
Abstract
Objective:
The aim of this study was to evaluate color longevity after different bleaching techniques.
Background:
Laser-activated bleaching methods are gaining popularity due to decreased chair time and increased patient compliance. However, the longevity of such methods has not been stated clearly.
Methods:
Sixty patients were divided into the following three groups (n = 20); group 1: chemical bleaching with 35% hydrogen peroxide (HP) gel, group 2: bleaching with 35% HP gel with diode laser activation, and group 3: bleaching with 35% HP gel with Er,Cr:YSGG laser activation. Color changes (ΔE*) were calculated by using two different formulas: (i) CIELAB (ΔEab) and (ii) CIEDE2000 (ΔE00) with a spectrophotometer before treatment, 24 h after treatment 3, 6, and 12 months after treatment. Evaluation of postoperative sensitivity was performed before and immediately after treatment, followed by re-evaluation 24 h and 1 week after treatment.
Results:
For ΔEab calculation, no significant difference was observed during both intra- and inter-group evaluations (p > 0.05). For ΔE00 calculation, no significant intergroup difference was observed (p > 0.05), whereas significant intragroup differences between the values of after treatment, 6–12 months. In the chemical bleaching group, increased postoperative sensitivity was observed after 24 h (p < 0.001). In the diode-laser-activated group, postoperative hypersensitivity was detected at 24 h and 1 week. No significant hypersensitivity was observed in the Er,Cr:YSGG-laser-activated group (p > 0.05).
Conclusions:
All three techniques provided efficient bleaching. Chemical and diode-activated bleaching methods resulted in slight sensitivity after application, whereas Er,Cr:YSGG-laser-activated bleaching did not cause sensitivity.
Introduction
Tooth whitening treatment has become widely used in daily clinical practice, but results vary based on the degree of tooth discoloration, tooth age, the concentration of the bleaching agent, and the time and frequency of treatment. There are two types of whitening treatment procedures, at-home and in-office. Both methods utilize hydrogen peroxide (HP) or carbamide peroxide for the purpose of whitening. 1
HP is widely used for in-office bleaching and is commercially available in different concentrations ranging from 15% to 40%. It can be further activated by light or heat for increased efficiency, and the duration of application may differ between 10 and 60 min depending on the concentration. 2,3 There are various assumptions on HP's mechanism of action; however, it is widely accepted that free radicals produced by HP penetrate the pores of the enamel and enter the dentin, where it can oxidize organic stains. 4 Light sources have been used to accelerate the bleaching action by catalyzing the oxidation–reduction reaction and thus increasing the amount of released hydroxyl (OH−) radicals. 5
There are different types of light sources used during the whitening process, such plasma arc lamps, quartz–tungsten–halogen lamps, and light-emitting diodes. Further, various laser devices with different wavelengths (e.g., carbon dioxide, Er:YAG, Er,Cr:YSGG, and diode) have also been used for increased efficiency and reduced chair time for the patient. 2,6,7 The diode laser, which has a 980 nm wavelength, is absorbed by water more than other wavelengths. 8 Although the use of a diode laser during the whitening process increases whitening efficiency, there are concerns about the laser's effect on the enamel. 9 However, because the diode laser is barely absorbed by hydroxyapatite, leading to minimal transmission and scattering of the laser's light, the anticipation of laser-induced enamel surface changes seems unreasonable. 10 Another laser used for bleaching treatment is the erbium, chromium: yttrium–scandium–gallium–garnet (Er,Cr:YSGG) 2780 nm wavelength laser, which is effective for the treatment of dental hard tissues. 7 However, its applicability for use during the whitening process has not been adequately investigated. Dionysopoulos et al. 11 found that the Er,Cr:YSGG-laser-activated bleaching process did not significantly change the mineral content or surface morphology of enamel compared with the conventional chemical whitening procedure. However, it is not known if these changes have clinical significance because they are reversible. 12
Tooth sensitivity during and after bleaching is a common complication related with the occurrence of microscopic superficial defects and pores, which allow the bleaching agent's rapid entry toward the pulp. 6 Further, tooth sensitivity that occurs immediately after bleaching is generally related to a high concentration of peroxide combined with a light source, which increases the temperature in the tooth and causes hypersensitivity. 13 The aim of this randomized clinical trial was to compare the effectiveness, color stability, and postoperative sensitivity after no light, diode-activated, or Er,Cr:YSGG-laser-activated bleaching procedures with HP gel.
