
Abstract
The numerous dermatology clinics have decreased or stopped phototherapy sessions due to the increased risk of getting COVID-19 during the current pandemic. In this context, poorly ventilated phototherapy units (PUs) should be redesigned in order to continue UV-based therapies and to protect our patients from getting COVID-19. Recently, it has been reported that ultraviolet C (UVC)-related dose and virus concentration may play a decisive role in the virucidal activity. Considering air changes per hour and viral inactivation time, 30 min of 30-W UVC radiation is able to inactivate poorly ventilated PUs of 3–4 m length, 5.5–7 m width, and 2.7–3 m height. Upper-air UVC radiation for 30 min between sessions would allow us to have more treatment options for numerous dermatological diseases in novel PUs during the COVID-19 pandemic and possible future pandemics.
To the Editor:
The numerous dermatology clinics have decreased or stopped phototherapy sessions due to the increased risk of getting COVID-19 during the current pandemic. In this context, poorly ventilated phototherapy units (PUs) can be redesigned to continue UV-based therapies and to protect our patients from getting COVID-19. Ultraviolet C (UVC) radiation at a wavelength of 254 nm that has the peak absorption of uracil is strongly absorbed by RNA and DNA, hence, UVC radiation has the most effective germicidal properties. Although UVA and UVB can make a small contribution to the inactivation of bacteria, there are no effects of both radiations to inactivate viruses and, in particular, SARS-CoV2. 1 It is noteworthy that a few recent studies first reported that UVC-related dose and virus concentration may play a decisive role in the virucidal activity. 2,3 In addition, it is stated that a very small dose of <4 mJ/cm2 was adequate to attain complete inactivation of the virus. Even at the highest viral input concentration [1000 multiplicity of infection (MOI)], viral replication was completely inactivated at a dose >16.9 mJ/cm2. 2
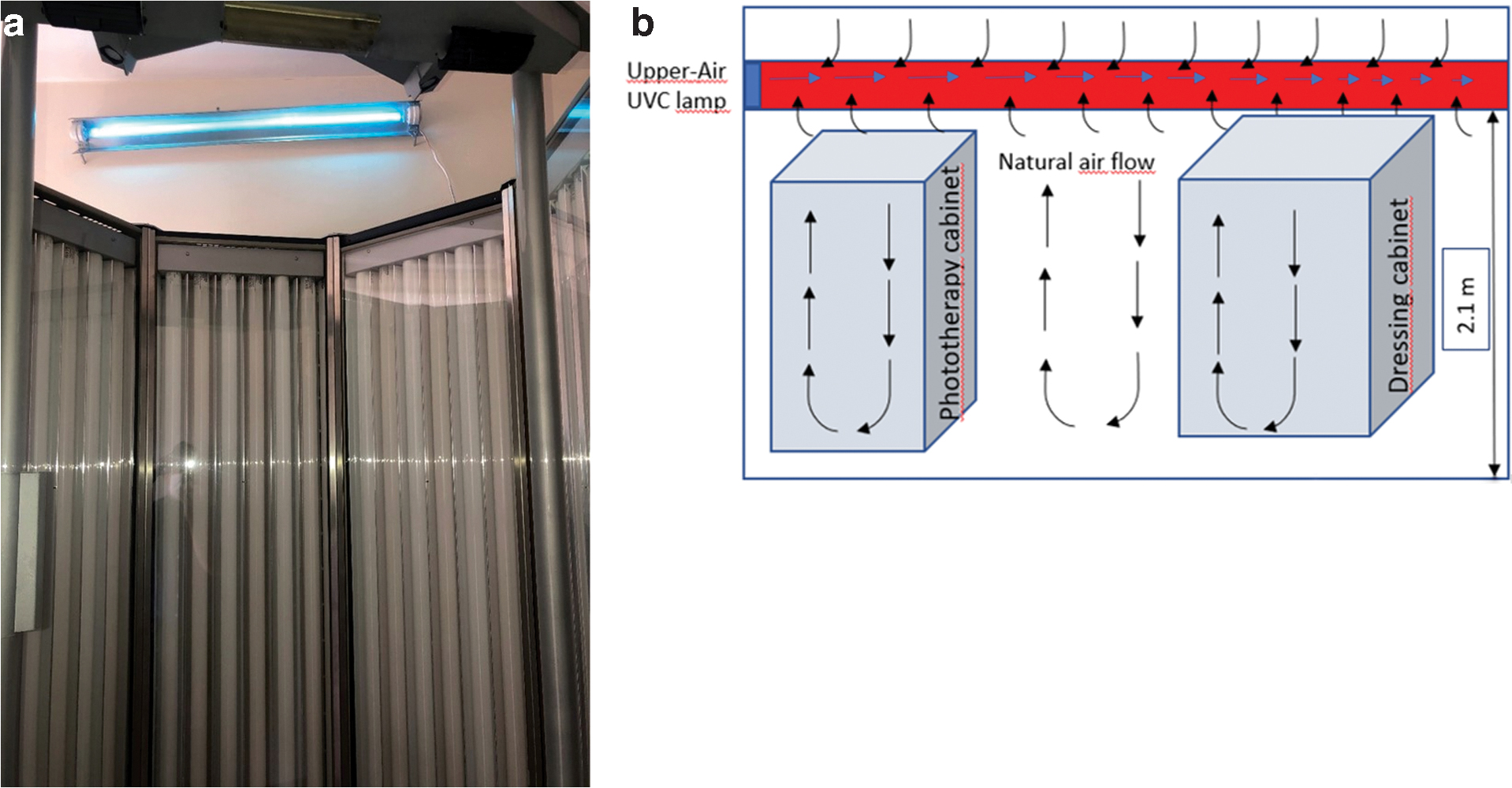
These results suggest that upper-air UVC devices that are designed and established to irradiate only air in the upper part of the rooms (>2.1 m) are able to inactivate SARS-CoV-2 in poorly ventilated PUs (Fig. 1a). 4 Upper-air UVC radiation can disinfect the entire PUs by air circulation. As the air in the room warms, it will rise and carry droplets containing viruses with it, and these viruses will enter the domain of UV (Fig. 1b). 4
