
Abstract
Introduction
P
Laser applications have received significant interest in periodontal disease treatment, with their various beneficial characteristics, such as bactericidal and hemostatic effects. 4,5 The diode laser is a semiconductor laser that generally includes a combination of gallium (Ga), arsenide (Ar), and other elements such as aluminum (Al), and indium (In) to convert electrical energy to light energy. The diode laser does not interact with dental hard tissues, making it convenient for soft tissue operations; cutting and coagulating gingival and oral mucosa, soft tissue curettage, or sulcular debridement. 6
Interleukin (IL)-1β plays fundamental role in inflammation and is the key inflammatory mediator in periodontal disease. 7 IL-1β is mainly a pro-inflammatory cytokine that stimulates the expression of many genes associated with inflammation and autoimmune diseases. 8 Gingival crevicular fluid (GCF) concentrations of IL-1β are increased at sites affected by periodontitis, and tissue levels of IL-1β correlate with clinical periodontal disease severity.
The aim of this study was to test the hypothesis that 810 nm laser as an adjunct to conventional periodontal therapy can improve periodontal healing significantly compared with SRP alone; this was done by evaluating both periodontal clinical parameters and GCF IL-1β levels.
Material and Methods
Participants and study design
This study was designed as a single-blinded, randomized-controlled, split-mouth clinical trial. A total of 21 patients (12 females and 9 males, between 26 and 55 years of age) diagnosed with generalized chronic periodontitis according to the American Academy of Periodontology (AAP) 1999 criteria, who were referred for periodontal treatment at the Department of Periodontology at the Faculty of Dentistry of Gaziantep University, were included in the study between February 2012 and November 2012. The study protocol was approved by the ethics committee of the University of Gaziantep, and all patients signed informed consent forms before entering the study.
Inclusion criteria were the presence of at least two incisors or canines at two quadrants (mandible or maxilla) with periodontal pocket depths between 4 and 7 mm.
Exclusion criteria were a history of any systemic diseases that could affect the periodontal therapy outcome (e.g., diabetes mellitus, cancer, metabolic or endocrine diseases), smoking, dental treatment in the past 6 months, antibiotic medication during the 6 months preceding the study, and related teeth with restoration.
Treatment protocols and laser parameters
Periodontal clinical assessments and GCF sample collections at all visits were performed by a single periodontologist (K.Ü.), who was not involved in the patients' subsequent treatment and was blinded to test and control quadrants. The operator who performed the treatments (S.Z.Ş.) was not involved in any evaluation before and after his intervention. With the exception of the periodontal pocket chart, which was necessary to deliver the treatment, he was unaware of the previously recorded data.
All patients received initial periodontal therapy consisting of thorough oral hygiene instructions and full-mouth supragingival and subgingival scaling with a combined use of hand (Hu-Friedy, Chicago, IL) and ultrasonic instruments (EMS, Nyon, Switzerland). One week after this initial therapy, patients underwent two different treatment modalities. Test and control sites were chosen with coin toss randomization. At the test site, patients received SRP and laser treatment; at the contralateral control site they received SRP treatment alone. The entire quadrant was treated according to the procedure, but only one incisor or canine was sampled. Test and control quadrants were treated at the same appointment, and the remaining quadrants were treated the next day. The periodontal pockets of the teeth on the test side were operated with an 810 nm diode laser (Fotona XD-2, Fotona d.d., Slovenia). Laser parameters were Ppeak=2.5 W, duty cycle ½, Pavg=1.25W, 20 Hz and 80 sec/tooth (mesialy, distally, lingually and buccally; 20 sec/site). Laser was applied before root planing. Laser application was performed by a 320 μm contact fiber tip inserted at the bottom of the periodontal pocket, and slowly moved from apical to coronal in a sweeping motion during laser light emission. Briefly, the fiber tip was carbonized before inserting the pocket. When the fiber came in contact with tissue and blood, the debris that immediately accumulated on its tip absorbed the intense infrared laser energy, thus heating the tip and carbonizing the debris and optic fiber end. As laser energy continued to be absorbed by carbon deposits, the tip reached a red hot temperature (∼760°C), causing tissue vaporization. 9 During the laser treatment, protective eyeglasses were used by patient and operator.