Materials and Methods
This study was conducted at Gaziantep University, faculty of dentistry, in the department of restorative dentistry and was approved by the Ethical Committee of Gaziantep University (2018/141). Informed consent was obtained from the subjects who agreed to return for follow-up evaluation.
Patients
For sample size calculation, a significance level of 5% (α = 0.05) was considered at (1-β) 0.80 by using G*Power 3.1.9 software. Based on this power analysis, color change values between two formulas represented value of 2.8 ± 2.5. Thus, minimum sample size in each group was determined as 14. Assuming any discontinuing patient during follow-up, six dropout subjects was added to each group.
Sixty male and female patients between 18 and 60 years of age were selected and randomly assigned to three groups according to the bleaching procedure. The inclusion criteria were as follows: (1) all teeth were present, (2) the teeth were color shade A3 or darker, and (3) the teeth were free of any restorations and/or caries. The exclusion criteria were as follows: (1) smoking, (2) a history of allergy to HP and/or adverse reactions to previous bleaching procedures, (3) pregnancy or breastfeeding, (4) tooth hypersensitivity, and (5) tetracycline-stained teeth.
Because two to three patients from each group did not return for follow-up, only 45 subjects were included in the final analysis to equalize the groups (n = 15). HP bleaching gel (Whiteness HP Blue Calcium; FGM, Joinville, Brazil) was used according to the manufacturer's instructions. Within each group, the bleaching procedure was repeated on five teeth in four different quadrants.
Study design
Group 1: chemical bleaching only
First, soft tissues were protected with a light-cured gingival barrier (Top Dam; FGM Prod. Odontol. Ltda., Joinville, Brazil). Then, the 35% HP gel was prepared by mixing the content of two different syringes according to the manufacturer's instructions. Then, the gel was applied uniformly over the buccal surface of the teeth at a thickness of 2 mm. The gel was kept on the surface of the teeth for two sessions of 20 min each.
Group 2: diode-laser-activated bleaching
All steps for group 2 were the same for group 1 except that the 35% HP gel was activated with a 980 nm diode laser (Gigaa Dental Laser Cheese, Wuhan, China) using a special bleaching handpiece (5.85 cm2 spot size) at an output power of 7 W for 12 sec at a distance of 5 mm from the surface of the tooth (energy density = 14.3 J/cm2, power density = 1.19 W/cm2). After irradiation procedure, the gel was kept on the teeth surfaces for 15 min. The laser irradiation cycle was repeated twice per bleaching application for each quadrant (total energy/session = 28.6 J/cm2).
Group 3: Er,Cr:YSGG-laser-activated bleaching
All steps for group 3 were the same as for group 1 except that a Er,Cr:YSGG laser (2780 nm; Waterlase MD Turbo; Biolase, Irvine, CA) was used to activate the HP gel. A special tip (800 μm diameter) was attached to the handpiece (Z-type glass tip, MZ8) and used at a distance of 2.5 cm from the tooth surface. The selected laser settings were an average power of 1.25 W, a pulse repetition rate of 10 Hz, and a pulse duration of 700 μs while water and air were off (energy density = 21.6 J/cm2, power density = 250 W/cm2). Laser irradiation was performed 2 × 10 sec per tooth. (total energy/session = 43.2 J/cm2). The total bleaching procedure lasted for 20 min.
All information of the laser system included is summarized in Table 1.
