
Abstract
Objective:
To determine effective treatment strategies against bacterial infections of burn wounds with Pseudomonas aeruginosa, we tested different treatment regimens with antibacterial blue light (BL).
Background:
Infections of burn wounds are serious complications and require effective and pathogen-specific therapy. Hereby, infections caused by P. aeruginosa pose a particular challenge in clinical practice due to its resistance to many antibiotics and topical antiseptics.
Methods:
LED-based light sources (450–460 nm) with different intensities and treatment times were used. Antibacterial effects against P. aeruginosa were determined by colony-forming unit (CFU) assays, human skin wound models, and fluorescence imaging.
Results:
In suspension assays, BL (2 h, 40 mW/cm2, 288 J/cm2) reduced bacterial number (>5 log10 CFU/mL). Applying 144 J/cm2, using 40 mW/cm2 for 1 h was more effective (>4 log10 CFU) than using 20 mW/cm2 for 2 h (>1.5 log10 CFU). BL with low irradiance (24 h, 3.5 mW/cm2, 300 J/cm2) only revealed bacterial reduction in thin bacteria-containing medium layers. In infected in vitro skin wounds only BL irradiation (2 h, 40 mW/cm2, 288 J/cm2) exerted a significant antimicrobial efficacy (2.94 log10 CFU/mL).
Conclusions:
BL treatment may be an effective therapy for P. aeruginosa-infected wounds to avoid radical surgical debridement. However, a significant antibacterial efficacy can only be achieved with higher irradiances and longer treatment times (min. 40 mW/cm2; >1 h), which cannot be easily integrated into regular clinical treatment protocols, for example, during a dressing change. Further studies are necessary to establish BL therapy for infected burns among tissue compatibility and interactions with previous therapeutic agents.
Introduction
Infections of burn wounds are one of the most important and potentially hazardous complications that occur in the acute period after burn injuries. 1,2 The thermal destruction of the skin barrier and the reduced local and systemic, cellular, and humoral immune responses of the body are critical factors that contribute to complications in patients with severe burns. 3 –5 Most nosocomial infections of burn wounds are caused by multidrug-resistant Gram-negative bacteria. 6 Pseudomonas spp. are one of the germs most frequently isolated from infected burn wounds. 6 –8 In particular, infections with Pseudomonas aeruginosa significantly increase mortality in burn patients, especially when the infection was acquired nosocomially. 9 P. aeruginosa is a Gram-negative, aerobic, sporeless, straight or slightly curved bacterium, which produces various extracellular virulence factors and has intrinsic resistance mechanisms against antibiotics. 10 –12
The ability of P. aeruginosa to maintain a chronic infection through the formation of biofilms can lead to a significant delay in burn wound healing. 13 Mostly, wound infections caused by P. aeruginosa are treated systemically with antibiotics. 14 In addition, infections of burn wounds are treated locally with the antiseptics, mafenide acetate and citric acid. 15,16 Mafenide acetate is a sulfonamide-type antibiotic that also has, besides an antimicrobial effect, cytotoxic properties and can cause metabolic acidosis through conversion to p-sulfamoylbenzoic acid and delay wound healing. 17 –19
It is known that blue light (BL) can have antimicrobial effect on many microbial strains, such as P. aeruginosa, Acinetobacter Baumannii, and Candida albicans, probably induced by photoexcitation of endogenously produced porphyrins. 20,21 Many previous studies showed that BL with a wavelength of 400–470 nm has antimicrobial properties against many clinically relevant pathogens such as Gram-positive and Gram-negative bacteria, mycobacteria, molds, yeasts, and dermatophytes. 22 However, most studies investigated the antimicrobial properties of violet light (400–420 nm) and only a few dealt with longer wavelength light (450–480 nm). 23 –28 A study showed that BL (415 nm) irradiation with 55.8 J/cm2 increased the survival rate (18.2%–100%) of mice with burn wounds infected by P. aeruginosa. 29 Also, daily BL exposures at 460 nm showed good results in the treatment of excision wounds in mice infected with methicillin-resistant Staphylococcus aureus (MRSA). 30 Compared with the nonirradiated control group, the BL treatment increased the survival rate (100% vs. 50%) and wound healing (90% vs. 18%).