Periodontal examination
Clinical periodontal parameters were evaluated at baseline and 1, 3, and 6 months after treatment. The patients' periodontal status was assessed using comprehensive standard periodontal parameters. The evaluated parameters were probing pocket depth (PPD), clinical attachment level (CAL), plaque index (PI), 10 and gingival index (GI). 11 PPD was defined as the distance from the free gingival margin to the bottom of the periodontal pocket. CAL was defined as the distance from the cemento enamel junction (CEJ) to the bottom of the periodontal pocket. PPD and CAL measurements were recorded at six points (mesio-buccal, mid-buccal, disto-buccal, mesio-lingual, mid-lingual, and disto-lingual) around each tooth with a manual periodontal probe (PWD, Hu-Friedy, Chicago, IL).
GCF collection
At baseline and after 1, 3, and 6 months, GCF samples were collected from the same tooth from each quadrant. The selected site was cleared of supragingival plaque, isolated with cotton rolls, and dried with a gentle stream of air to prevent saliva contamination. A sterile prefabricated paper strip (ProFlow Inc. Amityville, NY) was gently inserted into the periodontal pocket until mild resistance was felt, then left in place for 30 sec. Mechanical irritation was avoided, and strips contaminated with blood were discarded. The GCF sample volume was measured with a calibrated Periotron 8000 (ProFlow Inc. Amityville, NY), and then the readings were converted to actual volume (μL) with reference to the standard curve. Upon collection, the samples were immediately stored at −20°C before they were analyzed.
Analysis of IL-1β
The concentration of GCF IL-1β was determined by flow cytometry using the BD™ Cytometric Bead Array (BD Biosciences, San Diego, CA). The frozen GCF strips were eluted in an Eppendorf tube with 300 μL of phosphate buffered saline for 30 min; 50 μL of this solution was used for the GCF analysis. Sample processing and data analysis were performed according to the manufacturer's instructions. Briefly, GCF samples were incubated with the IL-1β cytokine capture beads and PE-conjugated detection antibodies for 3 h at room temperature and protected from light. The samples were washed, and IL-1β levels were assessed using a FACSCanto flow cytometer. Sample results were generated in graphical and tabular format using BD CBA analysis software (BD Biosciences, San Diego, CA).
Statistical analysis
The data were collected, tabulated, and analyzed with SPSS 11.5 (SPSS Corporation, Chicago, IL). The Kolmogorov–Smirnov goodness of fit test was used to check the data for normality assumption. Values obtained from patients were compared using either the paired-samples t test or its nonparametric equivalent, the Wilcoxon signed rank test. The α error was set at 0.05. The power of the study based on 1 mm as a significant difference between pocket probing depth of the groups was calculated to be 0.99, which justified the sample size of 14 patients.
Results
Nineteen out of 21 patients completed the study. Two patients did not attend the first month evaluation, and were, therefore, excluded from the study. Healing was uneventful in all cases. No adverse effects related to the laser irradiation were reported.
Among the 19 patients who completed the study, 12 were female and 7 were male. The mean age plus SD of the participants was 40.23±10.18.
The clinical parameters of the SRP alone and SRP and laser-treated teeth are illustrated in Table 1 and Fig. 1. GCF volume and IL-1β levels are shown in Table 2 and Fig. 2. In both groups, clinical parameters and IL-1β levels decreased significantly at all time points compared with baseline values. There were no significant (p>0.05) differences between the SRP and laser group and the SRP group in any evaluated parameter at baseline. In the 1st month PPD, GI, GCF volume and IL-1β levels were significantly (p<0.05) lower in the SRPand laser group than in the SRP group. At the 3rd month, PPD, CAL, GI, GCF volume, and IL-1β levels were significantly (p<0.05) lower in the SRP and laser group than in the SRP alone group. In the 6th month, PPD, CAL, GCF volume, and IL-1β levels were significantly lower (p<0.05) in the SRP and laser group than in the SRP group.