Parameters of Laser Irradiation
Color measurement
The change in color of the upper and lower incisors and canines was measured by touching the tip of a spectrophotometer (VITA Easy Shade Advance, Zahnfabrik H. Rauter, Bad Säckingen, Germany) on the middle third of the buccal surface at five time intervals: before the procedure, 24 h after the procedure, and 3, 6, and 12 months after the procedure. The digital spectrophotometer was calibrated in accordance with the manufacturer's guidelines before each use. The baseline color values were L*, a*, and b*, in which (1) L* represents brightness, the value or degree of lightness ranging from 0 (black) to 100 (white); and (2) a* and b* represent the shade, where a* represents the degree of red/green (+a: red, −a: green) and b* is the measurement along the yellow–blue axis (+b: yellow, −b: blue).
Total color differences were calculated using the following equation in previous studies. 13,14
However, recent color measurement studies 15,16 reported that in the assessment of acceptability and perceptibility thresholds for dental materials, CIEDE2000 color difference formula displayed better fit than the CIELAB formula in the evaluation of visual tolerances, supporting its use in dentistry. 15 Therefore, color changes were also calculated by using the CIEDE2000 (ΔE00) color difference formula 17 :
KL, KC, and KH are the terms for the experimental conditions. For this study, the parametric factors of the CIEDE2000 color difference formula were set to 1.0. CIEDE2000 (ΔE00) and the discoloration were evaluated on the basis of perceptibility and clinical acceptability thresholds. For this study, the perceptibility threshold was set to ΔE00 = 1.30 U and the clinical acceptability threshold was set to ΔE00 = 2.25 U. 15
Evaluation of tooth sensitivity
Participants were asked to record their tooth sensitivity using a visual analogue scale (VAS) scored within a range of 10 points. The range of sensitivity scores were as follows: 0–1, no pain; 2–3, mild pain; 4–6, moderate pain; 7–8, severe pain; 9–10, intolerable pain. VAS values were recorded before the bleaching treatment, immediately after bleaching, and 24 h and 1 week after bleaching treatment.
Statistical analysis
The normality of the data was analyzed using the Shapiro–Wilk test before statistical analysis. A two-way repeated analysis of variance was used to compare normally distributed data for intergroup. The Kruskal–Wallis and Pairwise tests were used to compare non-normal data between groups. The paired t-test with Bonferroni was used for dependent measurements with normal distributed variables. A value of p ≤ 0.05 was considered statistically significant.
Results
Color analysis
L*, a*, b* values at each time interval are presented in Table 2. For group 1, the L* color change measurements at 24 h (L2*), 3 months (L3*), and 6 months (L4*) were significantly different from baseline (L1*; p < 0.05), whereas at 1 year, the L5* value was not significantly different (p > 0.05). However, for groups 2 and 3, all L* values (L2*, L3*, L4*, and L5*) were significantly different from baseline (L1*; p < 0.05). For all groups, the b* values were significantly different from baseline (b1*) at 24 h (b2*), 3 months (b3*), 6 months (b4*), and 1 year (b5*; p < 0.001). None of the b* values rather than baseline (b1*) were significantly different from each other (p > 0.05). Similarly, for all groups, the a* values were significantly different from baseline (a1*) at 24 h (a2*), 3 months (a3*), 6 months (a4*), and 1 year (a5*; p < 0.05). The a* values rather than baseline (a1*) were not significantly different from each other (p > 0.05).
Color Evaluation Values For L*, a*, b*
Different superscripts in the same column represent statistically different groups. 1: baseline, 2: 24 h after bleaching, 3: 3 months after bleaching, 4: 6 months after bleaching, 5: 1 year after bleaching.
For CIELAB formula, the ΔEab values at each time interval are presented in Table 3 and Fig. 1. All the tested bleaching systems resulted in statistically significant color changes compared with baseline (p < 0.05). Among the groups, the color change (ΔEab) at each time point after bleaching (24 h, ΔEab1; 3 months, ΔEab2; 6 months, ΔEab3; 1 year ΔEab4) was similar (p > 0.05). Within each group, the color change (ΔEab) at each time point after bleaching was also similar (p > 0.05).
