
Abstract
Objective:
This study aims to evaluate the in vitro effects of different biomodification treatment methods on extracted tooth/root surfaces in terms of biologically acceptable changes favoring better periodontal healing.
Background data:
The use of various agents for root surface biomodification (RSB), during periodontal procedures is of critical importance to increase the success of the treatments through healing. Ethylenediaminetetraacetic acid (EDTA) is the most frequently used chemical RSB agent in periodontal clinical practice. Erbium-doped yttrium aluminum garnet (Er:YAG) lasers have well-known advantages on blood cell adhesion and fibrin network formation on root surfaces. Recently, novel titanium nitride (TIN) curettes are of great interest due to smoother surface changes obtained after their application.
Materials and methods:
Forty-four dentine specimens from extracted single-rooted teeth were randomly divided into four groups: Group 1: No treatment; Group 2: Er:YAG laser irradiation; Group 3: EDTA gel application; Group 4: TIN curette instrumentation. All specimen surfaces were wet polished before treatments. Before and after root surface roughness parameters of all specimens were assessed with a profilometer. Further, all scanning electron microscopy micrographs were analyzed and scored for root surface and smear layer morphology characteristics by two different blinded researchers.
Results:
There were no statistical differences between the initial roughness of all groups (p = 0.687). After treatments, EDTA gel group revealed an intact intertubular area, some smear debris on dentine surfaces, and partially occluded dentine tubules. Er:YAG laser created the highest roughness (p < 0.05) among all treatment groups with no smear layer and exhibited fully exposed dentine tubules and collagen fibrils. Surfaces instrumented with TIN curette were the smoothest (p < 0.05) and covered with a compact and thick smear layer.
Conclusions:
Within the limits of this study, Er:YAG laser-irradiated surfaces exhibited exposed collagen fibrils, and Er:YAG laser irradiation was found as the only method yielding the desired surface characteristics for better periodontal healing, where the fibrils are exposed in the absence of smear layer.
Introduction
Periodontitis is a multi-species chronic infection characterized by gingival inflammation that without treatment results in the loss of tooth-supporting tissues and involves a systemic response associated with several inflammatory mediators 1 showered into the bloodstream as a reactive result against the plaque biofilm bacteria. It is the sixth most prevalent disease affecting mankind causing tooth loss and disability through infections. 2
Based on its important systemic aspects with the entrance of periodontal pathogens and by-products of inflammation into the circulatory system, the biological rationale for its connection with systemic conditions, such as cardiovascular diseases, obesity, low birth weight, etc. is described by the common theme of chronic inflammation. 3 –6 Therefore, periodontal health is a critical component of systemic health/wellbeing and the prevention of periodontal diseases is of key importance. In individuals diagnosed with periodontitis, the control and treatment of the disease through mechanical nonsurgical and surgical approaches performed on root surfaces are the keystones of high-quality modern dental services.
Since the nature of the root surfaces following nonsurgical and surgical treatments has an impact on different periodontal healing types, it is important to characterize and compare the root surfaces prepared with different mechanical and chemical means for achieving successful periodontal treatment outcomes. It has been shown that following mechanical instrumentation, as today named as root surface debridement, a layer of organic and mineralized debris forms, and acts as a reservoir for bacteria jeopardizing the healing. 7 –9 This smear layer has been found to cover the mechanically instrumented root surfaces, occlude the dentin tubules, and affect the reattachment of the cells onto the root surfaces. 10 –12 Smear layer removal, especially in the periodontal regenerative procedures and root coverage techniques is of critical clinical interest in periodontology.