Recently, we confirmed antimicrobial properties of the BL against P. aeruginosa at wavelengths of 420 and 455 nm with irradiances of 50 mW/cm2 achieving a significant bacterial reduction of 6 log10 CFU at 180 J/cm2 in suspension assays. 28
Many studies indicate that BL, or more precisely violet light (400–440 nm), has toxic effects on skin cells, including keratinocytes, fibroblasts, and skin-derived endothelial cells even in considerable low doses. 25,27,31 –33 Nevertheless, BL at 440–460 nm did not damage dermal fibroblasts and keratinocytes at any used dose up to 500 J/cm2. 25,27,28
Therefore, BL (440–460 nm) can be a promising alternative option for the treatment of skin and wound infections. Since heat generation by high-intensity BL irradiation may be an issue for wound treatment, we evaluated in the presented study the antibacterial efficacy of different treatment regimens with lower irradiances against P. aeruginosa.
Materials and Methods
Light sources
The light sources we used were the Lullaby™ LED Phototherapy System (Ohmeda Medical, a Division of Datex-Ohmeda, Inc., Laurel, USA made in India, REF: 2052663-001, SN: SGT18500008PA) with peak emission at 458 ± 8 nm, LED Array (Philips, Amsterdam, the Netherlands) that emitted BL at a center wavelength of 455 ± 10 nm, and the LED Light Bar (BML Horticulture from Austin, USA) with a wavelength of 450 ± 11 nm was used (see Table 1). The irradiation intensities were determined using a calibrated densitometer (RM21; Dr. Gröbel, Ettlingen, Germany). The temperature development was measured using a digital thermometer (Digitalmultimeter, Type: EM392B, REV Ritter GmbH, Mörnbris, Deutschland; Signstek 3 1/2 6802 II Dual Channel Digital Thermometer Hertfordshire, England). All experiments were conducted using the same treatment parameters of the respective radiation source.
Table to Report Parameters in Experimental and Clinical PBM Articles
The distance between the samples and the Lullaby LED phototherapy system was 5 cm and the irradiance 20 mW/cm2. The times of the irradiation were 60 or 120 min. This corresponds to a dose of 72 or 144 J/cm2, respectively. The irradiation with the LED array took place with distance of 4 cm and an intensity of 40 mW/cm2. Irradiation for 60 or 120 min resulted in a radiation dose of 144 or 288 J/cm2. Long-term irradiation with the LED light bar and an intensity of 3.5 mW/cm2 took place over 24 h. At an irradiation distance of 17 cm, this corresponds to an irradiation intensity of 302 J/cm2.