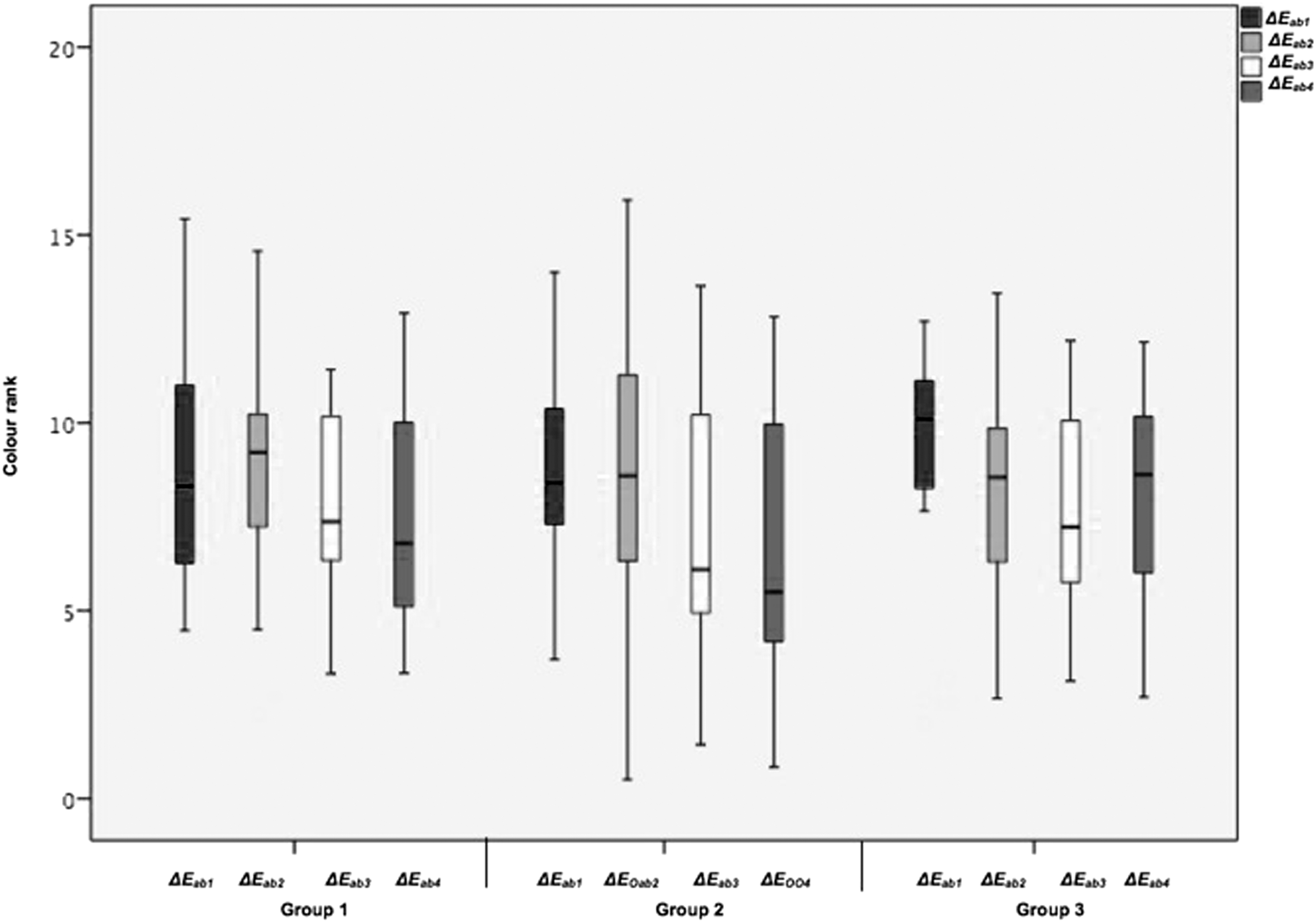
Color ranking in the different groups at each evaluation time for ΔEab .
Comparison of ΔEAB ± Standard Deviation Values for All Groups
Different lowercase superscript letters represent time-dependent intragroup differences (column). Different uppercase superscript letters represent intergroup differences (linear).
SD, standard deviation.
