
Abstract
Introduction
V
Phototherapy, as monotherapy or in combination with topical corticosteroids, topical calcineurin inhibitors, or vitamin D3 analogues, is considered the “gold standard” treatment of vitiligo, being effective in ∼50–75% of patients with recent onset of the disease. A number of ultraviolet (UV) wavelengths have been proposed, including psoralen plus UVA (PUVA), UVA1 (340–400 nm), UVA2 (320–340 nm), broadband (BB)-UVB (290–320nm), narrow-band (NB)-UVB (311–313nm), and monochromatic 308 nm excimer laser (MEL). 4 –8
Recently, a 355 nm monochromatic UVA1 laser source was demonstrated to be well tolerated and to determine positive clinical response patients affected by psoriasis. 9,10 The aim of the present study was to evaluate this 355 nm UVA1 monochromatic laser in the treatment of vitiligo.
The potential of the 355 nm wavelenghth, capable of a deeper penetration in the skin, may be more effective because of its immunomodulatory action. Further studies should be conducted comparing this laser to the classic NB 311 nm phototherapy or the 308 nm excimer laser.
Patients and Methods
Seventeen consecutive, unrelated, unselected patients (7 men and 10 women), 18–72 years of age (mean age: 39.23 years) were included in this open-label, prospective study. Five patients were affected by generalized vitiligo, seven showed acrofacial involvement, and five presented segmental vitiligo. The Fitzpatrick skin types were in the range II–IV. Disease mean duration was 6.56 years (range 0.8–31). Demographic data, including previous treatments, are summarized in Table 1. None of the patients had a history of skin cancers, recent radiotherapy, or current immunosuppressive treatment. Among women, none was pregnant or breast-feeding.
NB-UVB, narrowband UVB light therapy; MEL, monochromatic excimer laser.
The local ethical committee approved the study, and all patients gave written informed consent for treatment and photographs. Patients were instructed to wear protective glasses while vitiligo areas were selectively treated, and were instructed to avoid use of any topical or oral medication during treatment. Morphologic Wood's lamp examination and photographic evaluations were performed at the first visit, and at every session during therapy and follow-up. Adverse events were eventually documented after each session. Efficacy was assessed at each visit by the percentage of repigmentation in the treated area, with a scale ranging from 0 (no repigmentation) to 1 (poor repigmentation, 1–25%), 2 (moderate repigmentation, 26–50%), 3 (good repigmentation, 51–75%), and 4 (excellent repigmentation, 76–100%).
The system used (Alba 355nm - Elettronica Val Seriana s.p.a., Casnigo, Italy) is a solid-state laser that uses an active medium and a Neodymium-doped Yttrium Orthovanadate (Nd:YVO4) crystal. The light emitted by the Nd:YVO4 has a 1064 nm wavelenghth that is filtered producing a second (532 nm) and third (355 nm) harmonic wavelength delivery. The latter fits in the UVA1 light range, which is therapeutic for different skin diseases. The technology used has a 2.5 mm spot, and a scanning system designs variously shaped bidimensional figures that may cover the target lesions. This laser can deliver a fluence of 100 J/cm2 in 12 sec.
The therapeutic protocol consisted of the administration of moderate to high fluences (80–140 J/cm2), according to skin type and morphology. All patients were treated twice a week, never on consecutive days, without increasing the UV dose, for 8 weeks, followed by 12 weeks of observation to assess the stability of repigmentation. Cumulative doses, for a total of 16 sessions, ranged between 1280 and 2240 J/cm2.
Results
All patients completed 8 weeks of treatment. Results are summarized in Fig. 1. Clinical response was not body site or disease duration dependent. A clinical case of good repigmentation is shown in Fig. 2A and B. During the 12-week treatment-free follow-up period, the proportion of pigmentation achieved was stable and maintained in all patients. Treatment was well tolerated with mild side effects, including erythema and itch in three and two patients, respectively. No severe adverse events or local reactions, including blistering, phototoxic or photoallergic reactions, were observed.
