
Abstract
Objective:
To study the effects of carbon dioxide (CO2) lasers (λ = 10,600 nm) on remineralizing dental caries.
Methods:
This study involved performing a systematic search of English articles archived in the PubMed, Scopus, and Web of Science databases. The keywords used to identify the relevant articles were ((CO2 laser) OR (carbon dioxide laser)) AND ((dental caries) OR (tooth remineralization)). Publications before 2019 were selected. The titles and abstracts of the initially identified articles were screened. Duplicate records, reviews, and irrelevant studies were removed. Full texts were retrieved for publications that studied the effects of CO2 lasers on remineralizing dental caries.
Results:
The search identified 543 potentially relevant publications. A total of 285 duplicate records were removed. Sixteen articles were included in this review. Four studies reported that CO2 lasers inhibited bacterial growth. The growth of cariogenic bacteria, mainly Streptococcus mutans, on an irradiated tooth surface was slower compared with nonirradiated ones. Four studies investigated the reduction of the demineralization of enamel with cariogenic challenge. They found that CO2 lasers reduced the carbonate content of mineralized tissues and increased the microhardness of enamel. Nine studies used CO2 lasers associated with topical fluorides in remineralizing dental caries. The results of the synergistic effect of laser irradiation and fluoride application with regard to the inhibition of caries progression varied among these studies, whereas laser irradiation could enhance fluoride uptake to demineralized mineral tissues.
Conclusions:
CO2 laser irradiation increased acid resistance and facilitated the fluoride uptake of caries-like lesions. In addition, it reduced the growth of cariogenic bacteria.
Introduction
Dental caries, which was reported as the most prevalent oral condition in the Global Burden of Disease 2010 Study, remains a serious public health problem. 1 Approximately 3.9 billion people were affected by this oral condition, 1 which exerted a substantial influence on individuals or communities with regard to pain and suffering, systemic health, and quality of life. 2 Caries lesions were formed as a result of the dissolution of minerals from dental hard tissues, thus leaving a relatively porous tooth structure. Initial enamel caries lesions, constantly undergoing an everyday battle between progression and regression, 3 developed during irregular periods of demineralization and remineralization. The development of cavities takes 3–4 years. Thus, sufficient time exists to interrupt this process by using various preventive and restorative strategies. Noninvasive or minimally invasive management strategies that take into account the dynamic process of caries lesions are treatment choices that focus on the preservation of tooth structures as much as possible. 3 These strategies may effectively inhibit or even entirely reverse the caries process. Conventional noninvasive management for caries inhibition includes oral health promotion, dental plaque reduction/removal, and the use of fluoride tooth pastes or varnishes. Fluoride basically reduces the solubility of enamel and dentin and enhances the remineralization of tooth surfaces with early signs of mineral loss. 4 It has been suggested that caries progression may be remineralized when caries lesions are exposed to fluoride at levels of 0.095–0.190 ppm long term. 5 However, remineralization cannot be achieved with fluoride alone. The presence of calcium and phosphate ions is essential for remineralization to occur. When the salivary gland is not functioning properly, supplementing fluoride with calcium-based strategies, such as casein phosphopeptide amorphous calcium phosphate 6 and functionalized tricalcium phosphate, may greatly assist remineralization. Another novel noninvasive approach is the use of laser irradiation on enamel or dentin in inhibiting caries progression.
Maiman developed the world's first laser, a ruby laser, in 1960. 7 Four years later, in 1964, the first 10,600 nm carbon dioxide (CO2) gas laser was developed. 8 Nitrogen and helium gases were added to the CO2 laser tube to cool the laser gas, stabilize the electrical discharge process, increase pressure, and transfer energy to the laser gas. 9 Unlike neodymium-doped yttrium aluminum garnet (Nd:YAG) lasers (λ = 1064 nm) and argon lasers (λ = 488–514 nm), enamel and dentin heavily absorb CO2 lasers. CO2 lasers are usually centered at 9300, 9600, 10,300 and 10,600 nm. CO2 lasers emitting light at 9300 and 9600 nm have a higher absorption of hydroxyapatite than they do at 10,300 and 10,600 nm. However, a 10,600 nm CO2 laser has been commonly used in medicine and dentistry, and most of the commercially available CO2 lasers operate only at this wavelength. The effect of the irradiation of CO2 lasers in caries research has been studied since the 1960s. 10 A number of studies investigated the potential of laser irradiation on enamel or dentin in remineralizing caries progression. 11 –15 Studies reported that CO2 laser irradiation had an inhibitory effect on demineralized mineral tissues. Moreover, it has been suggested that the combination of laser irradiation and topical fluorides had promising effects in remineralizing dental caries. 16 –18 However, the effect of CO2 lasers on the caries remineralizing remains to be elucidated. A literature search in PubMed and Scopus found no comprehensive review evaluating studies investigating the effects of the actions of CO2 lasers in caries remineralizing. Therefore, the objective of this article was to review the evidence regarding the effects of CO2 lasers (λ = 10,600 nm) on remineralizing dental caries.
