
Abstract
Objective:
Our study aimed to detect whether 450 nm blue laser can be applied effectively and safely in endosocopic submucosal dissection (ESD) system for surgery in colonic tissue.
Background data:
Semiconductor blue laser has been applied in surgery due to its excellent cutting property, however, whether blue laser can be applied in colonic surgery has not been reported.
Materials and methods:
Porcine colon tissues were vaporized by 450 nm blue semiconductor laser at 10–25 W and at working distances from 0.5 to 3 mm, with a three-dimensional scanning system. Moreover, we designed an ESD model and applied blue laser at 10 W on porcine colonic tissues with this system. Dimensions of the vaporized tissues and coagulation zones were assessed under microscopy.
Results:
Since the thickness of colonic wall is no more than 1 mm, first we determined the cutting property and safety of blue laser on porcine colon tissue and found that blue laser at 10 W made lesions shallower than 1 mm and the depth of vaporization can be controlled effectively within muscularis mucosa and submucosa. Moreover, a large scale of porcine colonic tissue was vaporized precisely by blue laser at power of 10 W with the ESD system ex vivo.
Conclusions:
Our results indicate that 450 nm blue laser at 10 W can be well controlled for laser–tissue interaction with excellent cutting efficiency and less thermal damage in adjacent tissues especially side of the submucosa. Therefore, 450 nm semiconductor blue laser could be a safe alternative approach for colonic surgery.
Introduction
Nowadays, Endoscopic mucosal resection and endoscopic submucosal dissection (ESD) are the gold standard for treatment of early-stage gastrointestinal cancer. Recently, a variety of ablation modalities, including classical and fundamental ways of multipolar electrocautery probes, argon plasma coagulation, photodynamic therapy, and emerging technologies of radiofrequency ablation and cryotherapy, have been applied in gastrointestinal surgery. 1 On the contrary, several types of lasers have been applied to esophageal and gastrointestinal diseases, including carbon dioxide (CO2), Nd:YAG laser, KTP:YAG laser, neodymium–holmium laser, and diode lasers. 2,3 Several advantages of laser are presented when it is utilized for ablation of urethra, 4 bladder, 5 oral and periodontal 6 tissues, including precise tissue cutting ability, clean vision, noncontact incision, and good hemostatic properties. 6 Recently, novel blue lasers whose wavelengths were 450 and 445 nm have been introduced in stomatology, and the tissue incision and laser–tissue interaction were evaluated. 7,8 Comparing with traditional lasers applied to esophageal and gastrointestinal tissue, blue laser possesses vital superiorities of shorter wavelength and higher absorption coefficient in the target chromophores hemoglobin and melanin, and its optical penetration depths of human colon mucosa/submucosa are less deep. 9 In the previous studies, blue laser presented favorable vaporization and coagulation results and appeared to be an emerging surgical tool applied to the mucosal and submucosal lesions. 7,8 Since the thickness of human colonic wall is no more than 1 mm, 10 the low-power blue laser, which could be precisely controlled, vaporize tissue less deeply, and make good vessel coagulation, could be an excellent and safe tool for colonic surgery; however, whether blue laser can be applied in colonic surgery has not been reported.
In the present study, to evaluate the effect of blue laser on colon tissue surgery, we examined the cutting property of a new 450 nm semiconductor blue laser on porcine colon tissues in vitro to determine suitable parameters for blue laser application, and further tested the cutting property of 450 nm blue laser in a model of ESD. We found that this novel blue laser can be well controlled for laser–tissue interaction with excellent cutting efficiency and less thermal damage in adjacent tissues especially side of the submucosa.
Materials and Methods
Laser systems and experimental platform
A novel blue diode laser system was specially designed and made by Blueray Medical Ltd. (Xi'an, China) and the First Affiliated Hospital of Xi'an Jiaotong University (Xi'an, China). The laser consists of 36 blue laser diodes in TO56 package, each diode emits up to 1.6 W laser power with wavelength between 440 and 460 nm, centered at about 450 nm. The laser generates through a 2.5-m-long optical fiber with a core diameter of 760 μm. This output fiber with numeric aperture of 0.22, one end has a standard SMA905 connector to the laser and the other has a straight cut end producing 25-degree beam divergence, was used for all experiments in this study. The in vitro vaporization was operated on a three-dimensional custom-made x-y moving stage system. The system consists of two computer-controlled electrical step motors that can move stage in both x- and y-axes, and a fiber holder can manually adjust the distance from fiber tip to colon tissues.
