface≈3 mm in diameter (500×)
Discussion
The elimination of bacterial activity with cavity disinfectant agents with no adverse effect on bonding performance of adhesive resin cements could guarantee the long-term success of adhesive indirect restorations. One of the most commonly used antibacterial agents is 2% CHX solution. The reported results by most previous studies have shown that CHX application after acid etching has no effect on the bond strength of etch-and-rinse adhesives. 12 –15 It may function as a re-wetting agent or conserve and regulate the structural integrity of collagen material. 15 Also, the compatibility of CHX with a self-etch adhesive was determined. 13,16 However, a negative effect of CHX on some self-etch adhesives was reported. It was suggested that the interaction between CHX and adhesives may be material specific. 12
According to the result of the current study, CHX did not influence the bonding ability of both resin cements used, ED/P and Ex/V. Similar results were reported for Excite DSC in composite restorations 14 and associated with Variolink 2 in indirect restorations. 17,18 The compatibility of CHX with ED/P and single bond/RelyX ARC resin cement was observed. 18,19 Nevertheless, the negative effect of CHX on the bonding of ED/P in the study conducted by Hiraishi et al. 19 was attributed to 98% water contained in CHX solution or bonding CHX to the loose, superficial apatites within the smear layer. 13,19 However, the dentin surface in the current study as in our previous study was air dried after CHX application.
Bacteria are able to penetrate the periluminal dentin to extent of 1100 μm, whereas the penetration for chemical antibacterial agents is limited to a depth of 130 μm. 20 On the other hand, the antibacterial effectiveness of the laser irradiation is extended even at the depth of 500–1000 μm, 21 thereby favorable covering the existing bacteria in deeper layer of dentin 9,11 and inaccessible parts of tubular network. 21
Erbium lasers are used effectively to ablate dental tissues, achieving cavity preparation. Also, these lasers have been employed with energies below ablation threshold for reducing hypersensitivity, 22 reducing demineralization and susceptibility to secondary caries, 23 and pretreatment to improve bonding effectiveness. 24 Moreover, Er,Cr: YSGG laser with 0.75 and 1 W power outputs could be used as a disinfectant pretreatment following cavity preparation. 11 In the present study, the dentin surface pretreated with the use of Er,Cr:YSGG laser at 0.75 W, in conjunction with water/air cooling (as an antibacterial agent), produced similar bond strength value to that of control group for two resin cements.
The literature has demonstrated divergent results regarding the effect of erbium lasers on the bonding ability of various adhesives. 16,24 –27 In most of them, laser irradiation was employed for ablation, and, occasionally, for modifying the tooth surface to enhance the adhesion, or for cleaning and removing superficial debris, not just for disinfection. 24 –27 The various irradiation parameter settings used such as fluence, power, repetition rate, focal distance, beam spot size, pulse duration, irradiation time, water cooling, and optical characteristics (water and mineral contents) of the lased tissue can explain different effects caused by laser irradiation. 25,26 Therefore, direct comparison of the obtained results of this study with all previous studies is limited.
In the current study, the SEM observations of the wet laser-treated dentin revealed a rough, rugged, and clean surface with open tubules (Fig. 2), whereas in the unlased sample, the dentin was covered by a compact and uniform smear layer (Fig. 1). A similar appearance with open tubules and absence of smear layer was reported when higher power for ablation was used, 27 –29 compared with the low power (0.75 W) used in the current study. In an SEM analysis of dentin treated with different energy parameters, repetition rate, and pulse width of Er:YAG laser, these morphological alternations were produced by all settings. 30 It is noteworthy that the effects created after Er:YAG and Er,Cr:YSGG were reported in a same manner, except for rougher surfaces created by the Er,Cr:YSGG, 31 as the two lasers possess very similar wavelengths. The irregular appearance showing protruded peritubular dentin in intertubular dentin matrix may be the result of higher mineral and lower water contents of the former dentin. 7,27 It seems that this microretentive, altered surface does not show any interfering effect with subsequent bonding procedures. Nevertheless, microcrack formation following higher fluence of laser irradiation for cavity preparation may be responsible for a decreased bond strength reported by some authors. 26,27 According to our SEM evaluation, microcracks and surface damage were observed in the dry laser-treated dentin without water/air cooling (Fig. 3). This observation might be a reason for the decreased bond strength obtained in the group irradiated by dry laser. These harmful effects were not seen for the same low fluence laser- irradiated dentin surface associated with water cooling. The low fluence accompanied with water/air cooling appears to prevent the destructive thermal alterations. However, the laser is not capable of selectively removing hydroxyapatite and exposing collagen fibrils; 28 hence, application of an acidic primer or phosphoric acid after laser irradiation is recommended to produce a microporous and demineralized collagen network. 24,28
In the current study, the low fluence for effectiveness of disinfecting, but not for dentin removal, was employed according to the microbiological study performed by Türkün et al. 11 These authors proposed that the higher fluence for ablation associated with water cooling might lead to more effective antibacterial activity, in addition to the elimination of an additional step for disinfection of the prepared cavity. However, the interaction between the resin cements and dentin prepared by laser fluence for ablation needs to be assessed in other studies with this object.
On the other hand, in the microbiological studies, water cooling was not used during laser irradiation to prevent the risk of spreading the bacteria to the other surfaces. 9,11 It was reported that the presence of water cooling is mandatory for ablation by Er,Cr:YSGG, 29,30 and that dry irradiation at a fluence below the ablation threshold showed no harmful temperature rise in the pulp. 31 The low power (0.75 W) without water cooling used in the current study resulted in decreased bond strengths of the two resin cements, indicating lack of suitability of dry irradiation in clinical practice. In a recent study, 24 the low power of irradiation (0.25 W), particularly without water/air, decreased the bond strength of etch-and-rinse and one-step self-etch adhesives to dentin; however, the laser with water/air cooling did not alter the bonding of a two-step self-etch adhesive. In contrast, Celik et al. 16 demonstrated that Er,Cr:YSGG laser irradiation used for cavity disinfection with energy parameters similar to those applied in the current study improved the bonding of an etch-and-rinse (Adper Single Bond) and a two-step self-etch (Clearfil SE Bond) adhesive. Moreover, CHX decreased the bond strength of Clearfil SE Bond while increasing the bonding of Adper Single Bond adhesive. These contradictory results might be attributed to a difference in the testing methodologies used, and to various laser devices and energy parameters. Also, different inherent properties of the adhesives might play an important role in the interaction between the adhesive associated with resin cement and disinfected dentin by laser or chemical agent. With regard to favorable depth of antibacterial effectiveness of Er,Cr:YSGG laser, this new laser technology at the low fluence with water/air cooling might be safely employed to provide the sterile cavity prior to adhesive cementation. Nevertheless, effects of these antibacterial procedures on the bonding durability of adhesive indirect restorations should be evaluated.
Conclusions
Within the limitations of this in vitro study and based on the obtained results, the use of CHX and Er,Cr:YSGG laser at the low fluence with water/air cooling as the antibacterial agents do not adversely influence the bonding ability of the etch-and-rinse and the self-etch cements. Further long-term in vitro and in vivo studies are required to evaluate the combination of different antibacterial agents and resin cements in luting indirect restorations.
Footnotes
Acknowledgments
The authors thank the vice-chancellery of Shiraz University of Medical Sciences, for supporting the research (Grant #91-4545), Dr. M. Vossoughi from the Dental Research Development Center, for the statistical analysis, and Dr. N. Shokrpour for help with the English in the article.
Author Disclosure Statement
No competing financial interests exist.