Methods
Search strategy
Two investigators (K.L. and I.S.Z.) performed a systematic search of the articles archived in three databases: PubMed, Scopus, and Web of Science databases. The following keywords were used to identify the relevant articles: ((CO2 laser) OR (carbon dioxide laser)) AND ((dental caries) OR (tooth remineralization)). The last search was performed on January 31, 2019. Publications before 2019 were chosen. A list of potentially eligible articles was developed, including publications searched using the keywords (Fig. 1).
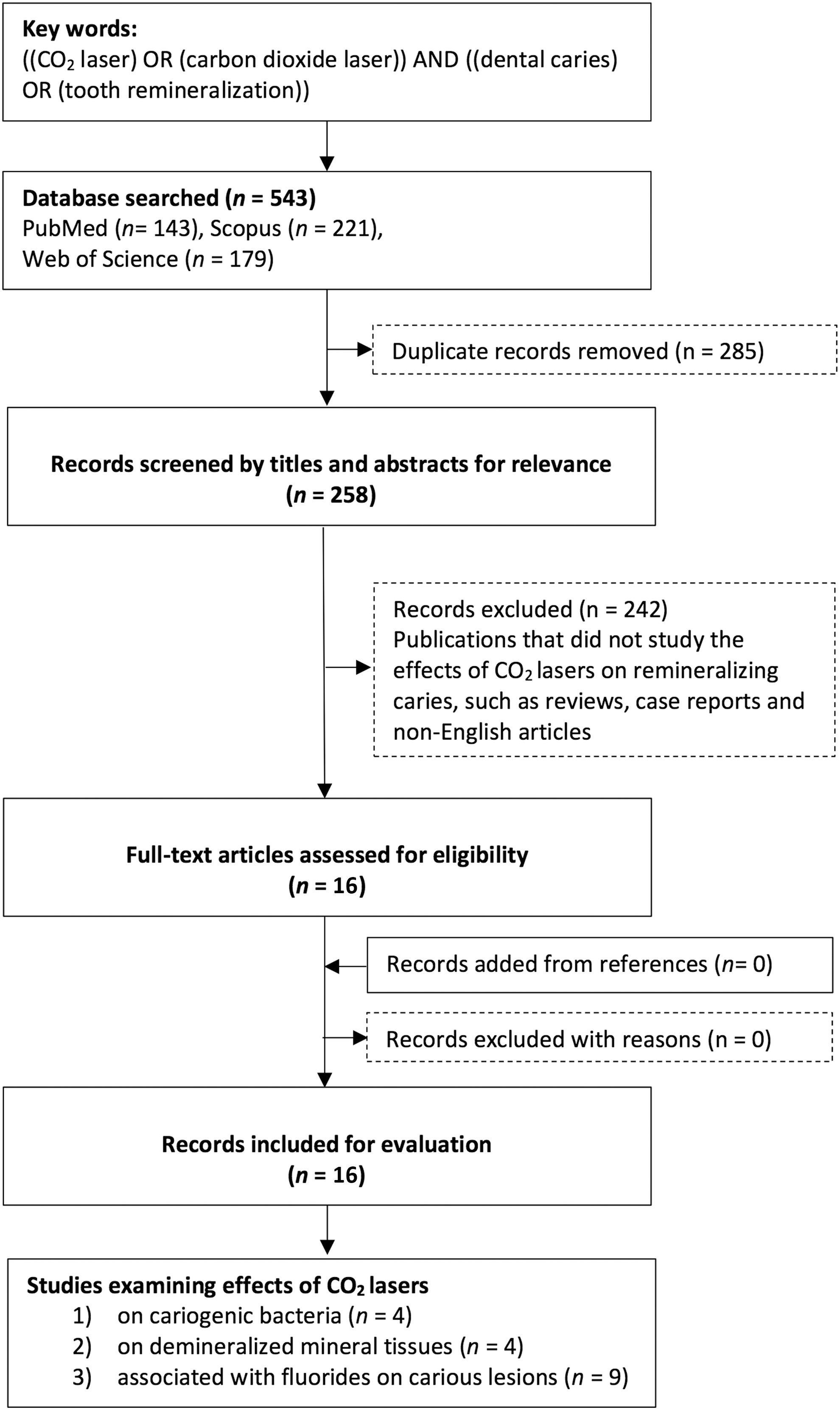
Flowchart of the literature search.