Porcine colon model and measurement of in vitro vaporization
Sharing a similar physical structure with human colon, porcine colon tissues were selected as the in vitro experimental model. All experimental procedures have been approved by the Institutional Animal Care and Use Committee (IACUC-XJTU-17353). Five fresh porcine colon tissues were obtained from a local slaughterhouse, and all of them were kept in saline at 4°C to minimize dehydration and structural changes for 4 h. Each specimen was split and then unfolded on the tissue holder infiltrated with 20°C saline.
To evaluate the depth, width, coagulation, and carbonization of the vaporized colon tissue, several parameter settings were selected, including four different stage moving velocities (0.5, 1, 1.5, 2 mm/sec), four working distances (WD) from fiber tip to colon tissue (0.5, 1, 2, 3 mm), and four laser power outputs (10, 15, 20, 25 W). In each vaporization process, the laser fiber stepped forward 10 mm along the x-axis to vaporize a groove, and then, another groove was made in a similar way with a 5–6 mm distance. Each set was repeated at least two times to make the results more reliable.
Two methods were used to measure the depth and width of the grooves described previously. 11,12 Macroscopically, the depth and width were measured by a Vernier caliper under optical microscopy and by an imaging scope (Canon G12). Histologically, the specimens were fixed in 10% neutral buffered formalin for at least 24 h, then embedded in paraffin, sectioned into slices (two slices per specimen), stained with hematoxylin and eosin (H&E), and examined by imaging with optical microscopy.
The model of endoscope and ex vivo vaporization
To test whether 450 nm blue laser can be applied in colon endoscopic surgery, we designed a model of the ESD (Fig. 4). A custom-made transparent container (the length, width, and height were 40, 33, and 28 cm, respectively) with a volume of about 16 L is simulating the adult human abdominal cavity (Fig. 4), and there is a metal box on the container undersurface, whose length, width, and height were 15 × 8 × 0.9 cm, respectively. Holes on two sides of the lateral and the cover of the container were drilled, respectively, for instrument entrance. In the bottom of the container, a custom-made metal tissue holder was used to fix the colon tissue. The length of the colon tissue was about 15 cm, whose end was fastened by 4-0 suture. The colon tissue was full of 20°C saline and the transparent container was poured half. A 10Fr cystoscope (Olympus) was placed into the cavity of the colon. Appropriate WD was controlled at 1–2 mm, from the laser tip to the colonic mucosa, and the vaporizing process of the blue laser was done at 10 W. Soft tissue specimens were fixed in 10% neutral buffered formalin, routinely processed, and paraffin embedded for H&E staining and examined by imaging with light microscopy.
Statistical analyses
All statistical analyses were performed with SPSS 18.0 and GraphPad Prism 5.0 software. Results are presented as mean ± SD.
Results
A 450 nm blue laser has an excellent cutting and coagulation property on porcine colon tissues in vitro
First, we determined the cutting property and safety of blue laser on porcine colon tissue. As shown in Fig. 1, 450 nm blue laser at 10 W made lesions on porcine colon tissues at treatment speeds of 0.5–2.0 mm/sec and with different WD of 0.5–3.0 mm. Moreover, we detected the coagulation zones made by the laser treatment under microscopy (Fig. 2). As shown in Fig. 3, we measured the depth, width, and coagulation zone thicknesses of the different blue laser treatments. The blue laser created grooves apparently deepest with 0.5 mm WD. However, coagulation zone thicknesses were almost not different among the four groups (Figs. 2 and 3). Further, we found that blue laser with power at 15, 20, and 25 W can make lesions much deeper than that made by blue laser at 10 W (p < 0.05, Fig. 3); on the contrary, blue laser at 10 W made lesions shallower than 1 mm and the depth of vaporization can be controlled effectively within muscularis mucosa and submucosa of colon tissue. In addition, the thickness of thermal zone was about 0.4 ± 0.1 mm (n = 390) as measured under the microscope. These results indicate that 450 nm blue laser at 10 W has excellent cutting efficiency and less thermal damage in adjacent tissues especially at the side of submucosa on porcine colon tissues.
