
Abstract
Background:
Split-thickness skin grafting (STSG) is a standard therapeutic technique in patients with extensive and deep ulcers. Hospitalization and surgery can result in complications, especially in children. Photobiomodulation (PBM) has been applied in a variety of conditions such as healing of surgical, venous, pressure, and diabetic wounds, but no clinical trial using this method for healing of burn ulcers in children was found on searching the literature. The aim of the study was to evaluate the effect of PBM on the outcome of burn ulcers in children.
Materials and methods:
Informed consent and protocols were reviewed according to Shahid Beheshti University of Medical Sciences' Medical Ethics Board (
Results:
Thirty-nine children completed the study. The mean ulcer size in the two groups was similar before treatment (PBM = 60.72 cm2 ± 13.8 and STSG = 63.74 ± 7.6). In the PBM group, all wounds healed within 10–12 sessions. Analysis of the burn area was performed 1, 3, and 6 months after injury. There was a significant difference (t test) in the burn area after 6 months in the PBM group compared with the STSG group (t test; p > 0.001).
Conclusions:
This is the first study to compare PBM and STSG in burn ulcers in children. Results indicated that PBM was an effective alternative to STSG, significantly decreasing the rate of scar and hypertrophic scar formation. Potential mechanisms of PBM that may be involved in burn tissue repair are discussed.
Introduction
Unintentional injuries, especially burns, are common and are one of the major reasons for hospitalization, disability, and mortality in children worldwide. They can also be a source of acute and long-term emotional, social, and behavioral difficulties for the child and ongoing stress for the entire family. Burns can be extremely painful and life-threatening in the acute phase, and in the longer term, children may need several years of reconstructive surgery and rehabilitation, as well as adjustment to permanent deformity and functional issues.
During the acute phase, treatment includes repeated painful dressings and other invasive medical procedures, including surgery, hospitalization or regular hospital visits, and scar management. 1 One of the main burn complications is hypertrophic scar formation, with an incidence of at least 50% in children. Hypertrophic scars are pathological scars due to abnormal responses to trauma, which might be painful and itchy and cause serious functional and cosmetic disabilities. 2
Extensive partial- or full-thickness burn injuries often need split-thickness skin grafting (STSG). In this technique, partial-thickness skin is harvested using a dermatome from a healthy area to be grafted to the damaged area. Donor site availability, contraction, and scaring of the grafted wound and donor site are significant limitations. 3 Treating the hypertrophic scars on the grafted or nongrafted burn area might take months or even years and none of the available treatments, including pressure garments, intralesion corticosteroid injections, silicone gel sheeting, cryotherapy, interferon, fluorouracil (5-FU), bleomycin, high-power lasers, and surgical interventions, result in complete amelioration. 4
The high treatment cost is an important clinical challenge in all countries, estimated at approximately $4 billion annually in the United States. The rehabilitation and medical charges are higher in developing countries due to the increased rate of burn incidence. 5
Photobiomodulation (PBM) is a promising method in the treatment of acute and chronic wounds, including diabetic, vascular, and pressure ulcers, and is supported by several reviews and meta-analyses. 6,7 Several molecular mechanisms have been proposed for PBM, including cellular proliferation, enhanced mRNA and protein synthesis, neovascularization and increase in vascular endothelial growth factor (VEGF), 8 and enhancement of transforming growth factor beta (TGF-α). 9 –11 PBM also has regulatory effects on the inflammatory response 12 and epithelialization during wound healing. 13
Our previous randomized controlled trials (RCTs) showed that this therapeutic modality is safe and effective in the treatment of burn wounds in adults. 14 –17 The aim of the current study was to compare the effect of PBM with STSG on the outcome and prognosis of deep burn ulcers in children.
Materials and Methods
The study was conducted in the specialized Motahari Burn Center. Informed consent, assent, and protocols were reviewed by the Medical Ethics Board of Medical Sciences, Shahid Beheshti University of Medical Sciences (
A convenience sample of 40 children, aged 1–14 years, with deep burn ulcers and who were candidates for STSG were selected (Fig. 1). Each patient was reviewed by a plastic surgeon and a laser specialist, and a detailed history and physical examination was performed. Children with underlying diseases such as epilepsy, photosensitivity, immunodeficiency, HIV, AIDS, diabetes, and active skin problems over the treatment areas, including psoriasis or cancer, were excluded. Children with grade 2b or grade 3 burns (deep burn ulcers) were recommended for STSG. Children whose parents did not agree for a surgical intervention were enrolled in the PBM group.