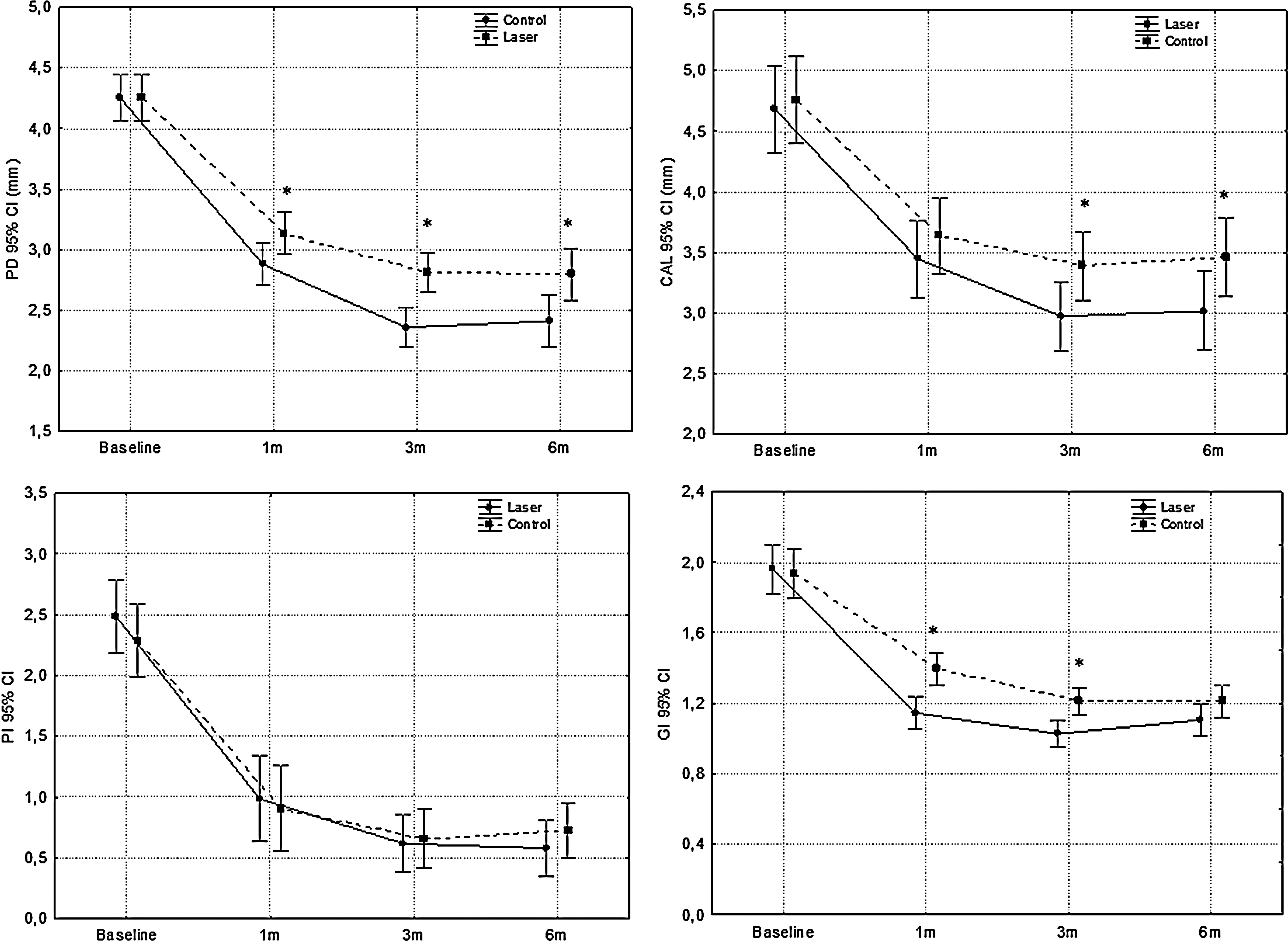
Probing pocket depth (PPD), clinical attachment level (CAL), gingival index (GI), and plaque index (PI) levels of scaling and root planing (SRP) and laser and SRP only groups. *p<0.05.