Study selection and data extraction
The records identified from the database search were checked for duplication. The titles and abstracts from the list of potentially eligible articles were screened after the duplicate publications were removed. Articles that did not study the effects of CO2 lasers on remineralizing dental caries were excluded after titles and abstracts were screened. The remaining articles were retrieved with full texts. The reference lists of all the included articles were screened to identify all possible eligible studies. The inclusion criterion for selecting studies for this review was as follows: studies investigated the effects of the actions of CO2 laser on remineralizing enamel and dentin caries, including its action on cariogenic bacteria and the combination effect with topical fluorides on caries progression. For the included articles, the following information was recorded: publication details (authors and years), methods, outcome assessments (various criteria for studying the remineralizing of caries: the reduction of carbonate content, lesion depth, microhardness, mineral loss, surface morphology, and bacterial counts), and the main findings. Two authors discussed any disagreements on study inclusion or data extraction with the third author (O.Y.Y.) until a consensus was reached.
Results
The initial literature search identified 543 potentially relevant articles (143 articles in PubMed, 221 articles in Scopus, and 179 articles in Web of Science). A total of 285 duplicate records were removed (Fig. 1). After the titles and abstracts were screened, 242 articles that were classified as literature reviews, case reports, non-English articles, or other irrelevant studies were excluded. No additional relevant publications were found from the references of the selected articles. Finally, 16 articles were found to meet the inclusion criterion and were included in this review. Among these articles, four studies examined the action of CO2 lasers on cariogenic bacteria (Table 1), four studies investigated the effect of CO2 lasers on demineralized mineral tissues (Table 2), and nine studies investigated the effect of CO2 lasers combined with topical fluorides on caries-like lesions (Table 3).
Summary of Studies on Effects of CO2 (10,600 nm) Lasers on Cariogenic Bacteria
CFU, colony-forming unit; CLSM, confocal laser scanning microscopy; CO2, carbon dioxide; FESEM, field emission scanning electron microscopy; PCR, polymerase chain reaction; SEM, scanning electron microscopy.
Summary of Studies on Effects of CO2 (10,600 nm) Lasers on Demineralized Mineral Tissues
EDS, energy-dispersive X-ray spectroscopy; FTIR, Fourier transform infrared spectroscopy; FTRS, Fourier transform Raman spectroscopy; MHT, microhardness testing.
Summary of Studies on Effects of CO2 (10,600 nm) Lasers Combined with Fluorides on Caries Lesions
AAS, atomic absorption spectrometry; APF, acidulated phosphate fluoride; NaF, sodium fluoride; nFHA, nano-fluorohydroxyapatite; nHA, nano-hydroxyapatite; PLM, polarized light microscopy.