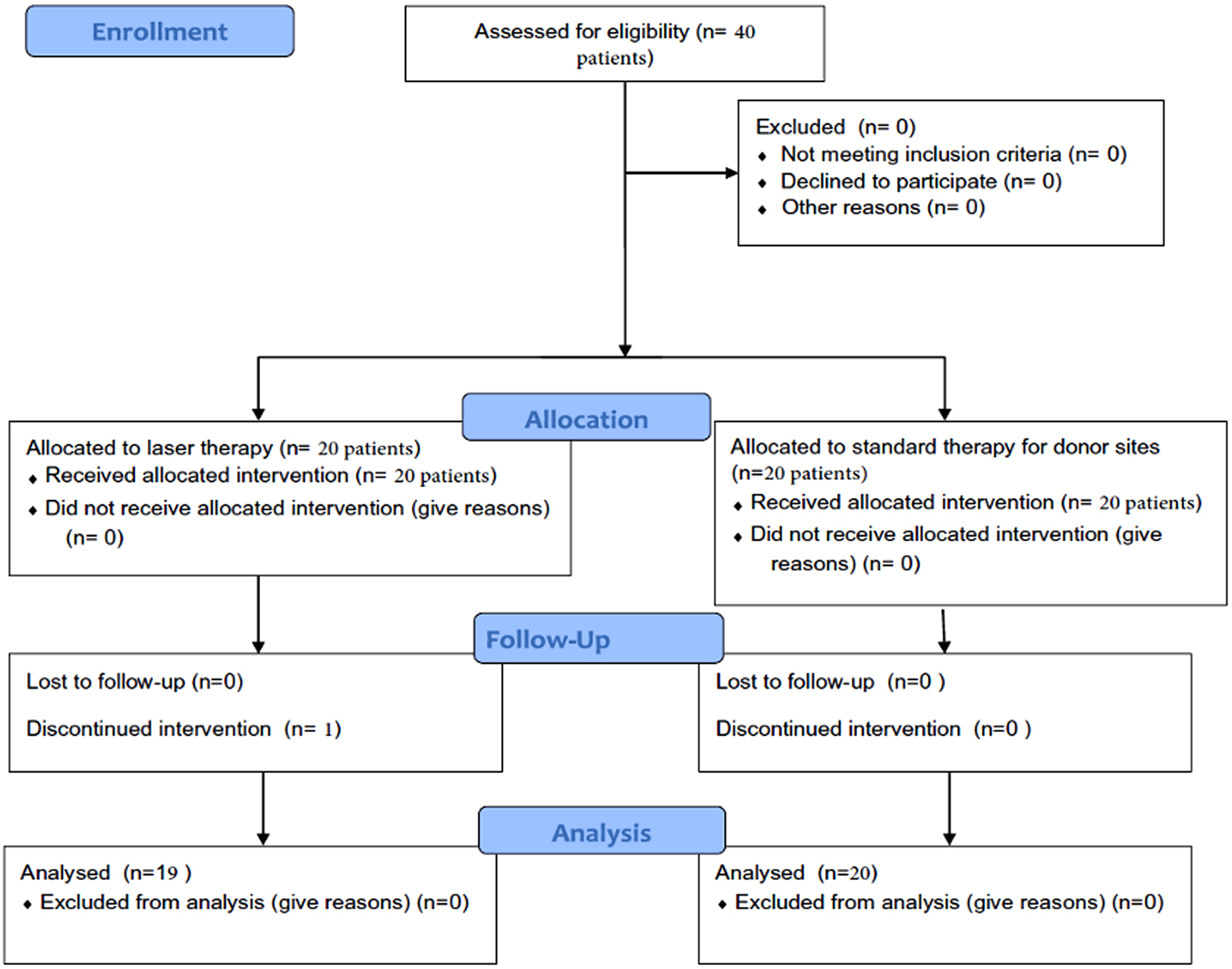
CONSORT flow diagram. CONSORT, Consolidated Standards of Reporting Trials.
Written consent was obtained from children's parents after discussing the treatment protocols. Burns were clinically evaluated for discoloration, scar and hypertrophic scar, and keloid formation. Digital photographs were taken using an iPhone 5s (United States) from a distance of 40 cm, without flash, parallel to the burn, before treatment, and at 1, 3, and 6 months after admission to the hospital. A standard ruler was used beside each wound for calibration and calculation using PictZar software (version 5.05.2).