The ΔE00 values for CIEDE2000 formula at each time interval are presented in Table 4 and Fig. 2. Different from CIELAB calculation, ΔE001 values (24 h) were significantly different from ΔE002, ΔE003, ΔE004 (3, 6 months, and 1 year respectively; p < 0.05) for groups 1 and 3. In addition, ΔE002, ΔE004 were also significantly different for group 1 (p < 0.05). For group 2 only ΔE003, ΔE004 were also different from each other (p < 0.05).
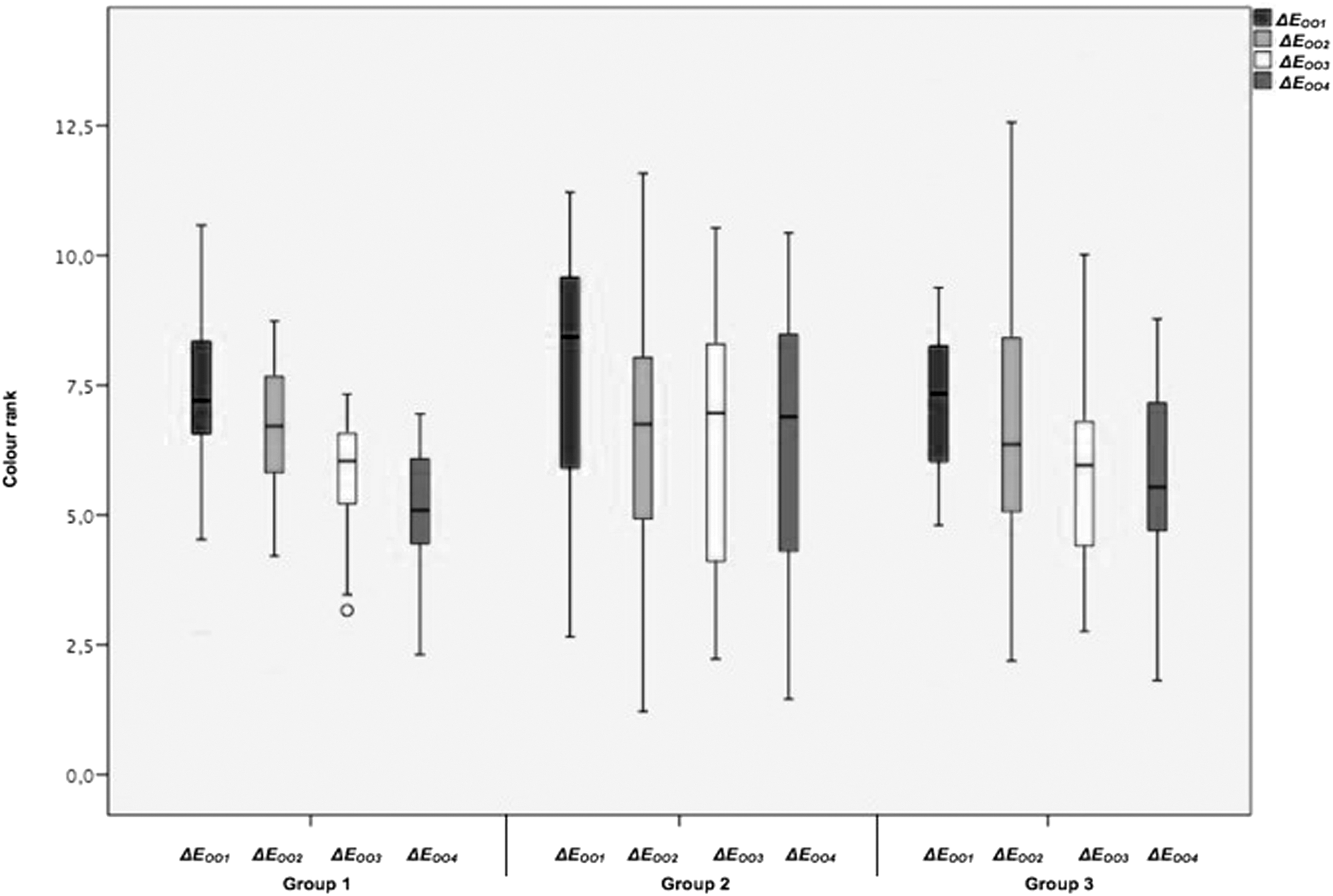
Color ranking in the different groups at each evaluation time for ΔE00 .
