
Abstract
Introduction
E
Traditionally, numerous strategies including mechanical (stainless steel hand files, NiTi rotary systems), chemical (solvents), and thermal (heat carrying instruments) techniques, and the combination of these techniques have been reported to eliminate root filling materials. 4,5 However, none of these techniques alone or in combination can completely remove the filling materials from the root canals. 6 –11 In addition, these methods may present some serious side effects, such as periapical tissue irritation, periapical inflammation, and postoperative flare-ups caused by excessive apical extrusion of root filling materials. 12 Therefore, more effective techniques are still requiring future investigations.
Additional methods, such as sonic, ultrasonic, and some laser devices, have been reported to improve the removal efficacy of root canal filling materials. 13 –15 Within laser-activated approaches, photon-induced photoacoustic streaming (PIPS) is a technique that was primarily developed for cleaning and debriding the root canal system. 16 This system uses a short pulse rate (50 ms) to create peak power spikes, which do not seem to cause thermal damage. 16 Previous studies showed that PIPS was significantly better than traditional techniques in debriding the root canal and removing calcium hydroxide paste medication. 16 –18 Therefore, PIPS may effectively remove filling remnants after the standard retreatment procedures.
To our knowledge, no studies have investigated the efficacy of PIPS in removing filling material residues from oval root canals. Therefore, the aim of this in vitro study was to evaluate the efficacy of PIPS, EndoActivator (sonic), and an ultrasonic technique for removal of gutta-percha and endodontic sealer after mechanical retreatment of oval root canals, using high-resolution micro-CT and scanning electron microscopy (SEM).
Materials and Methods
Twenty-eight freshly extracted human maxillary first premolars with completely developed apices and a single straight, oval-shaped root canal were selected and stored in a 0.1% thymol solution until further processing. Periapical radiographs were taken in the buccolingual and mesiodistal directions at 80 kV and 100 mA to confirm the presence of a single straight root canal and calculation of the canal diameter ratio. The oval root canal was defined as a cross-section ratio of long (buccolingual): short (mesiodistal) diameter ≥ 2.5 at 5 mm from the apex. 19 Teeth that presented previous endodontic treatment or fracture lines were excluded.
Canal instrumentation
The selected teeth were decoronated using round diamond burs in a high-speed hand piece at a length of ∼16 mm. A stainless steel size 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) was inserted into the canal until the tip of the file just reached the apical foramen. The working length (WL) was determined to be 0.5 mm shorter than this length. All canals were prepared using the crown-down technique, using ProTaper NiTi rotary instruments (Dentsply Maillefer, Ballaigues, Switzerland) following manufacturer's instructions. The canal instrumentation was completed with an F2 ProTaper file. Canals were irrigated with 2 mL of 3% sodium hypochlorite solution (NaOCl) using a 30-gauge blunt-tip needle (Terumo Corporation, Leaven, Belgium) at every change of file. After completion of canal instrumentation, canals were irrigated with 6 mL of 17% ethylenediaminetetraacetic acid (EDTA) solution, followed by flushing with 2 mL of 3% NaOCl. After aspiration of irrigation solution in the pulp chamber, the canals were dried using sterile paper points (Dentsply/Herpo, Petrópolis, Rio de Janeiro, Brazil).
Canal filling
Obturation of all root canals was performed using the continuous wave of condensation technique and the Touch'n Heat device (SybronEndo, Orange, CA), according to manufacturer's specifications. Briefly, a size 35 taper 0.06 gutta-percha master point (Dentsply, Rio de Janeiro, Brazil) coated with AH Plus sealer (Dentsply De Trey, Konstanz, Germany) was fitted with tug-back to the WL. The root canals were subsequently filled with Obtura II (SybronEndo). To obtain approximately the same volume of gutta-percha filling, a 14 mm length was uniformly filled from the apex of the root in each canal. The quality of the root canal filling was assessed using both mesiodistal and buccolingual direction radiographs. Specimens showing any voids in the obturation mass were discarded and replaced. The access cavities were sealed with Caviton (GC, Tokyo, Japan). All specimens were stored at 37°C and 100% relative humidity for 1 week to ensure that the sealer was completely set.