PBM irradiation
Children in the PBM group were treated (noncontact, 1 cm from the burn area) with a 650-nm red portable laser probe (Canadian Optic Laser Center, COL laser, Canada), which was used in continuous mode in a circular pattern and had a power of 150 mW, power density of 0.25 W/cm2, and spot size of 0.6 cm2. Treatment time was 10 sec with energy of 1.5 J per point, resulting in an energy density of 2.5 J/cm2, and the application technique was punctual contact (Table 1).
Laser Parameters
CW, continuous wave; LED, light-emitting diode.
The therapist, patients, and parents (if present in the room) wore protective eye goggles. Treatment was done every other day until complete healing (10–12 sessions). Following PBM therapy, a Mepilex Ag foam (Mölnlycke Health Care Pty. Ltd., New Zealand) was used for dressing. The laser was held directly over the burn area (noncontact) after removing all the dressings, taking care to conduct all procedures aseptically.
STSG method
For children in the STSG group, early excision and grafting were performed within 3–4 days after admission, after the children were resuscitated and stable. An electric dermatome (Humaca Instruments, Poland) was used to harvest donor sites and was set at 0.4 mm. Donor skin was mainly harvested from healthy skin of the thigh or back. The Mepilex Ag foam (Mölnlycke Health Care Pty. Ltd., New Zealand) was used for dressing the grafted and donor sites.
Follow-up was done 1, 3, and 6 months after completing the treatment for both groups to evaluate complications, including discoloration, scar, and hypertrophic scar formation.
Data analysis
Normality of data was tested using the Kolmogorov–Smirnov test. Comparisons between the two groups by sex and complications were performed using the chi-square test. An independent samples t test was carried out for comparison of PBM and STSG groups regarding the wound size. Statistical analysis was performed using IBM SPSS, version 21. The analysis was done 1, 3, and 6 months after injury.
Results
Of the 40 patients who enrolled in the study, a total of 39 children, 19 females (48.7%) and 20 males (51.3%), completed the study. Data on the age of children and wound size in