Actions of CO2 lasers on cariogenic bacteria
Four studies of the included articles studied the actions of 10,600 nm CO2 lasers on cariogenic bacteria. 12,16 –21 The effects of CO2 laser irradiation on bacterial viability, biofilm architecture, and the gene expression of Streptococcus mutans were investigated in these studies. Confocal laser scanning microscopy showed that dead and live bacteria were found in the marginal area of the irradiated spot and that no visible bacteria were left in the center of the irradiation area. 12 The total number of bacteria (live and dead) was less in the irradiated enamel than in the nonirradiated areas, and the number of live bacteria was larger than that of the dead ones, which were concentrated in the middle layers of the biofilm in all samples. 12 Irradiated enamel had a higher dead/live ratio in the top and deep layers compared with the nonirradiated sample. 12 A colony-forming unit confirmed less growth of bacteria in the irradiated group compared with the control group. 20 Another study 21 reported that little lethal effect (<10%) was shown when S. mutans biofilm samples were irradiated at a fluence of 31 J/cm2 compared with nonirradiated ones, whereas more lethal effects were presented when samples were exposed to fluences of 70 (23% killing effect) and 144 J/cm2 (30% killing effect). Scanning electron microscopy (SEM) image analysis revealed a clear thermal effect of CO2 laser irradiation on S. mutans biofilm, and a crater pattern in the biofilm was created, resulting in biofilm removal with a melted enamel surface in the irradiated spot. 12 Assessments using quantitative real-time polymerase chain reaction demonstrated that no significant difference in the gene expression (gtfB and gbpB) of S. mutans was found between laser-irradiated samples and nonirradiated ones. 20 However, another study 21 using DNA microarray analysis reported that 46 genes in the laser-irradiated samples showed changes in the gene expression at sublethal energies (31 J/cm2), and most of these genes were related to transport proteins and energy metabolism. Fifteen of these genes were upregulated, whereas 31 were downregulated. 21
Actions of CO2 lasers on demineralized mineral tissues
Four studies investigated the effects of 10,600 nm CO2 lasers on the chemical and morphological changes of demineralized enamel, as well as on the inhibition of caries—for example, lesion progression. With respect to chemical changes, Fourier transform Raman spectroscopy showed a statistically significant reduction of carbonate content in irradiated enamel compared with nonirradiated and sound enamel. 11 This was consistent with the findings of another study that reported an ∼40% loss of carbonate in the irradiated enamel using Fourier transform infrared spectroscopy. 12 Energy-dispersive X-ray spectrometry analysis showed an increase in the calcium-to-phosphorus ratio (Ca/P) in the laser-irradiated enamel covered by biofilm compared with nonirradiated samples. 12 Observations from SEM showed that no evidence indicated melting, fusion, or other morphological changes in CO2 laser-treated enamel in comparison with non-treated enamel, 11 whereas SEM photomicrographs of laser-irradiated enamel surfaces revealed the typical appearance of melting, cracks, and craters with discontinuities in another study. 14 In addition, an increase in surface microhardness was found in laser-treated enamel compared with the negative control, 13,14 which demonstrated that CO2 laser irradiation inhibited the progression of caries-like lesions.
Actions of CO2 lasers combined with topical fluorides on demineralized enamel and dentin
Eight studies investigated the combined effects of 10,600 nm CO2 laser irradiation and the application of topical fluorides on demineralized enamel, whereas the results of these studies varied. Five studies found a synergistic effect between laser irradiation and fluoride application in inhibiting enamel demineralization, 16 –18,22,23 whereas three other studies found that the combination of laser and fluoride had no additional impact on the inhibition of caries lesion progression in comparison with laser alone. 24 –26 Demineralized enamel samples treated with CO2 laser irradiation in conjunction with the application of amine fluoride showed less calcium dissolution and reduced surface alterations compared with those treated with laser only. 16 Additionally, laser irradiation through topical fluorides significantly enhanced fluoride or calcium fluoride uptake to the enamel surface layer when compared with laser alone. 16,26 Enamel surfaces treated with laser combined with fluoride showed a significantly higher microhardness than that with fluoride or laser only. However, it was also reported that a similar melting appearance was found in enamel surfaces treated with laser associated with or without fluoride, 14 and no synergistic effect was found for the inhibition of caries lesion progression. 26 One study investigated the combined effects of 10,600 nm CO2 laser irradiation and the application of topical fluorides on demineralized root dentin. The results showed that both main factors had significant effects on the increase of microhardness, but no additive benefit was found by combining these two strategies against the progression of root caries. 15
Discussion
PubMed, Scopus, and Web of Science are the three common research databases for dental research. Thus, they were used in this review for publication retrieval. PubMed is free for the public to access. Most of the journal articles it includes are on the field of medicine and biomedical science and were published after 1950. 27 PubMed provides multiple versions of the literature from early versions before the final versions were published. Scopus belongs to Elsevier, and Web of Science belongs to Clarivate Analytics. They are commercial companies that require access fees to use resources from the two databases. Most fields of science are covered in the two databases. They are complements to each other because both are not inclusive. 28 Scopus includes articles published since 1966. Web of Science is the oldest comprehensive scientific citation indexing database covering publications that can date back to 1900. 27 With the use of these three common databases, the results of the search were comprehensive. The results of the retrieval provided useful information on the effects of CO2 lasers on remineralizing dental caries.