Removal of canal filling material
After the temporary fillings were removed, the mechanical re-instrumentation of all root canals was removed using a standard protocol. First, the 3 mm length of filling materials from the cervical part of the root canal was removed using Gates Glidden burs size #3 (Dentsply, PA, USA). Then, the ProTaper universal retreatment system (Dentsply Maillefer, Ballaigues, Switzerland) was used to remove the filling material. The D1 (ISO 30, 0.09 taper), D2 (ISO 25, 0.08 taper) and D3 (ISO 20, 0.07 taper) files were sequentially used for the coronal, middle, and apical thirds, respectively. The ProTaper Ni-Ti rotary retreatment files (Dentsply Maillefer, Ballaigues, Switzerland) were used at 300 rpm and with a torque of 2 N/cm in a crown-down motion. The canals were irrigated between files with 2 mL of 3% NaOCl, followed by final irrigation with 5 mL of 17% EDTA. The criteria for completion of mechanical retreatment were as following: (1) the last file D3 reached the full WL, (2) no filling material covered the flutes of the files, and (3) the final irrigation solution was free of visible debris. 20 The specimens were then randomly divided into four groups of seven teeth each, and processed as follows.
Group 1 (n = 7): Control group
No further procedure was performed, and samples were ready for evaluation.
Group 2 (n = 7): PIPS procedure
Each specimen was irradiated using a 2940 nm Er.YAG laser (Fidelis AT, Fotona, Ljubljana, Slovenia), 1 W, 20 Hz, and 50 mJ per pulse with a 14 mm long and 300 μm diameter quartz tip. The pulse duration was 50 μs. The water and air spray of the laser units were turned off. The laser tip was fixed in place in the coronal part of the canal without touching the inner surface of the main canal wall and activated for 20 sec (3 × 20 sec).
Group 3 (n = 7): Sonic (EndoActivator) procedure
Each specimen was activated using EndoActivator (setting: headpieces 10,000 cycles/min) with a sonic tip (size 20, taper 0.02) (Dentsply Tulsa Dental Specialties, Tulsa, OK). The sonic tip was placed into the canal 1 mm short of the WL without touching the walls and activated for 20 sec (3 × 20 sec).
Group 4 (n = 7): Ultrasonic procedure
Each root canal was activated using an ultrasonic device on a 25% power setting in E mode 28 kHz (EMS, Le Sentier, Switzerland) and delivered using an ultrasonic tip (size 20, taper 0.02) (ESI Instrument, EMS, Le Sentier, Switzerland). A smooth ultrasonic file was placed into the canal to 1 mm short of the WL without touching the walls and activated for 20 sec (3 × 20 sec).
Irradiation and activation
Before irradiation or activation in groups 2, 3, and 4, the root canal was filled with 2 mL of 3% NaOCl solution. During irradiation or activation, the pulp chamber was refreshed using 3% NaOCl solution when the coronal reservoir level became low. The above-described irradiation/sonic/ultrasonic procedures were repeated three times for a total of 60 sec. All procedures were performed by the same endodontist.
Micro-CT measurement and evaluation
A high-resolution micro-CT (SkyScan 1172, Aartselaar, Belgium) was used at 80 kV, 100 mA and an isotropic resolution of 20 μm to scan the sample before instrumentation (scan 1), after gutta-percha filling (scan 2), after mechanical re-instrumentation (scan 3) and after a second re-instrumentation (scan 4). Each sample was placed in to a microcentrifuge tube (SPL Life Sciences, Pocheon-Si, Korea) that served as a sample container during the scanning procedure. A series of cross-section images were acquired with 20 μm pixel sizes. The region of interest was selected from the cementoenamel junction to the apex of the root. The original gray scale images in TIFF format were then processed using NRecon software (Version 1.6.9.18 Bruker micro-CT, Kontich, Belgium) to build a three-dimensional (3D) reconstruction of the sample. The reconstructed images in BMP format were then further processed using the SkyScan Analyzer software package (Bruker micro-CT, Kontich, Belgium) including a CT-analyzer program (CTAn, Version 1.14.4.1) for 2D and 3D quantitative analysis of reconstructed volumes, and a CT-volume program (CTVol, Version 2.2.3.0) for 3D visualization of scanned objects. The volume (in mm3) of the root canal, the filling materials after canal filling, the remaining filling materials after mechanical retreatment, and the remaining filling materials after additional irrigation/irradiation procedures were obtained from scans 1, 2, 3, and 4, respectively. The cleaning volume for the filling materials used in the additional irrigation/irradiation procedures was calculated by subtracting the volume of the remaining filling materials after the additional irrigation/irradiation procedures from the volume of the remaining filling materials after the mechanical retreatment.