Healthy root surfaces are rich in collagen and contain both intrinsic and extrinsic fibers, which form a connection between the root surface and the adjacent alveolar bone. This connection is of renewable nature. However, once the root is affected by periodontitis, it may be exposed to the periodontal pocket area and/or the oral cavity. On such a “pathological exposition,” root surface contamination and changes in mineral composition, as well as reduction of collagen fiber insertion may be observed. It has also been stated that a reduced capability to generate the required stimuli to initiate the migration of cells necessary for periodontal regeneration may be seen. 13 Therefore, root surface biomodification (RSB) procedures conducted by using mechanical agents such as lasers, 14,15 chemicals such as ethylenediaminetetraacetic acid (EDTA), 16 and biostimulators such as hyaluronic acid have been introduced in the literature to compensate for the aforementioned limitations in periodontal therapies. 17
RSB with demineralization agents suggests an increase in blood cells and fibrin adhesion on root surfaces at the early stages of periodontal healing leading to improvements in clot stabilization. 18,19 EDTA is an effective chemical demineralization agent. When used for RSB it is claimed to be effective not only in removing the smear layer but also in exposing collagen fibrils on dentine surfaces and promoting biologically acceptable surfaces. 20 Laser therapy has become an adjunctive tool in periodontal treatments with increasing interest. According to a recent systematic review and meta-analysis, it has been stated that lasers have been included in the treatment of inflammatory periodontal diseases for reducing the infection and bleeding, improving accessibility to challenging anatomical structures, decreasing patient discomfort, and stimulating the healing process. 21 Especially erbium lasers are the most appropriate application tools both on root surfaces and soft tissues due to the safety, friendly mechanism of action, and the wavelength well absorbed by water molecules. Further, it has been shown that erbium-doped yttrium aluminum garnet (Er:YAG) laser enhances blood cell adhesion and fibrin network and does not promote a smear layer formation, although root surfaces may exhibit micro-irregularities after irradiation. 22 –25 In recent years, titanium-coated hand instruments like titanium nitride (TIN) curettes have attracted attention since they do not require sharpening and have been shown to leave a very smooth root surface after application. 26
To the best of our knowledge, although there are morphological studies in this area using various measurement techniques and indices, 27,28 no comparative studies are available evaluating the changes on root surfaces and smear layer morphology characteristics created by Er:YAG laser, EDTA gel, and TIN curette for RSB purposes by using both a profilometer and scanning electron microscopy (SEM) analysis. Since the role of these aspects in periodontology is well considered, further studies on this topic could bring innovative treatment strategies to open a creative matter of debate in literature by adding new information. This study aims to evaluate the in vitro biomodification effects of different agents on extracted tooth/root surfaces in terms of biologically acceptable changes required for better periodontal treatment results.
Therefore, the hypothesis is set up to test the following: Er:YAG laser treatment reveals favorable root surface and smear layer morphology changes for periodontal healing in comparison to EDTA gel and TIN curette.
Materials and Methods
The present study was approved by both the Yeditepe University Dentistry Faculty Scientific Committee (Protocol no: 391/09/2020) and Yeditepe University Ethics Board (KAEK, 1424/2021). Sample calculation was performed by using a previous in vitro research: 29 α: 0.05, power (β) of 80%, d effect size of 1.365 for the Ra parameter, and standard deviation of 1.5. The calculated sample number was found to be minimum of 10 in each group. Since the samples were obtained from extracted teeth in periodontitis patients, all subjects were informed about their participation in the study and signed an informed consent form before extractions.
In this study, 22 single-rooted, radiographically and clinically compromised periodontally hopeless vital teeth indicated for extraction with grade 3 mobility and pocket depths over 8 mm were included. For maximum standardization, the following exclusion criteria were considered;
Systemic disease that could affect the periodontium.
Teeth with dental caries, dental restorations, and periapical infections.
History of nonsurgical and surgical periodontal treatment before extraction.
Experimental teeth were gently washed under running water and then stored in distilled water with Thymol solution at 4°C until sample preparation. Samples were prepared within 3 months.
Sample preparation
Sample preparations and all treatments were performed by a single experienced researcher and periodontist (O.L.T.).
Eleven mandibular (except for mandibular incisors) and 11 maxillary single-rooted teeth were used. For obtaining 5-mm-thick tooth slices, a low-speed diamond blade with water coolant (Isomet; Buehler Ltd., Lake Bluff, IL, USA) was used. Two parallel transverse cuts were made to prepare each slice. One cut was made at the cementoenamel junction and the other one was made ∼5 mm apical to the first cut. 25,26 The obtained 22 dentin slices were then further divided into 2 halves with a third longitudinal cut. At the end of the preparation, 44 dentin specimens were obtained.
All the specimens were then embedded in a cylindrical cast filled with acrylic resin. During the embedding procedure, the specimens were placed at a standard height. To avoid deviations in the profilometric analysis, the specimen surfaces were wet polished with a sequence of silicon carbide papers (320-600-1200 and 2000 grit). 30 All the specimens were then rinsed with sterile water solution and air dried.
Treatments
Maxillary eight premolars, two canines, one lateral incisor, and mandibular nine premolars and two canines were included in this study. A total of 44 dentin specimens with polished surfaces were prepared using these teeth and were randomly distributed using a website (
Group 1: No treatment (n = 11).