Pseudomonas strain and culture conditions
The bacterial cultures used originate from the Leibniz Institute DSMZ—German Collection of Microorganisms and Cell Cultures and were cultivated on casein/soy peptone agar plates. For this study, the subculture II of P. aeruginosa was used (batch no.: 0411).
For performing the experiments one colony was picked from a freshly streaked plate and solved in 5 mL tryptone soya broth (TSB). By means of a spectrophotometer (600 nm; BioTek, USA) and further dilution steps with TSB, the bacterial suspension was standardized to 1.5 × 108 CFU/mL, which corresponds to a 0.5 McFarland standard, and then diluted to the concentration required for the experiment. 28
BL inactivation of P. aeruginosa
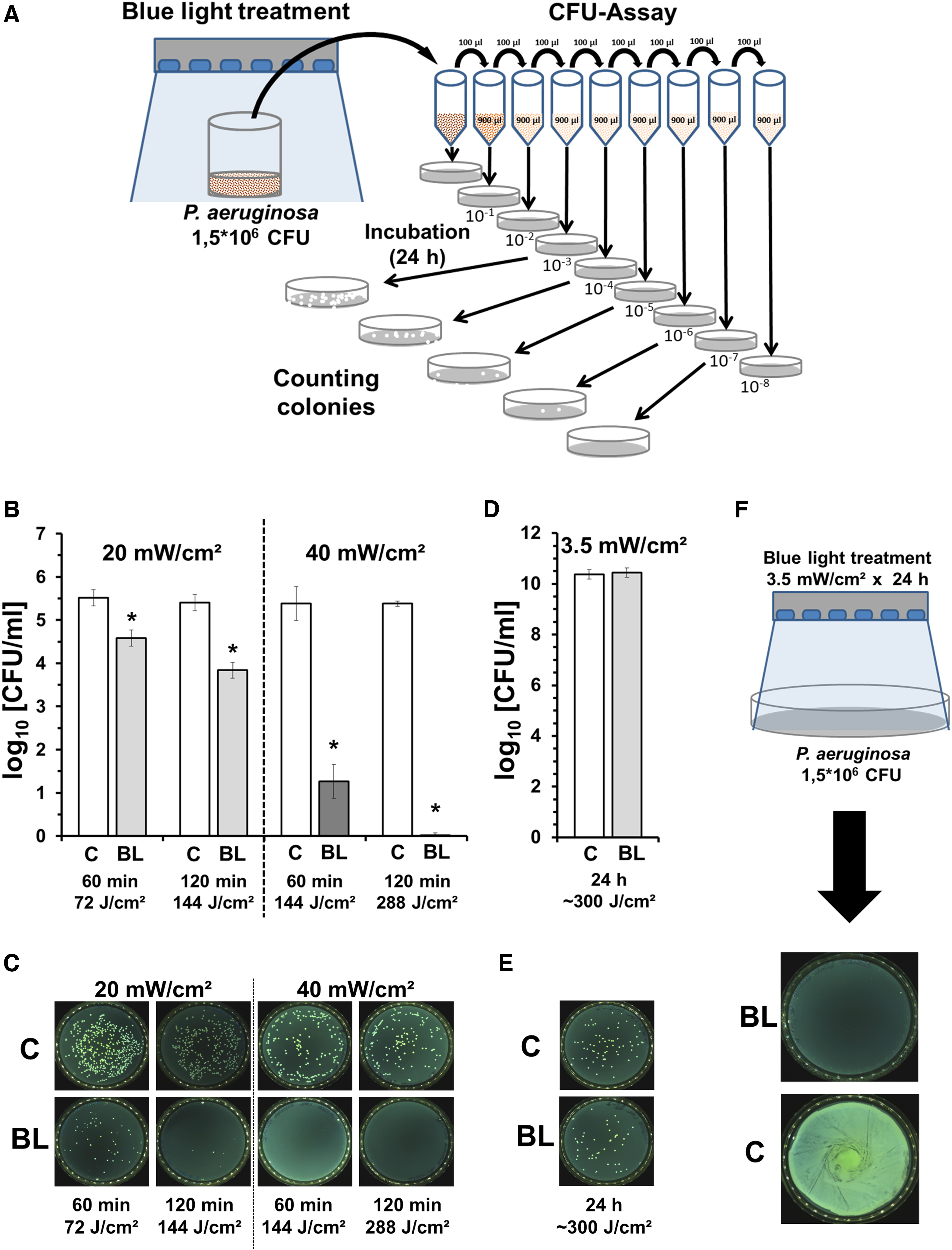
The antimicrobial efficacy of the BL was tested on bacterial suspensions of 1.5 × 106 CFU P. aeruginosa in 12-well cell culture (Sarstedt, Nümbrecht, Germany) plates with 1.75 mL TSB culture medium (n = 4–5) as shown in Fig. 1A. The temperature during the treatment with the Lullaby LED phototherapy system was 30°C, equivalent to this, the control groups were placed in a 30°C temperature-controlled incubator. Due to the heat generated during the irradiation with the LED Array, two additional fans were used to keep the temperature equivalent to the control group, which was maintained at ∼37°C in a temperature-controlled incubator. The long-term irradiation with the LED light bar took place in an incubator (Labotect, Dillenburg, Germany) under standard conditions (37°C with 5% CO2). The control groups were stored under the same conditions without irradiation. Bacterial counts were determined by colony-forming unit (CFU) assay.
BL (450–460 nm) exerts antimicrobial efficacy against Pseudomonas aeruginosa.
CFU assays
Immediately after BL irradiation, dilution series of samples and an untreated control of each experiment were prepared with TSB for quantitative determination of potential surviving bacteria and distributed on casein/soy peptone agar plates (Fig. 1A). Bacterial survival (CFU/mL) was determined by counting colonies with a colony counter (Interscience; Scan 500, Paris, France) after overnight incubation of the agar plates at 37°C (Thermo Fisher Scientific, Marietta, OH, USA).