Comparison of Δe00 ± Standard Deviation Values for All Groups
Different lowercase superscript letters represent time-dependent intragroup differences (column). Different uppercase superscript letters represent intergroup differences (linear).
Dental sensitivity analysis
The clinical VAS scores are shown in Table 5 and Fig. 3. In the time-dependent comparison, groups 2 and 3 were significantly more sensitive at 24 h (p < 0.05), whereas all other measurements were similar to baseline (p > 1.000). For the intragroup evaluation, the initial and 24-h measurements of group 1 (p < 0.001) and the initial, 24-h, and 1-week measurements of group 2 were significantly more sensitive (p < 0.001), whereas all other measurements were similar.
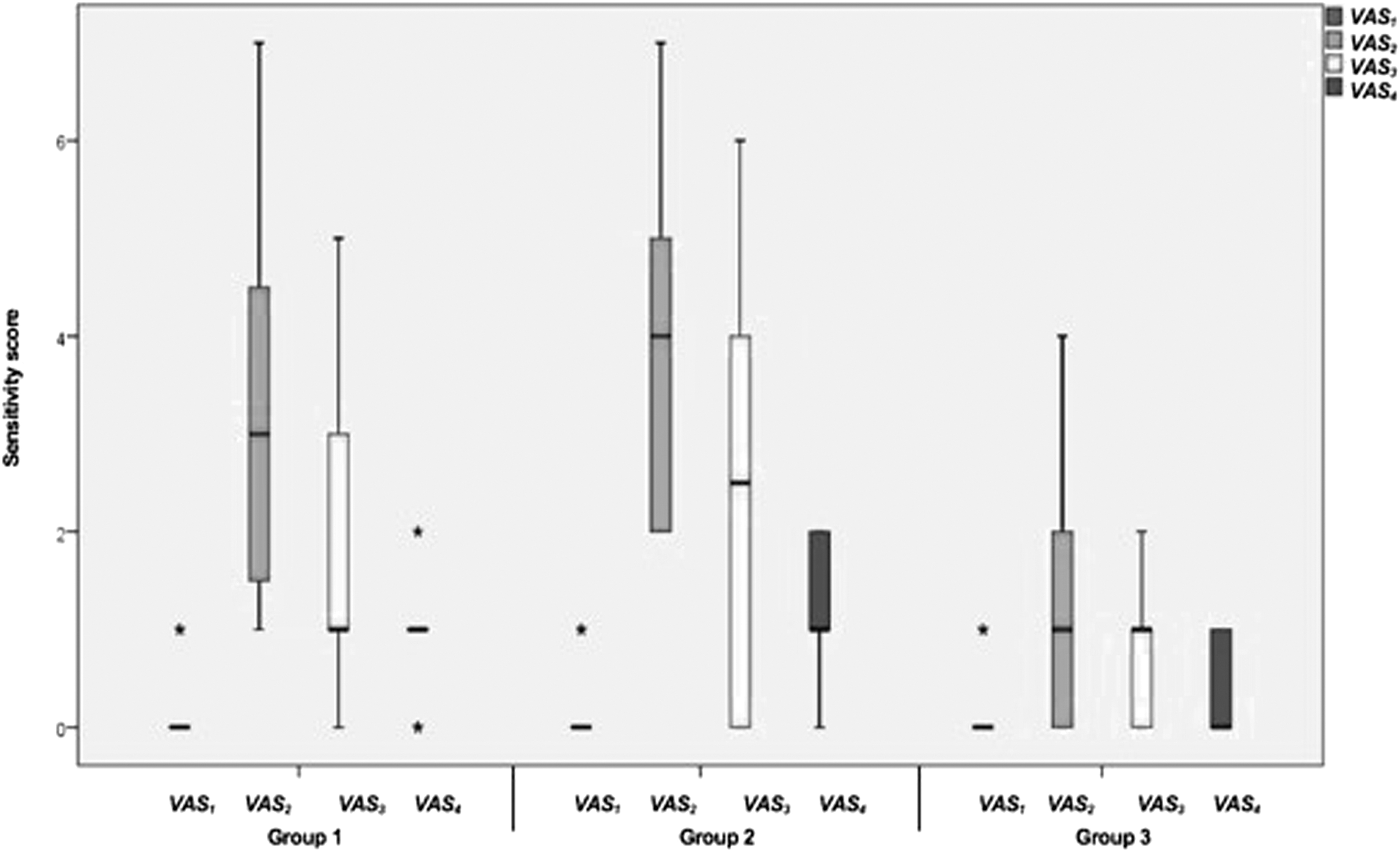
Sensitivity scores in the different groups at each evaluation time. VAS, visual analogue scale.