Group 2: Er:YAG laser irradiation (n = 11). Er:YAG laser (DE- Light; Hoya ConBio, Fremont, CA) with a chisel type quartz tip (1.2 × 0.4 mm rectangular shape) at an energy level of 50 mJ per pulse, and pulse repetition rate of 30 Hz in the oblique contact mode with an angle of 30° was applied. The contact tip was moved mesiodistally with sweeping motions on the entire surface for 45 sec while the irradiated area was cooled with the water spray. 31 To standardize the angulation of the laser beam, a rigid metal apparatus was designed with a guide bar at an angle of 30° to the sample surface. The main acrylic casts with the Er:YAG laser samples were fixed within this metal apparatus using a dental impression material. Therefore, to hold the chisel tip at 30° angulation throughout the whole instrumentation period, each sample was placed inside this apparatus before the laser irradiation and the bar served as a guide for the operator.
Group 3: EDTA gel application (n = 11). A prefabricated pH neutral, root surface conditioning 24% EDTA gel (pH 7.0) in carboxymethyl cellulose (PrefGel™ 0.6 mL; Straumann®, Basel, Switzerland) was applied for 2 min and then rinsed with sterile water for 60 sec and dried with air syringe.
Group 4: TIN curette instrumentation (n = 11). A TIN Gracey curette no 5/6 (American Eagle, USA) was applied with moderate to light pull strokes in the apico-coronal direction by an imbricated manner with sweeping motions for 20 sec. To operate with stable lateral forces, the experienced operator was educated and calibrated according to Braun et al. 32 previously 26 by training on extracted teeth as explained by Kawashima et al. 10 using the method of Kishida et al. 33 The pressure was aimed to be 500 g. 33,34
Root surface roughness analysis
A profilometer (Perthometer M1; Mahr, Gottingen, Germany) was used to evaluate the Ra of all specimens before and after the root surface treatments. The analysis was performed by an experienced blinded periodontist (B.E.K.). Five measurements were recorded for each specimen using different directions and different locations (randomly and without tracing the same location). 26,30,35 Profilometer measurements were done with a tracing length of 0.8 mm, and a cutoff length of 0.25 mm, and a stylus speed of 0.1 mm/sec. The mean Ra was determined by averaging the five readings. 30 The surface roughness tester (Mahr GrrbH, Gottinger, Germany) was used during the whole evaluation to periodically calibrate the profilometer.
SEM analysis
The surface morphology, smear layer, open dentine tubules, and surface patterns were analyzed with SEM microphotographs. All specimens of dentin were fixed for 24 h at room temperature using 2.5% glutaraldehyde in 0.1 M phosphate-buffered saline (pH 7.2), washed with distilled water, and then air dried.
The microphotographs of the specimens were taken using a SEM device (JSM 6335F; JEOL-USA, Inc., Peabody, MA, USA) with the technique described in our previous study. 26 To make accurate evaluations of the instrumented surfaces, SEM microphotographs of each specimen were taken at × 500, × 1000, × 2000, × 3000, and × 5000 magnifications. For the standardization of image locations, the intersection of the two diagonal lines at the midpoint of the sample surface was located under × 20 magnification. The intersection point was further zoomed at for obtaining microphotographs under higher magnifications.
Two blinded and calibrated periodontists (H.G. and E.Ö.K.) assessed the SEM microphotographs by employing the root surface and smear layer morphology characteristics index (SMCI) adapted from the literature of Aspriello et al. 36 Grades 1–4 represent the following: Grade 1: compact and thick smear layer, no dentin tubule openings; Grade 2: thin smear layer, absence of dentin tubules; Grade 3: smear debris residues on dentin surface and partially occluded dentin tubules; Grade 4: absence of smear layer on the surface with exposed collagen fibrils. Samples were examined at an increasing magnification starting from × 500 up to × 5000, by both examiners. The Kappa value was found as 96.9% (κ: 0.969; 95% confidence interval: 0.910–1.000) to verify the calibration of the two examiners.
Statistical analyses
IBM SPSS Statistics 22 was used for statistical analyses (SPSS IBM, Turkey). The Kolmogorov–Smirnov test was used for assessing the normal distribution. One-way analysis of variance (ANOVA) test was used for intergroup comparisons of parameters showing normal distribution, and Tukey's honestly significant difference (HSD) for the paired evaluation. Kruskal–Wallis test was performed for intergroup comparisons of parameters that did not show normal distribution, and Dunn's test was used for the paired evaluation to determine the group which caused the difference. Intragroup changes of parameters showing normal distribution were evaluated by the paired sample t-test. Significance was evaluated at the p < 0.05 level.