Low-dose long-term irradiation
For the irradiation of the agar plates with the LED Light Bar (450 nm Royal Blue), a bacterial suspension of 100 μL with 1.5 × 106 CFU P. aeruginosa was inoculated at the agar plates. Irradiation with the LED light bar took place in an incubator at 37°C, immediately after inoculation. Meanwhile, the control samples were placed under standard conditions in an incubator at 37°C. After a treatment period of 24 h, bacterial colonization was photodocumented and compared with the control group.
Colony size growth assay
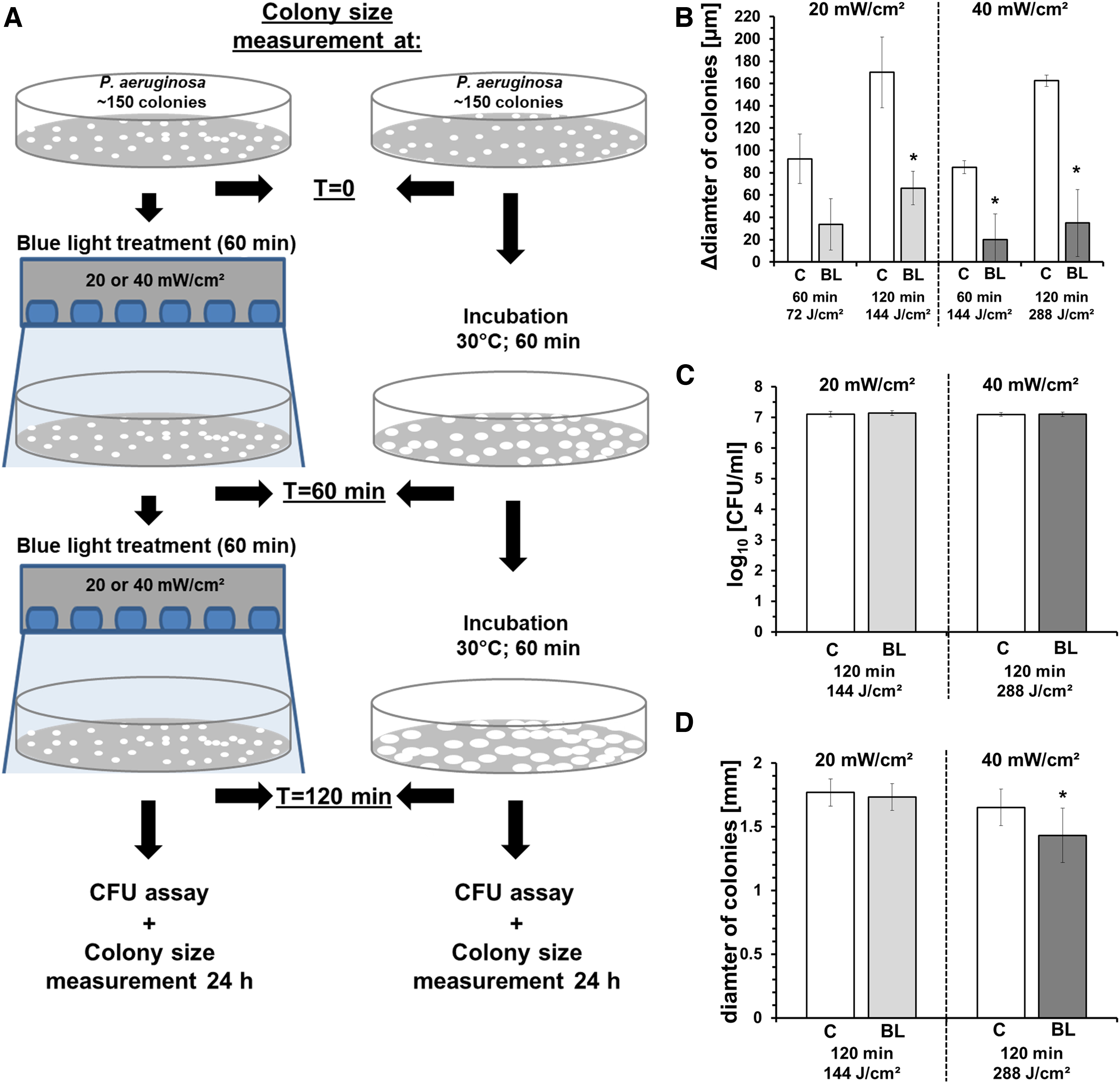
One day before irradiation with the Lullaby LED Phototherapy System and the LED array, a P. aeruginosa dilution series was prepared with the cell culture media TSB to inoculate the agar plates with the target number of colonies (∼150 CFU). After 24 h incubation at 37°C in the incubator, the number and mean diameter of CFU/colonies on the agar plates were first photodocumented, measured, and analyzed by colony counter (Interscience; Scan 500). Further photodocumentations and measurements were performed after 60 and 120 min irradiation by the respective source. Subsequently, the colonies of the samples were harvested and spread in a dilution series on agar plates for the determination of the bacterial survival rate (CFU assay). For the preparation of the dilution series, the bacterial concentrations were adjusted to the same concentration again using the spectrometer. There was no significant difference of needed dilution volumes during the initial adjustment of CFU 1.5 × 106 prior dilution series. After 24 h, the colonies of the samples were photodocumented, counted, and analyzed again. The experimental setup is illustrated in Fig. 2A.