both groups are shown in Table 2. One patient in the PBM group could not complete the study and was excluded. Age distribution and size of the burn ulcer in the PBM group and STSG group are shown in Table 3.
Age Distribution and Size of the Burn Ulcer in the Photobiomodulation Group and Split-Thickness Skin Grafting Group
PBM, photobiomodulation; STSG, split-thickness skin grafting.
Percentage of Participants Showing Complications Due to Burn Ulcers in Photobiomodulation and Split-Thickness Skin Grafting Groups
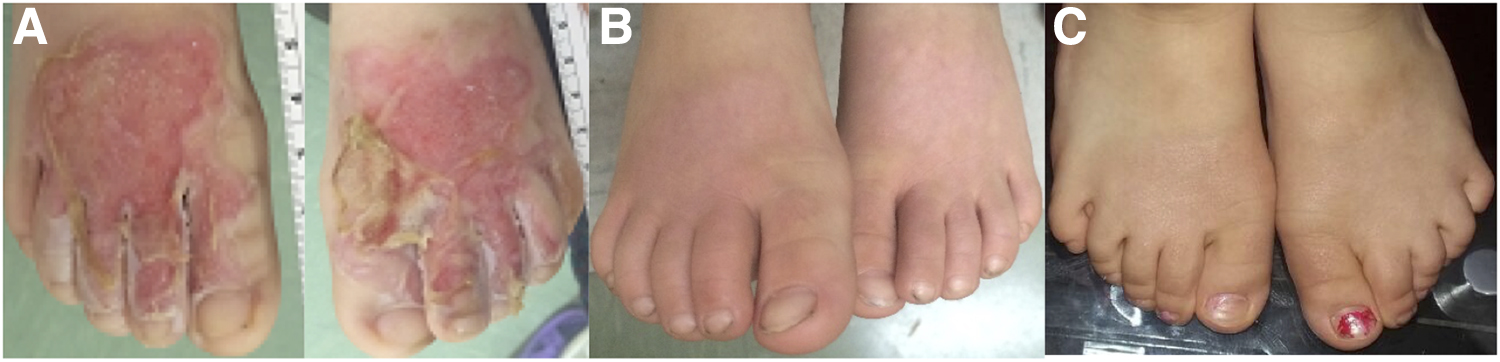
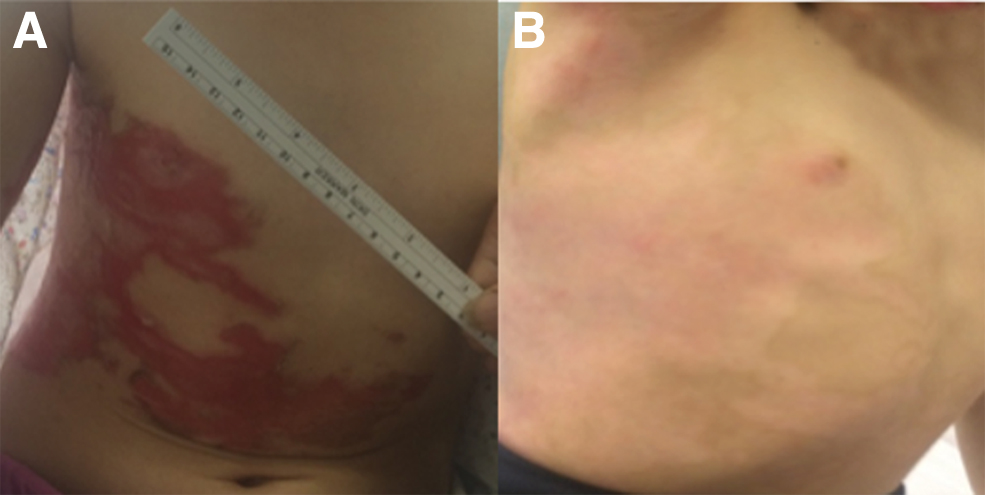
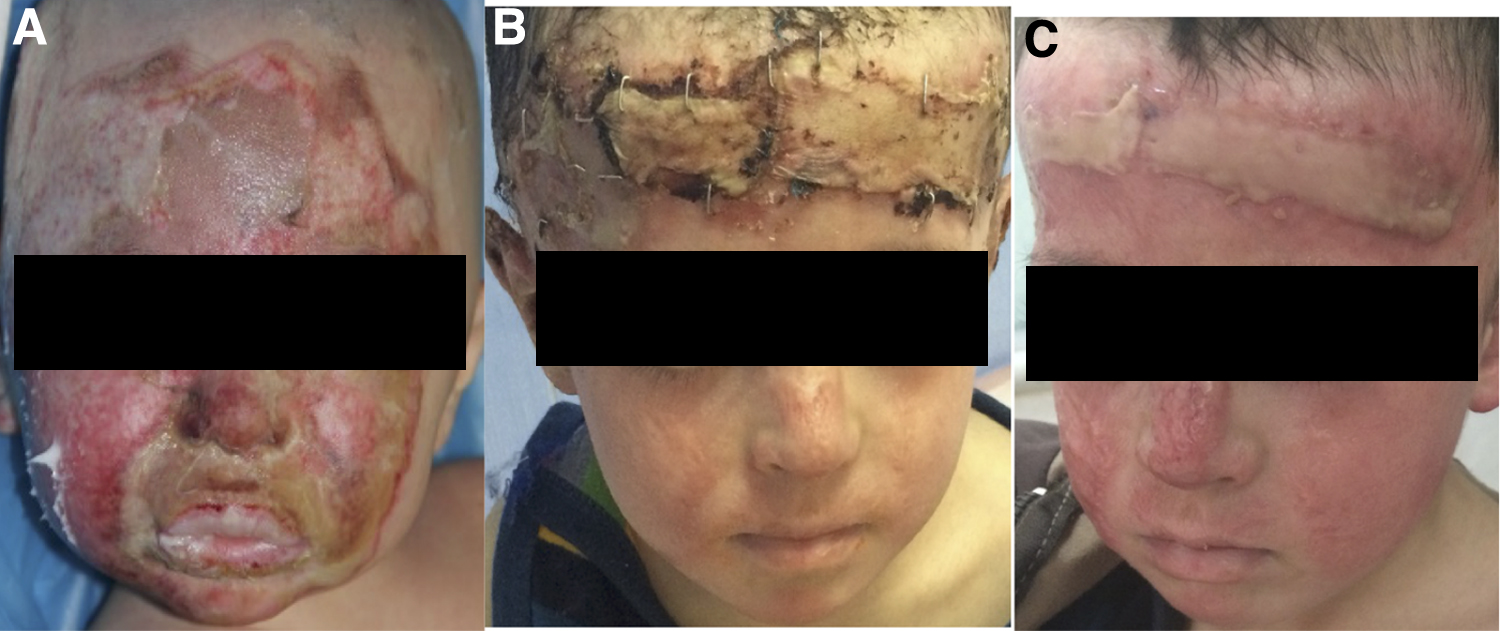
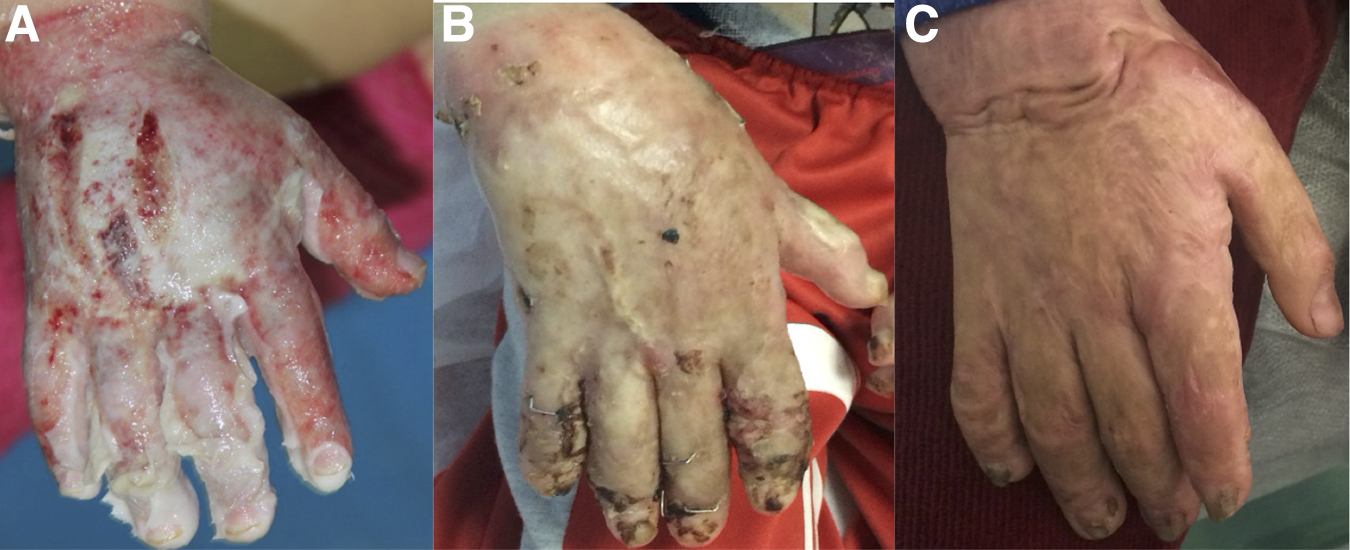
Seventeen of the 19 children in the PBM group healed completely without scar formation when evaluated at 6 months (Table 2, Figs. 2 –4). One child developed a scar and one child developed a hypertrophic scar in the burn area. In the STSG group (20 children), all had complications, including hypertrophic scar (16 children), scar (2 children), keloid (1 child), and discoloration (1 child) formation (Table 3, Figs 5 and 6).