Results
There was no statistically significant difference between the initial measurements of the mean Ra values of the groups (Table 1) (p > 0.05). In the multiple comparison of the post-treatment measurements, there was a statistically significant difference between the mean Ra values of the groups (p < 0.05). After the post hoc evaluations conducted to determine the significance in pairs, the mean Ra value of the Er:YAG laser group was found significantly higher than the EDTA gel and TIN curette groups (p < 0.05, p < 0.05), and also the mean Ra value of the EDTA gel group was significantly higher than the TIN curette group (p < 0.05) (Table 2). In terms of the multiple comparison of the differences between initial and post-treatment mean Ra values of the groups, a statistically significant difference was found (p < 0.05). All groups showed statistically significant increases between the initial values (p < 0.05) and at pairwise comparisons, the mean Ra value of the Er:YAG laser group increased significantly than EDTA gel and TIN curette groups (p < 0.05, p < 0.05). Also, the increase in EDTA gel group was significantly higher than the TIN curette group (p < 0.05) (Table 2).
Initial Roughness Values of the Groups
One-way ANOVA test, p < 0.05.
ANOVA, analysis of variance; EDTA, ethylenediaminetetraacetic acid; Er:YAG, erbium-doped yttrium aluminum garnet; SD, standard deviation; TIN, titanium nitride.
The Intra- and Inter-Group Comparisons of Roughness Values Before and After the Surface Treatments
a = Er:YAG-EDTA; b = EDTA-TIN; c = Er:YAG-TIN.
Paired samples t test (a1, b1, c1 represents the significance of intra-group changes).
Tukey's HDS test (a2, b2, c2 represents the paired significant differences of the changes within the groups).
One-way ANOVA test ( * represents the significance of multiple comparisons).
p < 0.05.
HSD, honestly significant difference.
The frequency distribution of the scores of SMCI in the groups are shown in Fig. 1 and their median values and ranges are shown in Table 3. There was a statistically significant difference between the groups (p < 0.05). In the No Treatment group, all samples represent 100% grade 2 score (thin smear layer, absence of dentin tubules) on the microphotographs. In the Er:YAG laser group, all samples represent 100% grade 4 score (absence of smear layer on the surface with exposed collagen fibrils). In the EDTA gel group 18.2% of samples represent grade 2 score, whereas 81.8% of samples represent grade 3 score (smear debris residues on dentin surface and partially occluded dentin tubules). In the TIN curette group 18.2% of samples represent grade 3 score, whereas 81.8% of samples represent grade 2 score. Er:YAG laser revealed a median value of grade 4, EDTA gel grade 3, and TIN Currette grade 1 compared with the No Treatment group with a median of grade 2 (p < 0.05). There was a statistically significant difference between the groups in terms of the index scores (p < 0.05) (Table 3). The representative SEM images of each group are presented in Figs. 2–5.
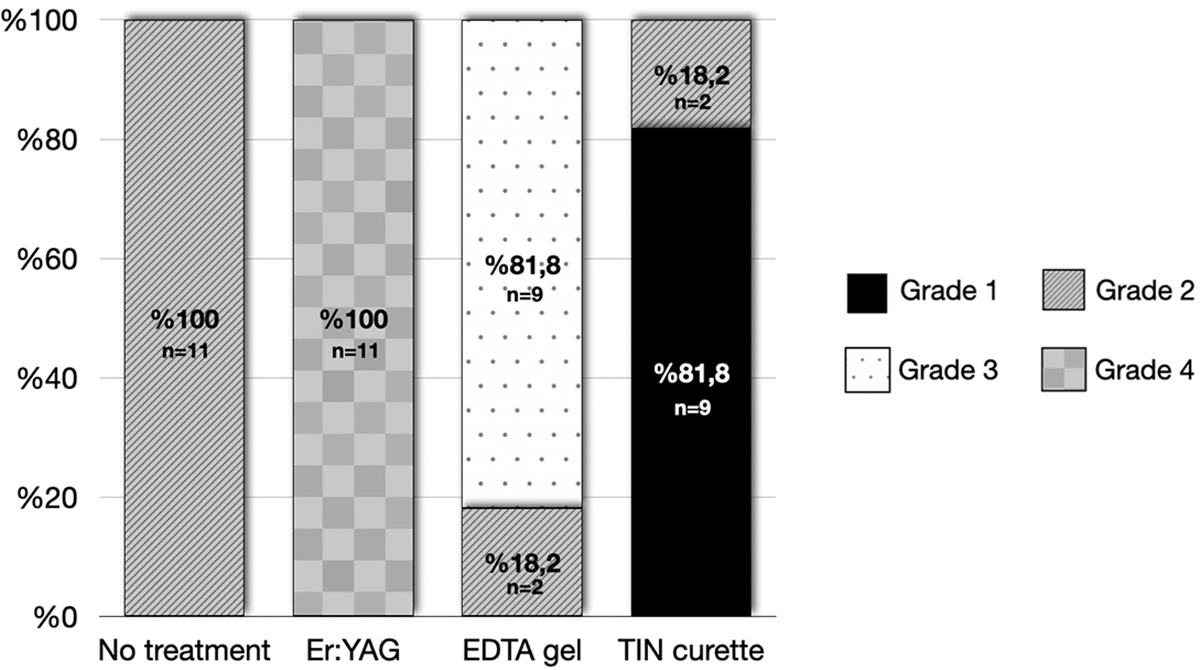
Illustration diagram of frequency distribution of root surface and smear layer morphology characteristics scores (SEM analysis). SEM, scanning electron microscopy.