SEM evaluation
After micro-CT scanning, all samples were grooved longitudinally in a buccolingual direction using a diamond disc and a high-speed hand piece, and then root canals were split into halves using a bone hammer. Samples were then dehydrated using increasing ethanol concentrations, dried at the critical point and sputter-coated with gold (Magnetron Ion Sputter Metal Coating Device, Msp-2S, IXRF System, Inc. MA, Japan). The presence of sealer remnants in the coronal, middle and apical thirds of each sample were evaluated using SEM (Hitachi, Tokyo, Japan) at 1000× magnification. The SEM images were rated by two calibrated examiners using the following scale: 0, no residue; 1, small amount of residue (≤20% of the surface covered); 2, moderate amount of residue (20–60% of the surface covered); and 3, large amount of residue (>60% of the surface covered). 21
Statistical analysis
Statistical analysis was conducted using SPSS software (SPSS 20.0 for Windows, SPSS, Chicago, IL). The normality and the equality of the data's variance were evaluated using the Shapiro–Wilk test and Levene's test, respectively. The effectiveness of retreatment among the groups was compared using Kruskal–Wallis H and Mann–Whitney U tests. The differences of the remaining filling material before and after additional activation techniques within each group was compered using Wilcoxon signed rank test. The level of significance was set as p < 0.05.
Results
Micro-CT imaging and evaluation
The percent volume of the remaining filling materials in the full root canal length and all thirds (coronal, middle, and apical) are shown in Table 1. The filling material volume reductions are summarized in Table 2. Overall, the PIPS technique was superior in removing filling materials compared with the sonic (EndoActivator), ultrasonic, and control groups (p < 0.05). However, none of the retreatment techniques completely eliminated all filling materials from the root canal (Fig. 1).
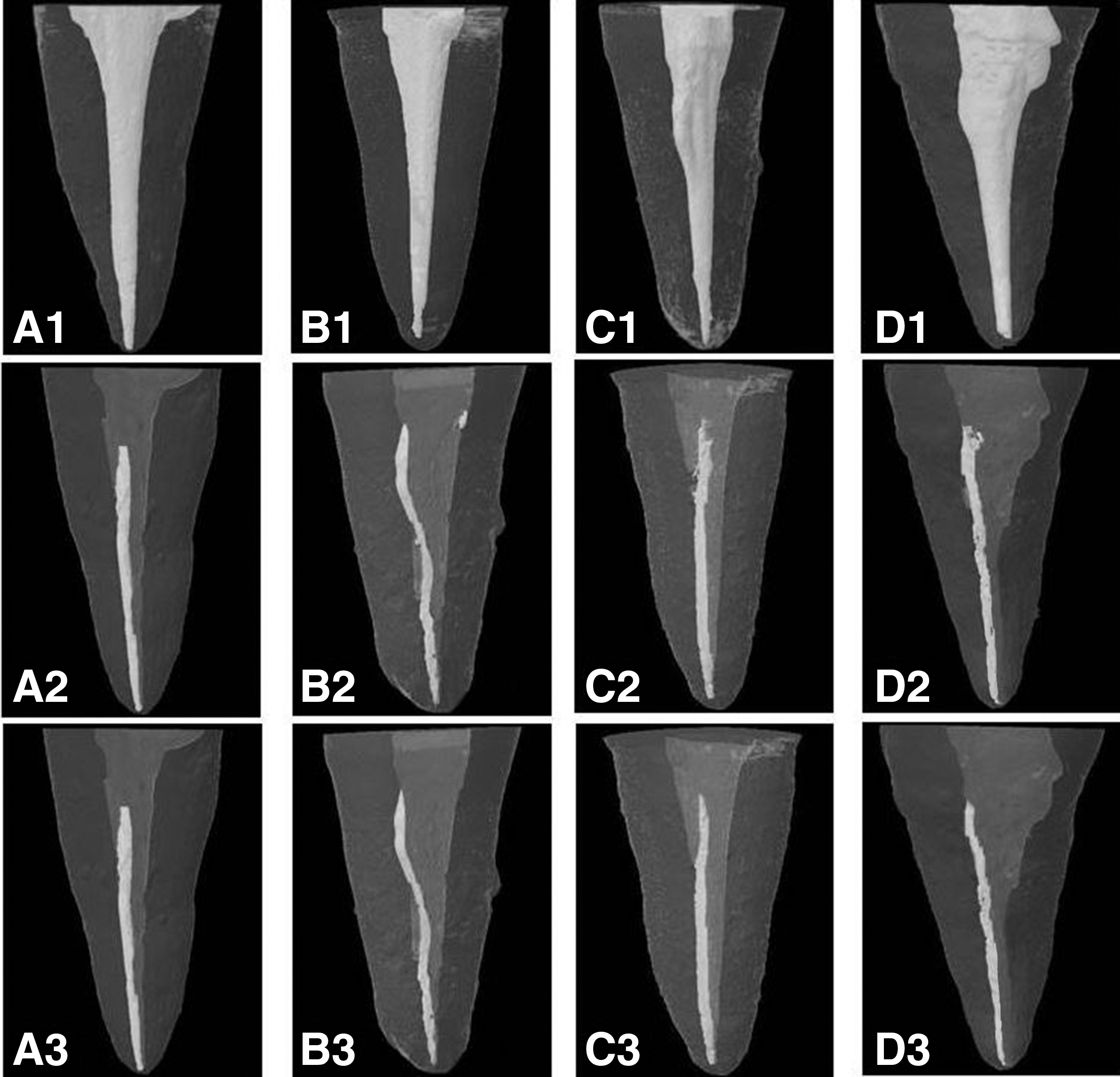