BL (450–460 nm) slows down colony growth of Pseudomonas aeruginosa.
Wound skin model
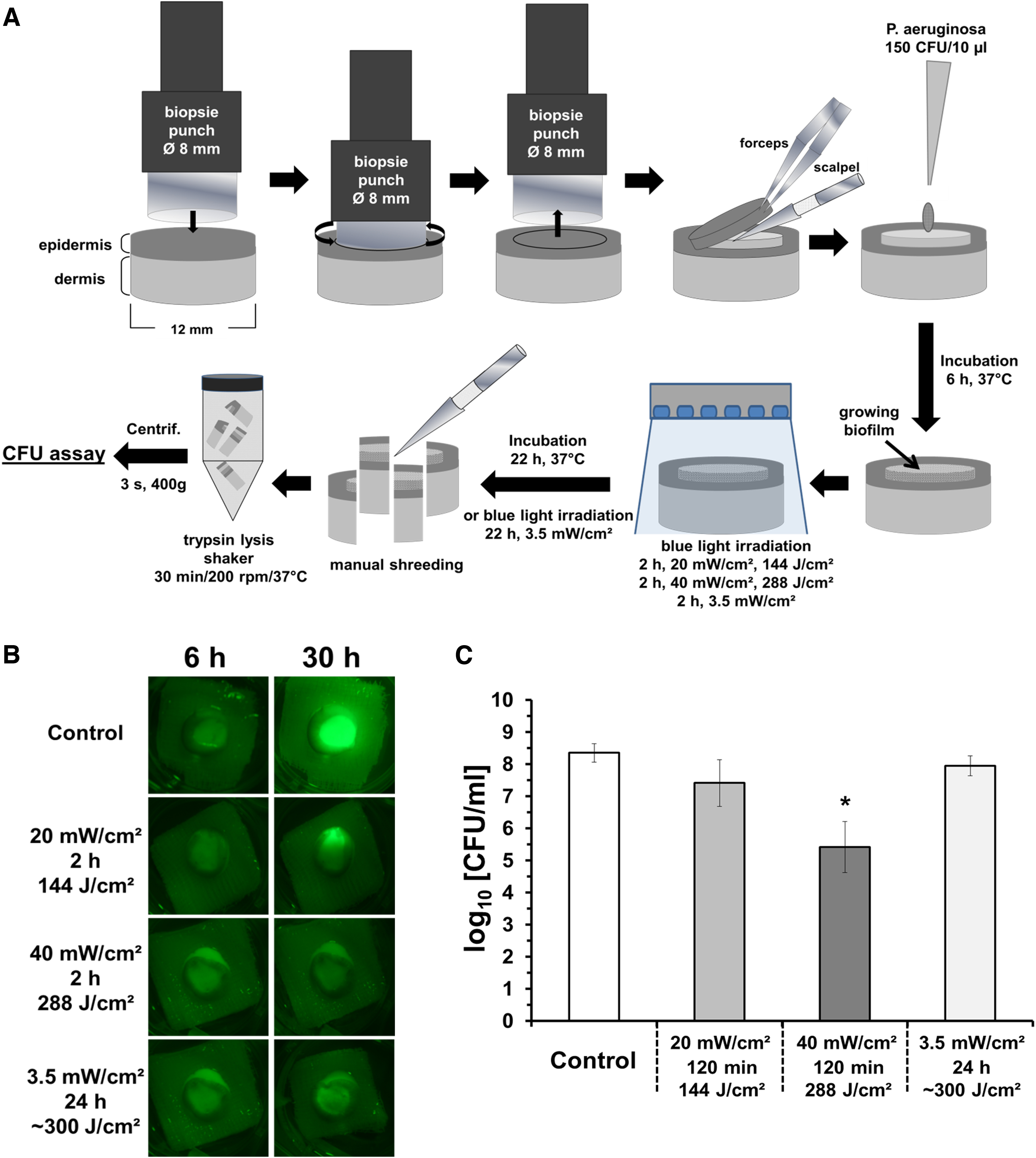
An overview of the experimental setup is shown in Fig. 3A. Tissues from abdominoplasties performed at the Clinic for Plastic Surgery, Hand Surgery, Burn Center, Cologne-Merheim Hospital were used as skin preparations. Material from three patients ages between 27 and 49 years (mean age 42 years) was used. The use of human skin samples were with donor consent and approved by the local Ethics Committee of the University of Witten/Herdecke (Votum No. 15/2018) and was in accordance with the Declaration of Helsinki. The skin preparations were transported postoperatively on ice in a sterile container to the laboratory. The skin was washed for 1 min with 70% ethanol (Carl Roth, Karlsruhe, Germany) before being processed within the experiments. Afterward, round skin samples were obtained by using biopsy punches (12 mm; Acuderm, Inc., Fort Lauderdale, USA). A standardized wound of 8 and 1 mm depth was prepared by removing the epidermis carefully with a biopsy punch (Acuderm, Inc.) and a scalpel [BRAUN (Aesculap AG), Tuttlingen, Germany] into each sample.
Antibacterial efficacy of BL (450–460 nm) treatments in skin wound model.
The samples were placed in six-well culture plates on cut sterile compresses of 1.5 × 1.5 cm surrounded by 5.0 mL of the cell culture medium, DMEM [1.0 g/L Glucose, w/o
The irradiation for 24 h with the LED Light Bar −450 nm Royal Blue took place in an incubator at 37°C with 5% CO2. After irradiation of the skin samples, all samples were prepared, manually processed in a standardized manner with the aid of trypsin solution [Trypsin 0.25%, with 10% phosphate-buffered saline (without Ca2+/Mg2+), and 0.02% EDTA (AN Biotech)] for evaluation with a dilution series onto agar plates to determine the bacterial survival rate (CFU). In preliminary experiments, we could exclude significant toxic effects of this enzymatic treatment on P. aeruginosa. These agar plates were incubated for 24 h in an incubator (37°C) and colony numbers were determined by a colony counter.