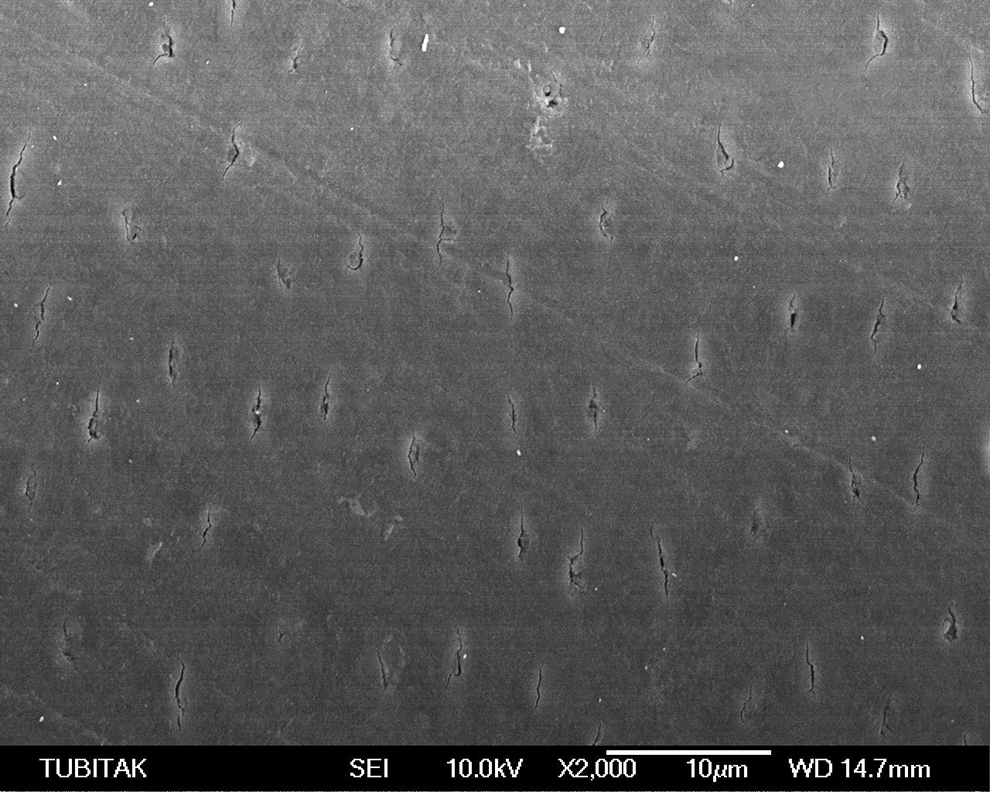
SEM image of no treatment group ( × 2000 magnification).
SEM image of Er:YAG laser-applied group ( × 2000 magnification). Er:YAG, erbium-doped yttrium aluminum garnet.