Three-dimensional reconstruction of micro-CT scans showing filling material after obturation, mechanical retreatment, and additional activation of NaOCl with different devices. Control (A1, after obturation; A2, after mechanical retreatment; A3 after additional irrigating procedure); EndoActivator (B1, after obturation; B2, after mechanical retreatment; B3, after additional irrigating procedure); ultrasonic (C1, after obturation; C2, after mechanical retreatment; C3, after additional irrigating procedure), and photon-induced photoacoustic streaming (PIPS) (D1, after obturation; D2, after mechanical retreatment; D3, after additional irrigating procedure).
Ranking: there were significant differences (p < 0.05) between groups with different ranks at the same level.
PIPS, photon-induced photoacoustic streaming.
Ranking: there were significant differences (p < 0.05) between groups with different ranks at the same level.
PIPS, photon-induced photoacoustic streaming.
After the mechanical retreatment (ProTaper universal retreatment system), the remaining filling materials ranged from 2.37 ± 0.49 to 2.46 ± 0.57 mm3, and there were no differences among the four groups (p > 0.05). This was followed by the additional activation procedures, and more filling materials were removed in the sonic, ultrasonic, and PIPS groups in all thirds than in the control group (p < 0.05). In all four groups, the remaining filling materials located mostly along the long axis of the oval canals (Fig. 2). In addition, in the coronal and middle thirds, the remaining filling materials in the PIPS group were significantly lower than those in the sonic and ultrasonic groups (both p < 0.05), and the amount remnants were also significantly lower in the ultrasonic group than in the sonic group (p < 0.05). In the apical third, significantly more filling materials were removed in the both PIPS and ultrasonic groups (0.11 ± 0.04 and 0.09 ± 0.03 mm3, respectively) than in the sonic group (0.03 ± 0.01 mm3, both p < 0.05), whereas there was no significant difference between the PIPS and the ultrasonic groups (p > 0.05). The Wilcoxon signed rank test showed that in the PIPS and ultrasonic groups, the amount of the remaining filling materials in all thirds was significantly less after additional activation technique compared with before additional activation techniques (all p < 0.05), and that there were no significant differences in the remaining filling materials between before and after sonic irrigation technique (all p > 0.05).