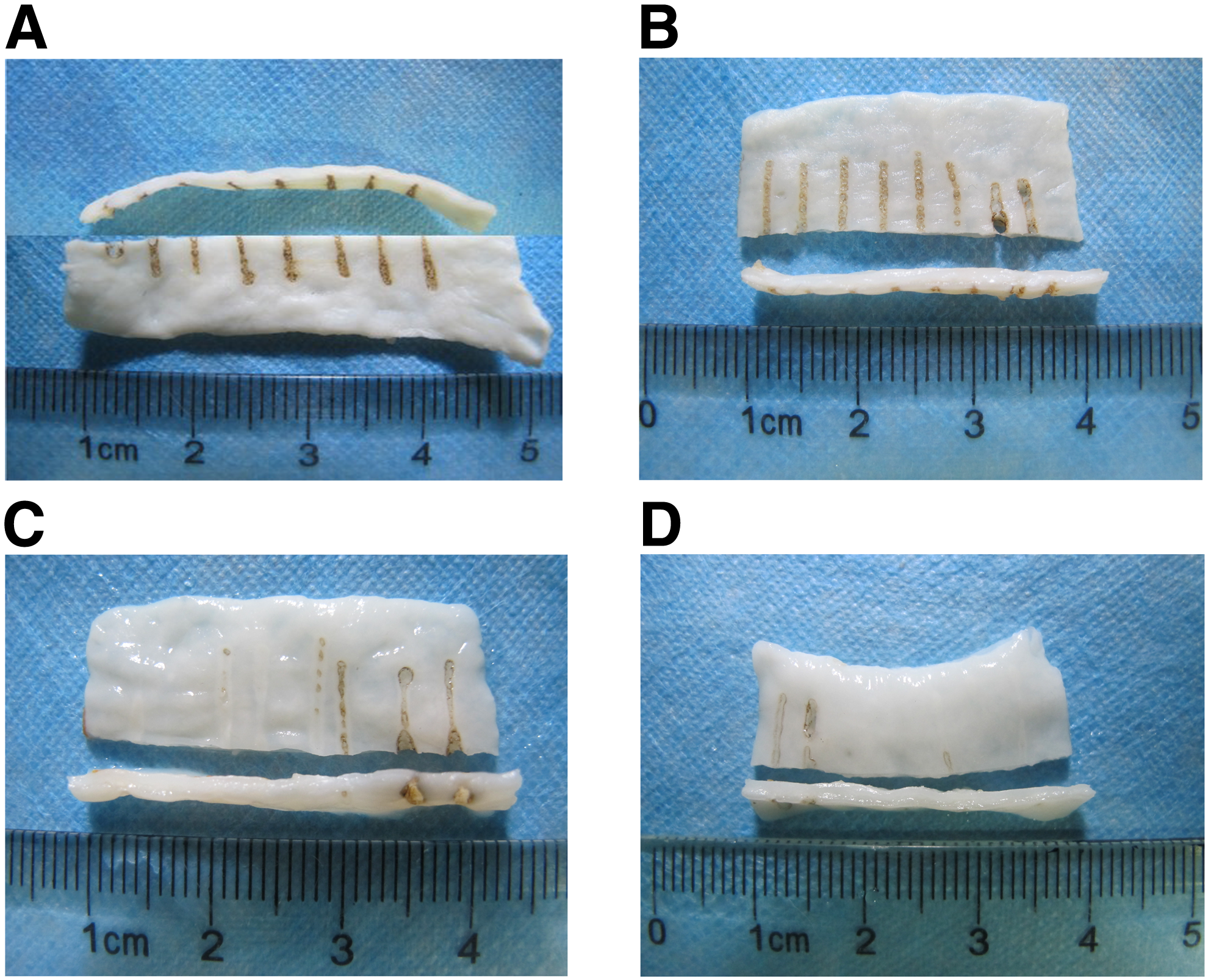
Images of the colonic tissue vaporization grooves at 0.5–3 mm WD [form the left side to the right
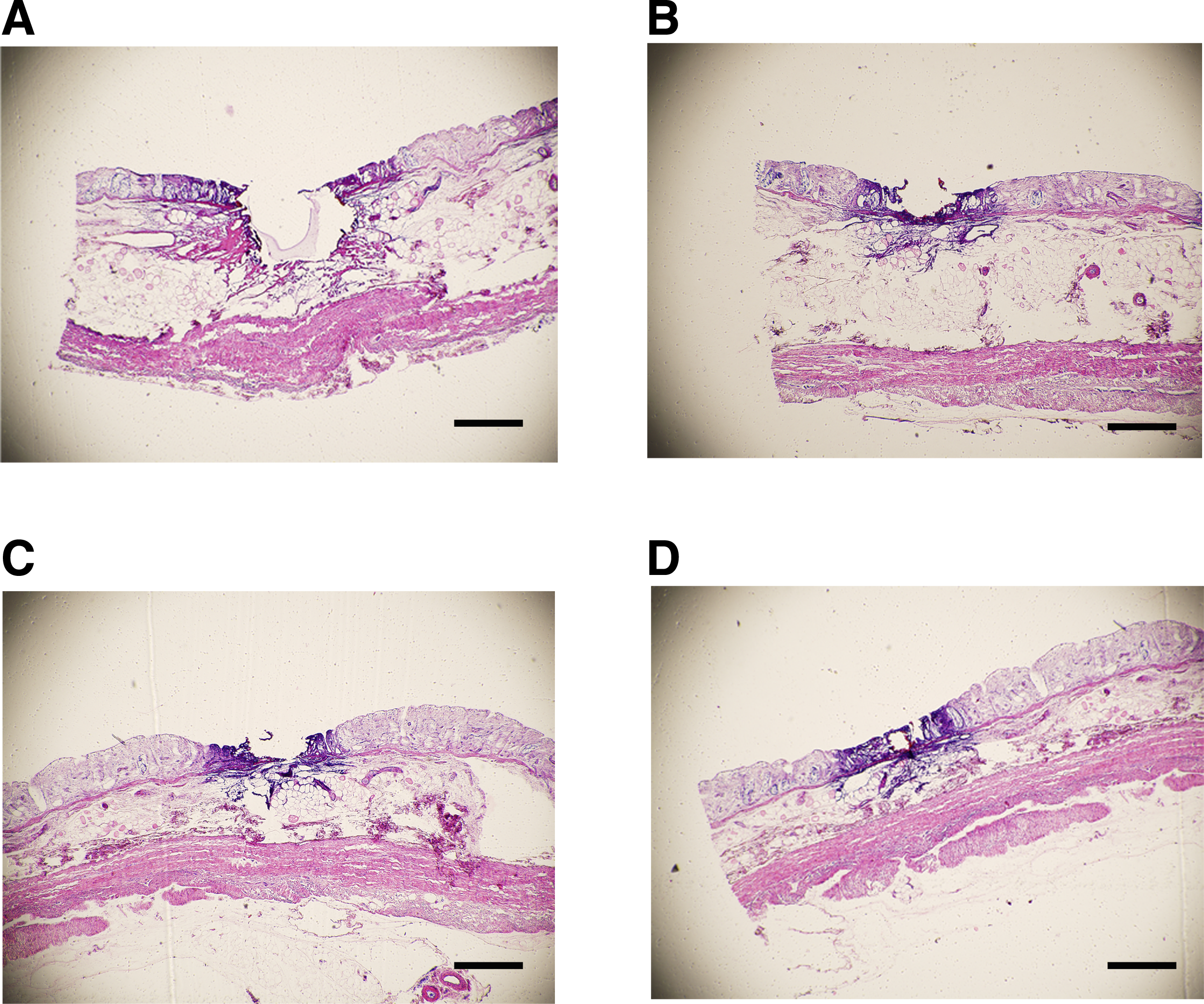
Histological images of the colonic tissue treated with blue laser at 10 W with 1 mm/sec treatment speed and 0.5–3 mm WD
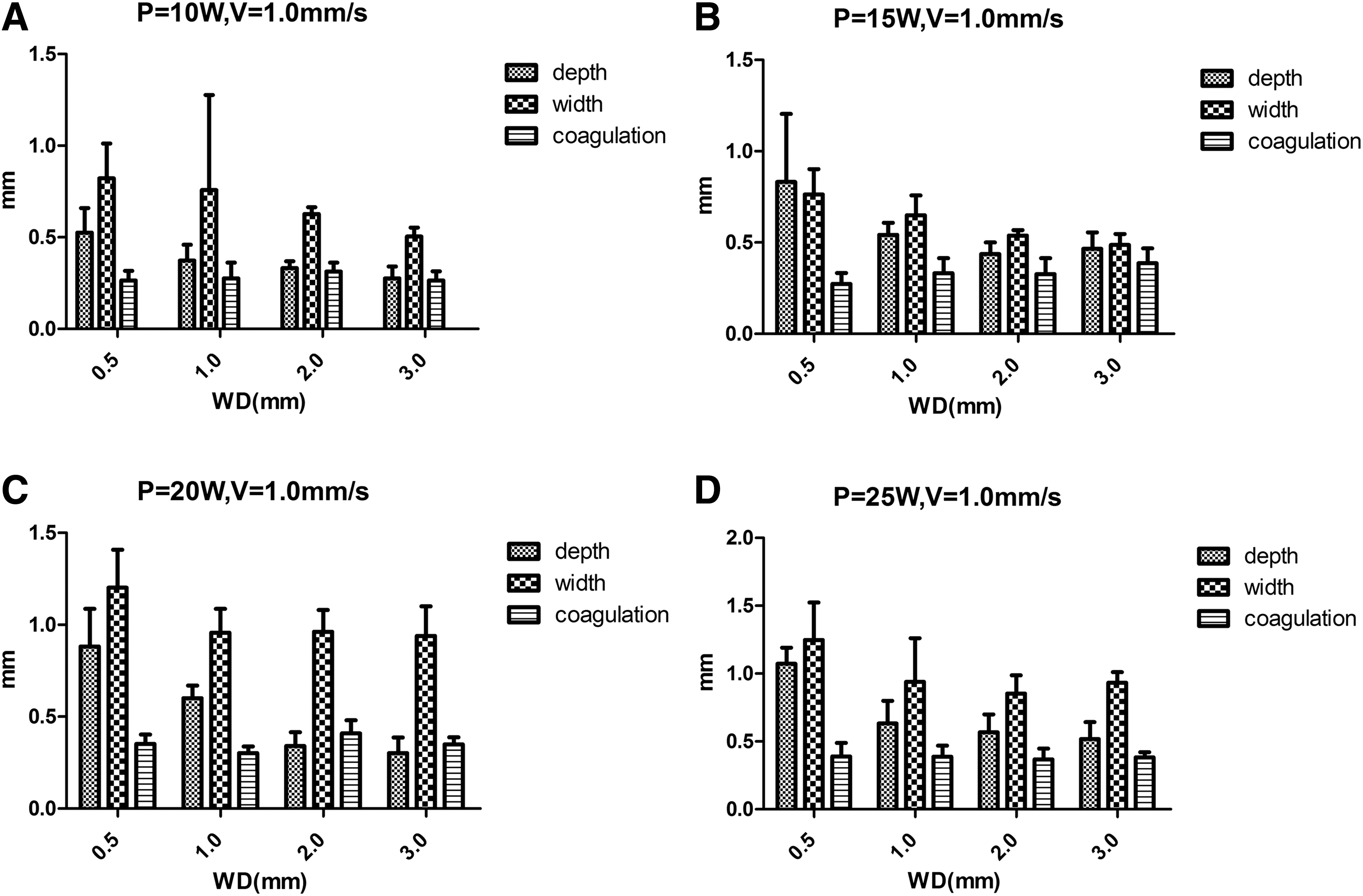