P. aeruginosa is known for its propensity to form biofilms in wounds and to produce pigments showing fluorescence in the violet spectra. 34 Therefore, in a darkened room, we used a commercially available LED black light torch (395 nm; Bestsun, Jiaxing, China) to trigger a possible bacterial autofluorescence in the wound area of our skin samples. Photos of the samples/autofluorescence were taken before the start of the treatment (6 h after inoculation of the bacterium) and before evaluation (after 30 h, of which were 2- or 24-h irradiation time) under black light illumination and standardized conditions (6-sec exposure time), using Schott filter (2 mm OG515 + 2 mm BG7; Advanced Optics SCHOTT AG, Mainz, Germany) and a camera (D5200; Nikon, Tokyo, Japan) with lens (DX AF-S Nikkor 18–55 mm).
Statistical analysis
For statistical analysis, GraphPad Prism Version 8.4.3 (San Diego, USA) was used. Significant differences were evaluated using one-way analysis of variance (ANOVA). A p-value of <0.05 was considered significant.
Results
BL has antimicrobial efficacy against planktonic P. aeruginosa
BL irradiation of planktonic P. aeruginosa cultures showed significant reductions of log10 CFU with 20 and 40 mW/cm2 (Fig. 1B, C). By using 40 mW/cm2 for 120 min (288 J/cm2), an inactivation efficacy >5 log10 CFU could be obtained. In comparison, applying a dose of 144 J/cm2, using 40 mW/cm2 was more effective (>4 log10 CFU) than using 20 mW/cm2 (>1.5 log10 CFU). Also, a dose of 72 J/cm2 obtained by a 60 min irradiation at 20 mW/cm2 showed a smaller but significant reduction by ∼1 log10 CFU. After applying 300 J/cm2 in 24 h with an irradiance of 3.5 mW/cm2, no significant antibacterial efficacy was detected (Fig. 1D, E). However, a low-level irradiation (3.5 mW/cm2, 24 h, ∼300 J/cm2) of a plated P. aeruginosa suspension on agar plate could suppress bacterial growth and colony forming completely (Fig. 1F).