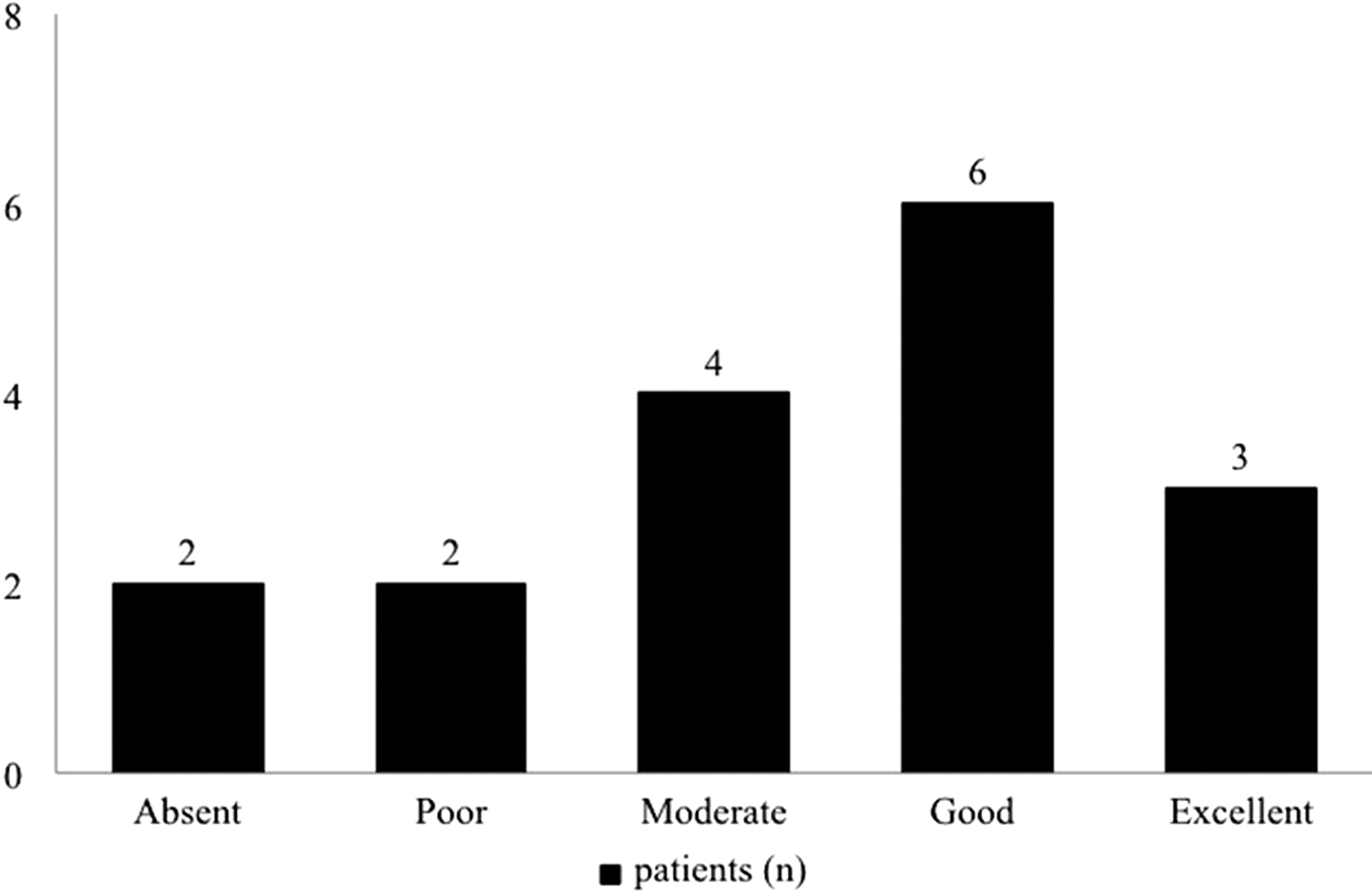
Number of patients showing poor, good, moderate, excellent, or no repigmentation after 8 weeks of UVA1 laser treatment. Nine out of 17 patients (52.94%), indicated in the panel as patients achieving good or excellent pigmentation, showed an improvement of vitiligo ≥50% from baseline.

Before
Discussion
Many therapeutic modalities have been used for the treatment of vitiligo. Among all the conventional therapies and the newly emerging techniques, UV irradiation in the range of either UVA or UVB remains to be the cornerstone of the therapeutic plan.