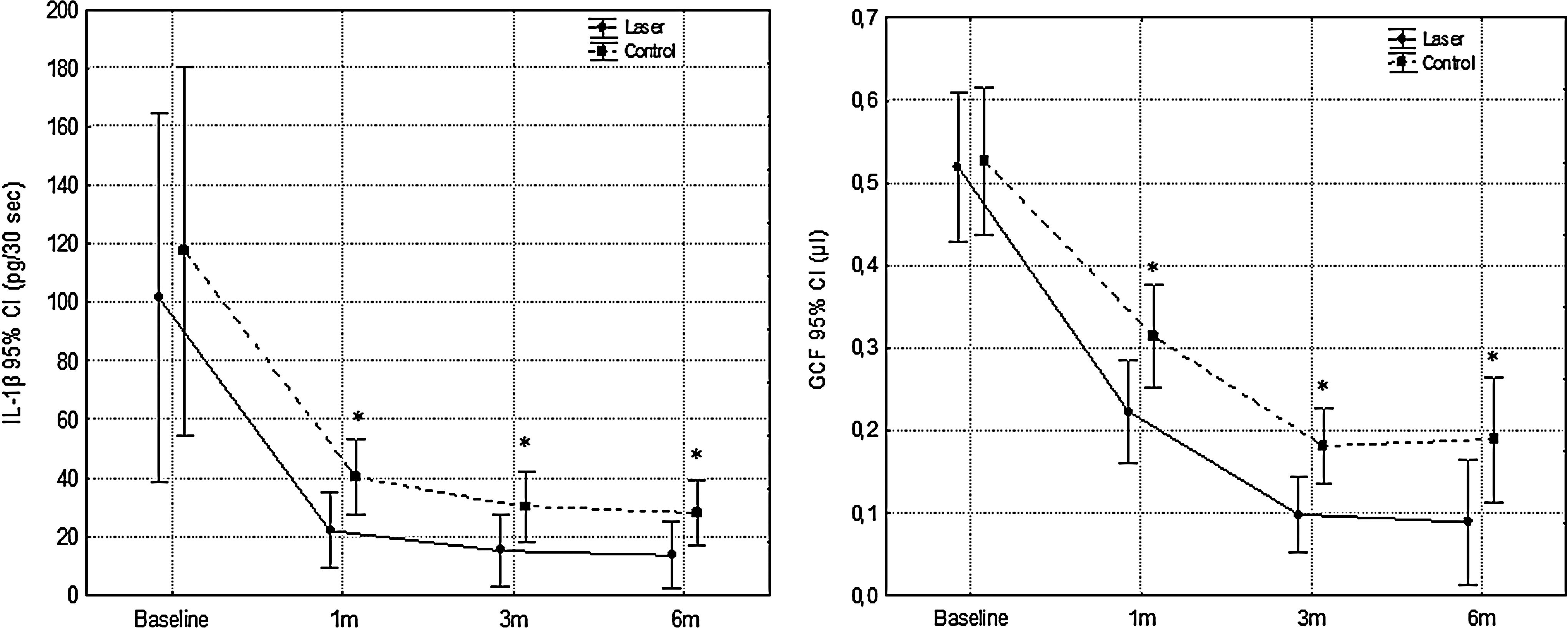
Interleukin (IL)-1β and gingival crevicular fluid (GCF) levels of scaling and root planing (SRP) and laser and SRP only groups. *p<0.05.
Measurements were recorded at six points (mesio-buccal, mid-buccal, disto-buccal, mesio-lingual, mid-lingual, and disto-lingual) around each tooth (n=19) and reported as mean±SD.
Significant difference compared with SRP only group (p<0.05).
Significant difference compared with baseline (p<0.05).
PPD, Probing pocket depth; SRP, scaling and root planing; CAL, clinical attachment level; PI, plaque index; GI, gingival index.
Values are reported as mean±SD (n=19).
Significant difference compared with SRP only group (p<0.05).
Significant difference compared with baseline (p<0.05).
GCF, gingival crevicular fluid; SRP, scaling and root planing.
Discussion
To our knowledge, this is the first study evaluating the effects of an 810 nm laser as an adjunct to periodontal therapy on IL-1β levels. In the present study, both treatment modalities resulted in significant improvements in all clinical and biochemical parameters. Sites irradiated with an 810 nm diode laser showed enhanced healing in all the registered periodontal variables, and decreased IL-1β levels compared with SRP alone.
There are controversial results in the literature regarding the additional benefits of lasers when compared with conventional treatment. Some authors have suggested that lasers are no more clinically beneficial than SRP, 12 whereas others have reported superior results compared with SRP alone. 9,13 –15 The reason for the discrepancy could be attributed to many factors, such as differences in the laser settings, wavelengths, and study designs.