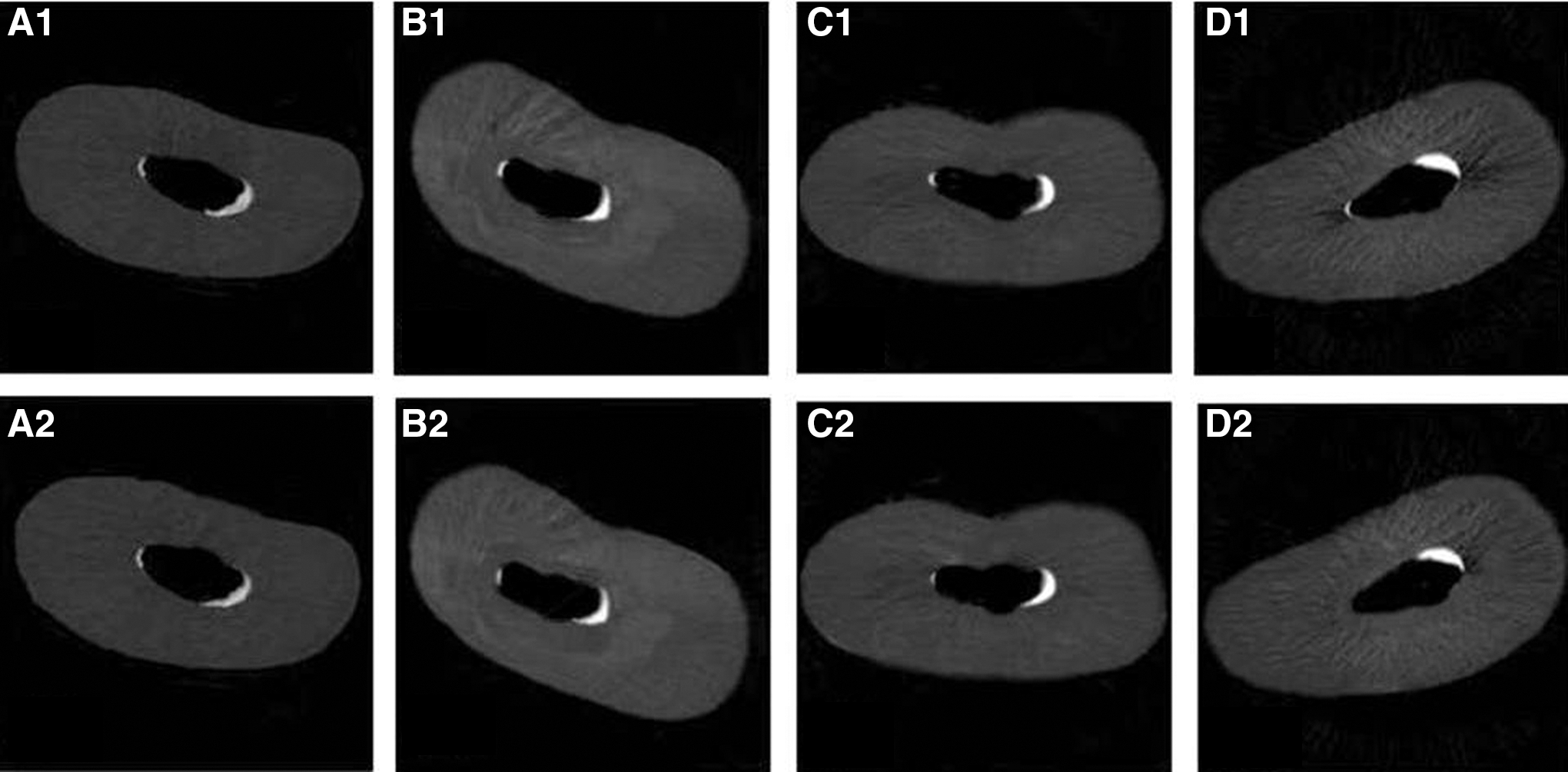
Cross-sectional micro-CT image of residual filling material before and after additional activation of NaOCl with different devices. Control (A1, before irrigation; A2, after irrigation); EndoActivator (B1, before irrigation; B2, after irrigation); Ultrasonic (C1, before irrigation; C2, after irrigation), and photon-induced photoacoustic streaming (PIPS) (D1, before irrigation; D2, after irrigation).
SEM observation and evaluation
The distribution of the remaining filling material scores in all thirds is presented in Table 3. There was low interexaminer variability in the SEM image evaluation (κ value = 0.95). In the coronal and middle thirds, the mean score of the residual filling material in the PIPS group was significantly lower than that in the ultrasonic and sonic (EndoActivator) groups (both p < 0.05), and it was significantly lower in the ultrasonic group than in the sonic group (p < 0.05). In the apical third, there was a significantly lower residue score for both the ultrasonic and PIPS groups (1.65 ± 0.33 and 1.76 ± 0.26, respectively) than for the sonic group (2.61 ± 0.43, both p < 0.05), but there was no statistical difference between the ultrasonic and PIPS groups (p > 0.05). All three experimental groups were significantly different from the control groups in the apical, coronal, and middle thirds (all p < 0.05). No groups demonstrated complete filling material removal from the canals (Fig. 3).