BL can reduce the colony growth rate of P. aeruginosa
BL irradiation P. aeruginosa colonies significantly inhibited the colony growth during irradiation applying 20 or 40 mW/cm2 up to 120 min (Fig. 2B). In this study, 40 mW/cm2 was roughly two times more effective than 20 mW/cm2.
When all colonies were picked after direct irradiation (120 min) for further CFU assays, no significant reduction of bacterial number was observed (Fig. 2C). Interestingly, as shown in Fig. 2D colonies of plated bacteria were significantly smaller in size, when they were picked from irradiated agar plates (40 mW/cm2).
BL shows antibacterial effects on P. aeruginosa in skin wound model
Using a quantifiable skin wound contamination model with P. aeruginosa (Fig. 3A), the effects of different BL irradiations were investigated. As demonstrated in Fig. 3B BL in all intensities were able to reduce the fluorescence signals of P. aeruginosa growing in the artificial skin wound.
As shown in Fig. 3B, low-level irradiation (3.5 mW/cm2) for 24 h (∼300 J/cm2) did not reduce the bacterial number. Also, it was observed that irradiation with 20 mW/cm2 for 2 h (144 J/cm2) did not result in a significant reduction, whereas by irradiation for 2 h with 40 mW/cm2 (288 J/cm2), a significant reduction of 2.94 log10 CFU/mL was achieved.
Discussion
Nosocomial infections of burn wounds with P. aeruginosa are unfortunately very common in burn centers and represent a life-threatening complication. 6,9
This is mostly due to its properties of intrinsic resistance mechanisms against antibiotics and its production of extracellular virulence factors. 10 –12
Many studies demonstrated the antimicrobial efficacy of BL irradiation against mycobacteria, molds, yeasts, Gram-negative bacteria, and also Gram-positive bacteria. 22,35
However, most of these studies investigated the antimicrobial efficacy of BL devices (LED) emitting with narrow band 405 or 415 nm. To avoid misunderstandings when using these wavelengths, the term violet light (400–440 nm) should be preferred instead of BL. 22 In general, violet not only demonstrated strong antibacterial efficacy, but also strong toxic effects on skin cells. 25,27,31 –33 In comparison, using BL at 450–460 nm did not show any cell-toxic effects on dermal fibroblasts and keratinocytes at any dose up to 500 J/cm2. 25,27,28
For cells within the skin, the situation is different, as the cornea and epidermis absorb a large part of the light. Dai et al. could show that BL irradiation (415 nm) at a dose of about 56 J/cm2 could not induce DNA damage/apoptosis in intact mouse skin. 36 We could show in a previous study on explanted human skin that BL (453 nm, 200 J/cm2) did not lead to an increase in apoptosis events. 37 However, it should be noted that in a wound, therefore without intact epidermis, the BL toxicity could possibly be higher, as the local cells, especially fibroblasts, would be exposed to a higher intensity and thus a higher, possibly toxic dose.
In a recent study, we could confirm that the antibacterial efficacy of the wavelength range of 402–420 nm is the most effective section of the BL spectrum, but we found that BL at 453 nm (50 mW/cm2) had also sufficient antimicrobial potential for dealing with Escherichia coli and Staphylococcus epidermidis and P. aeruginosa. Apart from observed antibacterial effects, in this study we also demonstrated that BL at 453 nm, effectively inhibited biofilm formation, in particular, against P. aeruginosa. Therefore, in the present study we used the non-cell toxic BL 450–460 nm and focused more on different treatment options with varying irradiances and treatment times as preclinical evaluation for treatment of P. aeruginosa-infected wounds.