Depth, width, and coagulation measured after the blue laser vaporizing the colonic tissues at different powers. (
Colonic endoscopic mucosal and muscularis mucosal dissection ex vivo
To further test whether 450 nm blue laser at 10 W can be applied in colon endoscopic surgery, we designed a model of the ESD (Fig. 4), and all procedures of the operation were performed by the same experienced endoscopic physician. We used this system to cut porcine colon tissue in saline with blue laser at 10 W and found that large scales of colonic mucosa were also vaporized (Fig. 5). Dimensions of the vaporized tissue and resultant lesions were assessed and we found that in the model of endoscopic condition, the mean thickness of coagulation and carbonization zone of colon was 0.4 mm (n = 60) and 0.03 mm (n = 60), respectively (Fig. 6). These results indicate that 450 nm blue laser at 10 W could be applied in colon endoscopic surgery effectively and safely.
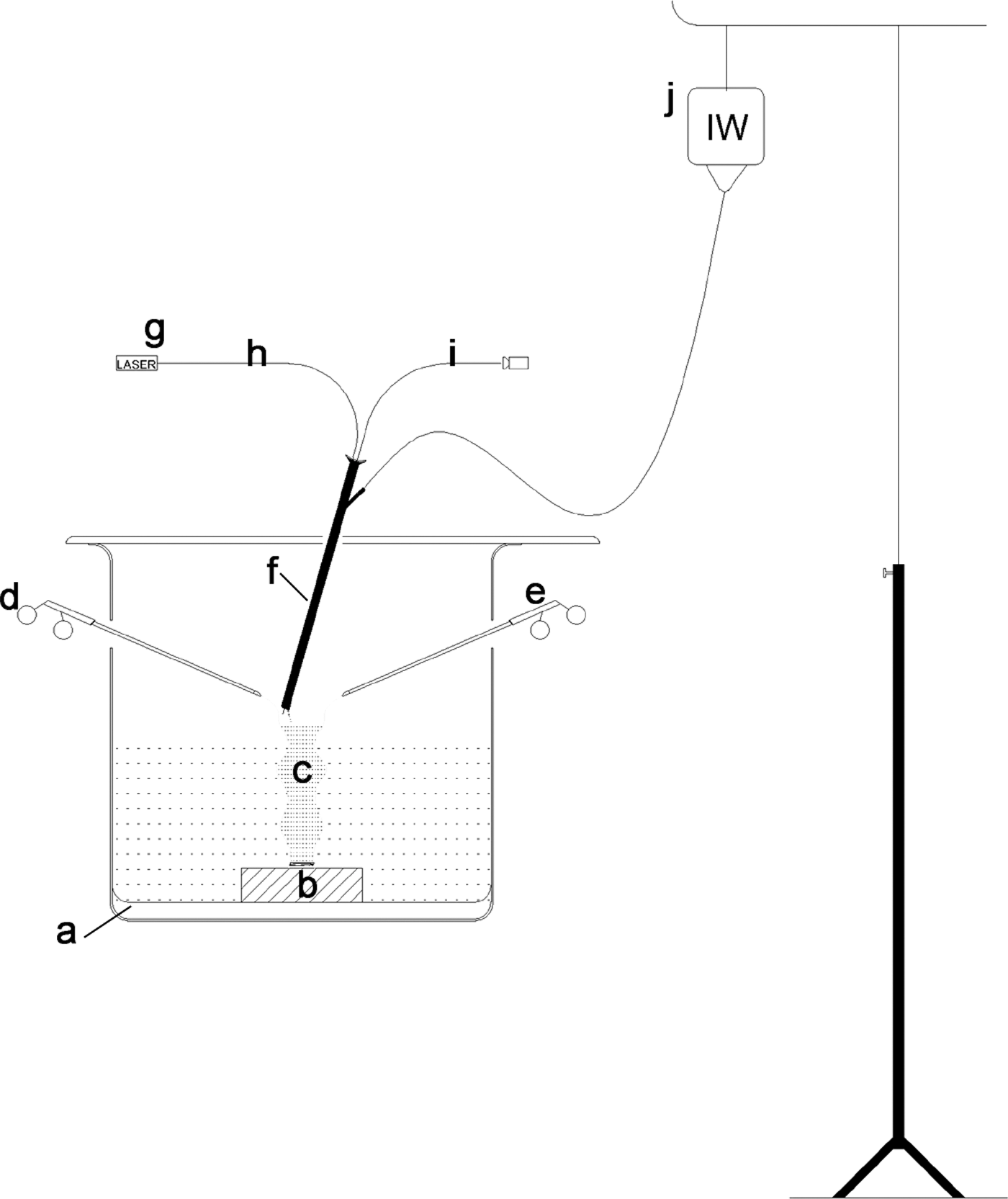
Schematic illustration of experimental setup, “a” indicates transparent plastic container; “b” indicates metal box; “c” indicates colon tissue filled with irrigation saline; “d” and “e” indicate instruments of laparoscopic forceps; “f” indicates 