Scanning electron microscopy (SEM) images of residual filling material in the coronal, middle, and apical thirds of the root canal after additional activation of NaOCl. Control (A1, coronal third; A2, middle third; A3, apical third); sonic (B1, coronal third; B2, middle third; B3, apical third); ultrasonic (C1, coronal third; C2, middle third; C3, apical third), and photon-induced photoacoustic streaming (PIPS) (D1, coronal third; D2, middle third; D3, apical third).
Ranking: there were significant differences (p < 0.05) between groups with different ranks at the same level.
PIPS, photon-induced photoacoustic streaming.
Discussion
Complete elimination of gutta-percha and sealer used in previous fillings is essential, and it ensures thorough disinfection and sterilization of the root canal systems, which is a crucial step in successful endodontic retreatment. 22 Infected pulp tissue, bacteria, or their products, which may be hidden beneath the residual canal filling material or entangled with the remnants, may largely reduce the cleaning and disinfecting capacities of the mechanical and chemical procedures. 23 Consequently, the unremoved pulp tissue, bacteria, and their products are major causes of persistent periapical infection. 24 Therefore, mechanical (stainless steel hand files, NiTi rotary systems), chemical (solvents), and thermal (heat carrying instruments) techniques and then combinations are used clinically. To date, there are no treatment regimens that could produce canal walls completely free of all root-filling residue. 25 Compared with hand files (Hedstrom files and K files) and other NiTi rotary instruments (ProFile, Mtwo and D-RaCe), the ProTaper universal rotary retreatment system can remove root canal filling material more quickly and effectively, but it is not able to completely eliminate filling materials. 26 –31 Additionally, high anatomical variability and complexity of oval-shaped root canals, obviously increasing the difficulty of the root canal cleaning and shaping, represents a major challenge and requires additional procedures in root canal retreatment. 10,32,33 In the present study, sonic (EndoActivator), ultrasonic and laser (PIPS) activation were examined as additional methods for removing remnant fillings from the oval-shaped root canal of the maxillary first premolar after the ProTaper universal rotary instrumentation.
Various techniques have been used to evaluate the residual filling materials left in the root canal after retreatment. SEM can often provide direct topographical and morphological data on the filling materials, especially the presence of sealer on the surface of the root canal walls. 34 Micro-CT can provide 3D information and accurate quantification data (volume) of the remaining filling materials. 20 There are two major techniques that are used for this type of study, as they are complementary and can provide sufficient data for analyzing the removal of filling materials from the root canal system. Therefore, the present study used both SEM and micro-CT to assess the effectiveness of the three additional activation techniques on removing the remaining filling materials.
SEM and micro-CT analysis results showed that additional sonic (EndoActivator), ultrasonic, and laser (PIPS) procedures significantly eliminated the remaining filling materials from the maxillary first premolars compared with the control group. Among the three experimental techniques, the laser (PIPS) activation procedure was the most effective of the three techniques at removing the filling remnants from the canal walls. Similarly, previous studies have shown that PIPS was effective at debriding and cleaning the root canal surfaces. 35,36 For example, Lloyd et al. found that PIPS was more effective at eliminating organic debris from the canal than was standard needle irrigation. 17 Our recent study also showed that PIPS irrigation techniques obtained a greater reduction of Ca(OH)2 and better cleanliness of the isthmus area than EndoActivator and needle irrigation. 18 All of these findings indicated that PIPS could be a highly promising laser application in endodontics and other areas of dentistry.
The PIPS mechanism in endodontics consists of an Er:YAG laser (wavelength of 2940 nm) with a 14 mm long and 300 μm diameter quartz tip at the pulp chamber. 16 This technique is mainly based on photoacoustic and photomechanical effects rather than on photothermal effects. 37 Therefore, it is reasonable to speculate that the better performance of PIPS in removing the residue from filling material was a result of the cavitation effect through formation of explosive vapor bubbles. 36 Moreover, Er:YAG laser energy exhibits the highest absorption rate in water and hydroxyapatite, which causes evaporation of fluid to allow for movement of the of fluid through the root canal system. 38,39 In addition, interaction of each impulse with the water molecules creates successive shock waves that result in the formation of a powerful streaming fluid, 16 which might facilitate the effectiveness of PIPS in removing the filling materials.