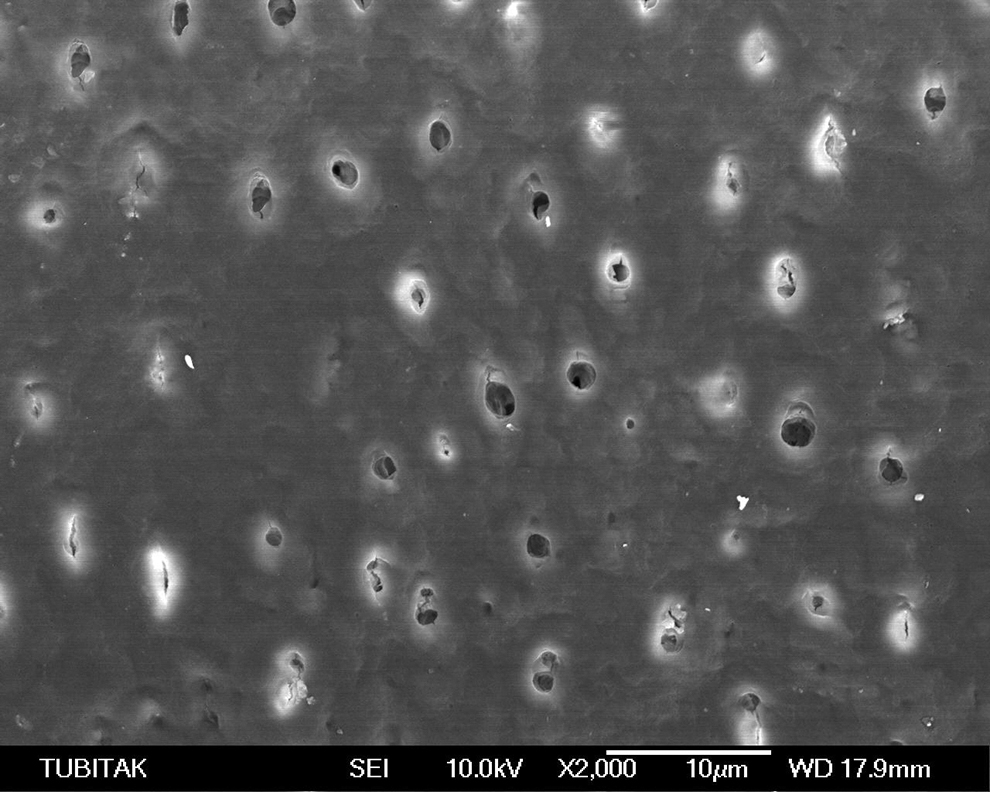
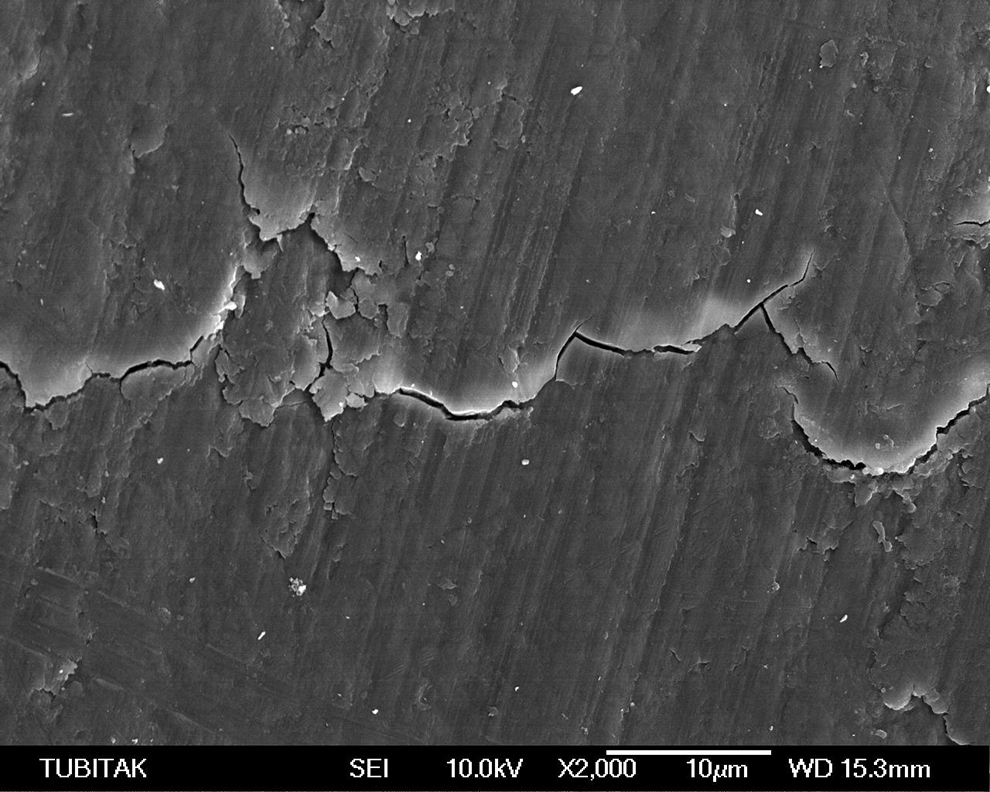
SEM image of 24% EDTA gel-applied group ( × 2000 magnification). EDTA, ethylenediaminetetraacetic acid.