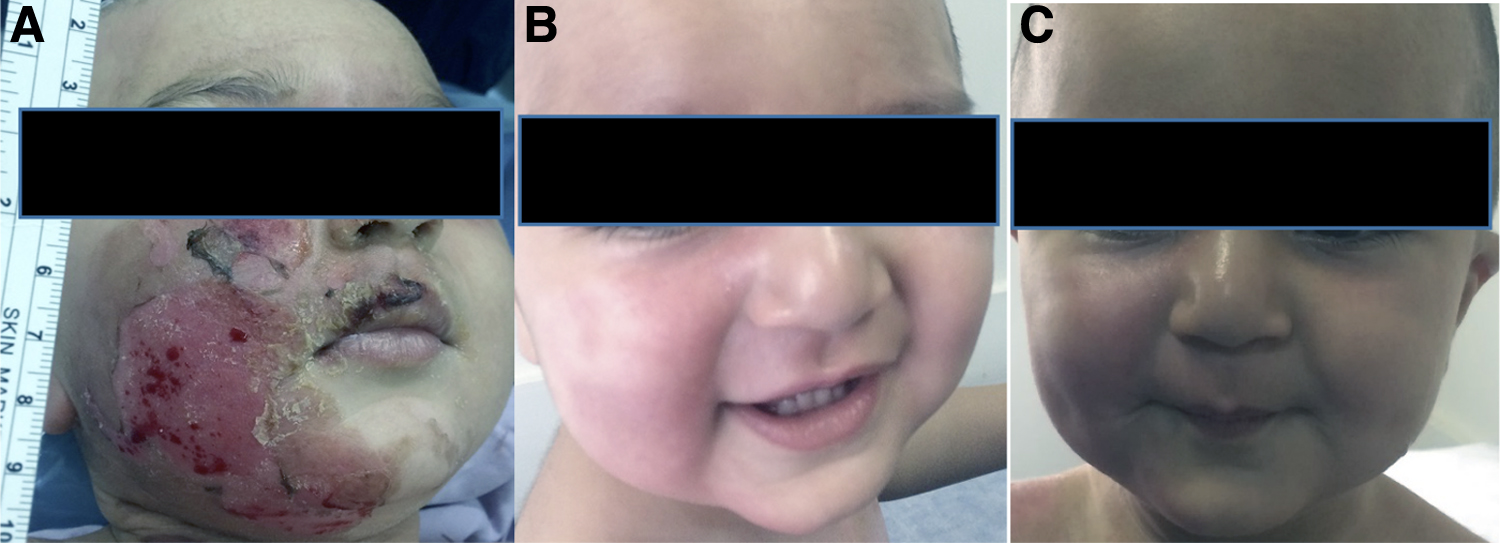
Burn ulcer in a 1-year-old boy with PMB treatment.
Burn ulcer in a 2-year-old girl.
Burn ulcer in a 6-year-old girl with PBM treatment.
Burn ulcer in a 2-year-old boy with STSG.
Burn ulcer in a 2-year-old boy with STSG.
Evaluation of the burn area after healing showed a significant difference in scar and hypertrophic scar formation between the two groups (p < 0.001).
Discussion
Burn scars are difficult to manage, and treatments that can prevent or improve scars are appreciated by both physicians and patients. In this study, we evaluated the effect of PBM for treating burn ulcers in children and compared the prognosis of this treatment with STSG. We showed that PBM can have significant therapeutic effects for wound healing compared with traditional surgical treatment.
The results strongly support the beneficial effect of PBM on burn ulcer healing without skin graft surgery and the prevention of hypertrophic scar formation compared with STSG (p < 0.001). In a previous trial, we applied PBM after skin grafting for burn ulcers in diabetic patients who were candidates for amputation. The treatment resulted in a significant improvement in the surgery prognosis. 15 Our other clinical trials also showed excellent results for PBM in the healing of donor and grafted areas in burn victims after skin graft surgery. 14,16
There have been relatively few other clinical trials using PBM for burns. Our results are consistent with an RCT conducted by Alsharnoubi et al. who reported significant positive effects of PBM to treat hypertrophic scars in children with burns. 19 In addition, an RCT was conducted by Freitas et al. 20 who also reported that PBM was effective in treating old and newly developed scars.
Results of a clinical trial by Gaida et al., 21 using a 670-nm laser to treat hypertrophic scars in burn patients, suggested a positive but limited effect of PBM on the macroscopic appearance, pain, and scars due to burns. They reported greater benefit for patients with burn scars of <12 months. They also proposed that regulation of inflammatory cytokine release and TGF-β1 stimulation have a direct impact on the scar outcome and that myofibroblast transition and epithelial–mesenchymal transition play important roles in scar formation, regulated by TGF-β1 as a critical driver. 22
There have been a number of studies of PBM and burns in animal models. Gupta et al. 12 evaluated the effect of 904-nm IR laser on the inflammatory response and healing of burn wounds in rats and reported enhancement of DNA and total protein, hydroxyproline, and hexosamine content by PBM. They suggested that PBM decreased nuclear factor kappa-light-chain-enhancer of activated B cell (NF-kB) and tumor necrosis factor alpha (TNF-α) levels and upregulated fibroblast growth factor receptor 1 (FGFR-1), VEGF, hypoxia-inducible factor 1 alpha (HIF-1α), heat shock protein 60 (HSP-60), HSP-90, and matrix metalloproteinase-2 and -9 levels.