Our results indicate that against P. aeruginosa BL at 450–460 nm, also at lower irradiances, can reveal significant antimicrobial effects, which depends on dose, and also on the intensity/irradiance during irradiation. Higher irradiance is normally correlated with deeper penetration of light into the irradiated medium/tissue; thus, as shown in Fig. 1B in a suspension bacterial assay, the antibacterial efficacy was higher using 40 mW/cm2 for 1 h than using 20 mW/cm2 for 2 h, although in both cases the used doses were the same. A low-level irradiation with 3.5 mW/cm2 for 24 h did not show antimicrobial effects in this assay setup, where suspensions of bacteria were irradiated in cell culture wells. However, when the medium level was reduced by plating P. aeruginosa on agar plates, low-level irradiation also inhibited bacterial growth (Fig. 1F). Furthermore, by irradiation of colonies on agar plates it becomes clear that a further important parameter for the antibacterial efficacy of BL is the bacterial density. Although BL significantly prevented the expansion of the colonies, it did not affect much the bacterial number within the colonies.
We hypothesize that the BL is ineffective because of the strong absorbance by the high bacterial density of the colonies. Eventually, the mean irradiance achieved within the biomass of a colony is not sufficient to kill the bacteria in deeper layers, but only at the margin of upper layers. Interestingly, although the direct BL-induced toxicity on colonies is marginal, it seems that BL irradiation may exert longer lasting effects on P. aeruginosa, as seen in smaller sizes of colonies derived/subcultivated from irradiated colonies 24 h after irradiation (Fig. 2E).
In a proof-of-concept study using human donor skin with defined wounds—the skin samples were partially deepithelialized and very similar to debrided skin—and standardized inoculums of P. aeruginosa, BL with all used irradiances induced a striking reduction of bacterial fluorescence. However, only a 2 h treatment at the highest irradiance (40 mW/cm2); thus, a dose of 288 J/cm2 exerted also a significant and clinically relevant reduction of bacterial number (Fig. 3).
Although the fluorescence signal decreased significantly in the contaminated skin wounds by low-level long-time irradiation, the bacterial count was hardly affected and not significantly different to the nonirradiated controls (Fig. 3). In this study, there is a possibility that BL irradiation already at lower, nonantibacterial irradiances may bleach or inhibit the formation of fluorescent bacterial pigments. Thus, an evaluation of bacterial colonization by fluorescence using a Wood lamp or a MolecuLight wound imaging device after BL exposure may not give reliable results. Low-level long-time irradiation by using for example an LED array under wound dressing may be a prophylactic approach when dealing with low bacterial number, but could possibly fail when dealing with manifest infection/BL contamination.
However, a combined therapy of BL with conventional or unconventional antibiotics, for example BL (405 nm) with phytochemical carvacrol and/or ciprofloxacin may represent a potential treatment strategy against P. aeruginosa or other multidrug-resistant infection. 38,39
In conclusion, treatment or prophylaxis of P. aeruginosa burn wound infections with BL represents an alternative. However, the irradiation time up to 2 h is too long and, therefore, unpractical in the clinical practice. Furthermore, higher irradiances are necessary for a relevant reduction of bacterial burden, which in turn can be accompanied by excessive heat generation in the wound/skin area. Thus, decreasing the treatment time by increasing the irradiances is limited. In this study, in our experience, irradiances around 40–50 mW/cm2 can be applied without active cooling, however, temperature monitoring is obligatory. Irradiation and cooling by ventilation may lead to drying of the wound area; thus, covering the wound area by transparent dressing may also be necessary during irradiation.
Possible alternatives are repeated irradiations with lower irradiances or the use of pulsed BL, which showed good results against Propionibacterium acnes in vitro. 40,41
Thus, further optimization of BL treatment parameters is needed prior a clinical use.
Whether BL irradiation as monotherapy has advantages against standard wound cleaning by irrigation and mechanical debridement, and the application of topical antibiotics, such as mafenide/acetic acid, needs to be evaluated in further studies. In addition, BL therapy combined with these established treatments and/or with unconventional antibiotics and photosensitizers may represent promising approaches in the treatment of critical skin and wound infections.
Footnotes
Authors' Contributions
M.-C.D.L.: Investigation (lead), formal analysis; writing (supporting); I.P.: Investigation; methodology (lead) writing (supporting); review and editing; and project administration; M.B.: Resources; writing—Review and editing; investigation; and validation; P.C.F.: Resources; writing—review and editing; and project administration; A.K.E.B.: Investigation; writing—review and editing; J.L.S.: Resources; writing—review and editing; C.O.: Supervision, funding acquisition, conceptualization, formal analysis, and writing–original draft.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the German Research Foundation DFG (OP 207/11-1).