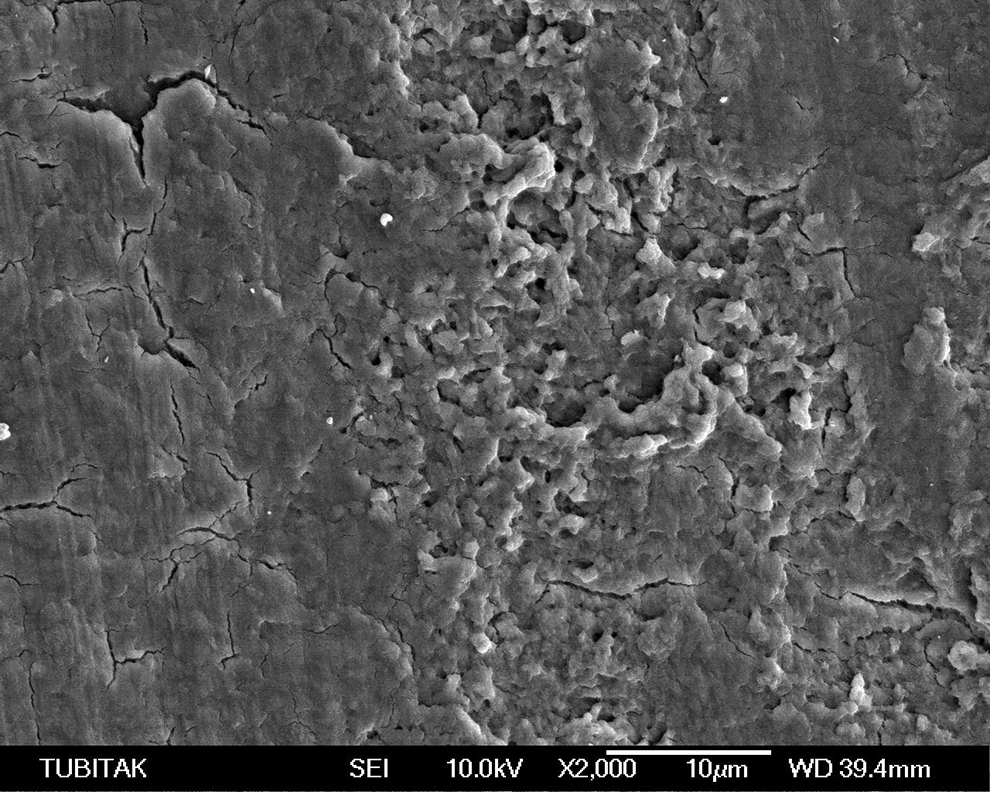
SEM image of TIN curette-applied group ( × 2000 magnification). TIN, titanium nitride.
Median Values and Ranges of Root Surface Smear Layer Morphology Characteristics Scores (Scanning Electron Microscopy Analysis)
Kruskal–Wallis test * p < 0.05.
Discussion
The creation of biologically acceptable root surfaces and the enhancement of the attachment of blood cells and collagen fibrils are of critical importance following periodontal procedures. 37 There is a complex healing process following periodontal treatments since the approached area consists of calcified tissues, including avascular and rigid root surfaces. Experimental findings suggest that in periodontitis, post-treatment improvements depend on the establishment and survival of a fibrin clot adhering to the root surface as well as the role of the inflammatory mediators of periodontitis on the post-treatment gingival healing. 4,38
The smear layer, formed as a result of mechanical instrumentation, acts as a reservoir for bacteria on the root surface and also affects the reaction of the blood cells, hence the healing. 11 Because of the contaminated nature of the smear layer, its presence on the root surfaces within the periodontal pocket or underneath the periodontal surgical flap may lead to negative consequences. The smear layer acts as a physical barrier and it can affect the migration, proliferation, and adhesion of gingival fibroblasts. 16 The purpose of biomodification with RSB agents is to remove the smear layer and improve treatment outcomes by providing biocompatible root surfaces. Collagen, which is exposed on the dentin surface by the removal of the smear layer, is also thought to be a chemoattractant for fibroblast cells. 39 However, the presence of great variability of the protocols used by the researchers in previous studies hinders consistent comparisons between different types of RSB agents. This in vitro study primarily aimed to compare surface roughness, as well as the root surface and smear layer morphology characteristics created by the usage of different RSB techniques on extracted teeth. The root samples embedded in the acrylic casts were initially wet polished with carbide papers. This was done to avoid deviations on the root surfaces during the profilometric analysis and to standardize the initial roughness and surface characteristics. There were no statistical differences between the initial mean Ra values of the groups. All the RSB methods adopted in this study increase the post-treatment mean Ra values significantly regardless of the method. However, the smoothest post-treatment surface was obtained by TIN curette instrumentation, whereas the roughest post-treatment surface without smear layer was obtained by Er:YAG laser irradiation. Er:YAG laser irradiation also provided exposed collagen fibrils as the only method yielding the desired surface characteristics for better periodontal healing where the fibrils are exposed in the absence of smear layer.