They concluded that the 904-nm laser reduced the inflammatory response and enhanced collagen deposition, cellular proliferation, and wound contraction in the process of burn wound healing. 12
In a study of second-degree burns in rats, Trajano et al. 13 suggested that the red laser accelerated reepithelialization; formation of granulation tissue; increase in type III collagen and TGF-β expression; and increase in macrophage and myofibroblast concentrations.
Yadav et al. 23 reported that infrared laser irradiation enhanced the activity of enzymes involved in energy production and significantly increased cytochrome c oxidase (CCO) activity and adenosine triphosphate (ATP) levels as well as enhanced nicotinamide adenine dihydrogen phosphate (NADPH) levels and decreased the NADP/NADPH ratio. In addition, glucose transporter 1 (GLUT1) and phosphorylated adenosine monophosphate-activated protein kinase alpha (pAMPKα) were upregulated and glycogen synthase 1 (GS1) was downregulated, implicating increased glucose transport across cell membranes.
They concluded that PBM augmented burn wound healing and enhanced intracellular energy content by modulating aerobic metabolism for maximum energy output. 23
After several decades of experimental and clinical use of PBM, the underlying mechanisms remain elusive. Several meta-analyses and review articles have suggested that the effectiveness of PBM for accelerating wound healing is mediated by stimulation of mitochondria, increasing ATP levels, and activation of fibroblasts and keratinocytes, enhancing angiogenesis and collagen synthesis and stimulating the growth factors involved in wound healing. 24 –27
In addition, previous studies report that under stressful situations, such as cellular damage, biostimulation is more significant. 28 Under these conditions, cells express proteins, including HSPs, which promote cell adaptation and induction or prevention of cell apoptosis. 29 The activation of HSPs by PBM has been hypothesized as a mechanism of tissue repair 30,31 since HSPs, especially HSP70, are important chaperone proteins in wound repair.
It has recently been shown that HSP70 expression can be modified by PBM in tendon injury, 32 which has implications for cytokine and chemokine release. It has also been suggested that a single laser illumination on mouse skin can affect HSP70 expression in a dose-dependent manner. PBM might facilitate homeostasis through increasing the transcription factor expression, which signals HSP70 and synthesis of other anti-inflammatory proteins that enhance healing. 33 It is important to note that this response of HSPs to PBM is not necessarily a thermal effect, but can occur at normal body temperatures due to stress conditions. 34
One of the mechanisms may be activation of TGF-β, which is an essential growth factor in the process of wound healing. This activates downstream mediators, SMAD2 and 3, and results in fibroblast differentiation into myofibroblasts. 35 TGF-β3 plays a significant role in dermal and epidermal cell motility regulation and has an association with antifibrotic and scarless wound healing activity. 36 Epithelialization is an important characteristic of successful wound healing and keratinocytes and growth factors play a key role in this process. 37
It appears that following PBM, TGF-β stimulates mitogenesis, cell migration, collagen deposition, apoptosis, and fibroblast differentiation. 38 Khan et al. 39 reported a significant increase in TGF-β1 signaling in skin keratinocytes and nuclear localization of phospho-SMAD2/3 in PBM-treated wounds, 9 days postwounding. They also reported that the near-infrared laser induced proliferation in epithelial keratinocytes. 40
There are a number of limitations in the current study. In addition to the small sample size, another limitation was the distance that families of the children needed to travel. Most of the children were referred from far away cities, which meant that opportunities for follow-up of children were limited. The study was also conducted as a nonrandomized clinical trial.
Since STSG is the standard treatment for burns and PBM is not yet approved for burn ulcers, children had to be treated with the standard treatment. Therefore, PBM treatment was used for children whose parents did not consent to the surgery due to its complications. Future studies should, if possible, be conducted as randomized clinical trials with a larger sample size and long-term follow-up.
Conclusions
The present trial evaluated the effect of PBM on the prognosis of wound healing in burn ulcers compared with STSG. PBM is an effective, painless, cost-beneficial, and safe treatment, which might be used as an alternative treatment for burn ulcers in children. We speculate that activation of HSP and TGF-α expression may be important mechanisms of action of PBM in burns.
Footnotes
Acknowledgments
The authors would like to thank the Motahari Burn Center staff for their assistance and the Canadian Optic and Laser Center for providing the laser apparatus.
Author Disclosure Statement
The authors have submitted this work in their own personal–professional capacity and are not employees of any U.S.-sanctioned government. Iran is a sanctioned country.
Funding Information
No funding was received for this study.