10Fr cystoscope; “g” and “h” indicate blue laser and optical quartz fiber, respectively; “i” indicates light source line; and “j” indicates irrigation saline water.
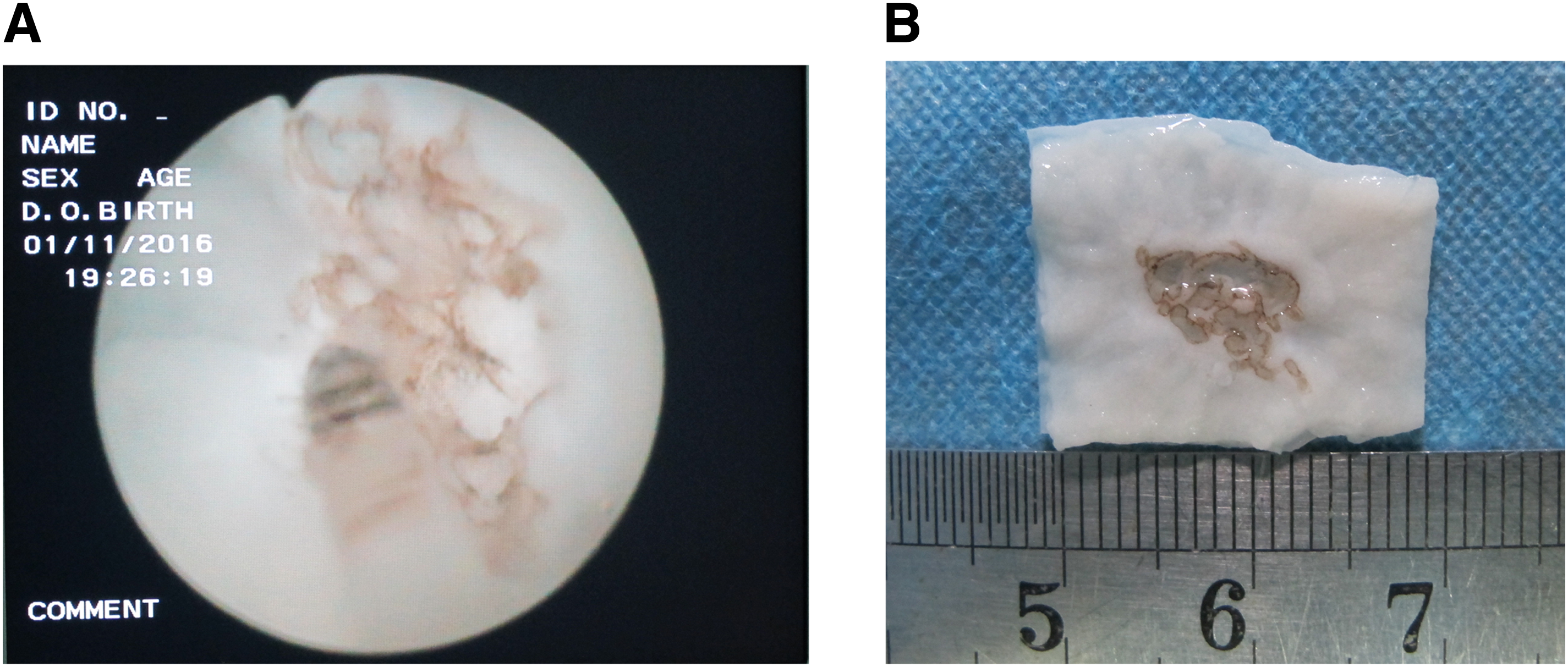
Images of
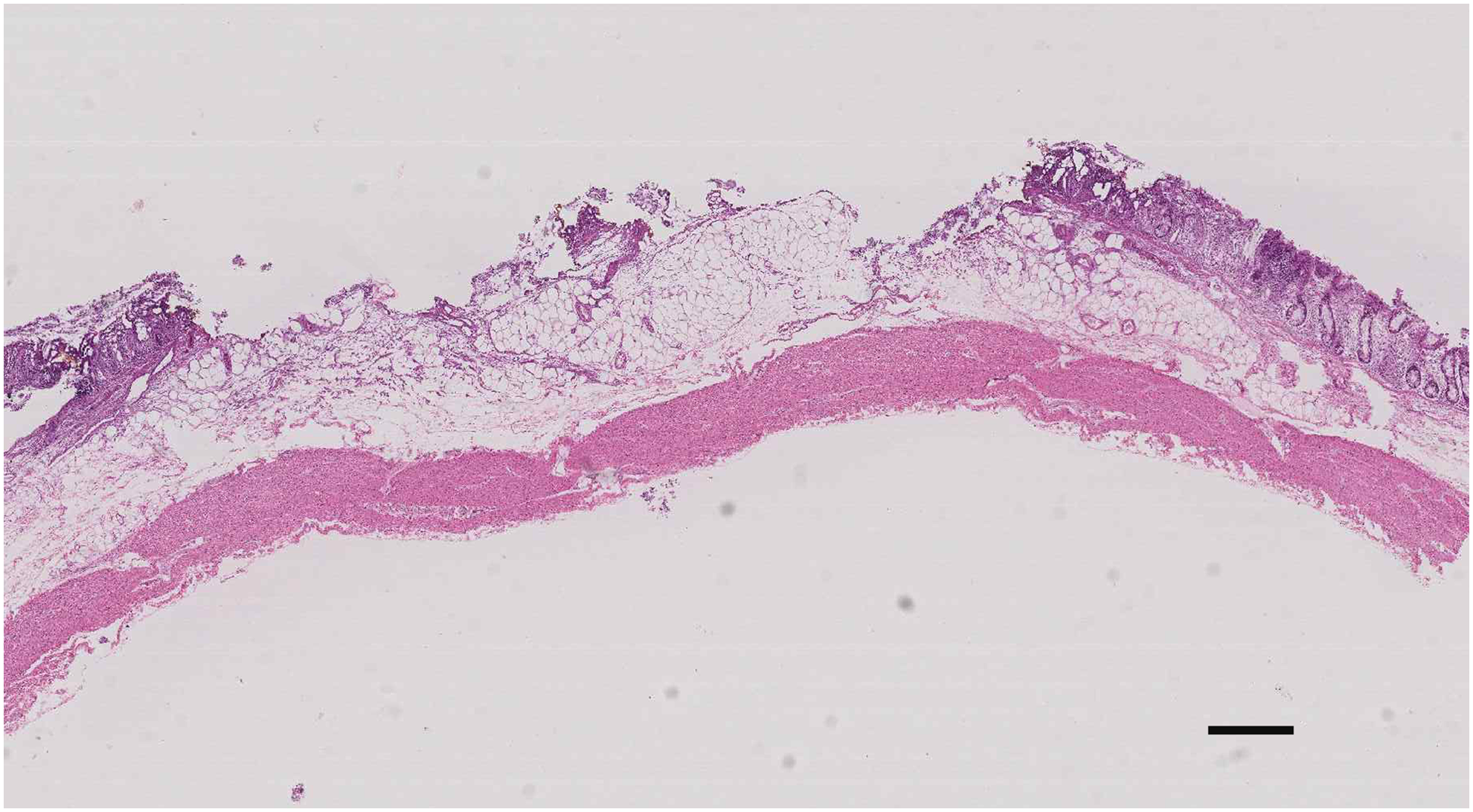
The vaporized colonic tissue treated with blue laser at 10 W and 2–3 mm WD. The original magnification is × 17. Scale bar: 300 μm.