PUVA has been used for many decades in vitiligo involving a large body surface area, but psoralen is not always well tolerated. Furthermore the long-term carcinogenic risk remains a concern, because the treatment of vitiligo requires long-lasting therapeutic cycles ranging from several months to 1 year. Finally, a complete repigmentation has been experienced in <20% of patients. 11 Westerhof and Nieuweboer first reported NB-UVB efficacy in vitiligo in 1997. This wavelength demonstrated a remarkable effectiveness in improving pigmentation and a more favorable safety profile than PUVA. 12 Interestingly, lesions located on the hands or feet are less responsive to both PUVA and NB-UVB than those on other parts of the body. 11
Among other available phototherapy modalities, MEL has been suggested to be as effective as either NB-UVB or PUVA. Furthermore, the possibility of treating single vitiliginous patches sparing unaffected areas could permit rapid achievement of therapeutic dosages. 5 –7 Nevertheless, the successful use of MEL is limited to lesions with shorter duration and localized in peculiar anatomic sites including the face, neck, and knees.
UVA1 wavelengths penetrate the skin more deeply than UVB, reaching the deep dermis and even the subcutis. Thereby, they can effectively modulate the activity of immune and inflammatory cell populations. 13 In particular, they activate specific apoptotic pathways in T and B cells and immature proliferating mast cells through the production of superoxide anions and singlet oxygen species, which then cause damage to the mitochondrial membranes. 14 –16
Further, it has been demonstrated that UVA1 phototherapy can modulate proinflammatory cytokines including tumor necrosis factor (TNF)-α, interleukin (IL)-12, and interferon (IFN)-γ, and can reduce the expression of intercellular adhesion molecule type 1 (ICAM-1), thus interfering with lymphocyte activation and trafficking into tissues. 17,18 Finally, UVA1 stimulates the expression and activity of melanocytes, increasing melanin density and elongation and branching of melanocyte dendrites, clinically resulting in increased pigmentation or tanning. 19
Mutzhas et al. reported their experience with a UVA1 lamp in eight patients affected by vitiligo, but only one patient showed repigmentation. 20
El Zawahry et al. compared UVA1 with NB-UVB lamps in 40 patients treated three times weekly for 12 weeks. Patients receiving UVA1 wavelength were divided into two subgroups according to energy density, as patients receiving moderate (40–70 J/cm2) or low (≤20 J/cm2) doses of UVA1. Despite the fact that the safety profile was comparable between NB-UVB and UVA1 treated patients, NB-UVB was more effective than UVA1. Further, this experience suggests that clinical response to UVA1 is dose dependent. 21 This latter observation is of interest because fluorescent lamps produce only low to medium energy densities whereas high-output metal halide bulbs that release high-energy fluences are associated with high costs and time-limited fluorescence. Further, moderate and low dose UVA1 radiation requires long exposure times that could be experienced as uncomfortable by patients, and could present a suboptimal safety profile with hyperpigmentation, erythema, and pruritus as common side effects. Other reported adverse events comprise an increased risk of herpes simplex virus activation, induction of polymorphic light eruption, bullous pemphigoid, photoaging, and photocarcinogenesis. 22 –30
In this view, a monochromatic laser source emitting in the UVA1 range (355 nm) could achieve high energy density, lowering the exposition time, and thus achieve clinical results in a short time period (8 weeks in the present study) as well as decreasing the incidence of adverse events. It is of note that the laser is considerably less expensive than metal halide lamps, which also require constant maintenance to maintain high tube brightness.
Our report suggests that the UVA1 monochromatic laser ALBA 355 nm can represent a valid alternative therapeutic approach in the management of vitiligo. It rapidly achieves high doses selectively targeting the vitiligous lesions, thus permitting repigmentation in 88.23% of patients and minimizing exposure to excessive UV radiation on nonlesional skin thereby considerably decreasing the risk of severe burning or pathogenic exposure to UV. Repigmentation was faster and more complete on recent lesions and on facial skin, and slower on the acral sites, similarly to what occurs in traditional NB-UVB treatment. In our experience, similarly to those from plaque type psoriasis and palmoplantar pustular psoriasis, 9,10 side effects were mild, and included transient post-treatment erythema and itching. The treatment could also extend its potential to other immunomediated skin disorders such as atopic dermatitis.
The major limits of the present study were the absence of a comparison group (i.e., NB-UVB) and the small number of patients evaluated.
Side effects seem to be similar to the ones shown after traditional 311 nm UV phototherapy, although large scale comparative studies should be conducted in the future. The costs of the devices and the limited number of centers may represent another limitation.
Conclusions
In conclusion, our report suggests that UVA1 laser could represent an applicable treatment modality in patients affected by vitiligo, solving the problem caused by the limits of conventional UVA1 lamps, even though further data on larger numbers of patients are necessary.
Footnotes
Author Disclosure Statement
No competing financial interests exist.