It has been stated that root surface debridement alone, as mechanical instrumentation, enhances the formation of a smear layer covering the entire surface, and occluding the dentin tubules. 40,41 However, in all of the studies published in the previous years, conventional stainless steel curettes were used. With the development of dental technology, the use of titanium-coated hand instruments as Gracey curettes has become more attractive due to their superior properties. However, to date, there are very few studies in the periodontal literature about these new instruments. In our previous study 26 evaluating the effects of different instrumentation tools on the roughness of the root surface, the results indicated that TIN curettes with a gentle mechanism of action created a smoother surface compared with stainless steel curettes. TIN curette group was included in this biomodification study to further evaluate the effects on surface changes and the thickness of the smear layer besides the surface roughness created by this pure mechanic surface-friendly gentle tool in comparison to No Treatment, Er:YAG laser, and EDTA gel groups. According to the SMCI scores, TIN curette instrumentation mostly produced a compact and thicker smear layer (Grade 1: 81.8%, Grade 2: 18.2%) on microphotographs when compared with the No Treatment group (Grade 2: 100%). However, intergroup comparison of the initial and post-treatment Ra changes revealed that Ra values provided by the TIN curette were found to be the lowest among the other treatment groups. Although TIN curette samples indicated low roughness, the presence of a thick smear layer should be taken into consideration cautiously during the root surface preparation especially before nonsurgical and surgical applications.
Since the smear layer is described as intimately associated with the root surfaces, its removal has been suggested to be accomplished through the application of chemical agents. 42,43 There are numerous demineralizing chemical agents (i.e., citric acid, phosphoric acid, tetracycline, doxycycline, EDTA, etc.) proposed for root conditioning. However, special care should be taken on the use of these agents with acidic pH due to the possibility of damage and impairment on the vitality of the surrounding soft and bone tissues. 44 On the other hand, agents with a neutral pH such as EDTA have been claimed to provide a biocompatible surface for early cell attachment and colonization without any harmful effects. 45 In the present study, the EDTA group displayed a SCMI score of Grade 3 (81.8%), representing partially opened dentinal tubule entrances with some smear layer residues. Regarding the surface roughness, the mean Ra value of the EDTA group was found to increase after application, possibly due to profilometer readings on the surfaces with the present open dentin tubule entrances. Further, the EDTA application provided intact intertubular spaces but failed to expose the collagen fibrils in any of the examined specimens. There are similar studies in the literature evaluating the surfaces on which EDTA gel is applied for different time durations. 46,47 In our study, the application time was for 2 min as stated by Blomlöf et al., 48 Fidyawati et al., 46 and Theodoro et al. 25 In those studies, it was observed that the application of neutral pH EDTA gel for 2 min was effective in removing the smear layer, but two of the above studies 25,46 did not mention any findings on the collagen fibril exposition, except Blomlöf et al. 48 Blomlöf et al. concluded that the concentration value of EDTA to obtain an acceptable smear layer removal and collagen fibril exposition within a clinically acceptable period of 2 min, was between 15% and 24%. The same group of researchers 49 asserted in another study that the long-time (3 min) applications may jeopardize the periodontal healing. In an in vitro study by Leite et al., 47 EDTA gel was applied for 3 min and it was concluded that using EDTA gel for RSB purposes may inhibit clot formation and stabilization on the root surface. Hence, the application time and concentration of EDTA should be considered as critical factors for RSB purposes.
In the present study, the surface irradiation with Er:YAG laser caused surface irregularities but exposed collagen fibrils. The literature suggests that collagen fibril exposure means of lasers can enhance the adhesion and formation of primary homeostatic buffers on root surfaces. 23 This positive effect may facilitate the healing process and fibroblast attachment. However, since the effect of collagen fibril exposure was accompanied by an increase in the surface roughness, it is possible to expect more dental plaque biofilm retention as a contributing factor for disease progression in the absence of an optimal oral hygiene level. 50 –52 However, it is well known that Er:YAG laser has a high bactericidal potential even if it is used at low energy levels. 53 Due to both the bactericidal effect and the collagen exposure without smear layer, its use for RSB procedures may well be considered.
Conclusions
Within the limits of this study, both EDTA gel and Er:YAG laser exposed the dentine tubule orifices. Er:YAG laser irradiation additionally was found as the only surface treatment method exposing the collagen fibrils together with the removal of the smear layer. Although Er:YAG laser created the highest surface roughness, it can be used for RSB purposes as it exposes the collagen fibrils in the absence of smear layer required for better periodontal treatment outcomes. Future cell culture studies are warranted to evaluate the attachment of fibroblasts onto the root surfaces following the application of comparative RSB methods. Further, clinical studies in periodontitis patients evaluating the periodontal responses after the application of RSB methods reinforced with the gingival crevicular fluid levels of the inflammatory mediators orchestrating the healing process, are of great interest.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research project was not funded by any agency(ies) or institution(s). It has been funded by the researchers.