Sensitivity Evaluation Values
Different lowercase superscript letters represent time-dependent intragroup differences (column). Different uppercase superscript letters represent intergroup differences (linear).
Discussion
With the increased interest and demand for bleaching treatments, different bleaching agents have been introduced to the market, and these agents can be used with different techniques to increase the effectiveness of treatment. However, there are still questions about the side effects and long-term success of the different types of bleaching treatment systems.
In this study, we compared the long-term efficacy of three bleaching treatments and the associated tooth sensitivity after the procedures. The ΔEab values did not show any significant differences between groups at any of the follow-up times. However, ΔE00 values represented significant reduction by time, which means considerable color regression. Further, the degree of regression in chemical bleaching group was slightly higher than laser-assisted groups. Although the difference is not significant, laser assistance seems slightly advantageous. In addition, in the chemical bleaching group, we saw increased sensitivity at 24 h, and in the diode-laser-activated group, hypersensitivity was detected at 24 h and 1 week. In the Er,Cr:YSGG-laser-activated group, no significant hypersensitivity was observed.
Light sources are used to accelerate the chemical reaction that occurs during the bleaching process. 18 Previous studies have determined that activation methods increase the efficiency of HP and shorten the time required for bleaching. 19 –21 On the contrary, in some studies, it has been shown that activation methods accelerate the reaction but do not affect the bleaching activity. 22 –24 In this study, two different wavelength lasers were used to accelerate the bleaching. The wavelength and the mechanism of action of the lasers are greatly influenced by the power of the transmitted radiation, and the mode of operation is an important parameter for its efficiency. 25 The aid of laser activation for tooth whitening treatments is related to the transformation of laser energy into heat thus, when selecting a laser wavelength to increase bleaching, it is important to pay attention to its degree of absorption and the conversion of laser energy into heat. 26 Absorption of laser light in the gel decreases the amount of light passing through the enamel and reaching the dental pulp. 27
For the diode laser, many different wavelengths are available. However, the 980 nm diode laser is the only one approved by the Food and Drug Administration for dental bleaching due to its superior absorption by water. 28 In a previous study, Polydorou et al. 4 found that the 980 nm diode laser did not increase the efficacy of bleaching. This is in accordance with the findings of this study, which found similar results after chemical and diode-laser-activated methods in terms of color change.
The Er,Cr:YSGG laser (a pulsed laser) is capable of generating high-power outputs in a short duration, which allows for fast cooling. This is an advantage compared with continuously irradiating lasers with similar energy output. 29 The Er,Cr:YSGG laser shows an affinity to hydroxyapatite and water more than other laser systems. 7 This feature provides added safety because the heat that generates on the outer surface of the tooth is not transmitted into the deeper layers of the tooth structure. 25 Er,Cr:YSGG lasers have recently started to be used for bleaching treatment; however, only one study by Dionysopoulos et al. 3 has compared Er,Cr:YSGG-laser-activated bleaching with conventional bleaching and found it to be more effective.