Discussion
Various lasers with different wavelengths and optical power have been developed for surgical treatment of different diseases; however, whether blue laser can be applied in colonic surgery is still not clear. In the present study, we evaluated the effect of 450 nm blue laser on colonic surgery. Since the thickness of human colon wall is no more than 1 mm, first we determined the cutting property of blue laser on porcine colon tissue. We tested blue laser vaporization with different powers at a WD of 0.5–3 mm and a treatment speed of 0.5–2 mm/sec, and found that blue laser with power more than 10 W can make lesions deeper than 1 mm, on the contrary, blue laser at 10 W made lesions shallower than 1 mm and the depth of vaporization can be controlled effectively within muscularis mucosa and submucosa of colon tissue (Fig. 3). To further explore whether blue laser can be used in colonic surgery, we made a system to mimic the model of ESD, and all procedures of the operation were performed by the same experienced endoscopic physician. With the blue laser at power of 10 W, we found that a large scale of porcine colon tissue vaporized by blue laser can be controlled well. Our results indicate that the novel 450 nm semiconductor laser system can effectively vaporize the colon intermediate mucosa and muscularis mucosa and can be safely used for large-scale intermediate mucosal and submucosal dissection in the ex vivo ESD model.
Laser–tissue interaction is dependent on the kind of lasing medium, properties of target tissue, duration of irradiation, energy or power density, and the types of optical fiber. 13,14 Domankevitz et al. 15 assessed the hemostasis of holmium laser in vivo during incisions made in the skin, liver, and small intestine, and concluded that appropriate irradiation parameters could allow the holmium laser to create suitable tissue effects for general use in a surgical instrument. Moreover, laser incision depths and denaturation of soft tissue also depended on the WD, treatment speed, the ambient air, and saline solution. 12,16 In the present study, we evaluate the 450 nm blue laser–colon tissue interaction with different parameters, such as output power, WD, and treatment speed, and found that 450 nm blue laser at 10 W made excellent vaporization in the saline solution with nice coagulation and low thermal damage on colon tissue.
The blue diode laser obtained more attention since Shuji Nakamura et al. invented high-power and high-efficiency blue light-emitting diode (LED) and won the Nobel Prize of Physics in 2014. 17 Figurova et al. 18 combined the blue LED (λ = 470 nm, power densities at 0.008 W/cm 2 , total daily doses of 3.36 J/cm 2 ) with low-level laser therapy (λ = 685 nm) successfully improving the healing of sutured skin incisions in minipigs. LED blue laser has also been successfully utilized in the treatment of acne vulgaris 19 and enhanced bone regeneration in critical-sized defects. 20 Several reports about blue laser and tissue interaction were mainly focused on the oral tissue in vitro experiments and resection of benign oral lesions. Comparing with traditional infrared diode laser and quantic molecular resonance scalpel, LED blue laser demonstrated excellent cutting property 6 –8,21 in assessed laser–tissue interactions in monolayer cultures. In addition, except the high cutting property of the 450 nm blue laser, the novel blue LED laser system used in this study is compact and portable, another advantage of LED blue laser.
Researchers have successfully combined lasers with the ESD system to explore whether lasers can be applied in surgery. 3 Our study demonstrated that 450 nm blue laser vaporized the mucosa and submucosa of the colon tissue and it did not create obvious thermal damage in adjacent tissues. To further evaluate the feasibility of the novel 450 nm semiconductor blue laser in ESD, we will compare it with other lasers, such as green laser and holmium laser, and other methods for tissue dissection; moreover, tissue hemostasis and tissue healing process will be observed in an in vivo study.
Conclusions
Our results demonstrate that the semiconductor 450 nm blue laser can be well controlled for laser–tissue interaction on porcine colon tissue with excellent cutting efficiency and less thermal damage in adjacent tissues especially side of the submucosa. Due to its safety and efficacy in colonic surgery and the portable system design, the 10 W 450 nm semiconductor blue laser could be a safe alternative approach for colonic surgery.
Footnotes
Acknowledgments
This study was supported by a key research and development program of Shaanxi Province, China (S2017-ZDYF-ZDCXL-SF-0047 to D.H.).
Author Disclosure Statement
The authors have no potential conflicts of interest and financial support to disclose.