UVC lamps have some characteristic features including power (W), wavelength (nm), and energy intensity (μW/cm2). The total power gives the required number of lamps according to unit size. Characteristics of UVC devices have been previously described according to the room size. In this regard, three lamps with 15 W or one lamp with 30 W or one lamp with 40 W has been reported to be adequate for disinfection in units of 3–4 m length, 5.5–7 m width, and 2.7–3 m height. 4,5 The energy intensity of the lamps is measured by the quantity of energy required per square centimeter according to 1 or 2 m distances. The energy intensity divided by the inactivated viral dose gives the effective times for viral inactivation.
[UV dose = UV intensity (μW/cm2) × exposure time (sec)].
Our lamp has 60 μW/cm2 intensity at a distance of 2 m, and has 30 W and 254 nm wavelength. Thus, the effective virucidal inactivation time of this lamp is only 3.55 sec (60 mJ/cm2 or 16.9 mJ/cm2) for SARS-CoV-2.
Considering air change per hour and viral inactivation time, 30 min of a 30-W UVC radiation is able to inactivate most of the entire poorly ventilated PUs. UVC lamp is used between the treatment section, therefore, there is no exposure of UVC and risk of carcinogenesis. Since the UV effect will increase as the distance of the target to the light source decreases, the shortest distance to see the whole target should be chosen.
There are numerous studies that support the inverse relationship between temperature and transmission of COVID-19. Also, the suitable temperature range for SARS-CoV2 survival was reported as 13–24°C. 6 In this context, it may be suggested that the room temperature should not be under 20°C.
Conclusions
The PUs that do not have adequate ventilation might be protected by upper-air UVC lamps since using chemicals alone to disinfect the rooms is not enough to inactivate viruses in aerosols. 3 In addition, this alternative may also be used in dental offices and emergency rooms where patients are often unable to use masks.
Using UVC radiation along with the rest of disinfection measures (cleaning of surfaces, masks to prevent direct respiratory contact, etc.) would allow us to have more treatment options for numerous dermatological diseases in novel PUs during the COVID-19 pandemic and possible future pandemics.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.