Spectrophotometers have previously been used for evaluating color changes before and after bleaching treatments. Stephen et al. 30 stated that a spectrophotometer provides an appropriate spectral curve by determining accurate L*, a*, and b* axes, which are used to determine precise color values. The b* value is the most important parameter for detecting color changes after bleaching treatment, followed by L* and a*. L* values increase after bleaching treatment, whereas a * and b * values are expected to decrease. A part of previous studies have used the CIELAB and/or CIEDE2000 color difference formulas. 31,32 These previous studies stated that CIEDE2000 formula identifies color changes more precise compared with CIELAB. 16,33 Igiel et al. stated that CIEDE2000 formula represents the human perception of color differences with a consistency degree of 95% with visual findings, whereas CIELAB formula does 75%. 34 Nevertheless, there are a few studies on color changes after dental bleaching using this CIEDE2000 formula. 35,36 These limited studies evaluated the color changes of restorative materials. There is only one follow-up clinical study evaluating the whitening of dental hard tissues by using CIEDE2000. 32 Thus, it can be stated that CIEDE2000 formula is more suitable for the evaluation of bleaching materials and techniques compared with commonly used CIELAB system.
Because these changes are reversible, we followed our patients for a 1-year period. 37 Results on the longevity of tooth whitening are controversial; however, an exact comparison is not possible due to the use of different color measurement methodologies. 38,39 In an in vitro study performed by Lima et al. 40 it was found that color change achieved after HP bleaching regressed 1 month after treatment. Matis et al. 41 found a mean color change reversal of 51–65% 6 weeks postbleaching. Another study revealed that color regression was not significant until 6 months after treatment. 29 Our 1-year follow-up results were similar to those by Marson et al. 42 and Wiegand et al. 43 who also reported regression of teeth bleaching at 12 months after treatment.
Tooth sensitivity is the most frequent adverse effect of bleaching in 8–66% of patients, resulting in moderate pain, particularly after the initial bleaching application. 44 The severity of hypersensitivity may change according to the type of technique and material used. 45 Protecting the pulp from increased temperatures from light sources is important because laser-activated bleaching with high-power lasers may enhance intrapulpal heat. 46 Although the exact mechanism of hypersensitivity after bleaching is not understood, it presumably results from HP penetration into the dental pulp. 47 The oxygen bubbles that penetrate dentinal tubules during HP application may lead to movements of dentinal fluid, which in turn agitates the peripheral nerve endings. 40 Another hypothesis correlates hypersensitivity with free oxygen radicals passing through the enamel and dentin, and subsequently causing damage to the pulp. 6 Further, HP is capable of etching enamel as a result of protons (H+) release and thus exposing micropores. 1 This may explain why chemical and diode-laser-activated methods resulted in increased sensitivity in this study. However, the Er,Cr:YSGG laser group showed no increases in sensitivity, presumably due to the laser's limited superficial action as mentioned earlier.
This study had several limitations, including ensuring the return of the subjects for follow-up, oral hygiene and dietary habits of the participants, and including only one type of bleaching gel. Variables such as smoking, drinking coffee, and poor oral hygiene may limit the effectiveness of the bleaching methods. 48 Further, the type and composition of the bleaching agent may affect the degree of laser light absorption, which in turn may influence the degree of both color change and sensitivity. 49
Conclusions
Within the limitations of this study, it can be concluded that all laser systems represented the same degree of color changes as chemical bleaching at all time intervals and no significant regression was detected at any recall visit. In addition, the Er,Cr:YSGG laser provided the same degree of whitening as both the chemical and diode-laser-activated bleaching, but for a lesser duration. The use of lasers to induce the bleaching reaction does not provide better aesthetic or long-term color stability. Further, the chemical and diode-laser-activated bleaching resulted in increased sensitivity after 1 day after the procedure, whereas the Er,Cr:YSGG laser seems safer in terms of post-treatment sensitivity.
Footnotes
Acknowledgments
The authors thank Associate Professor Uğur Aydin.
Ethical Approval
This clinical trial was approved by local ethics committee of the University of Gaziantep (2018/141) and all participants were given information about the research, and oral and written informed consent was obtained from all participants. All procedures performed in this study were in accordance with the Helsinki declaration.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was self-funded by the authors.