Results from the present study showed that an ultrasonic technique was superior to the sonic (EndoActivator) technique in removing filling material residue, especially in the coronal and middle thirds of the root canal. This result is in agreement with previous studies reporting that ultrasonic activation was significantly better at eliminating dentin debris than was sonic activation. 40 Theoretically, the mechanism of ultrasonic cleaning is based on the transmission of acoustic energy from an ultrasonically vibrating file to an irrigant, which means that high-frequency ultrasonic waves cause acoustic streaming and cavitation of the irrigant to remove the filling materials on root canal walls. 41 EndoActivator works by carrying a sonically driven tip to activate the irrigant to remove the filling materials. 42 A higher frequency wave results in a higher irrigant flow rate. 43 Therefore, a higher frequency ultrasonic system is expected to be more effective at removing filling materials than a sonic device.
In the present study, the additional use of PIPS and ultrasonic techniques after using the ProTaper Universal retreatment system resulted in a significant improvement in removing the remaining filling materials. Similarly, the additional effect of removing the residual filling materials were also observed by the use of the self-adjusting file (SAF) after ProTaper Universal retreatment system and R-Endo retreatment rotary instruments. 44,45 In contrast, arques da Silva et al. reported that the additional use of ProTaper F4 after using the ProTaper Universal retreatment system did not produce significant improvement in removing the remaining filling materials. 31 In addition to the laser or mechanical additional applications, Bodrumlu et al. reported that the combination of Gates Glidden drills (size 4) and Hedstrom files (size 30) could also be effectively eliminated the filling materials, especially for the straight root canal. 46 However, compared with these mechanical or manual additional techniques, PIPS, worked by only inserting the laser tip into the coronal third of the canal, might have a lower risk of instrument fracture or other complications.
None of the experimental techniques completely eliminate filling material residues from the maxillary first premolar root canals; filling materials in amounts ranging from 1.46 ± 0.30 to 2.21 ± 0.46 mm3 remained in the canals. This finding is in harmony with those of previous studies. 6 –8,30 Moreover, all three experimental techniques showed better efficacy in removing filling materials from the coronal and middle thirds compared with the apical third of the canal. Conversely, Abramovitz et al. reported that a self-adjusting file was more effective in removing residual gutta-percha from the apical section than the coronal and middle sections of the mesial canals of mandibular molar after using ProTaper Universal retreatment files. 30 This is likely because of the different techniques applied. When the PIPS tip was placed only in the coronal part, its photoacoustic shock wave may weaken over the distance to the apical one third, and, therefore, the effectiveness of PIPS in removing filling materials from the apical part was decreased. Similarly, Zhu et al. found that PIPS was more effective in removing the smear layer and debris in the coronal and middle thirds than in the apical third. 47 It is expected that ultrasonic and sonic techniques will be less effective in removing filling material in the apical region, and this was likely a result of the reduction in the acoustic microstreaming and/or cavitation effect after the ultrasonic file or sonic tips entered the apical vapor lock. 41,42 As mentioned, the optic tip of the PIPS device was only placed in the coronal third of the canal, which was likely to preserve the root structure. 16 To sufficiently remove the filling materials in the apical third of the root canal, further studies shoud be conducted to optimize PIPS parameters and the PIPS tip location in the root canal.
Limitations
Limitations of the present study should be noted. First, this study was conducted on teeth with straight oval root canals, and the findings cannot be directly applied to teeth with curved root canal systems, because root curvature is a crucial factor in affecting the efficacy of root canal instrumentation. 9 Second, similar to other similar studies, 24,31,35 decoronating teeth, which is impossible in the daily practice, were done in the present study in order to standardize the specimens; therefore, the conclusion of the current study cannot be directly extended to clinical conditions. Further research is needed to complement the results of the present study.
Conclusions
The additional use of PIPS for the activation of NaOCl was superior to sonic and ultrasonic techniques in removing the remaining filling materials after standard retreatment procedures using the ProTaper universal retreatment system. However, none of the experimental techniques completely removed the filling remnants from the root canal of the maxillary first premolars.
Footnotes
Author Disclosure Statement
The authors declare no competing financial interests.