There are several issues concerning the results of this study that should be considered. First, the choice of the correct laser parameters is of great importance. Low energy settings may be ineffective in the complete removal of pocket epithelium, and high energy settings may cause thermal damage to the surrounding tissues. Each individual system has its own effective settings. In this study, the 810 nm laser was set to Ppeak=2.5 W, duty cycle ½, 20 Hz, and applied with a 320 μm fiber. The fiber was introduced like a probe into the periodontal pocket. After the activation of the laser, fiber was slowly moved from apical to coronal in a sweeping motion to avoid thermal side effects. No complications related to laser application were reported with the described parameters and technique. The second difference that could have affected the results was the hot tip technique used in this study. 4 The hot tip technique was chosen because of its low tissue penetration, which permitted the complete removal of the gingival epithelium contaminated by intracellular periodontopathogens, with minimal injury to the underlying lamina propria. 4 In the present study, the transmission of 810 nm light to the tissue was likely to be minimal if it occurred at all, as the carbonized tip absorbed that wavelength and re-emitted much longer infrared wavelengths. Third, in the current study the laser was applied before SRP. Tseng and Liew noted that calculus seemed to separate from the underlying root structure following Nd:YAG laser treatment, which facilitated subsequent removal by scaling. 16 They suggested that SRP after laser therapy may be more efficient in removing root deposition. Furthermore, laser-exposed tooth surfaces exhibit several surface modifications, including charring and carbonization. 17 These alterations may require SRP to achieve the desired end-points of smoothness and detoxification. In this study, 1 week after initial periodontal therapy that included supragingival and subgingival scaling, laser was applied, and after laser irradiation, SRP was performed to achieve a smooth root surface. Laser light of 810 nm is well absorbed in hemoglobin and pigmented tissue. 18 If laser is applied before scaling, because of dark calculus present in the periodontal pocket, there will be excessive heating and tissue damage with the 810 nm laser. On the other hand, in this procedure, subgingival area was instrumented for the second time at the SRPand laser appointment, and this may be evaluated as an interruption to the healing process. Further studies are required to validate the benefits or disadvantages of this application. Fourth, only anterior teeth were evaluated in this study. Tissue changes obtained with nonsurgical periodontal therapy in molar furcation sites are less pronounced than those obtained in nonmolar sites. 19 Moreover, periodontal status and healing after nonsurgical treatment in proximal sites are negatively influenced by the presence of a deep furcation involvement in the adjacent site in the same proximal space. 20 Evaluating the outcomes of periodontal therapy in molar and nonmolar sites together may either result in the misinterpretation of the results, or mask significant differences. For this reason molar sites were not chosen for this study.
IL-1β plays a key role in inflammation and immunity, is closely linked to the innate immune response, and induces the synthesis and secretion of other mediators that contribute to tissue changes and tissue damage. 21 In addition to the improvements in the periodontal clinical parameters, a reduction in the IL-1β levels and GCF volume may indicate the efficiency of the treatment modalities for plaque-related periodontal pathologies. 22 Moreover, previous studies have confirmed that laser radiation has a potential to affect the production of cytokines and growth factors to speed up healing. 15,23,24 In the SRPand laser group, GCF volume and IL-1β levels were significantly lower than in the SRP group throughout the study (p<0.05). The improvement in not only CAL, PPD, and GI, but also GCF IL-1β levels achieved in this study supports previous findings of superior results in laser groups compared with conventional therapy. 4,5,9,13 –15 In previous studies, Eltas et al., Saglam et al., and Qadri et al., reported significant reductions in GCF volume in the laser groups compared with conventional therapy. 13 –15 In addition, Gomez et al., and Qadri et al., found significant reductions in IL-1β levels as a result of laser treatment, compared with conventional therapy. 15,24 We can speculate that as reported in the current study, the biological rationale for these findings indicating the additional benefits of lasers is the result of de-epithelization of the pocket epithelium and the antimicrobial effect of the laser light. Kreisler et al. suggested that higher reduction in PPD was probably related to the de-epithelization of the periodontal pockets, leading to an enhanced connective tissue attachment. 25 Our results and those of recent studies support this notion. 13 Moreover, the improvement in periodontal parameters, in particular PPD and GI on the laser side in our study, may be explained by the decrease in periodontal inflammation in these sites, as determined by reduction in GCF volume and IL-1β levels. In addition, the antimicrobial effect of diode lasers was previously shown by Fontana et al. 26 Although no microbial evaluation was performed in the current study, the antimicrobial effect may also contribute to the better treatment outcomes reported in laser groups. Although the beneficial effects of laser applications as an adjunct to periodontal therapy are now apparent and supported by a number of studies some authors have found that lasers have no clinical benefit over SRP. 12 The discrepancy between the findings of the current study and those reporting negative results may be the result of different laser parameters and laser application techniques, as previously mentioned.
Conclusions
In conclusion, within the limitations of this study, use of diode lasers as an adjunct to SRP produced significant improvements in clinical parameters as well as GCF IL-1β levels in the 6 month study period. New studies designed to uncover the underlying mechanisms responsible for enhanced treatment outcomes are needed to validate these findings.
Footnotes
Acknowledgments
The authors thank Digdem Taskaya, Application Specialist, BD Biosciences, for her valuable support during the biochemical analyses, and Yrd. Doç. Dr. Seval Kul for the statistical analysis. This study is supported by a grant from Gaziantep University DHF.09.03.
Author Disclosure Statement
No competing financial interests exist.