This review focused on the CO2 laser of 10,600 nm in wavelength, which was the first and commonly used CO2 laser in dentistry. Most commercially available CO2 laser devices use this wavelength. The CO2 laser of 10,600 nm has an absorption coefficient in hydroxyapatite that is 10 times lower than that of 9600 nm. 29 This allows for deeper penetration and higher fluence by a 10,600 nm CO2 laser to cause the desired thermal effects on caries inhibition compared with CO2 lasers at other wavelengths. 29 CO2 lasers with short-pulse durations and high peak power are available with the advancement of technology. The new generation of CO2 laser machines produces less collateral thermal damage. They are more versatile in dental clinical applications. 29
The results of this review showed three effects of CO2 laser on dental caries. The first one is the inhibition of the growth of biofilm. Dental biofilms consist of bacteria, a matrix of polysaccharides and other organic materials. They strongly adhere to tooth surfaces. Using chemical agents to remove biofilm is ineffective because they generally cannot penetrate deeply into biofilm. 21 The penetration of laser into biofilm makes it a possible alternative for disrupting or removing dental biofilms. Laser irradiation can affect the gene expression in bacteria. The mechanisms involve the direct absorption of laser by DNA or light-mediated photosensitizer with oxygen, causing DNA damage. 30 In addition, the photothermal effect of CO2 laser can indirectly induce changes in gene expression.
The reduction in bacteria viability by CO2 lasers was described as dose dependent. 21 Although a laser at low fluence with a short period of irradiation time had no significant effect on the viability of bacteria, the laser changed their gene expression, resulting in the immobilization of S. mutans in biofilm. 21 A CO2 laser at high fluence revealed lethal effects on S. mutans. 21 The low divergence of the wavelength, scattering, and backscattering of photons within the spot size area focused the energy and allowed deep penetration into the biofilm. 21 However, such exposure might cause thermal damage to dental hard tissue and pulp. The biofilm could be removed using a laser of high power and high-energy density, but a melted surface and morphological changes were observed on the enamel surface in another study. 12 The effects of laser on biofilm varied depending on laser parameters and irradiation methods. The mechanism included the prevention of the initiation of biofilm formation, 20 the alteration of gene expression and the immobilization of S. mutans in the biofilm, 21 killing the bacteria, 12,20,21 and morphological change with melting, fusion, and cracklines on the enamel surface, which affected bacteria adhesion. 12,20
Zancopé et al. first reported that a CO2 laser caused morphological changes on the enamel surface, such as fusion and melting. 20 Carbonate in the hydroxyapatite structure is unstable and is acid soluble, 31,32 CO2 laser irradiation on demineralized human enamel removed the carbonate. 11 This increased the microhardness without morphological changes on the surface. 13 However, CO2 laser irradiation could also cause melting and cracking on the enamel surface in the process of removing carbonate. 12 The cracking on enamel was undesirable because it might facilitate caries development along the cracklines. 33,34
The combination of laser irradiation and fluoride therapy has received much attention for the reduction of dental caries progression. The critical pH for the dissolution of enamel dropped in the presence of fluoride in the irradiated surface. 35 From this literature review, the interaction of various fluoride agents with a laser influenced the outcome of the caries inhibition. Although no synergistic effect on caries progression inhibition was found using acidulated phosphate fluoride on enamel in three studies, 17,25,26 differences were found on enamel surface characteristics with the continuous and pulse modes of CO2 lasers. Morphological changes in melting, recrystallization, and cracks were observed. No difference was found in enamel calcium loss between fluoride with the continuous mode of a CO2 laser, the laser alone, and fluoride alone. 25 However, the pulse mode of the CO2 laser after fluoride application improved the surface microhardness of enamel and calcium fluoride uptake, whereas no morphological changes were reported. 17,26 Different concentrations and acidity of sodium fluoride combined with pulsed laser irradiation showed no synergistic effects. 18,24 Enamel with the topical application of sodium fluoride showed higher microhardness when compared with laser irradiation alone. 18,24 Recently, enamel treated with laser with nano-fluorohydroxyapatite had higher microhardness compared with nano-fluorohydroxyapatite alone. 22
Conclusions
This review found that a CO2 laser (10,600 nm) could remineralize dental caries. Current evidence suggests that a CO2 laser could increase the acid resistance of caries lesions, inhibit the growth of cariogenic bacteria, and enhance fluoride uptake to demineralized mineral tissues.
Footnotes
Acknowledgments
The authors' institution supported this review. This study was supported by the Natural Science Foundation of Shenzhen University (2019129).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Natural Science Foundation of Shenzhen University (860-000002110146).